






Mental Health in Nurses: Impact of Work Stressors
Anxiety, Depression and Stress in Nurses in Relation to Some Parameters Related to the Profession
Ina Stašević ¹, Lidija Vincelj ², Darko Ropac ³
Methods: The study was conducted at the Sestre milosrdnice Universitiy Hospital Center. The study involved 254 participants. Anonymous survey questionnaire, created solely for the purposes of this research, and validated Depression, Anxiety and Stress Scale -DASS-21 were used as research instruments.
Results: The majority of participants did not show symptoms of depression, anxiety, and stress, while most of participants with present symptoms showed mild to moderate symptoms. A serious and extremely serious level of symptoms was rare. The incidence of symptoms of depression, anxiety and stress were 30.2%, 34.9% and 30.8%. There was a significant difference in the presence of anxiety and stress symptoms in regard to the clinic in which the participants work, and in the presence of anxiety symptoms in regard to the workplace. The most anxiety and stress symptoms were reported by participants that work in cardiology, surgery, and hospital emergency department, and the most-anxious workplace was the operating room. No significant difference was found in regard to gender, age, educational level, years of service and working hours of the participants.
Conclusion: Although the majority of participants does not show any symptoms, the incidence of depression, anxiety, and stress that is present in more than a quarter of respondents is relatively high. The study found that some workplaces expose nurses to more stressful situations. Therefore, it is necessary to emphasize the importance of maintaining mental health of nurses.
Keywords: mental health, nurses, depression, anxiety, stress
INTRODUCTION
Health in general, including mental health as a special but no less important aspect of overall health, certainly represents the most important value and wealth of every individual and society as a whole. It constitutes an important prerequisite and an important determinant of the quality of life. It is increasingly recognized that mental health represents a source of strength and security and is viewed as an important resource.1 Therefore, the promotion and improvement of mental health, raising awareness of the importance of investing all available resources in prevention, early detection, treatment and rehabilitation, and the destigmatization of mental disorders are of great interest, because only such an approach enables good mental health, which is in the interest of society as a whole.
Professional helpers, including nurses, play an important role in preserving and caring for mental health. In order to be able to provide adequate care and compassionate care to their users, it is essential that they themselves are in good mental health. When we consider the fact that nurses are exposed to numerous sources of professional stress and challenges that often exceed their capabilities in their daily work, it is quite clear that their mental health can be significantly jeopardized and impaired when working with people who need their help.2
Numerous studies to date indicate that nurses are not immune to mental health problems. The incidence of mental health problems in healthcare professionals is higher than in the general population. Although research on this topic has increased, proving that there are numerous factors that can negatively affect mental health, additional research is needed.3
Mental health, as defined by the World Health Organization (WHO), is a state of well-being in which the individual realizes his or her personal abilities, can cope successfully with and resolve the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to the community in which he or she lives. All recent European Union documents dealing with mental health issues highlight mental health as an important factor in the social and economic development of every society.4
From the above definition, it is possible to conclude that mental health implies the ability of every individual to cope successfully with everyday and normal stress and life difficulties, and to successfully solve problems. It also implies positive aspects of health, such as the realization of personal potential, productive activity, and contribution to the community, which emphasizes a holistic approach to human health. Mental health, thus accepted, is viewed as a general, public good, and a fundamental right of every human being.4 Such a definition of mental health is being given increasing importance, with the established understanding of mental health, which most often referred to mental disorders, being directed towards good (positive) mental health. Good (positive) mental health stands out as an important resource. It represents an important element of general well-being as well as the ability of each individual to perceive, understand and adapt to the environment and also to change it if necessary. Healthy mental abilities and functions provide us with the ability to perceive life as valuable and enable the creativity and productivity of members of society.5
Mental health problems refer to mental health problems, symptoms and disorders.6 Mental health problems are an increasingly common reason for people to seek help, and they usually occur during periods of high stress or negative events.1 The WHO states that mental health problems and disorders are one of the most important public health challenges and priorities, both globally and in the European Union. As such, they are the leading cause of disability and the third leading cause of the total burden of disease, after cardiovascular disease and cancer. The most common mental disorders in the general population are depression and anxiety disorders.7
WHO data are not encouraging at all, stating that almost half of the world’s population will suffer from some kind of mental illness at some point in their lives, while also pointing out that almost 10% of the population suffers from depression annually, and another 2.6% from psychotic disorders, with anxiety also being a major problem.1 Data for Croatia ranks the group of mental disorders in terms of the number of days of hospital treatment used in Croatia, with a share of 17.2% in the total number of days of hospital treatment. This actually shows that in Croatia every sixth day of hospital treatment was related to some kind of mental disorder.8
A number of factors influence an individual’s mental health and well-being. From genetic and personal factors, such as previous life experiences or stress coping skills, to social and economic circumstances and changes.9 Psychosocial factors related to the workplace also have an important impact on an individual’s mental health and well-being, which have recently received increasing attention.1 This is not surprising given the fact that most of the poor indicators of mental health problems and disorders relate to working individuals. Working individuals spend a large part of their day at their workplaces, performing work that largely defines them. They often spend more time at their workplaces than with their families. Work and the specifics of the workplace greatly affect an individual’s health, both physical and mental.10
If the workplace is characterized by positive elements that create a quality and safe work environment that provides support and enables quality performance of work tasks and at the same time the realization of one’s own potential, the possibility of participating in decision-making and quality communication, then the workplace has a positive effect and contribution to the mental health of employees. On the other hand, a workplace that is characterized by an unsupportive organizational culture is marked by numerous psychosocial hazards such as inappropriate expectations of the employer and excessive workload, frequent overtime hours that are not adequately paid, poor interpersonal relationships and inadequate communication, are just some of the numerous risk factors that have a negative effect on the mental health of employees.11
The consequences of poor mental health related to the workplace affect not only the employee and their family, but also have numerous consequences for the employer and the work organization. Poor mental health has a huge impact on a large number of temporary incapacity for work, absences from work and, consequently, early retirement. The Guidelines for the Implementation of a Comprehensive Approach issued by the European Commission state that the total productivity costs of absenteeism due to mental illness are estimated at €136 billion, of which €99 billion are related to depression and anxiety disorders.1
The healthcare profession as a helping profession has long been recognized as one of the most stressful.12 The largest number of employees in the healthcare system are nurses. They are an indispensable component of every healthcare system. The role of nurses in the healthcare system is of indescribable importance. In addition to providing care and assistance to patients, they participate in their rehabilitation, provide support to them and their families, and play an important role in promoting and preserving the health of the entire population. The demands for healthcare provision are increasing every day. Therefore, nurses are expected to follow modern trends, constantly acquire new knowledge and skills, and take on more and more responsibilities.
Nurses often struggle with difficult situations that are a source of stress in their professional work.13 Nursing is a job with great responsibility, and at the same time it is one of the most difficult professions, because it is associated with saving human health and life and often involves overcoming one’s own weaknesses. Nursing can be a source of inspiration, but it can also be a great burden.12 Nurses work in an environment and circumstances that are constantly changing. Increased life expectancy, the growth of the elderly population brings with it an increase in the number of patients. On the other hand, the insufficient number of staff that health systems in many countries face, long working hours, shift and night work that is characteristic of nursing, lack of professional support, can lead to reduced productivity and affect motivation and professional functioning.14 Such circumstances can affect job dissatisfaction due to the inability to provide satisfactory care and assistance to patients and be the cause of increased stress and possible impaired mental health of nurses.15
Nursing is an emotionally demanding profession and lack of mental well-being, along with common mental disorders, is associated with reduced productivity and absenteeism.16 A nurse is expected to be an emotionally mature and stable person who is able to deal with numerous ethical dilemmas, and to face the pain and suffering of others on a daily basis.
Nurses are indispensable to the health system and their mental health and well-being are of paramount importance as they significantly affect professional performance and the quality of care and healthcare provided.17 When nurses have good physical and mental status, they are more likely to make fewer mistakes at work, and their work motivation increases.18 However, health workers are more focused on improving the care they provide to patients than on taking care of their own health, especially in relation to occupational risks and mental health.19
Research shows that the demanding nature of their profession puts nurses at greater risk of developing depression, anxiety, and stress. Previous studies have shown that the constant stress they face can have negative effects on their psychological well-being. Poor mental health among healthcare providers can also interfere with their professional work and significantly impact the quality of care they provide to patients.20 Poor mental health can lead to a decrease in cognitive functions such as an individual’s ability to concentrate and process information, which can result in inadequate work performance, which can consequently endanger human lives and increase the risk of adverse medical events.20 The workplace and work process expose nurses to occupational risks, which can cause high levels of stress in the work process, reducing nurses’ productivity and quality of life.19 Mental health, occupational health and the work process are interconnected and can affect each other in a positive or negative way.21 Therefore, an environment that promotes good organization of the work process as well as appropriate relationships and communication between employees can contribute to preserving the mental health of employees.
Aim
The objective of this study is to determine the existence of negative emotional states (depression, anxiety, stress) in nurses, and the influence of sociodemographic and job-related variables (level of education, length of service, working hours, job position) on the occurrence of certain emotional states.
Participants And Methods
ETHICS
Written approval was obtained for the purposes of the study from the Ethics Committee of the Sestre milosrdnice University Hospital Center. Through informed consent, all respondents were thoroughly informed about the topic and purpose of the study and the fact that participation in the study was completely anonymous and voluntary. The study was conducted in accordance with the principles of good clinical practice, ethical principles and human rights.
RESEARCH DESIGN
The research was conducted as a cross-sectional study at the Sestre milosrdnice University Hospital Center (Zagreb/Croatia) at the Clinic for Internal Medicine, Clinic for Cardiovascular Diseases, Emergency Hospital Admissions, Clinic for Surgery, and Clinic for Psychiatry. The research was conducted over the past year.
PARTICIPANTS
Participants included in the study were nurses employed in one of the hospital departments. Inclusion criteria were nurses of all levels of education who voluntarily agreed to be interviewed. The survey questionnaires were completed by the participants in the presence of the researcher who could clarify any ambiguities. Exclusion criteria were incomplete and incorrectly completed questionnaires. A total of 254 participants met the inclusion criteria.
QUESTIONNAIRES AND RESEARCH INSTRUMENTS
An anonymous survey consisting of two questionnaires was used as the research instrument. The first part of the anonymous survey consisted of a Survey Questionnaire, which is the author’s work of the researcher and was developed exclusively for the needs of this research (Appendix). It consists of six questions relating to general sociodemographic data and work-related data (gender, age, level of education, years of work experience, working hours and job position).
The second part consisted of the validated questionnaire The Depression Anxiety Stress Scale-DASS-21.22 The scale is a self-assessment measure that examines the frequency and severity of negative emotional states of depression, anxiety and stress. The DASS-21 scale has proven to be a psychometric instrument with high internal reliability and validity.
STATISTICAL PROCEDURES
The results on the depression, anxiety and stress scales were expressed as qualitative data (categories of symptom severity) and as quantitative data (average score on the scale). All collected data were presented using descriptive statistics. Data expressed on the nominal scale were presented as absolute and relative frequencies and presented using arithmetic mean, standard deviation and minimum and maximum values. The chi-square test was used to compare the severity of symptoms on the depression, anxiety and stress scales with respect to age, gender, education, experience, clinic, workplace and working hours. The level of statistical significance was p<0.05. The SPSS Statistic program (version 20, IBM) was used for statistical analysis.
Results
A total of 254 respondents – nurses – participated in the study. Of the total number of respondents who participated in the study, 214 (84.3%) were female, while 40 (15.7%) were male. The average age of the respondents was 38 years. The youngest respondent included in the study was 19 years old, and the oldest was 64 years old. The majority of respondents included in the study had a secondary vocational education, or completed secondary medical school (52.2%). The remaining respondents had a university degree, of which 36.4% had completed an undergraduate professional/university study, while 11.5% of respondents had completed a graduate professional/university study in nursing.
The distribution of respondents according to the clinics in which they work is shown in Table 1. The majority of them were from the Clinic for Internal Medicine (38.6%).
| CLINIC | N | % |
|---|---|---|
| Internal | 98 | 38.6 |
| Cardiology | 60 | 23.6 |
| Surgery | 31 | 12.2 |
| HED | 32 | 12.6 |
| Psychiatry | 33 | 13.0 |
| SUMMA | 254 | 100.0 |
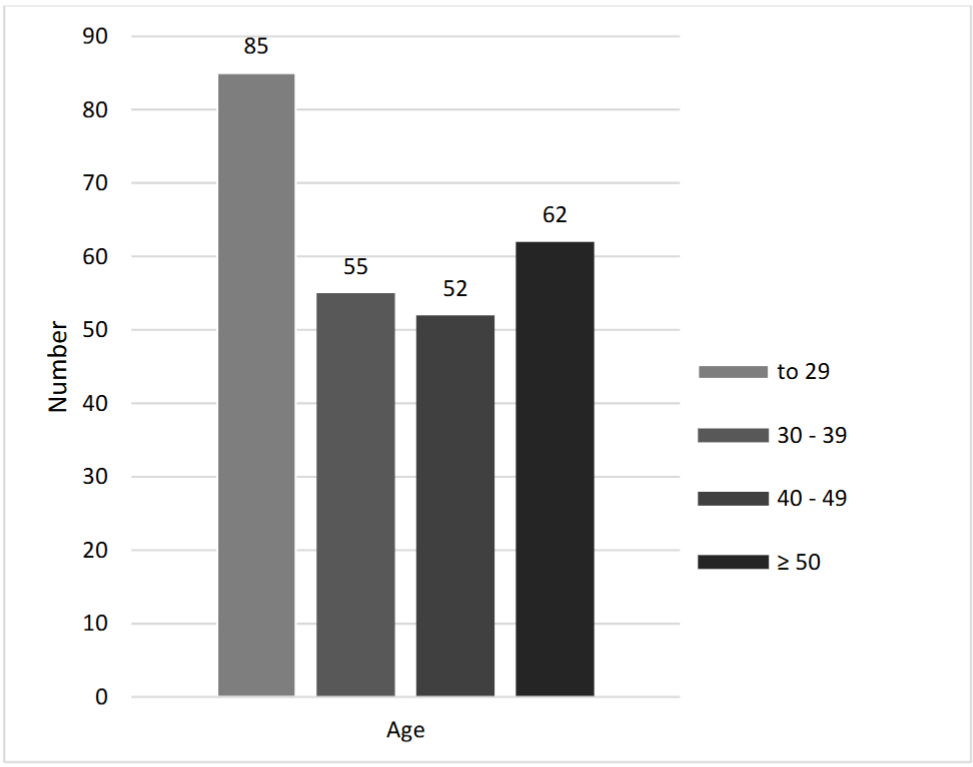
The largest proportion of respondents (33.5%) is under 30 years of age, while the proportion of other age groups is equal (30 – 39 = 21.7%; 40 – 49 = 20.5%; and ≥ 50 years = 24.4%) (Graph 1).
The majority of those included in the survey have less than 10 years of work experience (37.9%). The average length of service of the respondents is 17.5 years. The shortest length of service is six months, while the longest is 45 years. The length of service of the respondents is shown in Table 2.
| Work experience | N | % |
|---|---|---|
| ≤ 9 years | 96 | 37.9 |
| 10 – 19 years | 44 | 17.4 |
| 20 – 29 years | 51 | 20.2 |
| ≥ 30 years | 62 | 24.5 |
The majority of respondents, 48.8% of them, work in one of the hospital departments, while 20.9% work in an outpatient clinic, 12.6% work in an emergency room, and 9.8% work in an intensive or coronary unit. The smallest number of respondents (7.9%) works in the operating room. Most of them (57.9%) work in the “turnus” (12-24-12-48), followed by those who work only in the morning shift (30.3%). The result is shown in Table 3.
| WORKING HOURS | N | % |
|---|---|---|
| Only in the morning shift | 77 | 30.3 |
| In two shifts (morning and afternoon) | 9 | 3.5 |
| In three shifts (morning, afternoon, night) | 1 | 0.4 |
| “Turnus” (12-24-12-48) | 147 | 57.9 |
| Morning shift + on-call or standby | 20 | 7.9 |
The average values of the depression, anxiety and stress scales are shown in Table 4. The respondents, on average, achieved the highest score on the stress scale (M=11.30; SD=8.91), while they achieved the lowest score on the anxiety scale (M=6.71; SD=8.07).
| DASS-21 | N | AM | SD | Min | Max |
|---|---|---|---|---|---|
| Depressiveness | 248 | 7.24 | 8.79 | 0 | 42 |
| Anxiety | 252 | 6.71 | 8.07 | 0 | 42 |
| Stress | 249 | 11.30 | 8.91 | 0 | 42 |
The data in Table 5 show the distribution of respondents according to the severity of symptoms of depression, anxiety and stress. On each of the three scales, the largest number of respondents showed a normal level, i.e. no symptoms (depression – 69.8%, anxiety – 65.1%, stress – 69.1%). Of the respondents with an elevated result on individual scales (depression-30.2%, anxiety-34.9%, stress-30.8%), the majority showed mild to moderate symptoms. The smallest number of respondents showed serious and extremely serious levels of symptoms. Extremely serious symptoms were recorded most often on the anxiety scale (9.1%).
| DASS-21 | SEVERITY OF SYMPTOMS | N | % |
|---|---|---|---|
| Depressiveness | No symptoms | 173 | 69.8 |
| Mild | 25 | 10.1 | |
| Moderately | 30 | 12.1 | |
| Serious | 7 | 2.8 | |
| Extremely serious | 13 | 5.2 | |
| Anxiety | No symptoms | 164 | 65.1 |
| Mild | 19 | 7.5 | |
| Moderately | 36 | 14.3 | |
| Serious | 10 | 4.0 | |
| Extremely serious | 23 | 9.1 | |
| Stress | No symptoms | 172 | 69.1 |
| Mild | 29 | 11.6 | |
| Moderately | 28 | 11.2 | |
| Serious | 15 | 6.0 | |
| Extremely serious | 5 | 2.0 |
Statistically significant difference in the presence of anxiety symptoms (χ2=14.590; p=.008) and stress (χ2=9.877; p=.043) among the respondents with respect to the clinic in which they work is shown in Table 6. Among the respondents working in cardiology, surgery and on depression, anxiety and stress scales – HED, there is a higher proportion of those with present symptoms of anxiety and stress than among the respondents working in internal medicine and psychiatry. Among the respondents working in cardiology, there is the largest number of those with present symptoms of anxiety and stress.
| DASS-21 | Presence of symptoms | CLINIC | χ2 | p |
|---|---|---|---|---|
| Internal (n=95) | NO | 73.7% | 5.562 | 0.234 |
| YES | 26.3% | |||
| Cardiology (n=60) | NO | 58.3% | ||
| YES | 41.7% | |||
| Surgery (n=31) | NO | 67.7% | ||
| YES | 32.3% | |||
| HED (n=32) | NO | 75.0% | ||
| YES | 25.0% | |||
| Psychiatry (n=30) | NO | 76.7% | ||
| YES | 23.3% |
Also, the data show that there is no statistically significant difference in the presence of depressive symptoms among the respondents (χ2=5.562; p=.234) with respect to the clinic in which they work. Among the respondents working in different clinics, the same number of those who have present depressive symptoms is found. Although there is no statistically significant difference, the largest number of respondents who have present depressive symptoms was also recorded among the respondents working in the Cardiology Clinic (41.7%).
Further statistical analysis revealed that among the respondents with symptoms, there was no statistically significant difference in the severity of depression (χ2=10.464; p=0.575), anxiety (χ2=6.231; p=0.904) and stress (χ2=11.950; p=0.450) depending on the clinic they worked in. Among the respondents working in different clinics, there was an equal number of those who reported different levels of severity of depression, anxiety and stress symptoms.
Likewise, there was no significant difference in the severity of depression (χ2=2.685; p=.612), anxiety (χ2=2.007; p=.735) and stress (χ2=4.427; p=.351) among the respondents based on gender. Among men and women, there was an equal number of those who reported different levels of severity of depression, anxiety and stress symptoms.
The results show that there is no significant difference in the severity of symptoms of depression (χ2=13.140; p=.359), anxiety (χ2=6.073; p=.912) and stress (χ2=9.071; p=.697) among the respondents with regard to their age. Among the respondents of different age groups, there is an equal number of those who show different levels of severity of symptoms of depression, anxiety and stress. Among them, the majority show mild to moderate symptoms in all three scales. Extremely serious symptoms were recorded most on the anxiety scale (12.7%) in the age group of respondents 30-39 years.
The same results were obtained with regard to the level of education of the respondents. There is no significant difference in the severity of symptoms of depression (χ2=5.876; p=0.661), anxiety (χ2=7.385; p=0.496) and stress (χ2=6.893; p=0.548) among respondents with respect to their level of education. Among respondents with different levels of education, an equal number of those report varying levels of severity of symptoms of depression, anxiety and stress, with symptoms most often being mild to moderate in all three educational categories.
No significant difference was found in the severity of symptoms of depression (χ2=7.778; p=0.802), anxiety (χ2=6.679; p=0.878) and stress (χ2=9.311; p=0.678) among the respondents with respect to the length of service. Among the respondents showing symptoms, the highest proportion was recorded in the category of respondents with 30 and more years of service on the depression scale (38.3%), while in the category of respondents with up to nine years of service, the highest proportion of respondents (38.5%) showed symptoms mostly on the anxiety scale.
There is no significant difference in the severity of symptoms of depression (χ2=11.832; p=0.459), anxiety (χ2=19.758; p=0.072) and stress (χ2=10.101; p=0.607) among the respondents nor with respect to the organization of their working hours. The highest proportion of respondents showing extremely severe anxiety symptoms (22.2%) was recorded among respondents working two shifts (morning and afternoon).
| DASS-21 | Presence of symptoms | WORK PLACE | χ2 | p |
|---|---|---|---|---|
| 1 (n=51) | NO | 64.7% | 5.057 | 0.282 |
| YES | 35.3% | |||
| 2 (n=121) | NO | 67.8% | ||
| YES | 32.2% | |||
| 3 (n=20) | NO | 65.0% | ||
| YES | 35.0% | |||
| 4 (n=24) | NO | 87.5% | ||
| YES | 12.5% | |||
| 5 (n=32) | NO | 75.0% | ||
| YES | 25.0% |
The data in Table 7 show that there is a significant difference among respondents in the presence of anxiety symptoms (χ2=12.551; p=0.014) with regard to their workplace. Symptoms of anxiety are most common among respondents who work in the operating room (60.0%), while they are the least common among respondents who work in intensive care or coronary care units (12.0%). On the other hand, there is no significant difference among respondents in the presence of symptoms of depression (χ2=5.057; p=0.282) and stress (χ2=3.426; p=0.489) with regard to their workplace, although the highest proportion of respondents with symptoms of stress was recorded among those who work in the operating room (45.0%).
Among respondents with present symptoms of depression, there is a statistically significant difference in the severity of these symptoms (χ2=21.51; p=0.039) with respect to the workplace of the respondents (Table 8). Among respondents working in the outpatient clinic (polyclinic section), there is a greater number of those who have extremely serious symptoms of depression, compared to respondents working in other workplaces, while among respondents working in the intensive care unit, there is a greater number of those who have serious symptoms of depression.
| DASS-21 | Severity of symptoms | WORK PLACE | χ2 | p |
|---|---|---|---|---|
| 1 (n=18) | Mild | 27.8% | 21.851 | 0.039 |
| Moderate | 33.3% | |||
| Serious | – | |||
| Extremely serious | 38.9% | |||
| 2 (n=39) | Mild | 38.5% | ||
| Moderate | 41.0% | |||
| Serious | 10.3% | |||
| Extremely serious | 10.3% | |||
| 3 (n=7) | Mild | 28.6% | ||
| Moderate | 42.9% | |||
| Serious | 14.3% | |||
| Extremely serious | – | |||
| 4 (n=3) | Mild | 37.5% | ||
| Moderate | 33.3% | |||
| Serious | 66.7% | |||
| Extremely serious | – | |||
| 5 (n=8) | Mild | 45.5% | ||
| Moderate | 45.5% | |||
| Serious | – | |||
| Extremely serious | 9.1% |
Discussion
The study examined the frequency and severity of negative emotional states (depression, anxiety, and stress) among nurses in five different clinics, and the influence of sociodemographic and job-related variables (gender, age, level of education, years of service, working hours, and job position) on the severity of negative emotional states.
The results of the study show that the respondents, on average, achieved the highest score on the stress scale, while they achieved the lowest score on the anxiety scale. The distribution of respondents according to the severity of symptoms of depression, anxiety and stress shows that the largest number of respondents is in the category of no symptoms, while the majority of respondents who have an elevated score on certain scales show mild to moderate symptoms. Serious and extremely serious levels of symptoms are reported by the smallest number of respondents, and extremely serious symptoms are recorded most often on the anxiety scale. No significant difference was demonstrated in the presence of symptoms of depression, anxiety and stress with respect to gender, age, level of education, working hours and years of work experience of the respondents. However, a significant difference was demonstrated in the presence of symptoms of anxiety and stress with respect to the clinic in which the respondents work, and in the presence of symptoms of anxiety with respect to the workplace of the respondents. Respondents with a higher prevalence of anxiety and stress symptoms are from cardiology (anxiety 50.0%, stress 45.0%), surgery (anxiety 41.9%, stress 32.3%) and HED (anxiety 43.8%, stress 35.5%). The workplace with the most symptoms (anxiety 60.0%, stress 45.0%) is the operating room. Differences in the presence of depressive symptoms in both mentioned categories were not significant, but a significant difference in their severity was demonstrated. The highest number of extremely serious symptoms of depression (38.9%) are shown by respondents who work in outpatient clinics, and the highest number of serious symptoms (66.7%) by those who work in intensive care or coronary units.
Although the majority of respondents do not show symptoms, the proportion of those with elevated scores on certain scales is by no means negligible (depression -30.2%; anxiety -34.9%; stress -30.8%). The results of the study suggest that more than a quarter of the respondents meet the DASS-21 criteria and show some level of symptoms of depression, anxiety and stress. In this study, symptoms of depression, anxiety and stress in nurses have a prevalence of more than 30%, which is more common than in the general population.20
The frequency of depressive symptoms among nurses in this study is within the ranges recorded in other studies around the world. Depression rates in nurses range from approximately 18% to 53%.21 In two studies conducted in the USA, the prevalence of depression ranged from 35% to 41%, or 18%.22 In a study conducted in China, the rate was 38%.23 Similar result was in Norway.24 The results of a systematic literature review and meta-analysis show that the prevalence of depression among Iranian nurses is 22%.18 As many as 33% of French nurses and 10% of Canadian nurses suffer from depressive symptoms.20
The prevalence of anxiety symptoms in the subjects in this study, with a prevalence rate of more than 30%, shows that more than a quarter of the subjects met the DASS-21 criteria for anxiety, while the highest number of those showing extremely severe symptoms was recorded. The prevalence of anxiety among nurses in this study is also within the range reported in the literature.20 The lowest prevalence of anxiety (7%) was recorded in Japanese nurses, while the highest (43.2%) was recorded in Iranian nurses. In Singapore, 21% of nurses suffer from anxiety disorders, but a very small proportion sought help for their emotional problems (less than 4%). In the USA, about 20% of nurses from various hospitals had anxiety-related symptoms.24
Also, the results show that more than a quarter of the respondents meet the DASS -21 criteria and show some level of stress. Most respondents with an elevated score show mild to moderate symptoms of stress. The level of stress among nurses can generally be moderate to high, ranging from 40% to 90%.20,25 In today’s society in which the needs for health care are increasing and characterized by rapid changes, nurses are taking on more and more responsibilities than ever before. As a result, they must possess numerous competencies, professional knowledge and skills, constantly improve themselves and follow new achievements and technologies. They must be mentally and physically prepared to deal with emergencies, serious illnesses and death, and numerous ethical dilemmas. Therefore, it is not surprising that healthcare workers are often exposed to increased levels of stress.26
A similar study was previously conducted in Croatia among nurses in a psychiatric clinic, in the intensive psychiatric care unit, and in the Institute of Emergency Medicine in the city of Zagreb. According to the results of that study, as many as 50% of the respondents showed.27 Various factors, such as differences in personality, cultural, social and working conditions, and 13. The productivity of employees with emotional problems is reduced, often leading to high rates of absenteeism due to health reasons, which in turn reduces the number of staff caring for patients. Research shows that insufficient numbers of healthcare workers can put patients at risk and contribute to increased injuries at work.28 Although the number of nurses has increased in recent years, their shortage remains a major problem. In addition to physical health, their emotional well-being and good mental health are of paramount importance. They are then more likely to make fewer mistakes at work, be more satisfied, and their work motivation will be increased.18
Few studies have compared the levels of depression, anxiety and stress in nurses from different clinics and departments, meaning that there is no current consensus on whether nurses from certain departments are more exposed to these problems.29 The results of this study showed that there is a significant difference in the presence of anxiety and stress symptoms among respondents from different clinics, such that respondents working in cardiology, surgery and HED have a higher prevalence of anxiety and stress than others. The highest proportion of respondents with present anxiety and stress symptoms is found in cardiology (anxiety 50.0%, stress 45.0%), followed by respondents with HED (anxiety 43.8%, stress 35.5%) and surgery (anxiety 41.9%, stress 32.3%). When it comes to depressive symptoms, no significant difference was demonstrated, although the highest proportion of respondents with depressive symptoms (41.7%) was recorded in cardiology. One of the reasons could be that a part of the examinees from cardiology are examinees of the coronary unit and the room for invasive cardiology, which are among the most stressful workplaces.
Furthermore, working in HED is considered an extremely stressful workplace. In addition to the common stressors to which all nurses are exposed, HED employees are also affected by numerous specific stressors and unforeseen situations. Namely, emergency room workers are the first to come into contact with patients, provide care to acutely ill, life-threatening and injured persons and often perform resuscitation. In addition, they are in constant contact with family members, which can lead to emotional exhaustion. In order to be able to adequately perform their job, emergency room nurses must have considerable knowledge, know how to cope and react in a timely manner in every situation. Therefore, it is of utmost importance to recognize stressful situations in time and try to alleviate them, as well as to take care of the mental health of nurses in risky work environments.
A study conducted on 1253 nurses states that surgical departments have more stress factors that affect the work ability of employees compared to other departments.30 This is also consistent with the results of this study, in which respondents from surgery, along with cardiology and HED, stood out as those showing a higher proportion of present symptoms of anxiety and stress compared to other respondents.31 Although nursing is an extremely stressful and demanding healthcare system are equally affected by stress, anxiety and depression.32 In this study, the results related to the severity of symptoms of depression, anxiety and stress in nurses with regard to the workplace showed significant differences. A significant difference was demonstrated in the presence of anxiety symptoms, with them being most prevalent among respondents working in the operating room. Respondents working in the operating room also had the highest number of stress symptoms, although no significant difference was demonstrated. A significant difference was demonstrated in the severity of depressive symptoms, with the highest proportion of extremely serious symptoms (38.9%) being shown by respondents working in outpatient clinics, while serious depressive symptoms (66.7%) were shown by a higher proportion of those working in intensive care or coronary care units.
If the results are compared with those of other studies, a similarity is observed. The literature lists intensive care units, coronary care units, emergency departments, surgical departments, operating rooms, oncology departments, and psychiatric departments as the most stressful workplaces for nurses. It is believed that nurses are at higher risk of excessive stress due to the extremely difficult working conditions in these workplaces.21 The largest number of respondents in this study who showed symptoms were from the aforementioned workplaces.
The operating room is one of the most challenging and stressful workplaces. Those who work in the operating room are under constant pressure, often exposed to great risks. They are required to be agile and precise, constantly acquire new knowledge and techniques, and to handle precise and state-of-the-art instruments, strictly following the rules, with no room for error. The specificity of the work of an operating room nurse is significantly different from that of a nurse in a ward. The demands directed towards greater productivity for the implementation of perioperative procedures with time constraints, continuous and dynamic work, best describe the complex tasks performed by nurses in the operating room.22 Research data indicate that nurses in the operating room cite shift work, which is most often realized through 24-hour on-call, unplanned overtime due to long-term surgical procedures, and 24-hour responsibility as reasons for high levels of stress.33
The largest proportion of respondents who show serious symptoms of depression (66.7%) work in intensive care and coronary care units. These are precisely the jobs that are cited in the literature as the most stressful with a high risk of developing depression in employees. Employees working in the aforementioned units work with the most seriously ill patients who require 24-hour care and constant monitoring. In addition, they use the most modern medical equipment and technology in their work. Intensive care units include constant monitoring, continuous health care, life support for seriously ill, vitally endangered patients and their treatment. The specificities of work in intensive care units are numerous, and therefore healthcare workers are exposed to an increased risk of professional stress and, consequently, numerous mental health problems that can be caused by excessive stress.
When it comes to sociodemographic characteristics, research has shown that they have a certain influence on the presence of symptoms of depression, anxiety and stress. The literature to date has implied various demographic and work predictors for the relatively high prevalence of negative mental states in nurses. Previous studies have found common predictors such as age, job satisfaction, years of employment, and marital status to increase the likelihood of developing stress, anxiety, and depression.20 This study did not show significant differences in the presence of depressive, anxiety, and stress symptoms with respect to gender, age, education level, employment history, and working hours.
Lewko, Misiak and Sierżantowicz in their study also did not find a statistically significant effect of age on mental health status.12 The results of the study conducted by Ardekani et al. did not show a difference in the severity of depressive symptoms in nurses with respect to age.34 A study from Hong Kong also showed that age has an insignificant role in depressive symptoms, but is a significant correlate of anxiety and stress symptoms. The results also showed an inverse relationship between age and depression, anxiety and stress. As age increased, symptoms of depression, anxiety and stress decreased.33 Like the results of this study, the aforementioned study from Hong Kong did not prove a significant influence of gender on the prevalence of symptoms of depression, anxiety and stress.23 In contrast, the results of the study in Iran confirmed a higher rate of depression and stress in women, although gender was not associated with symptoms of anxiety.35 Debogović proved significant differences in the severity of symptoms of depression, anxiety and stress with respect to gender, and a trend of increasing symptoms with increasing length of service.27
The data from the study conducted by Qi et al. show that nurses with higher and higher levels of education and longer years of service experience higher levels of stress.32 A study conducted in China showed that nurses with higher education have higher levels of anxiety than nurses with lower education.25 In an earlier study in Croatia, the influence of age, level of education and length of service on the experience of stress was not proven.32
Other variables that were examined (length of service, working hours) also did not prove to be a significant predictor of the presence of symptoms of depression, anxiety and stress, similar to a study from China where no significant association was found between length of service and symptoms of anxiety.36 However, several studies have shown that nurses with longer service are more prone to depression.18 A systematic review of the literature, which included 37 papers, found no definitive evidence that shift work is associated with poorer mental functioning in nurses.12
Night work has been associated with negative somatic consequences, but less is known about its impact on mental health. Monroe and Reid found that night work is a risk factor for depressive symptoms, especially in women.37 However, the results of a study conducted in Norway did not prove an association between night work and anxiety and depression. Similarly, the cumulative effect of night shifts over the past 12 months was not determined for any parameter.38
Although no significant difference in the severity of negative emotional states was demonstrated with respect to gender, age, level of education, years of work experience and working hours, a significant difference was demonstrated with respect to the workplace of the respondents.
STRENGTHS AND WEAKNESSES OF THE RESEARCH
Most previous research has mainly studied the impact of stress, less depression, and rarely anxiety and associated factors in nurses. For this reason, the DASS 21 was used in the study to measure three dimensions of emotional states, instead of using traditional instruments to measure only one dimension. The results of the study are generally in line with previously published works and provide additional insight into the mental health of the respondents.
This research has certain shortcomings. First, since this was a cross-sectional study, it is not possible to establish a cause-and-effect relationship between the studied phenomena. Furthermore, it is a small sample, given that the respondents who participated in the research are from only one hospital, so the conclusions of this research cannot be generalized to other parts of Croatia. A possible drawback of this research could be that a self-assessment scale was used as a measuring instrument. Namely, since the mentioned self-assessment measures are associated with the potential possibility of giving socially desirable answers, the question arises to what extent the respondents answered the questions honestly. Also, it is not known whether the nurses who refused to participate in the research had more or less mental health disorders. For the reasons mentioned, the research provides only a partial insight into the mental health problems and professional exposure of nurses to mental disorders of varying degrees of intensity. Therefore, a multicenter study should be conducted in the future on a larger number of nurses and in a larger number of hospitals.
SUGGESTIONS FOR FUTURE RESEARCH
Future research should use a longitudinal study design. A more comprehensive assessment of demographic and personal factors that may be considered predictors of negative emotional states could also be useful. A number of factors were not taken into account, so including additional variables would provide better insight into the presence of the observed symptoms. Future research should also investigate the effect of the psychosocial work environment on the incidence of negative emotional states in nurses.
Conclusion
The conducted research showed that the largest proportion of nurses do not show symptoms of depression, anxiety and stress, while the majority of respondents who have certain disorders show mild to moderate symptoms. Serious and extremely serious levels of symptoms are shown by the smallest number of respondents, and extremely serious symptoms are recorded most on the anxiety scale. Among respondents working in cardiology, surgery and HED, there is a higher representation of those who have symptoms of anxiety and stress than respondents from internal medicine and psychiatry, while the largest proportion of respondents with symptoms of anxiety and stress is from cardiology. There is no statistically significant difference in the presence of depressive symptoms depending on the clinic in which the respondents work.
No significant difference was demonstrated in the severity of symptoms of depression, anxiety and stress with respect to gender, age, level of education, length of service and working hours of the respondents. A significant difference was demonstrated in the presence of symptoms of anxiety with respect to the workplace. Symptoms of anxiety are most prevalent among respondents working in the operating room (60.0%), while they are least prevalent among respondents working in intensive care or coronary care units (12.0%). There is no significant difference in the presence of symptoms of depression and stress with respect to the workplace of the respondents. Among respondents with present symptoms of depression, a significant difference was demonstrated in the severity of symptoms, with the largest number of extremely serious symptoms being shown by respondents working in outpatient clinics (38.9%), while serious symptoms of depression are shown by a larger number of those working in intensive care or coronary care units (66.7%). The frequency of symptoms of depression, anxiety and stress, which is present in more than a quarter of the respondents, is relatively high. Although the harmful effects on the professional functioning of nurses cannot be completely eliminated, it is important to raise awareness of their potentially negative impact on mental health and to strive to reduce them as much as possible. The study showed that nurses are exposed to stressful situations in their work, which can affect their mental health.
CONFLICTS OF INTEREST STATEMENT
The authors have no conflicts of interest to declare.
References
- Wynne R. et al. Promoting mental health in the workplace: guidance to implementing a comprehensive approach. 2014. European Commission. doi: https://op.europa.eu/en/publication-detail/-/publication/c1358474-20f0-11e8-ac73-01aa75ed71a1/language-hr
- Babapour AR, Gahassab-Mozaffari N, Fathnezhad-Kazemi A. Nurses’ job stress and its impact on quality of life and caring behaviors: a cross-sectional study. BMC Nurs. 2022;31;21(1):75. doi: 10.1186/s12912-022-00852-y. PMID: 35361204; PMCID: PMC8968092.
- Sarafis P, et al. The impact of occupational stress on nurses’ caring behaviors and their health related quality of life. BMC Nurs. 2016;15(1):1–9. doi: https://doi.org/10.1186/s12912-016-0178-y
- Antolić B, Novak M. Promocija mentalnog zdravlja: Temeljni koncepti i smjernice za roditeljske i školske programe. Psihologijske teme. 2016;25(2):317-339. doi: https://hrcak.srce.hr/161868
- Božičević V, Brlas S, Gulin M. Psihologija u zaštiti mentalnog zdravlja. Prijedlog smjernica za psihološku djelatnost u zaštiti i promicanju mentalnog zdravlja. Zavod za javno zdravstvo „Sveti Rok“ Virovitičko-podravske županije; 2011. doi: http://www.zzjzvpz.hr/hr/sadrzaj/djelatnost/1/publikacije/ZZJZ_Psihologija_u_zastiti_mentalnog_zdravlja_smjernice.pdf
- Silobrčić Radić M. Mentalno zdravlje. Hčjz. 2011;7(28):292-6. doi: https://hcjz.hr/index.php/hcjz/article/viewFile/292/296
- World Health Organisation. Mental health: Fact sheet. 2019. doi: http://www.euro.who.int/__data/assets/pdf_file/0004/404851/MNH_FactSheet_ENG.pdf?ua=1
- Croatian Health Statistical Yearbook for 2023. Zagreb, 2024. doi: https://www.hzjz.hr/wp-content/uploads/2019/10/Ljetopis_Yearbook_2024-1.pdf
- Gheshlagh G, Valiei S, Rezaei M, Rezaei K. The relationship between personality characteristics and Nursing occupational stress. J Nurs Educ. 2013;1(3):27–34. doi: http://ijpn.ir/article-1-91-en.html
- Mojdeh S, Sabet B, Irani MD, Hajian E, Malbousizadeh M: Relationship of nurse’s stress with environmental-occupational factors. Iran J Nurs Midwifery Res. 2008;13(1):1–5. doi: https://www.researchgate.net/publication/267399099_Relationship_between_nurse’s_stress_and_environmental_-occupational_factors
- Stansfeld S, Candy B. Psychosocial work environment and mental health: a meta-analytic review. Scand J Work Environ Health. 2006;32(6):443–462. doi: https://www.ncbi.nlm.nih.gov/pubmed/17173201
- Lewko J, Misiak B, Sierżantowicz R. The relationship between mental health and the quality of life of Polish nurses with many years of experience in the profession: a cross-sectional study. Int J Environ Res Public Health. 2019;16(10):1798. doi: https://www.mdpi.com/1660-4601/16/10/1798/htm
- Hsu MY, Kernohan G. Dimensions of hospital nurses’ quality of working life. J Adv Nurs. 2006;54(1):120–131. doi: 0.1111/j.1365-2648.2006.03788.x.
- Brown H, Zijlstra F, Lyons E. The psychological effects of organizational restructuring on nurses. J Adv Nurs. 2006;53(3):344–357. doi: 10.1111/j.1365-2648.2006.03723.x.
- Škrinjarić JS, Šimunović D. Izvori profesionalnoga stresa medicinskih sestara u ambulantama obiteljske medicine. Med Jadertina. 2018;48(1-2):13-22. doi: https://hrcak.srce.hr/197846
- Perry L, Lamont S, Brunero S, Gallagher R, Duffield C. The mental health of nurses in acute teaching hospital settings: a cross-sectional survey. BMC Nurs. 2015;14:15. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4405850/
- Parveen R, et al. The impact of occupational stress on nurses caring behavior and their health related quality of life. Saudi J Med Pharm Sci. 2017;3(9):1016–1025. doi: 10.1186/s12912-016-0178-y.
- Saeedi Shahri SS, et al. Depression among Iranian nurses: a systematic review and meta-analysis. Med J Islam Repub Iran. 2017;31:130. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6014776/
- Vasconcelos SC, et al. Nursing staff members mental’s health and factors associated with the work process: an integrative review. Clin Pract Epidemiol Ment Health. 2016;12:167–176. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5278561/
- Maharaj S, Lees T, Lal S. Prevalence and risk factors of depression, anxiety, and stress in a cohort of Australian nurses. Int J Environ Res Public Health. 2018;16(1):61. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6339147/
- Valiei S, Rezaei M, Rezaei K. The relationship between personality characteristics and Nursing occupational stress. Iran J Psychiatr Nurs. 2013;1(3):27–34. doi: https://api.semanticscholar.org/CorpusID:57737921
- Henry J.D, Crawford J.R. The short‐form version of the Depression Anxiety Stress Scales (DASS‐21): Construct validity and normative data in a large non‐clinical sample. Br J Clin Psychol, 2005;44(2),227-239. doi: 10.1348/014466505X29657
- Gong Y, Han T, Yin X, Yang G, Zhuang R, Chen Y, Lu Z. Prevalence of depressive symptoms and work-related risk factors among nurses in public hospitals in southern China: a cross-sectional study. Sci Rep. 2014;4:7109. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5384112/
- Richardsen AM, Burke RJ, Leiter MP. Occupational demands, psychological burnout and anxiety among hospital personnel in Norway. Anxiety, Stress & Coping: An International Journal, 1992;5(1),55–68. doi: https://doi.org/10.1080/1061580920825048717
- Shareinia H, Khuniki F, Bloochi Beydokhti T. Comparison between job stress among emergency department nurses with nurses of other departments. Q J Nurs Manag. 2018;6(3):48–56. doi: 10.29252/ijnv.6.3.4.48
- McGrath A, Reid N, Boore J. Occupational stress in nursing. Int J Nurs Stud. 2003;40(5):555–565. doi: 10.1016/s0020-7489(03)00058-0
- Debogović S. Stres na radnom mjestu i njegovi učinci na zdravlje medicinskih sestara i tehničara. Varaždin, Croatia: University North; 2015.
- Croatian Chamber of Nurses. Proclamation of the Sisterhood of the Republic of Croatia, 2020. doi: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.hkms.hr/wp-content/uploads/2020/02/Proglas-hrvatskog-sestrinstva-2020.pdf
- Cheung T, Yip PS. Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int J Environ Res Public Health. 2015;12(9):11072-100. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586662/
- Ekić S, Primorac A, Vučić B. Profesionalni stres kod medicinskih sestara i tehničara. JAHS. 2016;2(1):39-46. doi: https://hrcak.srce.hr/164835
- Park H, Oh H, Boo S. The Role of Occupational Stress in the Association between Emotional Labor and Mental Health: A Moderated Mediation Model. Sustainability. 2019;11(7):1886. doi: 10.3390/su11071886
- Jurišić M, Vlašić A, Bagarić I. Stres na radnom mjestu kod zdravstvenih djelatnika. Zdr glas. 2019;5(2):45-52. doi: https://hrcak.srce.hr/228912
- Zhou H, Gong YH. Relationship between occupational stress and coping strategy among operating theatre nurses in China: a questionnaire survey. J Nurs Manag. 2015;23:96-106. doi: https://www.ncbi.nlm.nih.gov/pubmed/23927607
- Ardekani Z, Kakooei H, Ayattollahi SMT, Choobineh A, Nasle Seraji G. Prevalence of mental disorders among shift work hospital nurses in Shiraz, Iran. Pak J Biol Sci. 2008;13: 956-960. doi: https://www.ncbi.nlm.nih.gov/pubmed/18819649
- Yazdanshenas Ghazwin M, et al. The association between life satisfaction and the extent of depression, anxiety and stress among Iranian nurses: a multicenter survey. Iran J Psychiatry. 2016;11(2):120–127. doi: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4947220/
- Parks SH, Pilisuk M. Caregiver burden: gender and the psychological costs of caregiving. Am J Orthopsychiatry. 1991;61(4):501-509. doi: https://onlinelibrary.wiley.com/doi/abs/10.1037/h0079290
- Monroe S.M, Reid M.W. Life Stress and Major Depression. Curr Dir Psychol Sci, 2009;18(2),68-72. doi: https://doi.org/10.1111/j.1467-8721.2009.01611.x
- Qyane NMF, Pallesen S, Moen BE, Akerstedt T, Bjorvatn B. Associations between night work and anxiety, depression, insomnia, sleepiness and fatigue in a sample of Norwegian nurses. PloS One. 2013;8(8):e70228. doi: https://doi.org/10.1371/journal.pone.0070228
APPENDIX
SURVEY QUESTIONNAIRE
Please circle or complete the following questions:
- Gender: a) Male b) Female
- Age (years of age) ________