





Central Neck Dissection in Thyroid Cancer: Strategies & Classifications
Refining strategies in Central Neck Dissection in Thyroid Cancer: A Novel Paratracheal Subclassification for Precision Surgery
Deepak Saharan1*, Vikas Sharma2, CH Sajid Rashid3, Sourabha Kumar Patro4
- Associate Professor, Department of Otorhinolaryngology and Head & Neck Surgery, All India Institute of Medical Sciences, Rajkot, Gujarat, India.
- Associate Professor, Department of Otorhinolaryngology and Head & Neck Surgery, Command Hospital, Kolkata, West Bengal, India.
- Fellow, Head & Neck Surgery, Tata Cancer Hospital, Mullanpur, Punjab, India.
- Associate Professor, Department of Otorhinolaryngology and Head & Neck Surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: Saharan, D., Sharma, V., et al., 2025. Refining strategies in Central Neck Dissection in Thyroid Cancer: A Novel Paratracheal Subclassification for Precision Surgery. Medical Research Archives, [online] 13(3). https://doi.org/10.18103/mra.v13i3.6429
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6429
ISSN 2375-1924
ABSTRACT
Central compartment neck dissection (CCND) is a cornerstone in the surgical management of thyroid gland carcinoma, targeting level VI and VII lymph nodes as the primary lymphatic drainage sites. Despite its established role, controversies persist regarding anatomical definitions, the extent of dissection (prophylactic vs. therapeutic, unilateral vs. bilateral, level VI alone vs. VI and VII), and the balance between oncologic efficacy and morbidity, hypoparathyroidism and recurrent laryngeal nerve (RLN) injury. This review synthesizes current evidence from anatomical, clinical, and technological perspectives, addressing ambiguities in level VI and VII boundaries, the applicability of en bloc resection, and the utility of emerging tools like near-infrared autofluorescence (NIRAF) and indocyanine green (ICG) imaging. We propose refined anatomical subclassifications and advocate for tailored, precision-based strategies to optimize outcomes while minimizing complications.
Keywords
Thyroid cancer, central neck dissection, paratracheal nodes, surgical management, hypoparathyroidism, recurrent laryngeal nerve injury.
Introduction
Thyroid gland carcinoma, primarily differentiated thyroid carcinoma (DTC), frequently metastasizes to the central compartment lymph nodes namely Levels VI and VII encompassing prelaryngeal, pretracheal, paratracheal, and superior mediastinal nodes. These nodes represent the “first echelon” of lymphatic spread, making CCND a strong tool in surgeons armamentarium to prevent residual or recurrent disease.
The American Thyroid Association (ATA) guidelines endorse CCND for both therapeutic (clinically node-positive, cN1) and prophylactic (clinically node-negative, cN0) indications, yet its application remains debated due to anatomical variability, oncologic necessity, and risk of post operative morbidity. Key controversies include the limits of level VI and VII compartments, the extent of dissection, and the preservation of parathyroid glands and RLN function. This review integrates insights from multiple studies, review, consensus guidelines to address these issues and propose future course of action.
Controversies in Anatomical Definition
Boundaries of Level VI:
Level VI is defined by the ATA as bounded as follows: Anteriorly: by the strap muscles Posteriorly: by the deep cervical fascia Superiorly: by the hyoid bone Laterally: by the sternohyoid muscles (surgically) by the common carotid arteries (radiologically) Inferiorly: by the suprasternal notch. This delineation, while practical, is challenged by imaging limitations and anatomical variations. Xing et al. noted ultrasonography’s low sensitivity (39%) for detecting central nodes, emphasizing intraoperative judgment over preoperative planning. Variability in strap muscle positioning and fascia layers further complicates standardization, necessitating clearer surgical landmarks.
Borderline Between Level VI and VII:
The inferior boundary of level VI at the suprasternal notch transitions into level VII, defined as superior mediastinal nodes up to the brachiocephalic artery (right) and its axial plane (left). The artery’s oblique course (50°-85° from the aorta) introduces interpersonal variability, rendering it an inconsistent landmark. Authors want to highlight the left brachiocephalic vein’s more stable horizontal course (variation <5%) is better alternative though it is not universally accepted.
Redefining level VII’s inferior boundary to the vein’s superior margin and lateral borders as the right brachiocephalic artery/common carotid and left common carotid enhances surgical precision, aligning with cadaveric data and practical feasibility.
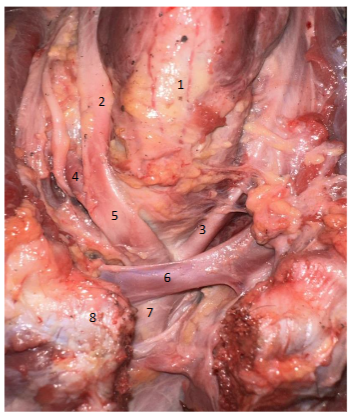
1. Trachea 2. Right common carotid 3. Left common carotid 4. Right subclavian artery 5. Brachiocephalic artery 6. Left brachiocephalic vein 7. Aorta 8. Sternum
Applicability Of En Bloc Resection
Traditional en bloc resection advocating removing lymph nodes with surrounding fibrofatty tissue, aims for comprehensive clearance but is contentious in thyroid surgeries with CCND due to proximity to the RLN and parathyroid glands. Takahashi et al. report a 20.3% persistent hypoparathyroidism rate with aggressive clearance, reflecting disrupted parathyroid vascularity. Given DTC’s favourable prognosis (10-year survival >90%), selective node removal (“berry picking”) may suffice in low-risk cases, a hypothesis supported by Giordano et al. who found comparable oncologic outcomes with reduced morbidity when preserving critical structures. This practice though is condemned by Head Neck Oncosurgeon and endocrine surgeons as the basic principles of neck dissection albeit for Head Neck malignancies strongly disallows it.
Indications of CCND
Prophylactic vs. Therapeutic Dissection in cN0 Patients:
Therapeutic CCND is standard for cN1 DTC, with Randolph et al. Linking metastatic node size and number to prognosis. Prophylactic CCND (pCCND) in cN0 disease, however, divides opinion. ATA guidelines do not recommend routine pCCND in cN0 patients due to the lack of demonstrated survival benefit and increased morbidity. However, selective pCCND is considered in high-risk cases, such as patients with T3/T4 tumors, extrathyroidal extension, or aggressive histology. Several studies argue that pCCND may provide staging benefits and reduce recurrence. Rao et al. reported occult metastases in 30%-60% of cN0 cases, with a lower recurrence rate (1.0% vs. 3.6%) when pCCND was performed. Yin et al. identified younger age (<55 years) and multifocality as key predictors of occult metastases, supporting selective pCCND in high-risk patients. Lykke et al. conducted a randomized controlled trial (RCT) that found no significant recurrence advantage in low-risk cN0 papillary thyroid carcinoma (PTC), but increased morbidity (transient hypocalcemia 14%-40%).
Unilateral vs. Bilateral Dissection:
Unilateral CCND targets tumor-side level VI nodes, while bilateral dissection includes contralateral nodes. ATA primarily recommends unilateral CCND unless there is clinical or imaging evidence of contralateral nodal disease, citing increased morbidity, (16% vs. 12% RLN palsy). Studies suggest bilateral CCND may upstage 25% of cN0 patients to N1a, impacting adjuvant therapy decisions. However, the presence of skip metastases (7%-10%) suggests that contralateral involvement may occur even in unilateral disease. Bilateral CCND is generally reserved for cases with bilateral tumors or ipsilateral nodal positivity.
Level VI Alone vs. Combined VI and VII Dissection:
ATA Guidelines recommend Level VI dissection alone is standard for cN0 cases, while level VII dissection is reserved for cN1 cases or when imaging suggests involvement. Alternative Perspectives given by articles like Rossi et al. found that 15% of cN0 patients had occult level VII involvement and suggested that combined VI and VII dissections in advanced disease may reduce mediastinal recurrence. However, level VII dissection increases hypocalcemia risk (52% vs. 40%), raising concerns about balancing oncologic benefit with functional preservation.
Preservation of Parathyroid Function
Hypoparathyroidism: Incidence and Impact
Hypoparathyroidism is a major CCND complication, with transient rates of 52% and persistent rates of 20.3% post-dissection. Giordano et al. link this to devascularization during fibrofatty clearance, with in-situ preservation of ≥3 glands achieving normocalcemia in 80% of cases. Autotransplantation recovers function in 70% of cases, though success varies with gland integrity.
Anatomical and Technical Challenges
Parathyroids, supplied by inferior thyroid artery (ITA) branches (80%-90%), are vulnerable due to their small caliber (<2 mm) and variable descent. ITA absence (2%-3%) complicates preservation, particularly on the left. Wang et al.’s “TBP” technique (thyroid-parathyroid-blood supply preservation) reduces hypoparathyroidism to 15% vs. 25% with standard methods, emphasizing meticulous capsular dissection.
Technological Advances
Magnification (≥2.5x loupes) and ICG imaging reduce hypocalcemia by 10%, while NIRAF cuts persistent hypoparathyroidism to 5%. Huang et al.’s trial combining NIRAF-ICG achieves 95% parathyroid viability, dropping postoperative hypocalcemia to 8%. These tools enable real-time parathyroid identification, shifting CCND toward precision surgery.
Proposed Paratracheal Subclassification
We propose subclassifying paratracheal nodes into superior (above ITA) and inferior (below ITA) subgroups for right and left sides.
| Paratracheal lymph node group of Level VI | Sub group nomenclature |
|---|---|
| Right | Rt Superior paratracheal |
| Rt Inferior paratracheal | |
| Left | Lt Superior paratracheal |
| Lt Inferior paratracheal |
Superior paratracheal “berry picking” avoids fibrofatty clearance near superior parathyroids, preserving function in DTC where soft tissue deposits are rare (<1%). Inferior paratracheal dissection, leveraging NIRAF-ICG, ensures ITA branch preservation. This subclassification enhances anatomical precision and awaits prospective validation.
Discussion
CCND’s controversies stem from balancing oncologic clearance with functional preservation. The brachiocephalic vein as a level VII boundary addresses arterial variability, improving consistency. Prophylactic CCND’s high occult metastasis rate (56%) supports its staging role in high-risk cN0 DTC, though morbidity (transient hypocalcemia 52%, RLN palsy 16%) mandates selective use. Bilateral and level VII dissection suit cN1 or advanced cN0 cases, while unilateral VI dissection suffices for low-risk PTC.
Parathyroid preservation remains paramount. En bloc clearance, suited to lateral neck dissections, mismatches DTC’s biology and central compartment anatomy. NIRAF-ICG and magnification reduce hypoparathyroidism to single digits, aligning with our proposed paratracheal subclassification for selective node removal. Limitations include limited level VII metastasis data and the need for long-term recurrence studies. Future research should validate these proposals via RCTs, integrating molecular markers (e.g., BRAF V600E) for risk stratification.
Conclusion
CCND for thyroid carcinoma navigates a complex landscape of anatomy, oncology, and function. Refining level VII’s boundary to the brachiocephalic vein and subclassifying paratracheal nodes address anatomical ambiguities. Prophylactic CCND benefits high-risk cN0 patients, with bilateral and VII dissection reserved for advanced cases. Precision technologies like NIRAF-ICG minimize morbidity, heralding a tailored approach to optimize outcomes in this evolving field.
Conflict of Interest: None.
Funding Statement: None.
Acknowledgements: None.
References:
- Xing Z, Qiu Y, Yang Q et al. Thyroid cancer neck lymph nodes metastasis: Meta-analysis of US and CT diagnosis. Eur J Radiol. 2020 Aug;129:109103. doi: 10.1016/j.ejrad.2020.109103. Epub 2020 Jun 13. PMID: 32574937.
- Robbins KT, Shaha AR, Medina JE, Califano JA, Wolf GT, Ferlito A, Som PM, Day TA; Committee for Neck Dissection Classification, American Head and Neck Society. Consensus statement on the classification and terminology of neck dissection. Arch Otolaryngol Head Neck Surg. 2008 May;134(5):536-8. doi: 10.1001/archotol.134.5.536. PMID: 18490577
- Takahashi T, Yamazaki K, Shodo R, Ueki Y, Horii A. Actual prevalence of hypoparathyroidism after total thyroidectomy: a health insurance claims-database study. Endocrine. 2022 Oct;78(1):151-158. doi: 10.1007/s12020-022-03153-1. Epub 2022 Aug 1. PMID: 35913569
- Giordano D, Valcavi R, Thompson GB, Pedroni C, Renna L, Gradoni P, Barbieri V. Complications of central neck dissection in patients with papillary thyroid carcinoma: results of a study on 1087 patients and review of the literature. Thyroid. 2012 Sep;22(9):911-7. doi: 10.1089/thy.2012.0011. Epub 2012 Jul 24. PMID: 22827494.
- Randolph GW, Duh QY, Heller KS et al; American Thyroid Association Surgical Affairs Committee’s Taskforce on Thyroid Cancer Nodal Surgery. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid. 2012 Nov;22(11):1144-52. doi: 10.1089/thy.2012.0043. Epub 2012 Oct 19. PMID: 23083442.
- Rao KN, Rajguru R, Dange P et al. Lower Rates of Hypocalcemia Following Near-Infrared Autofluorescence Use in Thyroidectomy: A Meta-Analysis of RCTs. Diagnostics (Basel). 2024 Feb 27;14(5):505. doi: 10.3390/diagnostics14050505. PMID: 38472977; PMCID: PMC10931323.
- Yin, S., Pan, B., Yang, Z. et al. Combined use of autofluorescence and indocyanine green fluorescence imaging in the identification and evaluation of parathyroid glands during total thyroidectomy: A randomized controlled trial. Front. Endocrinol. 2022, 13, 897797.
- Lykke E, Christensen A, Juhl K et al. Effect of near infrared autofluorescence guided total thyroidectomy on postoperative hypoparathyroidism: a randomized clinical trial. Eur Arch Otorhinolaryngol. 2023 May;280(5):2593-2603. doi: 10.1007/s00405-023-07867-4. Epub 2023 Feb 28. PMID: 36853388; PMCID: PMC9971666.
- Shaphaba K, Thakar A, Sakthivel P et al. Incremental value of magnification and indocyanine green for parathyroid preservation in thyroid surgery. Head Neck. 2023 Jul;45(7):1753-1760. doi: 10.1002/hed.27387. Epub 2023 May 5. PMID: 37144335.
- Rossi, L.; Vasquez, M.C.; Pieroni, E.; Ambrosini, C.E.; Miccoli, M.; Cetani, F.; Elisei, R.; Materazzi, G. Indocyanine green fluorescence and near-infrared autofluorescence may improve post-thyroidectomy parathyroid function. Surgery 2023, 173, 124–131.
- Tartaglia F, Blasi S, Giuliani A et al. Parathyroid autotransplantation during total thyroidectomy. Results of a retrospective study. Int J Surg. 2016 Apr;28 Suppl 1:S79-83. doi: 10.1016/j.ijsu.2015.05.059. Epub 2015 Dec 18. PMID: 26708849.
- Su A, Gong Y, Wu W, Gong R, Li Z, Zhu J (2018) Does the number of parathyroid glands autotransplanted affect the incidence of hypoparathyroidism and recovery of parathyroid function? Surgery 164:124–129.
- Ozgüner G, Sulak O. Arterial supply to the thyroid gland and the relationship between the recurrent laryngeal nerve and the inferior thyroid artery in human fetal cadavers. Clin Anat. 2014 Nov;27(8):1185-92. doi: 10.1002/ca.22448. Epub 2014 Aug 8. PMID: 25130905.
- Wang JB, Wu K, Shi LH, Sun YY, Li FB, Xie L. In situ preservation of the inferior parathyroid gland during central neck dissection for papillary thyroid carcinoma. Br J Surg. 2017 Oct;104(11):1514-1522. doi: 10.1002/bjs.10581. Epub 2017 Aug 7. PMID: 28782797.
- Saber, A.; Rifaat, M.; Ellabban, G.M.; Gad, M.A. Total thyroidectomy by loupe magnification: A comparative study. Eur. Surg. 2011, 43, 49–54.
- Pata, G.; Casella, C.; Mittempergher, F.; Cirillo, L.; Salerni, B. Loupe magnification reduces postoperative hypocalcemia after total thyroidectomy. Am. Surg. 2010, 76, 1345–1350.