






CBT for Psychosis: Case Report on Recovery and Therapy
Cognitive Behavioural Psychotherapy with a person presenting with a second episode of psychosis: A Case Report
Kara McTiernan1,2
- Health Service Executive, HSE Unit 1 Techport, Coolmine Industrial Estate, Blanchardstown, Dublin 15.
- School of Psychology, Newcastle University, 4th Floor, Dame Margaret Barbour Building, Wallace Street, Newcastle Upon Tyne, UK.
OPEN ACCESS
PUBLISHED: 28 Febuary 2025
CITATION:MCTIERNAN, Kara. Cognitive Behavioural Psychotherapy with a person presenting with a second episode of psychosis: A Case Report. Medical Research Archives, [S.l.], v. 13, n. 2, mar. 2025. Available at: <https://esmed.org/MRA/mra/article/view/6248>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i2.6248
ISSN 2375-1924
ABSTRACT
Background: Mental health services are prioritizing the delivery of Cognitive Behavioural Psychotherapy (CBTp) for people with psychosis. However, it is recognized that there is scope to further research and to adapt this evidenced based therapy for the client group. Recovery processes could also be explored. Single case designs may be informative in gaining detailed knowledge of the nuances in how individuals respond to CBTp.
Case report: This case report investigates an individual’s response to CBTp, within the context of a secondary care service. The person, aged in her 30’s, was recovering from a second episode of psychosis and was presenting with residual symptoms linked with a delusion. The intervention incorporated: the stress vulnerability framework, identifying maladaptive cognitive processes, challenging cognitions, decision making and a behavioral experiment. Positive Psychotherapy (PPT), which aligns with recovery was integrated into the therapy. The case report details the person’s response up until session ten of twenty-three appointments. Idiosyncratic measures of emotion and cognition were recorded. There was a decrease in the client’s level of anxiety and in the intensity of the negative cognition. The client gained a cognitive understanding of the connection between negative cognition as a maintaining factor in psychosis and actively managed this. Moreover, there was a notable increase in the person’s level of functioning.
Conclusion: The findings indicate that CBTp is beneficial in: reducing anxiety, tempering negative thoughts as well as improving functioning. Evidently CBTp can be delivered with Positive Psychotherapy and there are gains in doing so. However, further research is required in monitoring individual responses to specific therapeutic processes. Future single case research could also explore the novel finding that internet use triggers and maintains processes underpinning delusions.
Keywords
CBT, Psychosis, Delusions, Positive Psychotherapy, Recovery and Internet use.
Practitioner points
- The case report tracked the nuances in an individual’s response to CBTp.
- CBTp was found to decrease anxiety and the intensity of the negative cognition.
- There is evidence that CBT can be delivered with PPT, which is a recovery oriented therapy.
- Internet use may be implicated in the triggering and maintenance of delusions.
Introduction
Mental health services are placing an emphasis on devising and delivering therapy for people with psychosis. Historically there is a lack of psychological intervention for this cohort of people attending services and an absence of therapeutic research. Cognitive Behavioural Psychotherapy (CBT) and family therapy are evidenced based interventions. Meta reviews indicate that the individual intervention of CBT results in small to modest effects. There is therefore scope to continue to improve the intervention. Psychologists are currently investigating targeting specific maintaining processes, predictive coding as well as new methods of delivery including virtual reality. It is also suggested that outcomes may differ if heterogeneous outcomes to interventions are recorded. This too would facilitate greater attunement to monitoring the overall therapeutic process and to documenting the complexity inherent in psychosis. This differs from the pre/post design of randomized control trials which primarily researches group rather than individual outcomes. Despite the innovations it is noteworthy that CBT remains symptom/problem focused and therefore it does not directly attend to the person’s broader sense of self (i.e. personality) or to indicators of recovery, which go beyond symptom distress. However, recovery is currently a key strategic objective of mental health services including the Irish Health Service. Psychologists working with people with psychosis are therefore broadening CBT to include indicators of functioning and recovery alongside the associated measures. However, Positive Psychotherapy (PPT) is the empirically supported therapy which specifically addresses the person’s broader sense of self and subjective wellbeing. It therefore provides the processes for attaining personal recovery. It centers on the positives within people rather than the problems which people experience. It is an active therapy, with therapists drawing out and instilling positive psychological resources within people. Despite the differences it is proffered that CBT and PPT could be delivered in tandem, yet this is under researched. The current case report therefore monitors an individual’s response to CBTp. It also investigates the delivery of CBT with Positive Psychotherapy.
Assessment
PRESENTING ISSUE.
‘Mary’ was in her early thirties and completing a masters programme when she first experienced a psychotic episode. She presented to the services with: persecutory delusions, paranoid ideation and unusual behaviour. Substance misuse was implicated in the presentation. Mary was discharged from the service with stable mental health and returned to college. Two years later, a second episode of psychosis occurred. This centred again on paranoid ideation and persecutory delusions, specifically Mary believed that there was a bug in her brain and that google was monitoring her. There was no evidence of substance misuse. This resulted in a three-week hospital admission and the commencement on Olanzapine 10mg daily. Mary discontinued her college programme, returned to Dublin and was transferred to the current community mental health team in 2023.
FAMILY CONTEXT
In considering the context, there is a parental history of severe depression alongside hospital admission. Mary’s next of kin is an older adult, with a history of positive mental health. However, there was a death in the family in 2016 which the family are processing. Mary has highlighted that her next of kin has high levels of emotional intelligence and this is a supportive relationship. Mary is the youngest of three siblings. One sibling lives locally and there can be minor conflicts within this relationship, which can be a source of stress. Another sibling lives abroad and this is a close relationship. When Mary’s next of kin realised that Mary was experiencing psychosis, she was directed to return home and her sibling ensured that this occurred. In contrast with Mary’s next of kin, her siblings do not have complete insight into psychosis and to the ongoing management of mental health.
PERSONAL HISTORY
Mary has no history of a mental health difficulty or a significant health issue prior to the first episode of psychosis. There is no history of early life trauma or trauma either within the family or the social context. Mary experienced a stable childhood with no issues within her family relationships. She is currently single and has a longstanding social network, with friendships from primary school. There are no: alcohol, substance abuse, or addictive issues present.
EDUCATIONAL AND OCCUPATIONAL FUNCTIONING
Mary was noted to be ‘good, friendly and funny’ within her primary and secondary schools. She attained the leaving certificate and then completed an undergraduate degree. Mary was subsequently employed within a related sector before deciding to complete the masters programme. She reached the final year of this course and submitted sixteen of the seventeen assignments.
CURRENT MULTIDISCIPLINARY TEAM INTERVENTION
Mary is regularly reviewed by Psychiatry and is currently prescribed Aripiprazole 20mg once a day. There is also the continuous intervention with her Clinical Nurse Specialist, who also links with her next of kin.
PROTECTIVE FACTORS
In considering protective factors, a supportive family network is present. Mary is: reflective, organized and has an interest in CBT. It is noteworthy that she takes notes of her conversations with mental health professionals and is active in writing and setting her future goals. This includes planning to make a decision in relation to her college course. She is currently working on her mental health by: following the care plan, communicating with other people and by being mindful of healthy behaviours in relation to her diet and exercise schedule. Interests are noted in relation to: reading, socialising and being active in a weekly crafts group.
CURRENT MENTAL HEALTH STATE
Mary is orientated to the time and to the place and has insight into the experience of psychosis. There are currently no issues in Mary’s speech. There is a fear of a significant relapse as well as adjustment to the process of ongoing review and management. There is no evidence of risk with regards to herself or to other people. Mary is currently experiencing residual symptoms of psychosis specifically in relation to negative affect as well as paranoid ideation and persecutory cognitive processes. There is negative affect occurring as a result of social comparisons to siblings and friends as well as from distancing herself from the college social network. The latter of which may link with self-stigma as a result of experiencing psychosis within this context. She is compliant with the care plan and is mainly supported by her next of kin. Options are being considered in terms of accessing the rehabilitation service.
IMPRESSION
In line with NICE guidelines it may be beneficial to deliver CBTp in order to address the maladaptive self-cognitions (implicated in maintaining the residual symptoms of the persecutory delusion) and to increase levels of functioning. The latter of which aligns with Mary’s main goal, which is ‘I hope to work again’. There is also anxiety occurring in relation to (1) the longer-term impact of experiencing repeated episodes of psychosis as well as (2) fears in completing the college course.
ETHICAL STATEMENT
This case report adheres to HSE procedures. Identifiable information pertaining to the participant and to the service was therefore removed. The client consented to the undertaking of this work and to its publication. This is in line with the Psychological Society of Ireland code of professional ethics.
Intervention
1. FORMULATION
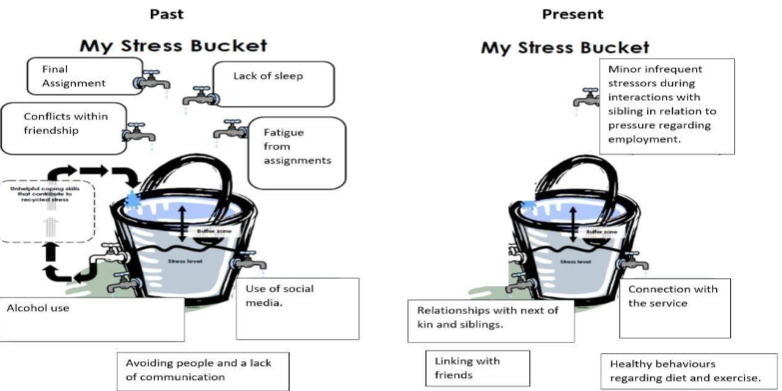
Mary presented with the cognitions that: the world is dangerous, other people are harmful and within herself, I am vulnerable. The following formulation, which involved integrating: a notes review, clinical observations and a clinical interview was constructed with Mary. This information was revisited during appointments through the use of the stress vulnerability framework.
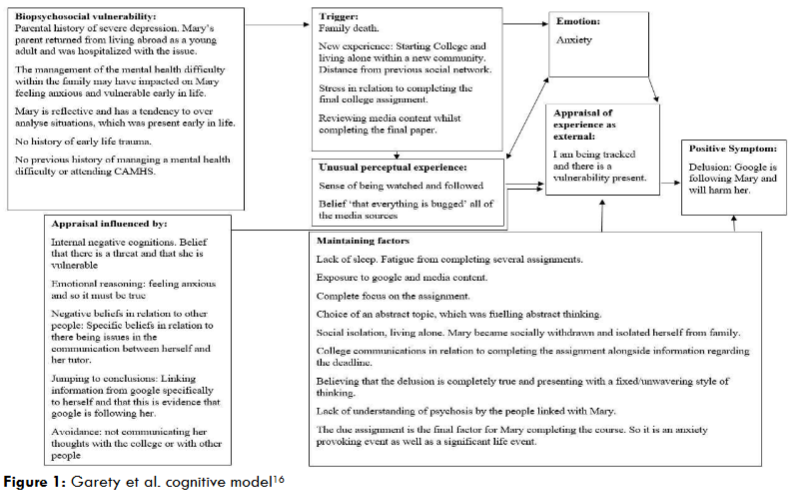
This framework reinforced the improvements within Mary’s mental health and that the levels of adaptive resources/coping strategies were increasing. Later in the intervention Mary communicated a natural metaphor of ‘I am swimming’ whereby there was a stability emerging within her mental health as well as coping with day to day activities. During the intervention the intensity of maladaptive cognitive processes underpinning the persecutory delusions re-emerged on two occasions (1) when Facebook contacted Mary in relation to deactivating her account and (2) when there was an assessment for the rehabilitation service. This reactivated cognitions in relation to other people being harmful, feeling vulnerable and it reactivated a pattern of avoiding people. This was managed with the use of the stress bucket and by actively removing a main trigger of social media use. She also worked through the reality of how the rehabilitation service can be a useful option in terms of people managing mental health. However, there was an awareness that it was a choice to complete the assessment with the service as there were family supports present.
2. AWARENESS OF MALADAPTIVE COGNITIVE PROCESSES
Mary became conscious of maladaptive cognitive processes which were maintaining the anxiety and the residual symptom of the persecutory delusions, specifically:
- a. Recurring false beliefs within the present. For example, believing (1) that her next of kin contacted the Gardaí (police) in order to arrest her (2) the false belief that family felt negative towards Mary as a result of previous conflicts and (3) that there was a cognitive issue from the previous substance misuse. Mary engaged in checking such false beliefs and accepted the facts that (1) her next of kin contacted the Gardaí as she was distressed and support was required in order to bring her to hospital (2) Mary is valued within the family, as evidenced by ongoing contacts with her siblings and (3) a previous scan found no cognitive issues as a result of this behaviour. It was accepted that a cognitive distortion was occurring which may be linked to the negative affect stemming from the psychosis.
- b. Focusing on the past and recalling negative events which was resulting in negative affect towards herself in the present. There was a particular emphasis on past events of writing information in relation to war on social media when the delusion was fixed as well as on a conflict with a cousin. She worked on this by focusing on the present and by being active in setting out day to day goals in the present, for example: meeting with friends, shopping, attending appointments and planning pleasant events. Towards the end of the intervention Mary reflected on how she valued her relationship with her cousin and that the conflict could be understood within the context of psychosis. She contacted her cousin and arranged social activities. Mary’s next of kin and uncle also reinforced healthy relationships within the family network.
- c. A broad style of thinking where issues were over complicated by exploring multiple options for activities. For instance, by considering multiple differing choices of employment, rather than focusing on a particular sector. This was resulting in not moving forward with goals. Early in the intervention this may have reflected the anxiety which Mary was experiencing. Decisions were therefore simplified to one or two options and tailored to align with specific criteria. This resulted in the decision that as a result of the psychosis, one criteria was not to place additional stressors onto her mind. It was therefore decided to consider employment opportunities which involved being behaviourally active.
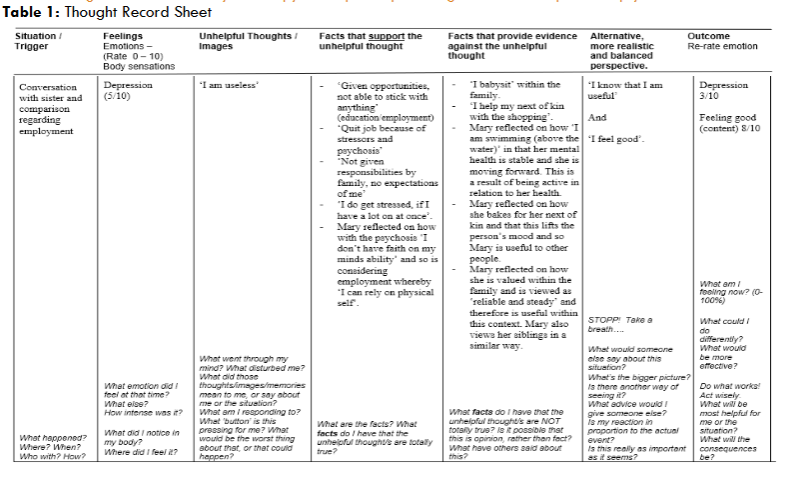
- d. Focusing on the negatives whilst discounting the positives. Mary became conscious of ongoing negative self-thoughts which were reinforcing the psychosis. The ongoing negative cognition of ‘I am useless’ was challenged through the use of the following thought record:
3. DECISION REGARDING RETURNING TO COLLEGE
It was clear that there was unfinished business in relation to the decision regarding the college course. Reflecting on this was triggering anxiety. It was also resulting in recalling traumatic memories from the psychosis which was negatively impacting on mood and reinforcing negative cognitions of being ‘useless’. Mary became conscious of the choice in returning to college or not returning to college. There was also a choice in making the decision or delaying the decision. It was decided to contact the college in order to gain further information in relation to the programme. The college was responsive to Mary and it was agreed that Mary could return to the course, with the option of attending online. This was useful in terms of Mary continuing with the care plan. Within this context a cost benefit analysis was undertaken as detailed in table 2.
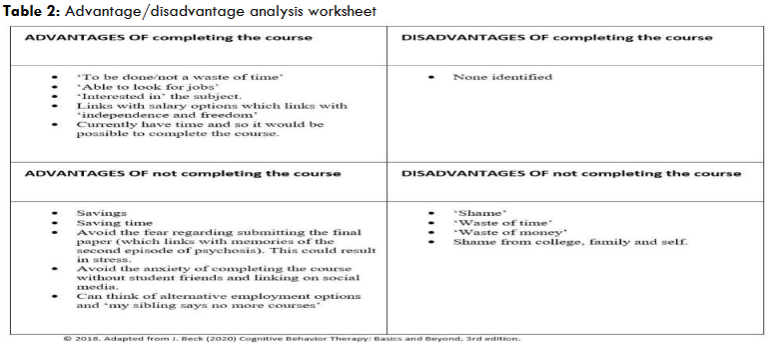
Mary decided not to return to the course as health continued to be prioritized. However, the goal of returning to employment remained. One of the factors which was negatively impacting on potential employment options was the false belief that socially ‘I am awkward’. This cognition emerged from Mary reflecting on a previous employment experience. This cognition was challenged through the use of a behavioural experiment as outlined in figure 3.
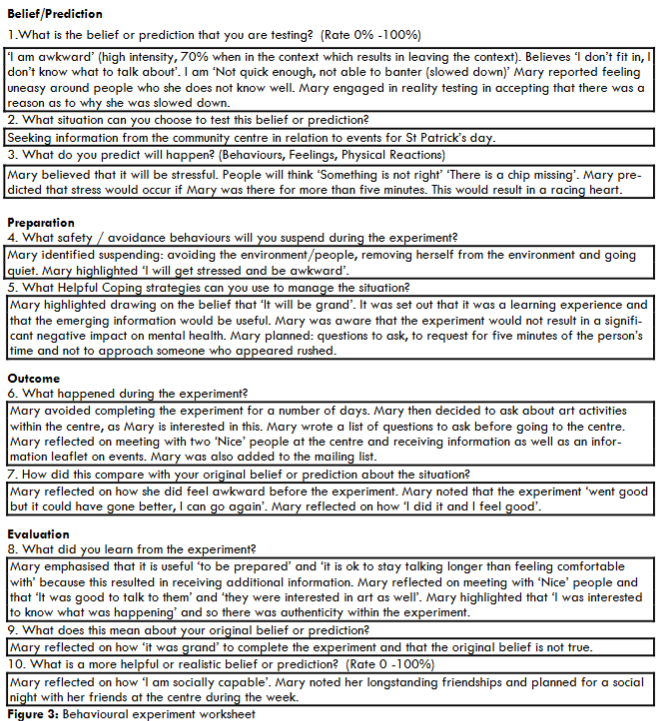
Belief/Prediction
- What is the belief or prediction that you are testing? (Rate 0% -100%) ‘I am awkward’ (high intensity, 70% when in the context which results in leaving the context). Believes ‘I don’t fit in, I don’t know what to talk about’. I am ‘Not quick enough, not able to banter (slowed down)’ Mary reported feeling uneasy around people who she does not know well. Mary engaged in reality testing in accepting that there was a reason as to why she was slowed down.
- What situation can you choose to test this belief or prediction? Seeking information from the community centre in relation to events for St Patrick’s day.
- What do you predict will happen? (Behaviours, Feelings, Physical Reactions) Mary believed that it will be stressful. People will think ‘Something is not right’ ‘There is a chip missing’. Mary predicted that stress would occur if Mary was there for more than five minutes. This would result in a racing heart.
Preparation
- What safety / avoidance behaviours will you suspend during the experiment? Mary identified suspending: avoiding the environment/people, removing herself from the environment and going quiet. Mary highlighted ‘I will get stressed and be awkward’.
- What Helpful Coping strategies can you use to manage the situation? Mary highlighted drawing on the belief that ‘It will be grand’. It was set out that it was a learning experience and that the emerging information would be useful. Mary was aware that the experiment would not result in a significant negative impact on mental health. Mary planned: questions to ask, to request for five minutes of the person’s time and not to approach someone who appeared rushed.
Outcome
- What happened during the experiment? Mary avoided completing the experiment for a number of days. Mary then decided to ask about art activities within the centre, as Mary is interested in this. Mary wrote a list of questions to ask before going to the centre. Mary reflected on meeting with two ‘Nice’ people at the centre and receiving information as well as an information leaflet on events. Mary was also added to the mailing list.
- How did this compare with your original belief or prediction about the situation? Mary reflected on how she did feel awkward before the experiment. Mary noted that the experiment ‘went good but it could have gone better, I can go again’. Mary reflected on how ‘I did it and I feel good’.
Evaluation
- What did you learn from the experiment? Mary emphasised that it is useful ‘to be prepared’ and ‘it is ok to stay talking longer than feeling comfortable with’ because this resulted in receiving additional information. Mary reflected on meeting with ‘Nice’ people and that ‘It was good to talk to them’ and ‘they were interested in art as well’. Mary highlighted that ‘I was interested to know what was happening’ and so there was authenticity within the experiment.
- What does this mean about your original belief or prediction? Mary reflected on how ‘it was grand’ to complete the experiment and that the original belief is not true.
- What is a more helpful or realistic belief or prediction? (Rate 0 -100%) Mary reflected on how ‘I am socially capable’. Mary noted her longstanding friendships and planned for a social night with her friends at the centre during the week.
It is noteworthy that throughout the intervention Mary engaged in social events with her siblings and friends, all of whom were present before the psychosis. These facts were utilized in order to challenge the cognition of being socially awkward. Mary noted that she was self-focused, which was not previously the case. It was highlighted that this can occur with psychosis. A goal was therefore set to focus on other people without becoming overwhelmed by other peoples’ stressors. This was practiced by questioning about events within her niece’s life.
4. STRENGTHS
At the midpoint of the therapy Mary completed the VIA personality inventory of strengths, which is derived from Positive Psychotherapy. This innovative therapy focuses on the person’s sense of self (personality) and the direct cultivation of subjective wellbeing. Mental health services are placing a greater emphasis on attending to the broader recovery of people who have experienced psychosis. The results highlighted enduring personality traits of being: honest, loving and grateful. This information was utilized to reinforce Mary’s mental health and to consciously set out behaviours activating strengths.
Outcomes
In line with CBT measurement, the level of anxiety was regularly tracked on a ten-point scale throughout the intervention, both as it was occurring each day and during the week. As detailed below the negative cognition of ‘I am useless’ was also monitored. It is noteworthy that there was a spike in the anxiety on a day when Mary was stressed in relation to organizing receipts.

At the tenth appointment Mary reflected on CBT and stated ‘I feel better’ as a result of the intervention. It was emphasized that ‘being in the here and now, relieved stress a lot’. The therapy was also beneficial in terms of knowing that ‘I am stable’, ‘safe and grounded’. Moreover, Mary noted that it was therapeutic to reinforce her traits of being ‘kind and reliable’, which aligns with the assertions to broaden CBTp in order to activate the positive schemas of clients. It was apparent that the level of anxiety decreased throughout the intervention. Mary’s thoughts became more present focused and her trust as well as communication with other people increased. Furthermore, Mary gained a greater understanding of the management of psychosis and how mental health/recovery is an ongoing process. Towards the end of therapy Mary was offered employment, yet decided not to take the post due to the stressors in traveling. However, she continued with this goal and was later employed within a local service. Attaining this goal is reflective of the increasing emphasis of attending to the social recovery with people with psychosis.
Discussion
Mary’s mental health improved from the intervention, specifically in relation to reducing the levels of anxiety as well as the intensity of the negative cognition. There were also benefits in delivering CBT with PPT. However, there were fluctuations within Mary’s presentation as perceived stressors occurred. This resulted in the re-emergence of the intensity of the maladaptive cognitive processes linked with the delusion. This was managed through the use of CBT interventions as well as the therapeutic relationship. As the therapy progressed the focus changed from reducing the anxiety and the associated cognition of being vulnerable, towards challenging automatic negative thoughts towards herself. This also reflected the psychological changes which were occurring within Mary as she was focusing on her goal of employment.
This process has reinforced the usefulness of CBT in formulating and documenting maladaptive cognitive processes as a way of monitoring when there is a negative change within the person’s mental health. It also reinforced the usefulness of activating cognition and a cognitive response in managing a crisis and an intensely emotionally distressing situation. However, Comfort notes that the crisis literature underestimates the importance of maintaining a dynamic and individual cognitive response. Nevertheless, during a mental health crisis people often rely on professionals in setting out care plans, each of which is tailored to the individual. Within the current context focusing on the present and cognitively setting out steps/a plan to achieve goals in the present resulted in improvements in mental health. However, questions still remain in terms of when is the most effective time to deliver CBT. Moreover, there are issues in identifying and challenging negative cognitions when there is a reduction in the person’s ego strength as well as the presence of a fixed/unwavering style of thinking. Mary presented with residual symptoms, whereby the intensity of the maladaptive cognitions increased with stressors, yet she was also capable of working through and activating adaptive processes.
The findings raise questions in relation to the role of the internet in influencing and triggering delusions, which is an emerging area of research. There is debate in relation to redefining the criteria pertaining to a delusion. On the one hand it is proffered that the defining criteria of a delusion remains the same and it is the content which changes, which often reflects collective issues/themes within the community such as espionage during World War Two. Currently there is an increase in people presenting to services with delusions centring on the internet, with the first case recorded in 1997. Alternatively, it is suggested that the advancement of the internet has resulted in the emergence of a new type of delusion, which requires redefining the criteria. There is further complexity present considering that people can join multiple online communities which hold diverse views which are not always reflective of the ideas within the local community. However, Stompe et al. highlight that it is the themes of: persecution, grandiosity, religion, hypochondria, guilt and love which have remained stable throughout time. Despite these issues there is evidence that internet use triggers and reinforces delusions, thus resulting in challenges in alleviating psychosis distress. Internet use may also cultivate: referential thinking, thoughts of being controlled as well as thoughts of being observed by other people. Moreover, the information on social media is not always reality based, which results in therapeutic challenges in realigning cognitions. In light of such issues there is debate in relation to the use of virtual reality with people with psychosis. This therapeutic medium could reinforce negative cognitive processes as well as social isolation whilst not orientating people to be present within the reality of day to day functioning. It could also cultivate illusions of embodiment and there could be issues in terms of personal autonomy. Alternatively, it may be a stepping stone in activating neural pathways, which could then be utilized in real life, in a similar process as imagined exposure is proven to do so. Research is currently emerging within this domain.
In considering the limitations of this case report, it pertains only to one person and the findings therefore cannot be generalized to other people. It may have been optimal to have administered a standardized measure that was specific to delusions. However, there is emerging evidence that with complex presentations it can be useful to tailor interventions to individuals, and to utilize idiosyncratic outcome measures which are meaningful to clients and which can measure subtle changes. This can include indicators of functioning and recovery. Another limitation may be the lack of direct family involvement. Whilst Mary communicated learnings from CBT with her next of kin, it may have been useful to invite significant others to an appointment so as to reinforce adaptive cognitive processes. It may have also been informative to measure the association between internet use and maladaptive cognitive processes, which could be explored with future research.
Conclusion
To conclude CBTp was found to decrease anxiety and the intensity of negative cognition whilst increasing functioning. Moreover, it was therapeutic to deliver PPT with a focus on attending to peoples’ strengths. Mary will continue to attend for CBTp and there will be a particular emphasis on repeating the material. Mary will also continue to receive evidenced based interventions within the team. Therapy will therefore continue to interweave: the person, the therapist, the therapeutic relationship as well as the CBTp framework, which is congruent with the therapist’s frame of reference. However, within this context the question still remains as to what is the specific factor with the most influence on the therapeutic outcome?
Conflicts of Interest Statement:
There is no conflict of interest.
Funding Statement:
There was no additional funding for this case report.
References
- Tarrier N, Haddock G, Barrowclough C, Wykes T. Are all psychological treatments for psychosis equal? The need for CBT in the treatment of psychosis and not for psychodynamic psychotherapy. Psychology and Psychotherapy: Theory, Research and Practice. 2002; 75, 4, 365-374. doi: 10.1348/147608302321151871
- Wykes T, Steel C, Everitt B, Tarrier N. Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor. Schizophrenia Bulletin. 2008; 34, 3, 523-537. doi: 10.1093/schbul/sbm114
- Freeman D, Emsley R, Diamond R, et al. Comparison of a theoretically driven cognitive therapy (the Feeling Safe Programme) with befriending for the treatment of persistent persecutory delusions: a parallel, single-blind, randomised controlled trial. The Lancet Psychiatry. 2021; 8, 8, 696-707. doi: 10.1016/S2215-0366(21)00158-9
- Sheffield J M, Brinen A P, Feola B, Heckers S, Corlett P R. Understanding cognitive behavioral therapy for psychosis (CBTp) through the predictive coding framework. Biological Psychiatry Global Open Science. 2024: 100333. doi:10.1016/j.bpsgos.2024.100333
- Freeman D, Freeman J, Ahmed M, et al. Automated VR therapy for improving positive self-beliefs and psychological wellbeing in young patients with psychosis: a proof of concept evaluation of Phoenix VR self confidence therapy. Behavioural and Cognitive Psychotherapy. 2024; 52,3, 277-287. doi: 10.1017/S1352465823000553.
- Newman‐Taylor K, Bentall, R. Cognitive behavioural therapy for psychosis: The end of the line or time for a new approach? Psychology and Psychotherapy: Theory, Research and Practice. 2024; 97,1, 4-18. doi: 10.1111/papt.12498
- Peterson C. A Primer in Positive Psychology. Oxford University: 2006.
- Health Service Executive. HSE Mental Health Division. The National Framework for Recovery in Mental Health 2024-2028. HSE; 2017.
- Hutton P. Positive clinical psychology and the promotion of happiness, compassion, and autonomy in people with psychosis. In Wood A M, Johnson J eds. The Wiley Handbook of Positive Clinical Psychology. Wiley: 2016: 245–260.
- McTiernan K, Gullon-Scott F, Dudley R. An exploration of strength use and its relationship with life satisfaction, positive self-beliefs and paranoid ideation. International Journal of Wellbeing. 2020; 10, 53-70. doi: 10.5502/ijw.v10i2.883
- Hall P L, Tarrier N. The cognitive behavioural treatment of low self esteem in psychotic patients: a pilot study. Behaviour Research Therapy. 2003; 41, 3, 317-332. doi: 10.1016/S0005-7967(02)00013-X.
- Seligman M E, Steen T A, Park N, Peterson C. Positive psychology progress: empirical validation of interventions. American Psychologist. 2005; 60, 5, 410 doi: 10.1037/0003-066X.60.5.
- Beck A, Beck J, Seligman M. Massive MAPP Meetup April 18 2020 https://www.mappmagazine.com. Accessed 02/09/2024.
- National Institute of Health and Clinical Excellence. Psychosis and Schizophrenia in Adults: Prevention and Management. National Institute of Health and Clinical Excellence. NICE; 2014.
- Psychological Society of Ireland. Code of Professional Ethics. Psychological Society of Ireland. PSI; 2019.
- Garety P A, Kuipers E, Fowler D, Freeman D, Bebbington P E. A cognitive model of the positive symptoms of psychosis. Psychological Medicine. 2001; 31, 2, 89-195. doi:10.1017/s0033291701003312
- Brabban A, Turkington D. The search for meaning: detecting congruence between life events, underlying schema and psychotic symptoms. In Morrison A P ed. A Casebook of Cognitive Therapy for Psychosis. Brunner-Routledge; 2002: 59-75.
- Greenberger D, Padesky C. Mind Over Mood: A Cognitive Therapy Treatment Manual for Clients. Guilford Press; 1995.
- Vivyan, C. Thought record. Get Self Help 2010: www.getselfhelp.co.uk/unhelpful.htm Accessed 02/09/2024
- Phillips, W. The Think CBT Workbook. Think CBT; 2024.
- Peterson C, Seligman ME. Character Strengths and Virtues: A Handbook and Classification. Oxford University Press; 2004.
- Rashid T, Seligman M. Positive Psychotherapy: Clinician Manual. Oxford University Press; 2018.
- McTiernan K, McCarthy O. A pilot investigation of the use of Positive Psychotherapy for people with a first episode of psychosis. J Schizophr Res. 2023; 9, 1, 1044. doi:10.26420/jschizophrres.2023.1044
- Fowler D, Garety R, Kuipers, E. Cognitive Behaviour Therapy for Psychosis: Theory and Practice. Wiley; 1995.
- Beck A T, Himelstein R, Grant P M. In and out of schizophrenia: Activation and deactivation of the negative and positive schemas. Schizophrenia Research. 2019; 203, 55-61 doi:10.1016/j.schres.2017.10.046
- Freeman D, Pugh K, Dunn G, et al. An early Phase II randomised controlled trial testing the effect on persecutory delusions of using CBT to reduce negative cognitions about the self: the potential benefits of enhancing self confidence. Schizophrenia Research. 2014; 160, 1, 186-192 doi:10.1016/j.schres.2014.10.038
- Fowler D, Hodgekins J, French P. Social recovery therapy in improving activity and social outcomes in early psychosis: current evidence and longer term outcomes. Schizophrenia Research. 2019;203:99-104 doi 10.1016/j.schres.2017.10.006
- National Institute of Health and Clinical Excellence. Service User Experience in Adult Mental Health: Improving the Experience of Care for People Using Adult NHS Mental Health Services. NICE; 2011.
- Comfort L K. Crisis management in hindsight: Cognition, communication, coordination, and control. Public Administration Review. 2007; 67, 189-197. doi 10.1111/j.1540-6210.2007.00827.x
- Shamim A, Banu S, Blassingame J, Guilford K L, Williams J. Delusions and fixed beliefs in the age of the internet: when do conspiracy theories become illness? Psychiatric Annals. 2023; 53, 4, 171-174. doi 10.3928/00485713-20230313-03
- Stompe T, Ortwein-Swoboda G, Ritter K, Schanda H. Old wine in new bottles? Stability and plasticity of the contents of schizophrenic delusions. Psychopathology. 2023; 36, 1, 6-12. doi 10.1159/000069658
- Cannon B J, Kramer L M. Delusion content across the 20th century in an American psychiatric hospital. International Journal of Social Psychiatry. 2012; 58, 3, 323-327. doi: 10.1177/0020764010396413
- Lerner V, Libov I, Witztum E. Internet delusions: The impact of technological developments on the content of psychiatric symptoms. Israel Journal of Psychiatry and Related Sciences. 2006; 43, 1, 47.
- Tan S, Shea C, Kopala L. Paranoid schizophrenia with delusions regarding the Internet. Journal of Psychiatry and Neuroscience. 1997; 22, 2, 143.
- Bell V, Grech E, Maiden C, Halligan P W, Ellis H D. ‘Internet delusions’: A case series and theoretical integration. Psychopathology. 2005; 38, 3, 144-150 doi:10.1159/000085845
- Madary M, Metzinger T K. Real virtuality: A code of ethical conduct. Recommendations for good scientific practice and the consumers of VR technology. Frontiers in Robotics and AI. 2016; 3, 3. doi: 10.3389/frobt.2016.00003
- Hoppe J M, Holmes E A, Agren T. Exploring the neural basis of fear produced by mental imagery: imaginal exposure in individuals fearful of spiders. Philosophical Transactions of the Royal Society B. 2021; 376, 1817, 20190690. doi: 10.1098/rstb.2019.0690
- Freeman D, Rosebrock L, Waite F, et al. Virtual reality (VR) therapy for patients with psychosis: satisfaction and side effects. Psychological Medicine. 2023; 53, 10, 4373-4384. doi:10.1017/S0033291722001167.
- Rus-Calafell M, Garety P, Sason E, et al. Virtual reality in the assessment and treatment of psychosis: a systematic review of its utility, acceptability and effectiveness. Psychological Medicine. 2018; 48, 3, 362-391. doi:10.1017/S0033291717001945.
- Freeman D, Yu L M, Kabir T, et al. Automated virtual reality (VR) cognitive therapy for patients with psychosis: study protocol for a single-blind parallel group randomised controlled trial (gameChange). BMJ open. 2019;9, 8, e031606. doi:10.1136/bmjopen-2019-031606.
- Dudley R, Aynsworth C, Cheetham R, McCarthy-Jones S, Collerton D. Prevalence and characteristics of multimodal hallucinations in people with psychosis who experience visual hallucinations. Psychiatry Research. 2018; 269, 25-30 doi:10.1016/j.psychres.2018.08.032