

Improving Pediatric Type 2 Diabetes Outcomes with Dashboards
Electronic Dashboard and Strategies to Improve Outcomes in Pediatric Patients with Type 2 Diabetes Mellitus
Rob Gonsalves, D.O.¹; Vinay Vaidya, M.D.¹; Dorothee Newbern, M.D.¹; Maria Silva, M.H.A, R.D.N., C.D.C.E.S.¹; Yessica Chavez¹; Mary Kay Walsh, B.S.N., R.N.¹; Linda Black, B.S.N., R.N.¹; Chirag Kapadia, M.D.¹
- Phoenix Children’s Hospital, Phoenix, AZ
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Gonsalves, R., Vaidya, V., et al., 2025. Electronic Dashboard and Strategies to Improve Outcomes in Pediatric Patients with Type 2 Diabetes Mellitus. Medical Research Archives, [online] 13(9). https://doi.org/10.18103/mra.v13i9.6933
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.6933
ISSN 2375-1924
ABSTRACT
Background: In the last decade, the prevalence of Type 2 Diabetes Mellitus (T2DM) has dramatically increased in children and adolescents. This population is at increased risk of long-term complications compared to those diagnosed in adulthood.
Methods: A comprehensive program was developed to help manage our patients with T2DM. The healthcare team is comprised of multiple members and utilizes both manual and electronic tools, including a PowerBI electronic dashboard with data integration to the Electronic Medical Record (EMR), to optimize care. Goals included reducing hemoglobin A1c (A1c), increasing communication, and decreasing frequency of missed visits. A quality nurse was assigned to monitor this disease state, and, because of the capacities of the technology, she was able to monitor population health in this disease state, and 5 others, at the same time.
Results: The percentage of newly diagnosed patients who achieved an A1c less than 8.0% within 6 months improved from 42% to 80%. Outpatient follow-up 10 weeks after diagnosis increased from 57% to 72%. After implementation of an electronic dashboard, our total patient population with A1c of less than 8% improved from 55% to 59%, and total missed appointments decreased from 40% to 23%.
Conclusions: Manual tracking and utilization of an electronic dashboard resulted in significant improvement of care in our patients with Type 2 diabetes. Electronic dashboards provide a low-cost and efficient way to better understand clinic demographics and track improvements for a specific patient population. Efforts should focus on increasing communication and continuity of care for pediatric patients with Type 2 diabetes, given its increasing prevalence and impact on patient wellbeing and the healthcare system.
Keywords
Type 2 Diabetes Mellitus, pediatric patients, electronic dashboard, healthcare outcomes, A1c, missed appointments
Introduction
The prevalence of Type 2 Diabetes Mellitus (T2DM) has dramatically increased in children and adolescents in the last decade. Quality of care for these patients is directly related to the frequency of correspondence between the patient or family and the multidisciplinary diabetes team, which typically includes a physician or clinician, a Certified Diabetes Care and Education Specialist (CDCES), a registered dietitian, and a psychologist or social worker. Per standard of care, these patients should be seen several times per year.
Evidence shows that pediatric-onset T2DM progresses more rapidly than adult-onset T2DM, which puts this population at increased risk of complications. This is compounded by more variable glycemic control due to hormonal changes, socioeconomic factors, peer influence, emotional factors, and more limited treatment options compared to adults. Overall, risk of long-term complications is higher and presents more rapidly in pediatric-onset T2DM.
Locally, at Phoenix Children’s, a pediatric tertiary care in Phoenix, Arizona, the incidence of new diagnoses of T2DM more than doubled within several months following the onset of the coronavirus disease 2019 (COVID-19) pandemic. Similar increases have been noted in many pediatric centers nationally and globally. It is thought that a combination of COVID-19 infections, which can affect insulin-producing pancreatic beta cells, and the pandemic’s negative impact on lifestyle such as reduced activity and poor diet may have played a role.
At Phoenix Children’s, we currently care for approximately 450 patients with T2DM, though the number making it to an appointment each year is closer to 400. Not adhering to scheduled routine care visits is a major issue, with approximately 40% of patients missing a follow-up appointment in 2022. A missed follow-up appointment is defined as no appointment within 90 days after the previous one, together with also having no future scheduled appointment. This often results in reduced or non-existent follow-up care.
Starting in early 2022, we set out to use both manual and automated data-gathering methods to optimize care for this population. This manuscript is a description of several rounds of progressive efforts to improve continuity of care for patients with T2DM per standard of care at our institution. The principles of quality improvement, specifically continuous and systematic data-driven actions, were used to develop and implement our interventions and monitor our progress. The presence of a quality nurse monitoring several Endocrine disorders including Type 2 diabetes, was one of the key interventions.
Methods:
Our primary aims initially, when we started in 2022, were to decrease the A1c of newly diagnosed patients and re-establish care of high-risk patients, specifically those with an A1c greater than 9.5% with a missed follow-up appointment. To this end, we developed a program designed at scheduling close follow-up outpatient appointments for patients with newly diagnosed T2DM requiring admission for insulin treatment. It was modeled after a successful program conducted in our Type 1 Diabetes (T1DM) population. Upon admission, the T2DM program coordinator systematically schedules two follow-up outpatient visits, the first at four weeks and the next at ten weeks post-discharge. A CDCES is also assigned as a “coach” to provide close support for the patient and family until the first scheduled appointment. Patients are also scheduled for virtual diabetes self-management training group classes taught by the CDCES team. For our second aim, we generated lists of patients with missed appointments and A1c greater than 9.5%. Missed appointments were defined as having no appointments for 90 days PLUS having nothing set up for the future either. These were then shared by our quality nurse with our scheduling team to assist with scheduling a follow-up visit. Much of what was done in 2022 was manual, using excel spreadsheets, and a lot of staff labor through EMR chart reviews.
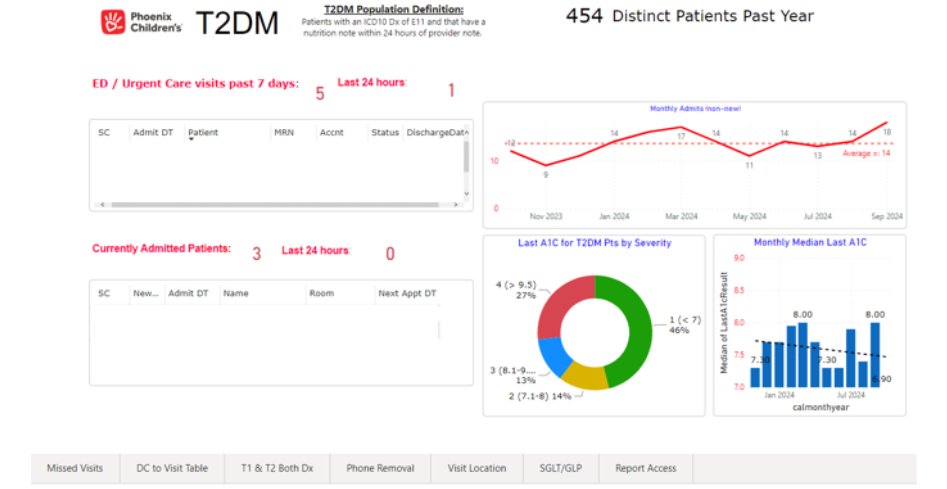
After some modest progress in 2022, we adjusted our aims and methods based on our initial results and experience. In 2023, we adjusted our aims to focus on established patients more, to increase the net percentage of total patients with an A1c of 8% or less, while still focusing on reducing missed appointments. To do this, we created an electronic PowerBI dashboard (Figure 1), with data integration to our EMR, that facilitated our work. This dashboard was modeled after a successful dashboard we developed for our T1DM population, which is described in more detail in an article previously published.
The PowerBI dashboard is linked to our electronic medical record (EMR) and identifies patients with a diagnosis of T2DM. The dashboard contains multiple tabs that help us sort data by category. Figure 1 depicts the general overview tab that shows patients who have visited one of our emergency departments or urgent cares in the past 24 hours, as well as patients who are currently admitted to the hospital. It additionally tracks our monthly admissions, last outpatient A1c, and our monthly median A1c. This is our general ‘quality tab’ we use to monitor our program and the population health of the T2DM patients we care for.
The “Missed Visits” tab, which is a separate section, generates a list of patients with a missed follow-up appointment (as defined above), and shows when they were last seen in clinic by which provider. We act on this list through both electronic (text) and manual (call) methods to try to get their care re-established. The “DC to Visits” tab generates a list of all patients discharged within the past 30 days and the date of their outpatient follow-up appointment, to ensure that nobody is being hospitalized without appropriate post-hospital follow-up. We run this list monthly, and if anyone is noted to have not had an appointment set up, we contact them.
Other tabs provide information pertaining to patients who have been prescribed glucagon-like-peptide 1 (GLP-1) agonists and sodium/glucose transporter 2 (SGLT-2) inhibitors, to help us understand the characteristics of these patients and to understand why some patients with T2DM who meet indication are not yet on these medications.
The dashboard contains a feature that allows us to send text messages directly to patients and families to facilitate scheduling and continuity; these text messages include the ability to ‘click to schedule.’ Furthermore, to help increase access and availability, we created evening telehealth visits for this population. Lastly, an incentive with small value ($5) gift cards, provided by a donor, were given to patients who demonstrated increased effort and adherence including improving their T2DM care.
Results:
Table 1 outlines some of our patient demographics, and our education efforts. We saw a total of 393 patients in 2023, with 45% having a BMI ≥ than the 99th percentile, and 23% between the 95th and 99th percentile. Number of patients on insulin in the prior 6 and 24 months is also presented. This shows that patients are gradually able to come off insulin post-diagnosis, especially with greater use of newer therapeutic agents such as GLP-1 or SGLT-2.
| Data derived from T2DM Dashboard | Number (%) |
|---|---|
| Total distinct patients seen in 2023 | 393 |
| Patients with BMI 95th-98th percentile | 91 (23%) |
| Patients with BMI ≥ 99th percentile | 175 (45%) |
| Patients on insulin in the prior 6 months | 110 |
| Patients on insulin in prior 24 months | 235 |
| Total phone notes in prior 24 months | 2745 |
| Total education encounters in prior 24 months | 1432 |
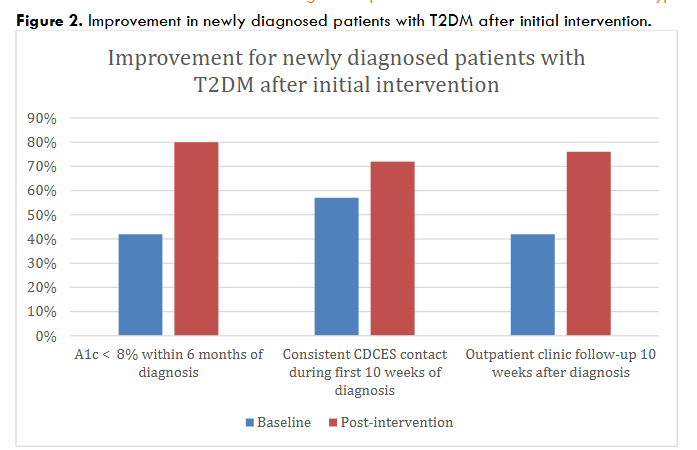
Our 2022 efforts showed modest progress. Our most significant improvement came from newly diagnosed patients and is depicted in Figure 2. The percentage of patients who achieved an A1c below 8.0% within 6 months of diagnosis increased from 42% to 80% with these initial interventions in 2022. The percentage of patients following with their CDCES coach over the 10 weeks after new diagnosis increased from 42% to 76% and those who attended their 10-week follow-up appointment increased from 57% to 72%.
Our initial efforts did not result in significant improvement for patients with longstanding T2DM. The number of missed follow-up appointments for established patients with an A1c > 9.5% remained unchanged at approximately 50% by year end, and for all patients it remained near 40%.
The percentage of patients with an A1c less than 8% at their latest visit in 2022 stayed near 55%.
We had better results on established patients after implementation of our dashboard and electronic reports. The percentage of all patients with A1c less than 8% increased from 55% to 59%, and the percentage of established patients with missed appointments decreased from approximately 40% at end of 2022, to 23% at the end of 2023 (102 missed visits for 440 patients).
Discussion
Manual tracking by our CDCES team for patients with newly diagnosed T2DM resulted in significant improvement in A1c and follow-up visit adherence. These methods were less effective for established patients with an A1c > 9.5%.
The development of a dashboard with automated data gathering and innovative contact methods followed in 2023 onwards, and this resulted in improvements beyond just the new-onset period, with established patients showing an increase in those with an A1c < 8% and significant decrease in missed patient visits in this population as well.
The PowerBI dashboard has also helped us better characterize our T2DM population regarding A1c stratification, insulin needs, and body mass index (BMI) percentage. It also helped track our number of phone and education encounters.
Simply being able to understand the characteristics of our population has helped inform our clinicians’ practice patterns.
We can now keep track of recently hospitalized patients, ensuring they return for outpatient follow-up clinic visits, and make early identification of missed visits, so efforts can be made to re-establish care before too much time has passed.
We are able to utilize a quality nurse in this effort, and she is monitoring 5 other disease states other than Type 2 Diabetes at the same time, as well. Having one nurse monitor population health on 5 Endocrine disease states shows how the technology allows efficiencies of scale. We have published separately on some other areas where similar technologies have been used, such as congenital hypothyroidism (manuscript in process), and T1DM.
Conclusions:
PowerBI Electronic dashboards are a low-cost, efficient, and sustainable way to better understand clinic demographics and needs of a specific patient population. This information can then be used to implement interventions and track improvement with the ultimate goal of improving patient care.
Our overall experience is that the T2DM population is harder to improve care on, despite efforts, at a population health level, than our T1DM population, despite employment of similar data tools and levels of staff effort.
The next phase of our project is aimed at identifying patients for newer pharmacotherapy options such as glucagon-like-peptide 1 (GLP-1) agonists and sodium/glucose transporter 2 (SGLT-2) inhibitors. Our hope is that as we continue to sustain our current efforts and increase the use of these new medications, we will see continued improvement of A1c, decrease in percentage of patients requiring insulin therapy, and overall improvement of patient health and wellbeing.
Acknowledgements:
We would like to thank the Pinkus family for the generous grant that helped support our quality work 2022 through 2024.
Conflict of Interest Disclosures:
The authors have indicated they have no potential conflicts of interest to disclose.
Credit Author Statement
Conceptualization: Rob Gonsalves, Chirag Kapadia, Vinay Vaidya
Methodology: Rob Gonsalves, Chirag Kapadia, Maria Silva
Software: Vinay Vaidya
Validation: Dorothee Newbern, Maria Silva
Formal analysis: Chirag Kapadia, Vinay Vaidya
Investigation: Rob Gonsalves, Yessica Chavez, Mary Kay Walsh
Resources: Linda Black, Yessica Chavez
Data Curation: Maria Silva, Yessica Chavez
Writing – Original Draft: Rob Gonsalves, Chirag Kapadia
Writing – Review & Editing: All authors
Visualization: Vinay Vaidya
Supervision: Vinay Vaidya, Dorothee Newbern
Project administration: Rob Gonsalves, Maria Silva
Funding acquisition: Not applicable
Declaration of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this manuscript titled “Electronic Dashboard and Strategies to Improve Outcomes in Pediatric Patients with Type 2 Diabetes Mellitus”.
References
- ElSayed, N. A., Aleppo, G., Aroda, V. R., Bannuru, R. R., Brown, F. M., Bruemmer, D., Collins, B. S., Hilliard, M. E., Isaacs, D., Johnson, E. L., Kahan, S., Khunti, K., Leon, J., Lyons, S. K., Perry, M. L., Prahalad, P., Pratley, R. E., Seley, J. J., Stanton, R. C., & Gabbay, R. A. (2023). Children and adolescents: Standards of care in diabetes—2023. Diabetes Care, 46(Suppl 1).
- Xu, H., & Verre, M. C. (2018). Type 2 diabetes mellitus in children. American Family Physician, 98(9), 590–594.
- Haines, L., Wan, K. C., Lynn, R., Barrett, T. G., & Shield, J. P. H. (2007). Rising incidence of type 2 diabetes in children in the U.K. Diabetes Care, 30(5), 1097–1101. https://doi.org/10.2337/dc06-1813
- Narasimhan, S., & Weinstock, R. S. (2014). Youth-onset type 2 diabetes mellitus: Lessons learned from the TODAY study. Mayo Clinic Proceedings, 89(6), 806–816. https://doi.org/10.1016/j.mayocp.2014.01.009
- Fotea, S., Ghiciuc, C. M., Stefanescu, G., Cianga, A. L., Mihai, C. M., Lupu, A., Butnariu, L. I., Starcea, I. M., Salaru, D. L., Mocanu, A., Chisnoiu, T., Thet, A. A., Miron, L., & Lupu, V. V. (2023). Pediatric COVID-19 and diabetes: An investigation into the intersection of two pandemics. Diagnostics, 13(14), 2436. https://doi.org/10.3390/diagnostics13142436
- Sandblom, L., Kapadia, C., Vaidya, V., Chambers, M., Gonsalves, R., Holzmeister, L. A., Hoekstra, F., & Goldman, S. (2024). Electronic dashboard to improve outcomes in pediatric patients with type 1 diabetes mellitus. Journal of Diabetes Science and Technology, 18(5), 1102–1108. https://doi.org/10.1177/19322968231159401
- Buonalumi Tacito Yugar, L., Sedenho-Prado, L. G., Castilho da Silva Ferreira, I. M., Moreira Silva, C. A., Sposito, A. C., & Cercato, C. (2024). The efficacy and safety of GLP-1 receptor agonists in youth with type 2 diabetes: A meta-analysis. Diabetology & Metabolic Syndrome, 16, Article 92. https://doi.org/10.1186/s13098-024-01337-5
- Huang, A., Roberts, A., Mohsenian, Y., & Kim, G. (2025). Improving prescribing rates of glucagon-like peptide 1 receptor agonists in youth with type 2 diabetes. Clinical Diabetes, 43(3), 429–434. https://doi.org/10.2337/cd24-0070
- Klinkhammer, A. (2023). The efficacy of GLP-1 agonists in pediatric patients with type 2 diabetes: A literature review. University of North Dakota Physician Assistant Scholarly Project Papers, 200. https://commons.und.edu/pas-grad-papers/200/