





Aspirin Use in Primary Prevention of Cardiac Events
Aspirin guided by coronary artery calcium scoring for primary prevention in persons with subclinical coronary atherosclerosis
Arthur J. Siegel, M.D.1,2,3
- Division of General Internal Medicine, Massachusetts General Hospital, Boston, MA, USA.
- Department of Internal Medicine, McLean Hospital, Belmont, MA, USA.
- Harvard Medical School, Boston, MA, USA.
Email: [email protected]
OPEN ACCESS
PUBLISHED: 28 Febuary 2025
CITATION: SIEGEL, Arthur J.. Aspirin guided by coronary artery calcium scoring for primary prevention in persons with subclinical coronary atherosclerosis. Medical Research Archives. Available at: <https://esmed.org/MRA/mra/article/view/6297>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i2.6297
ISSN 2375-1924
ABSTRACT
Coronary artery calcium scoring reliably identifies persons with subclinical coronary atherosclerosis who are at risk for major acute cardiac events. Aspirin guided by such enhanced risk stratification can be used to advance primary cardiovascular prevention. This approach has been recommended to prevent cardiac arrests in middle-aged men during marathons and sudden cardiac deaths during recreational sports activity in the elderly persons. These strategies are supported by demonstration of a 44% reduction in first heart attacks in healthy middle-aged men in decrease in major acute cardiac events in persons at moderate risk with the addition of aspirin to the polypill in the TIPS-3, which are both randomized controlled primary prevention trials. Beyond preventing sports-related exertional cardiac events, aspirin use guided by coronary artery calcium scoring may reduce the risk for major acute cardiac events in patients with conditions in which inflammation promotes progressive coronary atherosclerosis, such as autoimmune illnesses and infection with human immunodeficiency virus. This strategy may furthermore be applicable in general medical practice to identify persons with subclinical coronary atherosclerosis for enhanced primary prevention with aspirin in the absence of contraindications.
Keywords:
aspirin, cardiac arrest, sports activity, primary cardiovascular prevention.
THE EUROPEAN SOCIETY OF MEDICINE
Medical Research Archives, Volume 13 Issue 2
REVIEW ARTICLE
Aspirin guided by coronary artery calcium scoring for primary prevention in persons with subclinical coronary atherosclerosis
Marathons increase cardiac arrest risk:
While endurance exercise such as training for a marathon confers an overall cardioprotective benefit and perhaps enhances longevity, specific episodes of vigorous physical exertion such as marathon races transiently increase the risk for cardiac arrest and sudden death. A 10-year prospective registry of road races in the United States beginning in 2000 identified male gender and the marathon as significant and independent risk factors for cardiac arrest, which events increased significantly over time in runners with a mean age in the mid-40s. A concurrent retrospective review showed that fatalities occurred mainly in middle-aged men with subclinical coronary atherosclerosis, which condition is paradoxically promoted by endurance exercise as reviewed below.
Inflammation induced activation of atherothrombosis post-race:
An explanation for the adverse cardiovascular effects of marathon running in middle-aged men may emerge from a connection to findings in same-aged male physician-runners, who provided pre- and post-race blood samples at Boston marathons beginning in the 1970s. These asymptomatic middle-of-the-pack subjects crossed the finish line with elevated inflammatory biomarkers due to exertional rhabdomyolysis, initiating the same cytokine storm which occurs in patients at the onset of an acute myocardial infarction. Activation of atherothrombosis by exertional rhabdomyolysis was accompanied by a concurrent hemostatic imbalance with prothrombotic effects including in vivo activation of platelets. As if anticipating the demonstration of a pro-atherogenic inflammatory response demonstrated during SARS-CoV-2 infection in human coronary vessels, the pathogenic sequence of skeletal muscle injury leading to heart damage was advanced in a research study on runners in the inaugural Boston marathon in 1897.
Endurance exercise increases coronary artery calcium deposition:
In a 1800 paradigm shift from the viewpoint that marathon running confers virtual immunity from coronary heart disease, current evidence indicates that endurance exercise such as marathon training promotes coronary artery calcium deposition and its progression. While the clinical significance of such findings is regarded as inconclusive, race-related cardiac arrests in middle-aged men due to coronary atherosclerosis would indicate otherwise. The increased calcium burden consequent to the volume of training provides the background for acute coronary events triggered by activation of atherothrombosis during the intensity of races. Inflammation consequent to exertional rhabdomyolysis may lead to rupture of previously stable coronary plaque, as has been demonstrated at cardiac catheterization in patients after exertional cardiac arrests and in Boston marathon runners after races. Myocardial fibrosis demonstrated by magnetic resonance myocardial imaging in some older endurance athletes is an adverse consequence of underlying coronary heart disease.
Race-related acute coronary risk versus myocardial adaptations to endurance exercise:
The above considerations regarding coronary calcium burden in middle-aged men promoted by marathon training must be distinguished from findings which relate to transient myocardial dysfunction and release of cardiac-specific biomarkers including troponins in same-aged asymptomatic male participants after races. These latter transient findings are regarded as physiological adaptations to endurance exercise, which are non-ischemic and are not associated with acute events or long-term adverse cardiac effects. On this basis, some experts maintain that the net cardiovascular benefits of marathon running justify it as promoting heart health in middle-aged men, discounting concerns related to coronary artery calcium burden. Ongoing life-threatening cardiovascular medical encounters during marathons in South Africa from 2014 to 2019 led to an urgent call for novel preventive strategies.
Coronary artery calcium scoring provides enhanced risk stratification:
Gated coronary artery calcium CT scanning has been recommended to enhance risk stratification for male marathon runners, independently predicting the risk for major acute cardiac events including sudden death even in younger persons. Sequential coronary artery calcium scoring has furthermore been shown to reliably predict risk for all-cause including cardiovascular mortality. One-time coronary artery calcium score is well suited for pre-marathon preparticipation screening in men at middle-age and beyond, although the utility of this approach has been questioned due to the low frequency of index events. An incidence of 0.7 cardiac arrests per 100,000 participants was characterized as good news for marathon runners by some, albeit that this rate is 30-fold greater than that for which a black box warning was placed on azithromycin by the United States Food and Drug Administration.
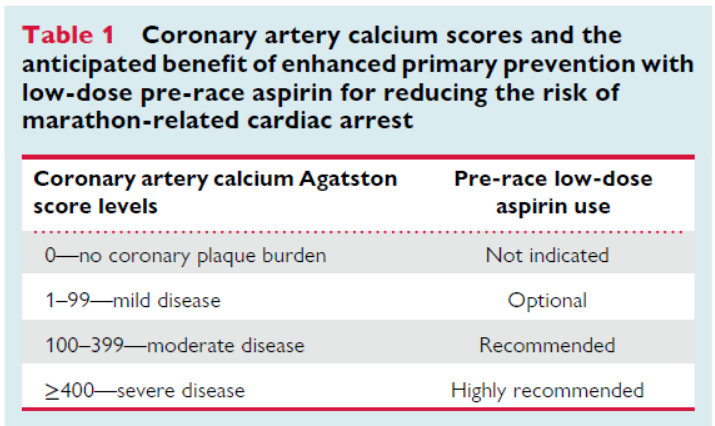
Aspirin to reduce marathon-related cardiac arrests:
Aspirin is undoubtedly effective due to its anti-inflammatory and anti-thrombotic effects. This measure is supported by a 44% reduction in first heart attacks in same-aged men in the TIPS-3 Study, a randomized controlled primary prevention trial. Compared to persons with coronary artery calcium scores <100 Agatston units, values >100 Agatston units confer an 85% increased likelihood of a major acute cardiac event including in younger persons. The anticipated benefit of this measure guided by coronary artery calcium scoring is shown in Table 1.
The strategy above is congruent with guidelines of the American College of Cardiology and the American Heart Association which endorse aspirin for primary prevention in those aged 40-70 years at high atherosclerotic cardiovascular disease risk in the absence of contraindications and has been robustly supported in current clinical evidence reviews. Once accepted by runners upon support from the sports medicine community, the efficacy of this intervention may be assessed prospectively for reducing cardiac arrest and sudden death in competitive and recreational athletes, as addressed in a review from the American College of Cardiology Sports and Exercise Leadership Council. It would qualify as poetic justice if a medicinal substance known to Hippocrates in the time of Pheidippides were to demise in the index event in 460 BC.
Beyond protecting marathon runners, aspirin use guided by coronary artery calcium scoring may reduce the age-dependent increasing incidence of sudden cardiac death during recreational sports activity in elderly persons. This similar recommendation is supported by a 31% reduction in major acute cardiac events in persons at moderate cardiovascular risk with the addition of aspirin to the polypill in the randomized controlled TIPS-3 prevention trial. Low-dose aspirin use during sports beyond middle age provides the additional benefit of having on board the only substance with a Class 1A recommendation by the American Heart Association for pre-hospital administration in acute coronary syndromes.
Aspirin for primary prevention beyond sports activity:
Beyond exercise-related considerations, aspirin use guided by coronary artery calcium scoring may benefit patients with conditions in which inflammation promotes progression of coronary atherosclerosis. Infection with human immunodeficiency virus and autoimmune disorders are diagnoses among others in which chronic inflammation promotes progressive coronary artery atherosclerosis. Asymptomatic patients with these disorders can be screened and monitored to identify those who might benefit from aspirin use for enhanced prevention. This strategy may also be relevant for patients with schizophrenia, which condition shares genetic links to cardiovascular disease risk factors and confers a four-fold increase in unexpected sudden cardiac death in those aged 18 to 35.
Based on a predominance of current clinical evidence, an emerging consensus would support aspirin use guided by coronary artery calcium scoring in general medical practice when counseling patients on strategies to promote heart health. A one-time determination in selected patients can provide prognostic information to guide treatment beyond results from conventional risk calculators. This approach may decrease some of the sudden cardiac deaths associated with unaccustomed high-intensity physical activity in daily life, which are currently the presenting symptom of coronary heart disease in up to 40% of cases. A primary care provider in the trenches may thus help reduce the burden of atherosclerosis, which is projected to increase until 2050 as forecast by the American Heart Association.
Conclusion:
Aspirin guided by coronary artery calcium scoring is evidence-based for primary prevention of major acute cardiac events in persons with subclinical coronary heart disease, reducing the risk for cardiac arrest and sudden death during sports activity at middle age and beyond.
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
None.
Take-away points:
- Endurance exercise such as marathon training promotes coronary artery calcium deposition.
- Marathon running increases cardiac arrest risk in middle-aged men with coronary atherosclerosis.
- Coronary artery calcium scoring independently stratifies acute cardiovascular risk.
- Aspirin significantly reduced acute cardiac events in two randomized controlled primary prevention trials.
- Aspirin guided by coronary artery calcium scoring is prudent for primary prevention of major acute cardiac events in persons with subclinical coronary atherosclerosis.
Disclosure:
The views expressed herein are solely those of the author and not attributable to any organizations with which he has been associated.
References:
- Veerman L, Tarp J, Wijaya R et al. Physical activity and life expectancy: a life-table analysis. Br J Sports Med 2024;0;1-6 DOI;10.1136/bjsports-2024-108125.
- Franklin BA, Thompson PD, Al-Zaiti SS, et al. On behalf of the American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Stroke Council. Exercise-related acute cardiovascular events and potential deleterious adaptations following long-term exercise. Downloaded from http://ahajournals.org by on March 3, 2020. Exercise-Related Acute Cardiovascular Events Circulation 2021;141(13):e705-e736.
- Kim JH, Malhotra R, Chiampas G, et al. Cardiac arrest during long-distance running races. N Engl J Med. 2012;366(2):130-40. doi:10.1056/NEJMoa1106468.
- Mathews SC, Narotsky DL, Bernholt DL, et al. Mortality among marathon runners in the United States, 2000-2009. Am J Sports Med. 2012;40(7):1495-500. doi:10.1177/0363546512444555.
- Siegel AJ, Silverman LM, Lopez MS. Creatine kinase elevations in marathon runners: relationship to training and competition. Yale J Biol Med. 1980;53:275-279.
- Siegel AJ, Stec JJ, Lipinska I, et al. Effect of marathon running on inflammatory and hemostatic markers. Am J Cardiol. 2001;88(8):918-20, A9. doi:10.1016/s0002-9149(01)01909-9.
- Kratz A, Wood MJ, Siegel AJ, Hiers JR, VanCott EM. Effects of marathon running on platelet activation markers. direct evidence for in vivo platelet activation. Am J Clin Pathol 2006.125:296-300.
- Eberhardt N, Noval MG, Kaur R, et al. SARS-CoV-2 infection triggers pro-atherogenic inflammatory response in human coronary vessels. Nature Cardiovascular Research 2023;2:899-916.
- Williams H, Arnold H. The effects of violent and prolonged exercise upon the heart. Phila Med J. 1897;1233-1235.
- Bassler TJ. Marathon running and atherosclerosis. B Med J. 1977.Jan 22;1(6055):229.
- Aengevaeren VL, Mostard A, Sharma S, et al. Exercise and coronary atherosclerosis: observations, explanations, relevance and clinical management. Circulation.2020;133-1350.
- Aengevaeren VL, Mostard A, Bakker EA, et al. Exercise volume versus intensity and the progression of coronary atherosclerosis in middle-aged men and older athletes: findings from the MARC-2 Study. Circulation. 2023.
- De Bosscher R, Dausin C, Claus P, et al. Lifelong endurance exercise and its relation with coronary atherosclerosis. Eur Heart J. 2023; httpsdl.d2Lu.gl.L0-U93.Leubeutjl.ghadJ52.
- Karam N, Pechmajou L, Dumas F, et al. Comprehensive assessment of coronary artery disease in sports-related sudden cardiac arrest. Circulation 2018;138:429-431.
- Albano AJ, Thompson PD, Kapur NK. Acute coronary thrombosis in Boston marathon runners. N Engl J Med. 2012;366(2):185-186.
- Karlstedt E, Chelvanathon A, Da Silva M, et al. The impact of repeated marathon running on cardiovascular function in the aging population. J Cardiovasc Magnetic Resonance 2012; 14:58-66.
- Mohlenkamp S, Lehmann N, Breuckmann F, et al. Running: The risk of coronary events. Eur Heart J 2008. 29; 1903 1910.
- Dores H, Goncalves PA, Cardim N, et al. Coronary artery disease in athletes: an adverse effect of intense exercise? Cardiologia 2017. https://doi.org/10.101/j.repc.2017.0.00
- Graziano F, Juhasz V, Brunetti G, et al. May strenuous endurance of sports activity damage to the cardiovascular system of healthy athletes question a narrative review. J Cardiovasc Dev Dis. 2022;9;347-369.
- Nielan TG, Januzzi JL, Lee-Lewandrowski E, et al. Myocardial injury and ventricular dysfunction related to training adequacy among non-competitive participants in the Boston Marathon. Circulation. 2006;114(22):2325-33.
- Zilinski JL, Contursi ME, Isaacs SK, et al. Myocardial adaptations to recreational marathon training among middle-aged men. Circ Cardiovasc Imaging 2015;8:e00247. Doi 10.111/CIRCIMAGING.114.00
- Baggish AL, Lavine BD. Coronary artery calcification Circulation.2017;136:147-151.
- Green D, Sewry N, Derman WF, et al. A high incidence of serious life-threatening cardiovascular medical encounters during a marathon (2014-2019) calls for prevention strategies: SAFER XL. Physician Sports Medicine 2024. Doi:10.1080/00913847.2024.2399495.
- Siegel AJ, Noakes TD. Aspirin to prevent sudden cardiac death in athletes with high coronary artery calcium scores. Am J Med. 2019;132:138-141.
- Nurmohamed NS, Min JK, Antopolos R, et al. Atherosclerosis quantification and cardiovascular risk: the ISCHEMIA trial. Eur Heart J. 2024 00; 1-13. https//doi.org/10.1093/eurheartj/ehae471.
- Razavi AC, Uddin SMI, Dardari ZA, et al. Coronary Artery Calcium for Risk Stratification of Sudden Cardiac Death: The Coronary Artery Calcium Consortium. JACC Cardiovasc Imaging. 2022;15(7):1259-1270. doi:10.1016/j.jcmg.2022.02.011.
- Fuchs A, Kuhl JT, Sigvardsen PE, et al. Subclinical Coronary Atherosclerosis and Risk for Myocardial Infarction in a Danish Cohort: A Prospective Observational Cohort Study. Ann Intern Med. 2023;176(4):433-442. doi:10.7326/M22-3027.
- Fuster V, Garcia-Alvarez A, Mass V, et al. Influence of subclinical atherosclerosis burden and progression on mortality. J Am Coll Cardiol Img. 2024; 84(15):1391-1403.
- Chandra N, Papadakis M, Sharma S, et al. Preparticipation screening of young competitive athletes for cardiovascular disorders. Phys Sports Med 2010.1(3):54-63.
- Holst AG, Wikel BG, Theilade J, et al. Incidence and etiology of sports-related sudden cardiac death in Denmark: implications for preparticipation screening. Heart rhythm 2010; 7: 1365 1371.
- Shirakawa T, Tanaka H, Kinoshi T, et al. Analysis of sudden cardiac arrest during marathon races in Japan. Internat J Clin Med.2017;8;472-480.
- Nearman S. Cardiac deaths in the marathons much lower than previously thought. AMAA Journal. Winter 2012: 7 8.
- FDA drug safety communication: Azithromycin (Zithromax or Zmax) and the risk of potentially fatal heart rhythms. U.S. Food and Drug Administration (2019). https://USFDA.org. Accessed Dec 20, 2024.
- Siegel AJ, Noakes TD. Can pre-race aspirin prevent sudden cardiac death during marathons? Br J Sports Med. 2017;51(22):1579-1582.
- Siegel AJ. Pre-race aspirin to protect susceptible runners from cardiac arrest during marathons: Is opportunity knocking? Open Heart 2015.2.e00010 2. doi:10.1136/openhrt-2014000102.
- Patrono C, Garcia-Rodriguez LA, Landolfi R, et al. Low-dose aspirin for the prevention of atherothrombosis. N Engl J Med 2005;353:22-29.
- Ridker P, Cushman M, Stampler MJ, Tracy RP, Hennekens CH. Inflammation, aspirin and the risk of cardiovascular disease in apparently healthy men. N Eng J Med..1997; 336:973-979.
- Steering Committee of the Physicians’ Health Study Research Group. Final report on the aspirin component of the ongoing Physicians’ Health Study; N Engl J Med. 1989;321(3): 129-35. doi:10.1056/NEJM198907203210301.
- Haq A, Veerati T, Walser-Kuntz T, et al. Coronary artery calcium and the risk of cardiovascular events and mortality in younger adults: a meta-analysis. Eur J Prev Cardiol 2023 Dec 19, 2023. https://doi.org/10.1093/eurjpc/zwad399.
- Siegel A. Pre-race aspirin to attenuate the risk for marathon-related cardiac arrest: deconstructing the legacy of Pheidippides. Eur Heart J. 2023, ehad641. https://doi.org/10.1093/eurheartj/ehad641 25.
- Siegel A. Rationale for pre-race aspirin to attenuate risk for marathon-related cardiac arrest: confounding the legacy of Pheidippides. Medical research archives (online) 11 (4). https://doi.org/10.18103/mra.v 1114.3741.
- Arnett DK, Claas SA. 2019 ACC/AHA Guideline for prevention of CVD. J Am Coll Cardiol 2019; 8(19):e01460.