






3D Collagen Scaffold for Chronic Wounds: Case Series Insights
Three-Dimensional Hepatic Collagen Scaffold for Chronic Wounds Involving Exposed Bone and Tendon: Case Series and Benchmark Panel
Robert J Snyder, DPM, MBA, MSc, CWSP, FFPM RCPS (Glasgow)1
- Honorary Visiting Professor, Centre for Medical Education, Cardiff University School of Medicine, Cardiff, Wales, UKWCCC, Executive Officer, Board of Directors Master, American Professional Wound Care Association Past President, Association for the Advancement of Wound Care Past President, American Board of Wound Management Associate Editor, Wound Care and Limb Preservation, Journal of the American Podiatric Medical Association Co-Chair, Florida Board of Podiatric MedicineGlobal Clinical Scholars Research Training (2020-2021), Harvard Medical School Fellowship, Bioethics, Harvard Medical School (2025)
OPEN ACCESS
PUBLISHED:30 April 2026
CITATION: Snyder, R., 2026. Three-Dimensional Hepatic Collagen Scaffold for Chronic Wounds Involving Exposed Bone and Tendon: Case Series and Benchmark Panel. Medical Research Archives, [online] 14(4).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Background: Chronic wounds with deep structural involvement (e.g., tendon or bone exposure in advanced diabetic foot ulcers and full-thickness stage IV pressure ulcers) are clinically challenging due to volume deficit, bioburden risk, and barriers to durable granulation and closure when flap coverage is not feasible.
Objectives: To describe outcomes from a locked case-series evidence package using a three-dimensional acellular collagen scaffold (Miro3D, Reprise Biomedical, Plymouth, Minnesota) and to contextualize outcomes against a prespecified comparator benchmark panel of diabetic foot ulcer and stage IV pressure ulcer studies.
Methods: A primary 3D-ACM dataset was standardized using prespecified rules (DFUs required explicit tendon exposure in source text; stage IV pressure ulcers were treated as exposed-structure cases by prespecified rule). Outcomes were extracted descriptively at reported time points, including closure and, when reported, tunneling/undermining milestones. A targeted comparator panel of diabetic foot ulcer and stage IV pressure ulcer studies was assembled for contextual benchmarking at each study’s prespecified primary assessment timepoint.
Results: The locked dataset comprised five exposed-structure cases (two DFU with tendon exposure; three stage IV pressure ulcers). Documented closure occurred in 4/5 cases between Day 42 and ~20 weeks. One stage IV pressure ulcer achieved tunneling resolution by Day 56 but was lost to follow-up prior to reported closure. The comparator panel included six diabetic foot ulcer studies and two pressure ulcer randomized trials with heterogeneous designs, follow-up windows, and endpoint definitions.
Conclusions: In this non-comparative exposed-structure case series, documented closure occurred in most cases with available follow-up, and deep-wound improvement (tunneling resolution) was captured when reported. Findings support prospective evaluation using standardized, time-anchored endpoints in volume-deficit wounds.
Keywords: Diabetic foot ulcer; Pressure injury; Extracellular matrix; Collagen scaffold; Wound healing; Bone exposure.
INTRODUCTION
Chronic cutaneous wounds impose a substantial clinical and economic burden. Pressure injuries alone contribute to meaningful healthcare costs. When chronic wounds involve deep tissue loss or expose supporting structures such as tendon or bone, risks of infection, osteomyelitis, and limb loss rise markedly. Diabetic foot ulcers (DFUs) exemplify this challenge: 15% – 25% of patients with diabetes will develop a DFU over their lifetime, and recurrence is common. DFUs are strongly associated with lower-limb amputation pathways in clinical practice, with ulcers frequently preceding amputation events. Stage IV pressure injuries share many of the same anatomic and biologic barriers to healing when deep structures are involved.
Pathophysiology of Non-healing Exposed Structures
Failure of chronic wounds to heal reflects a sustained pro-inflammatory milieu. Impaired perfusion, repetitive mechanical stress, bacterial biofilm, and excessive protease activity degrade growth factors and extracellular matrix (ECM), derailing normal repair. In deep or volume-deficit wounds, these factors are compounded by structural and geometric barriers to healing. Exposed cortical bone or desiccated tendon lacks a vascular substrate for fibroblast migration and epithelial advancement, trapping the wound in the inflammatory phase. In pressure injuries with full-thickness tissue loss, undermining, tunneling, and irregular wound contours often create dead space that must be managed before durable closure can occur. As a result, clinical decision-making in these wounds is frequently driven not only by surface coverage, but by the ability to support three-dimensional wound bed formation and progression through intermediate milestones such as granulation/coverage and resolution of tunneling or undermining.
Limitations of Current Reconstructive Options
Local or free-flap coverage remains the traditional approach to restore a vascularized soft-tissue envelope over exposed structures. Although durable, flaps require operating room resources, anesthesia, and adequate donor tissue-constraints that many elderly vasculopaths, or medically complex patients cannot meet. Negative pressure wound therapy (NPWT) may stimulate granulation and manage exudate but may be insufficient to bridge exposed bone or tendon without a biologic scaffold. Thin acellular dermal or placental matrices can provide surface protection yet may resorb or delaminate in deep, undermined defects, particularly when stable contact across depth is difficult to maintain.
Evolution of Biologic Scaffolds
Over two decades, dermal/ECM substitutes have progressed from planar collagen scaffolds to diverse constructs used for wound repair and regeneration. While these advances have improved options for wound bed support and closure, many commercially used matrices remain relatively thin and are often deployed as surface-oriented constructs, which can limit their ability to obliterate dead space in cavities or irregular three-dimensional defects. Clinical evidence in DFU populations suggests biologic scaffolds can accelerate healing compared with standard care in selected settings, yet outcomes vary with wound depth, perfusion, bioburden, and offloading. Moreover, across contemporary studies, endpoint definitions and reporting are inconsistent-closure at a timepoint is commonly available, whereas intermediate deep-wound milestones (e.g., coverage/granulation over exposed structures, resolution of tunneling/undermining) are less consistently reported and are often not extractable for cross-study interpretation.
The Three-Dimensional Acellular Wound Matrix Concept
Miro3D (Reprise Biomedical, Plymouth, MN), a three-dimensional acellular collagen matrix (3D-ACM) represents a volumetric, three-dimensional ECM scaffold derived from porcine liver via perfusion decellularization, which removes cells while preserving the organ’s microvascular framework. The resulting non-crosslinked construct is designed for placement in depth and may be layered to fill cavities and manage irregular wound geometries. Prior characterization has described retention of key ECM components (e.g., collagen and associated structural proteins) within an interconnected porous architecture intended to support cellular ingress and integration throughout the defect. The scaffold is pliable, hydrophilic, and fully resorbable, supporting use in wounds where conformability and volumetric contact are practical considerations.
Rationale and Study Aim
For patients in whom flap surgery is not feasible, a deep, conformable scaffold that can support rapid establishment of a vascularized wound bed over exposed tendon or in full-thickness stage IV pressure injuries is clinically attractive. Recent clinical experience has described the use of a three-dimensional acellular collagen matrix in deep or tunnelling DFUs. The present manuscript reports a locked, non-comparative 3D-ACM case-series evidence package focused on a prespecified exposed-structure phenotype (DFUs with explicit tendon exposure; stage IV pressure ulcers by definition) and contextualizes results against a targeted comparator benchmark panel assembled via PRISMA-guided screening of DFU and stage IV pressure-injury studies evaluating alternative matrix-based approaches for wounds with deep structural involvement. Comparator outcomes are presented as contextual benchmarking rather than head-to-head comparative effectiveness, with emphasis on closure at study-specific primary timepoints and on the presence or absence of intermediate deep-wound endpoints when reported.
Methods
Study design and oversight
This manuscript combines (1) a retrospective, descriptive case-series evidence package of wounds treated with a three-dimensional porcine hepatic-derived acellular collagen scaffold (3D-ACM), and (2) a PRISMA-guided selection of a targeted comparator benchmark panel of DFU and pressure-ulcer studies evaluating contemporary matrix-based therapies. The 3D-ACM cases were derived from previously presented clinical materials (e.g., posters, case presentations, and published proceedings) and were synthesized in de-identified form for descriptive reporting consistent with the Declaration of Helsinki. Written consent for clinical photography and public presentation was obtained by treating clinicians per local practice.
Case identification and prespecified eligibility rules (scaffold cohort)
A primary 3D-ACM exposed-structure dataset was standardized and locked using prespecified, conservative criteria designed to minimize inference and maximize extractability:
- Wound type coding: diabetic foot ulcer (DFU) versus pressure ulcer/injury (PU).
- Exposed-structure coding (required for primary set):
- DFU: exposed structure required explicit documentation of exposed tendon in the source text.
- PU: Stage IV pressure ulcer/injury was treated as exposed structure by prespecified coding rule (full-thickness tissue loss with exposed or directly palpable deeper structures).
- No inference rule: Exposed structure was not inferred from images alone; exposure had to be explicitly stated (DFU tendon exposure) or established by Stage IV designation (PU).
- Demographics: restricted to age and sex only for consistency across cases.
Primary set inclusion/exclusion criteria
Included (primary exposed-structure set): cases meeting the prespecified exposed-structure coding rule above (DFU: explicit tendon exposure in source text; Stage IV pressure ulcer: treated as exposed-structure by prespecified rule), with extractable baseline wound descriptors and at least one time-anchored outcome (e.g., closure time, PAR at a specified week, or a clearly stated deep-wound milestone such as tunneling resolution).
Excluded: cases without explicit exposed tendon (DFU) and without Stage IV designation (PU), cases lacking extractable outcomes, and cases where exposure status could only be inferred from photography.
Clinical management and adjunctive care
Because the 3D-ACM evidence package was assembled from clinician-generated source materials, wound bed preparation, dressing selection, and adjunctive therapies reflected routine site practice and were recorded as described in the source documents. Where reported, cases typically included debridement and standard-of-care measures appropriate to wound type (e.g., offloading for plantar DFU; pressure redistribution and shear minimization for PU), with NPWT used in some cases.
Scaffold description
The three-dimensional scaffold is supplied as a sterile, dry, ~2-cm-thick volumetric scaffold produced by perfusion decellularization of porcine liver, leveraging native vascular pathways to preserve three-dimensional microarchitecture within a collagen-rich extracellular matrix. The resulting construct is designed for placement in depth and conformal contact within irregular wound geometries, allowing trimming, packing, or layering to fill cavities or undermined/tunneled defects and maintain apposition to the wound base during healing.
Wound bed preparation, application, and aftercare
Because this evidence package was assembled from clinician-generated source materials (e.g., posters, case presentations, and proceedings), wound preparation, dressing selection, and adjunctive care reflected site practice and were recorded as described in the source documents. Where reported, wounds underwent debridement and standard wound bed preparation prior to 3D-ACM placement. The scaffold was trimmed to wound dimensions and applied to achieve contact with the wound bed; in wounds with depth, undermining, or tunneling, material was placed into the defect to support conformability within the wound geometry. Dressings and adjunctive therapies (including NPWT in some cases) were used per local practice. For diabetic foot ulcers, offloading protocols were incorporated as described; PU cases incorporated pressure redistribution and shear minimization strategies as described in the source materials.
Outcomes and safety endpoints
All analyses were descriptive. Primary extracted outcomes were time-anchored endpoints reported in the source documents, including: (1) time to complete epithelial closure (when reported), recorded in weeks (with days in parentheses when the source reported days); (2) percent area reduction (PAR) at stated timepoints (when available); and (3) explicitly reported deep-wound milestones relevant to volume-deficit wounds (e.g., tunneling/undermining resolution). Safety observations (e.g., infection, operative revision, amputation, or device-related adverse events) were recorded only when explicitly reported in the source documents.
Data collection and measurement
Data was extracted directly from clinician-provided materials, including narrative descriptions and serial measurements when provided. Standardized digital planimetry and a protocol-defined assessment schedule were not mandated. Accordingly, outcomes were summarized as reported, and missing elements were treated as not reported rather than inferred.
Comparator literature benchmark panel (DFU/PU): PRISMA-guided targeted selection
Review question and scope
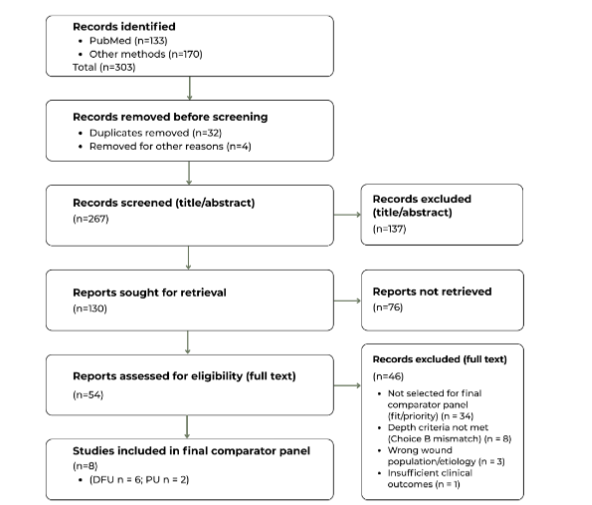
To contextualize outcomes observed in the 3D-ACM case series, a targeted comparator benchmark panel of human clinical studies evaluating matrix-based therapies in complex diabetic foot ulcers (DFU) and advanced pressure ulcers/injuries (PU) was assembled. This workflow was designed to identify a clinically coherent benchmark reference set, not to estimate pooled comparative effectiveness. The panel selection and record disposition are summarized in a PRISMA-shaped Comparator Panel Selection Flow (Figure 1A-B).
Because reconstructive goals and operative techniques differ substantially from lower-extremity and pressure-injury wound management, scalp-only reconstruction series were screened but excluded from benchmarking analyses.
Information sources and search strategy
A targeted comparator search was performed on January 18, 2026, using PubMed and supplementary web-based sources (Google Scholar, Semantic Scholar, and targeted Google Search). Records were compiled into a master library (n = 303), comprising PubMed (n = 133) and other sources (n = 170; Google Search 87, Google Scholar 48, Semantic Scholar 35). Search concepts included diabetic foot ulcer (DFU) and pressure ulcer/stage IV terms combined with depth/exposure terms (tendon/bone exposure, osteomyelitis, tunneling/undermining) and matrix/scaffold terms (ECM, dermal substitute, ADM, collagen matrix, skin substitute, placental membrane), including common spelling and plural variants.
Record management and screening (PRISMA-style flow)
All records identified across sources were consolidated into a master library managed in Excel and then operationalized in AirTable for staged screening and extraction. Duplicates were removed using an exact-title matching approach, retaining the most complete record (e.g., PMID present) as the canonical entry (Deduplication Report). Records then underwent staged screening using prespecified eligibility rules:
- Title/abstract screening to identify human clinical wound studies in DFU and/or PU populations evaluating a matrix/ECM/dermal-substitute class intervention with potentially extractable outcomes.
- Full-text review for the subset prioritized for retrieval and assessment, applying the same clinical frame and confirming extractability of time-anchored outcomes. Uncertain cases and edge conditions were resolved by the corresponding author through re-review against the prespecified eligibility rules and confirmation of extractability of time-anchored outcomes; an explicit not reported (NR) convention was used when key details were absent.
Eligibility framework (benchmark alignment)
Studies were screened for (i) human clinical diabetic foot ulcer and pressure ulcer cohorts, (ii) matrix/scaffold/dermal substitute class interventions, (iii) depth/complexity consistent with the comparator benchmark (Choice B), and (iv) extractable clinical outcomes relevant to wound progress (e.g., closure at a defined timepoint or follow-up, and/or other clinically reported healing endpoints). Because this was a targeted benchmarking panel rather than a comprehensive systematic review, some full-text exclusions reflect panel fit/priority (i.e., comparability and outcome extractability) rather than strict in/out eligibility alone.
Full-text exclusion categories (PRISMA reasons)
Among the 46 excluded full texts, primary reason categories were: not selected for final comparator panel (fit/priority) (n = 34), depth criteria not met (Choice B mismatch) (n = 8), wrong wound population/etiology (n = 3), and insufficient clinical outcomes (n = 1).
Full-text extraction and benchmark panel finalization
Full-text articles retrieved and assessed against the comparator frame were extracted into a standardized grid capturing study design, setting, cohort/unit of analysis, depth-related inclusion language, intervention/comparator arms and adjunctive care, follow-up window, endpoint definitions, and extractable outcomes. From the eligible set, a final benchmark panel of 8 studies was selected to maximize clinical relevance and outcome extractability for contextual comparison, stratified into DFU (n=6) and PU (n=2) subsets (Tables 1 and 2).
Endpoint handling and synthesis approach
Given heterogeneity in study designs, adjunctive therapies, and endpoint definitions, no meta-analysis was performed. Outcomes were summarized descriptively. Closure outcomes were harmonized to weeks as the primary unit, with days reported in parentheses when sources reported outcomes in days. For Tables 1A-B and 2, each study’s primary assessment timepoint was defined as the prespecified primary endpoint assessment timepoint when stated; when not stated, the principal final follow-up assessment timepoint reported in the study was used.
Because the comparator set was assembled as a targeted benchmarking panel (rather than a comprehensive systematic review) and because endpoints and reporting were heterogeneous across designs, a single formal risk-of-bias tool was not applied across all included studies. Study design, endpoint definitions, and key reporting limitations were captured during extraction and are addressed qualitatively in the Discussion.
Statistical considerations
All outcomes are summarized descriptively. No imputation was performed for missing outcome elements; missing items were recorded as not reported. Safety events were recorded only when explicitly reported in the source studies.
Role of the sponsor
Reprise Biomedical provided the 3D-ACM scaffold and supported data collation. The sponsor had no role in patient selection, clinical decision-making, treatment delivery, or outcome assessment at participating sites. The corresponding author had full access to the extracted data and had final responsibility for the decision to submit the manuscript for publication.
Reporting standards
Methods and flow follow PRISMA principles for transparent reporting of identification, screening, eligibility, and inclusion for the targeted comparator benchmarking panel, with a PRISMA-shaped diagram summarizing record disposition and reasons for exclusion.
Results
Study Selection and Comparator Panel
The search identified 303 unique records (133 from PubMed and 170 from supplementary sources). After removal of 32 duplicates and 4 additional records during database reconciliation, 267 titles/abstracts were screened. Of these, 137 were excluded at title/abstract screening and 130 records advanced to full-text retrieval.
Full text was not retrievable for 76 records, leaving 54 full texts assessed for eligibility. From these, 8 studies were selected for the final comparator benchmark panel: 6 DFU comparator studies and 2 PU comparator studies. The remaining 46 full texts were not selected for inclusion in the final benchmark panel; where explicitly recorded, reasons included mismatch to the deep/complex comparator frame, non-target wound population, or insufficient extractable clinical outcomes.
Outcomes in exposed-structure cases
In the locked primary 3D-ACM exposed-structure set (n = 5 cases), two cases were diabetic foot ulcers (DFUs) with explicit exposed tendon documented, and three cases were Stage IV pressure ulcers/injuries (PUs/PIs) meeting deep exposure criteria by definition (full-thickness tissue loss with exposed or directly palpable deeper structures). Complete wound closure was documented in 4/5 cases with available follow-up; one Stage IV PU/PI case achieved a deep-tissue milestone (tunneling resolution), but the patient was lost to follow-up before a closure endpoint was documented. The number of 3D-ACM applications ranged from 2 to 9 across cases.
Among DFU tendon-exposure cases, complete closure was reported at 13 weeks in one case and at approximately 20 weeks in one case. Among Stage IV PU/PI cases with closure outcomes, closure was reported by 6 weeks (42 days) in one case and by approximately 10 weeks (71 days) in one case. In the Stage IV PU/PI case without documented closure, tunneling resolved by 8 weeks (56 days), after which the patient was lost to follow-up. These outcomes are summarized in Table 3.
Across the locked exposed-structure dataset (n = 5), the number of scaffold applications ranged from 2 to 9, with wound bed preparation and adjunctive care reflecting routine practice for each wound type (e.g., debridement and offloading for diabetic foot ulcers; debridement and pressure redistribution for stage IV pressure ulcers), and negative pressure wound therapy used in select cases where reported. Time-anchored outcomes showed documented closure in 4 of 5 cases, ranging from Day 42 to approximately 20 weeks. In diabetic foot ulcer cases with explicit tendon exposure, closure was reported at Week 13 in one case and at approximately 20 weeks in the second case, with interim progress captured by percent area reduction when available. In stage IV pressure ulcer cases, closure was reported by Day 42 following four applications in one case and by Day 71 following two applications in another, with intermediate deep-geometry milestones captured when reported (including tunneling resolution after the first application and undermining resolution by Day 35 in the Day 42 closure case). In the remaining stage IV pressure ulcer case, tunneling resolution was documented by Day 56 after seven applications, but closure could not be confirmed due to loss to follow-up. Collectively, these cases illustrate feasibility of applying a volumetric scaffold within complex wound geometries and tracking time-anchored endpoints that include both closure and clinically meaningful deep-wound milestones when available.
Narrative Case Summaries (Narrative case summaries (locked exposed-structure set; n=5)
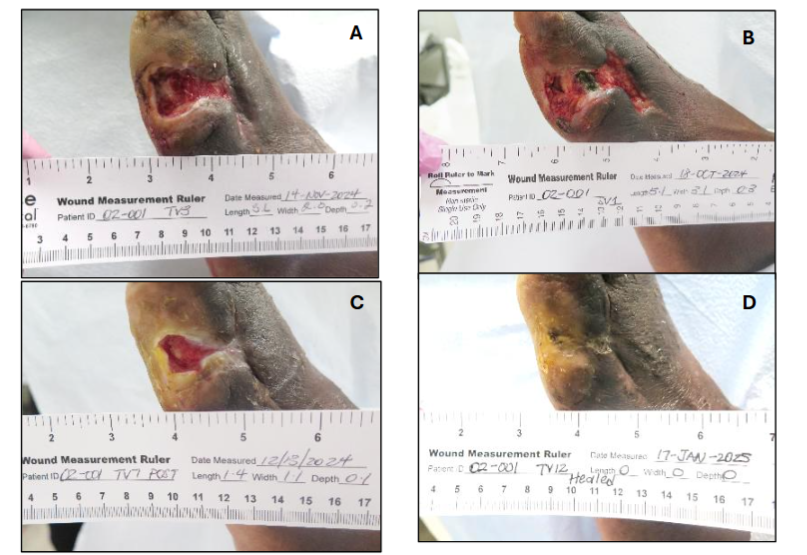
Case 1 (DFU; exposed tendon). A 64-year-old male with a chronic plantar DFU on the left foot (baseline wound area 15.81 cm²) and explicit tendon exposure was treated with serial applications of 3D-ACM after 55 days’ wound duration prior to enrollment. Applications were performed weekly for the first 4 weeks, then biweekly through Week 13, in conjunction with standard dressing changes per protocol and adherence to prescribed offloading. The wound achieved 54.5% percent area reduction (PAR) by Week 4 and 90.3% PAR by Week 8, with wound area reported as 1.5 cm² at Week 8. Complete closure was reported at Week 13.
Case 2 (DFU; exposed tendon). A 60-year-old male with diabetes and neuropathy presented with cellulitis and a right anterior ankle ulcer following prior incision and drainage (I&D) of an abscess with NPWT. The ulcer demonstrated drainage with exposed tibialis anterior tendon and undermining; MRI was consistent with phlegmon/necrotic tissue with likely abscess and infectious tenosynovitis, with no osteomyelitis reported. After repeating operative management, baseline measurements at 3D-ACM initiation were 8.0 × 6.0 × 1.0 cm (area 48 cm², volume 48 cm³) with a ~2.5 cm tunnel (Wagner grade 3). The scaffold was packed into the tunnel and wound bed and managed with NPWT (125 mmHg continuous) and antibiotics. By day 31, integration with a granular base was observed and the wound measured 6.2 × 4.5 × 0.2 cm (approx. area 28 cm², volume 6 cm³; 42% area reduction and ~88% volume reduction). The wound was reported fully closed by day 138 (~19.7 weeks).
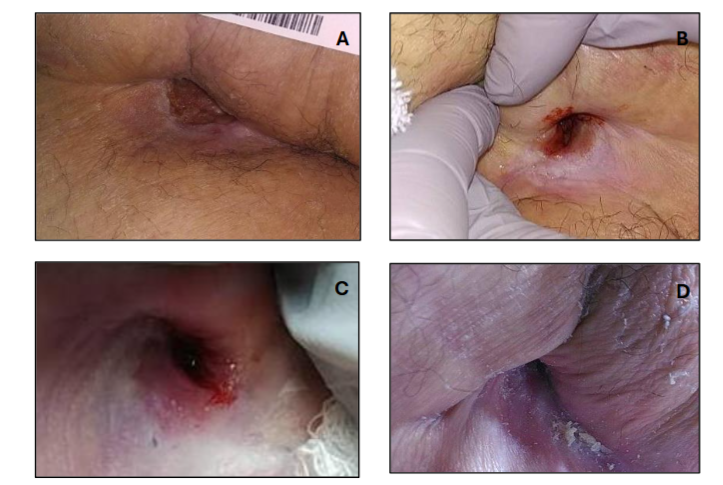
Case 3 (Stage IV PU; by definition). An 82-year-old paraplegic female with a chronic Stage IV sacral pressure ulcer and significant comorbidity burden (including type II diabetes and hypertension) following a prolonged course of standard and advanced wound care. At initial presentation (approximately one year prior to 3D-ACM initiation), the sacral wound measured 4.3 × 3.5 × 0.5 cm; immediately prior to 3D-ACM initiation, it measured 2.4 × 1.7 × 0.5 cm. Baseline undermining was 1.3 cm (10–4 o’clock) with a 1.4 cm tunnel (1 o’clock). The wound received four 3D-ACM applications over approximately four weeks; tunneling resolved after the first application, and the wound was reported fully closed by Day 42 following the fourth application.
Case 4 (Stage IV PU; by definition). A 68-year-old male with multiple sclerosis and impaired mobility presented with a Stage IV sacral pressure ulcer that had persisted for ~7 months despite 13 weeks of on/off NPWT and daily dressing changes, without achieving a ≥50% size reduction. At baseline, the wound measured 3.0 × 2.5 × 1.5 cm with undermining from 6–1 o’clock and extensive tunneling (6.0 cm at 3 o’clock; 7.5 cm at 2 o’clock). Following the first 3D-ACM application, the wound rapidly contracted to 0.6 × 1.1 × 1.0 cm and tunneling/undermining improved (undermining 4.3 cm; tunnel 5.7 cm), consistent with marked early collapse of dead space. A second 3D-ACM application was performed at Day 36, at which time the wound measured 0.5 × 0.5 × 0.5 cm with residual undermining (3.0 cm). The ulcer continued to progress with resolution of undermining/tunneling by Day 57 and was reported fully healed by Day 71 after the first application (two total applications).
Case 5 (Stage IV PU; by definition). In the same patient as Case 3, a concurrent Stage IV right hip/trochanter pressure ulcer developed in the setting of a complicated clinical course that included right hip osteomyelitis and recurrent hospitalizations with antibiotic exposure complicated by C. difficile. At treatment initiation, the hip wound measured 4.3 × 4.1 × 1.0 cm, with a posterior-lateral tunneling tract (1.0 cm) and an undermining ridge (1.5 cm) from 9–3 o’clock. The wound received seven 3D-ACM applications; tunneling was reported resolved by Day 56, with a meaningful decrease in the main wound bed during the treatment period. The patient was subsequently lost to follow-up, and complete closure could not be assessed.
Representative Case Illustrations
To illustrate the range of clinical presentations and progressive tissue responses observed with 3D-ACM, three representative cases are shown with serial photographs depicting baseline appearance, mid-treatment granulation, and complete closure. These examples highlight diverse wound types (outpatient plantar DFU with explicit tendon exposure, Stage IV sacral pressure ulcer with osteomyelitis, and Stage IV sacral pressure ulcer with extensive baseline tunneling/undermining) and demonstrate the scaffold’s versatility across care environments.
Case 1. Plantar DFU with Tendon Exposure
A 64-year-old man with type II diabetes was treated entirely in an outpatient setting for a chronic plantar DFU with exposed tendon. Six sequential 3D-ACM applications were performed every one to two weeks. Granulation and 90% area reduction were achieved by week 8, followed by full closure by week 13. No recurrence occurred through six months of follow-up.

Case 3 – Stage IV sacral pressure ulcer
An 82-year-old paraplegic woman with chronic Stage IV sacral ulceration and a complicated course including right-hip osteomyelitis began treatment with 3D-ACM following prolonged advanced care. At initial presentation (approximately one year prior to 3D-ACM initiation), the sacral wound measured 4.3 × 3.5 × 0.5 cm; immediately prior to 3D-ACM initiation, it measured 2.4 × 1.7 × 0.5 cm. Baseline undermining was 1.3 cm (10–4 o’clock) with a 1.4 cm tunnel (1 o’clock). After serial applications, tunneling resolved after the first application, and the sacral ulcer achieved complete epithelial closure by Day 42 following four 3D-ACM applications; undermining was reported resolved by Day 35.
Case 4. Stage IV sacral pressure ulcer with extensive baseline tunneling/undermining
A 68-year-old male with a Stage IV sacral pressure ulcer present for 7 months (baseline 3.0 × 2.5 × 1.5 cm; undermining 1–6 o’clock; tunnels 6.0 cm [3 o’clock] and 7.5 cm [2 o’clock]) received two 3D-ACM applications with serial measurements documented; the wound was reported resolved/closed by Day 71.
Comparator panel outcomes
Study selection for the comparator benchmarking panel is summarized in Figure 1; the final panel included eight studies (DFU n = 6; PU/PI n = 2) with extractable outcomes for contextual benchmarking. Across DFU studies, prespecified primary assessment windows varied substantially (e.g., 16 weeks, 26 weeks, or longer follow-up), and several single-arm cohorts prioritized granulation/coverage-focused endpoints (time-to-granulation/coverage or granulation by a fixed timepoint) rather than complete closure as the primary endpoint.
| Study (author, year) | Design / setting | Population / depth eligibility | Arms (n) | SOC / adjuncts | Intervention vs control |
|---|---|---|---|---|---|
| Caporusso et al., 2025 (cUC RCT; TTAX01/Neox 1K) | RCT (mixed patients) | DFUs with exposed bone/tendon/muscle/joint capsule; controlled osteomyelitis | 220 | Debridement, dressings, offloading, bone resection, 6-week antibiotics | cUC + SOC vs SOC |
| Dardari et al., 2024 (KereFish/IFSG RCT) | RCT (mixed patients) | UT grade 2 (tendon/capsule) or UT grade 3 (bone/joint); deep DFUs | 255 | Weekly cleansing/debridement, petroleum gauze/foam dressings, offloading, vascular evaluation | Intact fish skin graft + SOC vs SOC |
| Guerriero et al., 2023 (Novasorb BTM cohort) | Prospective single-arm (mixed) | Neuropathic LE wounds; tissue deficit or exposed deeper structures (bone/tendon) | 22 (23 wounds) | Revascularization, debridement, staples/sutures, NPWT 5–7 days, antimicrobials, offloading | BTM (single arm) |
| Cazzell et al., 2017 (DermACELL D-ADM) | Prospective single-arm (mixed) | Wagner 3–4; defect below subcutis with exposure (fascia/ligament/tendon/muscle/bone) | 61 | Debridement, standardized dressings, removable boot offloading; HBO excluded; osteomyelitis treated | D-ADM (single arm) |
| Frykberg et al., 2017 (vCHPM) | Prospective single-arm | Complex DFUs with exposed tendon/bone (per study eligibility) | 31 | Weekly cleansing/debridement, absorptive foam, standardized offloading; no NPWT | vCHPM (single arm) |
| Lullove, 2021 (mHADM + NPWT pilot RCT) | Pilot RCT (inpatient; both arms NPWT) | Wagner ≥2 DFUs; surgery indicated (per study) | 30 | Angiography/angioplasty, debridement incl bone, NPWT both arms, antibiotics | mHADM + NPWT vs NPWT |
| Study (author, year) | Primary endpoint | Closure at primary timepoint (n/N, %) | Key secondary endpoint | Safety |
|---|---|---|---|---|
| Caporusso et al., 2025 (cUC RCT; TTAX01/Neox 1K) | Time (days) to complete healing within 26 weeks (182 days) | 49.2% (58/118) vs 47.1% (48/102) | Median time-to-closure (healed): 106 vs 104 days | Index ulcer complications 11.9% vs 18.6%; amputations 7.6% vs 12.7%. |
| Dardari et al., 2024 (KereFish/IFSG RCT) | % completely closed by 16 weeks | 44.4% (56/126) vs 38.8% (45/116) | RMST to closure (≤24 wks): 17.31 vs 19.37 weeks | Wound infection 30.2% vs 29.3%; AEs most common. |
| Guerriero et al., 2023 (Novasorb BTM cohort) | Complete healing; primary time point 12 months | 64% (14/22) | Median time-to-closure (healed wounds): 126 days | Post-BTM infection 3/23; amputations: 1 minor, 2 major. |
| Cazzell et al., 2017 (DermACELL D-ADM) | Time to 100% granulation/coverage; assessed through 16 weeks | 24.6% (15/61) | Mean time to 100% granulation: ~4.1 weeks (ITT) | Infections 14.8%; amputation 11.1%; no graft-related AEs. |
| Frykberg et al., 2017 (vCHPM) | 100% granulation by 16 weeks | 51.6% (16/31) | 100% granulation by 16 weeks: 83.9% (ITT) | ≥1 AE 59.3%; infections/procedural events; no product-related complications reported. |
| Lullove, 2021 (mHADM + NPWT pilot RCT) | (1) Granulation during 120 days; (2) healing at 6 months | 86.7% (13/15) vs 57.1% (8/14) | Granulation by 120 days: 100% vs 64.3% | One withdrawal (major amputation), one death post-study; recurrence NR. |
Note: For retrospective single-arm cohorts without a prespecified fixed primary timepoint, outcomes are reported as overall healed proportion and/or time-to-healing as provided; subgroup healed n/N may be NR.
Note: Comparator data derived from published clinical studies of acellular matrices in complex wounds with exposed bone or tendon.
Discussion
Building on this contextual benchmarking, the Discussion interprets the case-series findings against the published comparator outcomes while acknowledging key limitations imposed by differences in study design, endpoint definitions, wound depth criteria, and follow-up windows. It interprets outcomes from the locked 3D-ACM exposed-structure case series in the context of a prespecified comparator benchmark panel, emphasizing what can – and cannot – be compared across heterogeneous designs and endpoints. This statement underscores the clinical difficulties of volume-deficit wounds with exposed deep structures and the lack of standardized methods to assess healing beyond closure.
Comparison With Contemporary Matrix-Based Therapies
The comparator panel provides context for how outcomes are reported across commonly used matrix-based therapies in DFU and pressure ulcer populations. Across included DFU studies, reported outcomes at prespecified primary assessment timepoints vary widely, reflecting differences in study design (randomized trials vs. single-arm cohorts), patient selection, wound definitions and depth criteria, standard-of-care protocols, and follow-up duration. In the pressure ulcer comparator studies, closure at the reported assessment timepoints is summarized for benchmarking; in Narayan et al., the prespecified primary endpoint was percent wound area reduction, with closure additionally reported. Importantly, these data are presented as contextual benchmarking rather than comparative effectiveness and should not be interpreted as product-to-product comparisons across dissimilar study designs.
Beyond study-specific closure outcomes at prespecified assessment timepoints, the comparator panel underscores a key limitation of the contemporary evidence base for deep or exposed-structure wounds: endpoints that directly capture progress in volume-deficit wounds – such as time to granulation/coverage over exposed structures, resolution of tunneling/undermining, or standardized documentation of deep-structure involvement – are inconsistently reported. Several DFU studies did not report a distinct granulation/coverage endpoint, and where such endpoints were reported, definitions and reporting conventions differed across studies. As a result, the broader literature often forces interpretation of deep-wound performance primarily through closure metrics, which may under-represent intermediate milestones that matter clinically in exposed-structure wounds.
Clinical and Practical Implications
Variability in how complete closure is defined and confirmed across studies can further limit interpretability when benchmarking outcomes. Because the comparator panel was assembled for contextual benchmarking rather than comparative effectiveness, results should be interpreted as descriptive reference ranges within each study’s design, analysis set, and endpoint definition, not as cross-study estimates of treatment effect. Differences in cohort selection, adjunctive care, follow-up windows, and outcome definitions limit direct comparability even when similar timepoints are reported. Benchmarking can therefore clarify how outcomes are reported across contemporary studies and the magnitude of outcomes observed within each study’s framework, but it cannot establish superiority, equivalence, or causality across interventions. For exposed-structure and volume-deficit wounds, closure status at a single timepoint may not fully reflect clinically meaningful progress that occurs within depth and complex geometry. More consistent reporting of wound geometry and intermediate deep-wound milestones (e.g., granulation/coverage over exposed structures, tunneling/undermining change) alongside time-anchored closure outcomes would improve interpretability and better align published evidence with clinical decision-making.
Exposed-structure wounds are uniquely challenging because they commonly combine dead space (volume deficit), heightened bioburden/infection risk, and barriers to granulation over relatively avascular tissue (e.g., tendon or bone). Clinical management often requires not only infection control, debridement, and optimization of offloading/pressure redistribution, but also strategies that support stable three-dimensional wound bed formation. In this context, a conformable 3D acellular matrix may be clinically useful because it can be placed into irregular geometries, improving scaffold-to-tissue contact within depth and around contours rather than bridging across cavities.
Mechanistic interpretation (background context)
Biologic ECM scaffolds are designed to provide a three-dimensional microenvironment that supports cellular infiltration and constructive remodeling. In preclinical and translational literature, decellularized ECM materials can modulate the wound microenvironment in ways that support angiogenesis and tissue deposition, with host immune and stromal cell interactions playing a central role in remodeling. Perfusion-based decellularization approaches have been used to preserve native tissue architecture while removing cellular components, providing a plausible mechanistic rationale for volumetric scaffold performance in dead-space wounds.
Within the locked primary 3D-ACM exposed-structure set, closure was documented in most cases with available follow-up, and a deep-tissue milestone (tunnel resolution) was captured when closure could not be confirmed due to loss to follow-up. These observations support feasibility of applying a 3D matrix in exposed-structure contexts while tracking clinically meaningful endpoints (closure and, when reported, intermediate deep-wound milestones). However, these outcomes should be interpreted as descriptive clinical experience rather than evidence of comparative effectiveness.
Clinical workflow and patient-centered considerations
Where flap reconstruction is not feasible or is undesirable because of operative burden and comorbidity, an approach that can be delivered within standard wound-care workflows may be valuable. A scaffold that can be trimmed and conformed to wound geometry and used with common adjuncts (e.g., standard dressings and, when indicated, NPWT) may help clinicians manage irregular wound architecture while progressing toward a vascularized wound bed suitable for closure.
Standard pressure ulcer care remains foundational, including pressure redistribution, wound bed preparation, and optimization of contributing factors such as nutrition and infection control.
Economic considerations (hypothesis-generating)
Although this report does not include a cost analysis, chronic wounds and advanced pressure injuries are associated with substantial resource utilization at the system level. Strategies that advance deep wounds toward closure without escalating to operative reconstruction may plausibly influence episode-of-care burden; prospective studies with prespecified economic endpoints are warranted.
Strengths and Limitations
This manuscript intentionally pairs a tightly defined 3D-ACM case series with a comparator panel selected to support contextual benchmarking. A key strength is the focus on a difficult wound phenotype – exposed-structure DFUs and Stage IV pressure ulcers – while applying conservative, prespecified rules for what qualifies as exposed structure (explicit tendon exposure or Stage IV by definition) and restricting reporting to extractable, time-anchored outcomes.
Several limitations constrain inference. First, the 3D-ACM dataset is a small, non-randomized case series and is subject to selection bias, variation in adjunctive care across cases, and incomplete follow-up in at least one case; it cannot estimate treatment effect or support product-to-product comparisons. Second, the comparator panel includes heterogeneous designs (RCTs and single-arm studies), follow-up durations, and endpoint definitions, limiting comparability. Third, comparator reporting of deep-wound milestones (granulation/coverage, tunneling/undermining resolution, explicit deep-structure outcomes) is inconsistent, restricting interpretation primarily to closure rates at study-specific timepoints. Finally, benchmark panel selection was restricted to studies meeting prespecified criteria for DFU and pressure ulcer comparators and designed to anchor interpretation to extractable outcomes; therefore, benchmark outcomes should be interpreted as descriptive context rather than a comprehensive synthesis of all evidence.
Future directions
Future prospective evaluations should focus specifically on exposed-structure wounds using standardized definitions of exposure (tendon vs bone vs fascia; Stage IV pressure injury) and consistent reporting of deep-wound geometry (depth, tunneling, undermining) and intermediate milestones (time to granulation/coverage over exposed structures; tunnel/undermining resolution). Controlled studies or registries that combine these milestones with closure at prespecified timepoints and durability of closure would improve external validity and allow more clinically meaningful comparisons across matrix-based approaches. In parallel, harmonizing endpoint definitions and reporting conventions across trials would strengthen interpretability and reduce reliance on closure-only outcomes to judge performance in volume-deficit wounds.
Conclusion
In this multicenter case series of complex wounds with exposed deep structures (explicit tendon exposure in DFUs and Stage IV pressure ulcers by definition), 3D-ACM was used as a volumetric ECM scaffold within standard wound-care workflows and was associated with documented closure in most cases with available follow-up and with meaningful deep-wound improvement in a case lacking closure follow-up. When contextualized against a prespecified comparator benchmark panel, these observations support feasibility of a 3D conformable matrix approach for volume-deficit wounds while underscoring major evidence limitations in the literature, including heterogeneous designs and inconsistent reporting of deep-wound milestones. Prospective studies using standardized exposure definitions and consistent reporting of coverage/granulation and tunneling/undermining resolution alongside closure endpoints are warranted.
Acknowledgements
The author thanks the participating clinicians and wound care teams for their contributions to patient care and for providing de-identified clinical materials used in this report.
Funding
Reprise Biomedical provided the 3D-ACM scaffold and supported data collation. The sponsor had no role in clinical decision-making, outcome assessment/adjudication, or the decision to submit the manuscript.
Conflicts of interest
R.J.S. serves as a consultant to Reprise Biomedical.
Ethics and consent
This manuscript reports de-identified data compiled from clinician-generated materials (e.g., posters, case presentations, and proceedings) and does not include direct patient identifiers. Clinical photography and public presentation consent were obtained by treating clinicians per local practice where applicable. Where required, ethics/IRB review was handled according to local site policies for retrospective, de-identified case reporting.
Author contributions
The author contributed to study conception and design, data collation and extraction, interpretation of findings, and manuscript drafting and revision, and approved the final version for submission.
Data availability
The datasets generated and/or analyzed during this study are not publicly available because they are derived from de-identified clinician-generated source materials. Aggregated data supporting the findings are available from the corresponding author upon reasonable request.
Role of the sponsor
Reprise Biomedical provided the 3D-ACM scaffold and supported collation of de-identified source materials. The sponsor had no role in clinical decision-making at participating sites. The corresponding author had full access to the extracted data and final responsibility for the decision to submit.
References
- Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care (New Rochelle). 2021;10(11):281-292.
- Padula WV, et al. The economic burden of pressure injuries. Int Wound J. 2019;16(1):201-207.
- Senneville É, Albalawi Z, van Asten SA, et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab Res Rev. 2024;40(3):e3687. doi:10.1002/dmrr.3687.
- Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367-2375.
- Zenn MR, Jones G. Reconstructive Surgery: Anatomy, Technique, and Clinical Applications. Elsevier; 2018.
- Wu S, et al. Best practice for wound repair and regeneration: use of cellular, acellular and matrix-like products. J Wound Care. 2023;32(4 Suppl B):S1-S32.
- Badylak SF. The extracellular matrix as a biologic scaffold material. Biomaterials. 2007;28(25):3587-3593.
- Costa A, Naranjo JD, Londono R, Badylak SF. Biologic scaffolds. Cold Spring Harb Perspect Med. 2017;7(9):a025676.
- Driver VR, et al. A prospective multicenter randomized controlled trial of Integra Dermal Regeneration Template for diabetic foot ulcers. Wound Repair Regen. 2015;23(6):891-900.
- Turner NJ, Badylak SF. The use of biologic scaffolds in the treatment of chronic non-healing wounds. Adv Wound Care (New Rochelle). 2015;4(8):490-500.
- Ott HC, et al. Perfusion-decellularized matrix: using nature’s platform to engineer a bioartificial heart. Nat Med. 2008;14(2):213-221.
- Abdo RJ, Couch AL. Use of three-dimensional acellular collagen matrix in deep or tunnelling diabetic foot ulcers. J Wound Care. 2024;33(9 Suppl):S1-S12.
- Li Y, et al. Reconstruction of lower-extremity wounds with exposed bones and tendons using acellular dermal matrices. BMC Surg. 2022;22:249.
- Simman R, et al. Managing wounds with exposed bone and tendon using esterified hyaluronic acid matrix. Plast Reconstr Surg Glob Open. 2018;6(7):e1848.
- Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel pressure injury staging system: revised pressure injury staging system. J Wound Ostomy Continence Nurs. 2016;43(6):585-597. doi:10.1097/WON.0000000000000281.
- Frykberg RG, Gibbons GW, Walters JL, Wukich DK, Milstein FC. A prospective, multicentre, open-label, single-arm clinical trial for treatment of chronic complex diabetic foot wounds with exposed tendon and/or bone: positive clinical outcomes of viable cryopreserved human placental membrane. Int Wound J. 2017;14:569-577. doi:10.1111/iwj.12649.
- Dardari D, Piaggesi A, Potier L, et al. Intact fish skin graft to treat deep diabetic foot ulcers. NEJM Evid. 2024;3(12). doi:10.1056/EVIDoa2400171.
- Caporusso J, Motley T, Lantis JC II, et al. A multi-centre, randomised, controlled clinical trial assessing cryopreserved ultra-thick human amniotic membrane in the treatment of complex diabetic foot ulcers. Wound Repair Regen. 2025;33:e70110. doi:10.1111/wrr.70110.
- Lullove E. Acellular fetal bovine dermal matrix in the treatment of nonhealing wounds in patients with complex comorbidities. J Am Podiatr Med Assoc. 2012;102(3):233-239.
- Cazzell S, Moyer PM, Samsell B, Dorsch K, McLean J, Moore MA. A prospective, multicenter, single-arm clinical trial for treatment of complex diabetic foot ulcers with deep exposure using acellular dermal matrix. Adv Skin Wound Care. 2019;32:409-415.
- Guerriero FP, Clark RA, Miller M, Delaney CL. Overcoming barriers to wound healing in a neuropathic and neuro-ischaemic diabetic foot cohort using a novel bilayer biodegradable synthetic matrix. Biomedicines. 2023;11:721. doi:10.3390/biomedicines11030721.
- Brown-Etris M, Milne CT, Hodde JP. An extracellular matrix graft (Oasis® wound matrix) for treating full-thickness pressure ulcers: a randomized clinical trial. J Tissue Viability. 2019;28:21-26. doi:10.1016/j.jtv.2018.11.001.
- Narayan N, Ramegowda YH, Raghupathi DS, Chethan S, Gowda S. Biological skin substitutes in pressure ulcers: high-purity type I collagen-based versus amnion/chorion membrane. Cureus. 2025;17(8):e90956. doi:10.7759/cureus.90956.
- Snyder RJ, Swartz M. Use of a three-dimensional acellular collagen matrix to treat a chronic diabetic foot ulcer with tendon exposure: a case study. Poster presented at: Symposium on Advanced Wound Care (SAWC) Spring; March 2025.
- Methodius WR. Treatment of stage IV pressure ulcers using a three-dimensional acellular collagen wound matrix: case series. Poster presented at: Symposium on Advanced Wound Care (SAWC) Spring; April 2024.
- Roberts KM. 3-dimensional wound matrix for complex pressure ulcers: a case series analysis. Poster presented at: Symposium on Advanced Wound Care (SAWC) Fall; September 2024.
- Gould L, Li WW. Defining complete wound closure: closing the gap in clinical trials and practice. Wound Repair Regen. 2019;27(3):201-224. doi:10.1111/wrr.12707.
- Gould LJ, Alderden J, Aslam R, et al. WHS guidelines for the treatment of pressure ulcers – 2023 update. Wound Repair Regen. 2024;32(1):6-33. doi:10.1111/wrr.13130.