

Eidetic Model of Growth for Intellectual Disabilities
The Theory and Practice of the Eidetic Model of Growth for People with Intellectual Disability: A Clinical Review
Akhtar Ali Syed¹ PhD, ADCP, CIT. C. Psychol. PsSI and Shazia Neelofur² PhD, ADCP, CIT. C. Psychol. PsSI
- Principal Clinical Psychologist Brothers of Charity South East, Waterford, Ireland
- Principal Clinical Psychologist, Brothers of Charity South East, South Tipperary, Ireland.
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Syed, A. A. and Neelofur, S. 2025. The Theory and Practice of the Eidetic Model of Growth for People with Intellectual Disability: A Clinical Review. Medical Research Archives, [online] 13(9).
https://doi.org/10.18103/mra.v1i9.6836
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v1i9.6836
ISSN 2375-1924
ABSTRACT
Background: The Eidetic Model of Growth (EMG) is the only imagery-based form of psychotherapy for people with intellectual disability (PWID). It is an adaptation of Akhter Ahsen’s Eidetic Psychotherapy. It consists of two distinct parts. One, carried out by staff, contributes to the creation of a therapeutic environment that encourages people with intellectual disabilities to engage in meaningful and skill-enhancing activities of their choosing while protecting them from environmental stresses. The second arm is intended to provide therapeutic support in overcoming experiential, emotional, and deep-seated traumatic experiences. This review, though, focuses on the therapeutic arm of EMG.
Aim and Scope: The purpose of this review is to provide a fundamental understanding of eidetic theory and how consciousness functions in PWID, stressing the similarities and differences between them and typically developing individuals. With a theoretical basis, this review examines five cases of various prevalent difficulties in the ID population to explain the procedures and efficacy of techniques evolved in EMG.
Outcome: The appraisal of five cases suggests that EMG approaches are effective in addressing chronic behavioural and emotional issues, corroborating the eidetic theory regarding how consciousness functions in PWID.
Implications: Firstly, this review attempts to highlight the theoretical comparison between how consciousness functions in PWID and typically developing individuals. Secondly, it explains how eidetic theory when comes into therapeutic format, produces remedial outcomes. This review presents a theoretical framework, scientific evidence for imagery-based psychotherapy for PWID, and therapeutic procedures based on five cases of varying difficulty and ability. Thirdly, it indicates the potential of PWID to receive psychotherapy to overcome the chronic issues deeply rooted in their developmental and experiential history. Fourthly, it indicates at the potential of eidetic imagery to generate remedial outcomes in those with language barriers. This way, multi-layered theoretical and therapeutic implications of EMG are attempted to highlight.
Keywords: intellectual disability, psychotherapy, eidetic model of growth, imagery.
1. Introduction
Eidetic Psychotherapy is adapted into the Eidetic Model of Growth (EMG) for people with intellectual disability (PWID) and related issues. This adaptation aims to help PWID overcome behavioural and mental health issues and grow psychologically, emotionally, and cognitively.
Initially it was developed to support ID service personnel who work with people who have extreme aggression, self-injurious behaviour (SIBs), and inappropriate social behaviour, sometimes called as challenging behaviour. These services support PWID and related problems, including verbal, physical, medical, and mental health concerns. As experienced psychologists and psychotherapists are scarce, EMG therapies were adapted to train lay therapists to fulfil the high demand. The EMG also helped frontline staff create a therapeutic environment to lessen behavioural issues. Intellectually disabled people helped achieve this goal by participating in meaningful and skill-building activities. As indicated by Behaviouristic Models, the EMG uses Eidetic Imagery and avoids reinforcement to achieve this purpose. EMG is person-centred and good for personal growth.
The Eidetic Model of Growth is the first to use imagery-based psychotherapy for PWID. This method has showed potential and efficacy in addressing mental disorders, trauma of sexual abuse, bereavement-related emotional issues, and deinstitutionalisation.
Notwithstanding other psychotherapy approaches, Eidetic Psychotherapy is easier to deliver to PWID than to those with typically developing individuals (TDIs), because PWID do not have the complexities TDIs generally have and make the therapeutic work complicated.
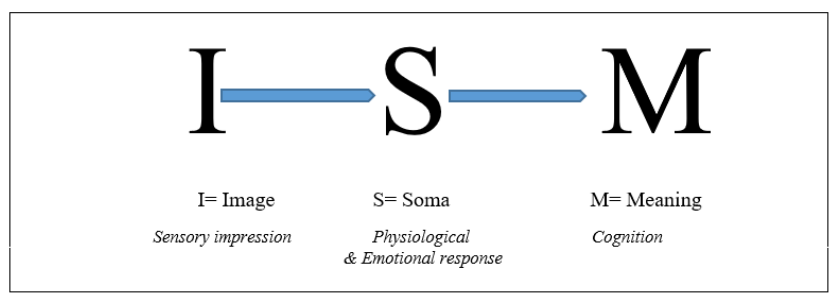
The essential part of Ahsen’s work is his definition of eidetic imagery. According to him, emotionally significant experiences are stored in the brain as eidetic images carry all intricate sensory, physiological, and cognitive details tied to our experiences. Thereby, they shape our consciousness. He not only offered a new definition, but also established its tripartite structure (ISM).
1.1 EIDETIC PSYCHOTHERAPY OF AKHTER AHSEN
Eidetic Psychotherapy (EP) was founded by Akhter Ahsen (1933-2018). This is the only psychotherapy model that utilizes eidetic imagery in therapeutic manner. The EP claims to promote growth, healing, and transformation beyond therapeutic procedures. In the 1950s, Ahsen, a pioneer in imagery-based psychotherapy, introduced the structure of eidetic imagery; the ISM model, which states that eidetic images include imagery, somatic response, and meaning. This triadic paradigm helps people overcome emotional and cognitive challenges if the ISM model is executed as described in EP.
The core of Eidetic Psychotherapy (EP) is an eidetic image, a vivid mental representation. Eidetic image redefined by Ahsen. His definition was a complete departure from the traditional definitions of mental imagery as a higher cognitive function and eidetic image as a joint venture of cognition and perception. Ahsen distinguished his structural definition from Jaensch’s typographic one. Ahsen’s definition differed from the literal definition of eidetic image, which is a photographic image that is a detailed representation of a stimulus and stays in mind longer than an after image. It is rare, estimated to exist in five in 100 children and less than one in 1000 or even one in a million adults. Ahsen defined eidetic image uniquely. Ahsen described eidetic imagery as a normal subjective visual image with high vividness that may or may not be evoked by a real experience. Eidetic imagery generates cognitive and physiological changes. Thus, Ahsen’s structural eidetic brought sensory, physiological, and cognitive outcomes, all together.
Eidetic images, unlike pathological images, are natural and foster psychological growth. Ahsen explained these images are microcosms of important life challenges, exposing narratives that move from superficial perceptions to deep insights and often use dramatic conclusion like theatrical or artistic expression. Every significant experience is recorded in an ISM format, hence the record of all the difficult and traumatic experiences are kept not by the mind but human brain, according to Ahsen. The tripartite model of ISM not only provides the theory of consciousness but also the theory of disorder in EP.
1.2 THEORY OF DISORDER IN AHSEN’S MODEL
Ahsen’s theory of disorder is based on his ISM model. In eidetic theory of Ahsen, emotionally significant experiences either actual or imagined, personal or primordial are at the core of development of disorderly presentation. Stressful or painful (mental or imaginary) experiences trigger automatic triadic recording. This recording naturally shapes up in the ISM format to cause the sensory input and somatic (emotional) and cognitive outcomes. Imagery researchers other than Ahsen agree that consciousness stores stressful/painful experiences. Kosslyn (2005) found that high levels of cerebral activity during visualisation can influence larger physiological systems. He explained how stressful images persist in consciousness and exacerbate psychopathology. A traumatic experience leads to emotionally charged perceptual information being stored, which in turn, can produce mental images that evoke many of the same hormonal reactions as did the actual experience. These stress reactions can disrupt normal thinking, and over the long run could possibly even damage the brain. Images help processing all critical experiences, which is why Ahsen believes they are crucial to psychopathology’s development and treatment. Holmes and Mathews reported similar results. They pointed out mental imagery’s link to emotions and emotional illnesses. Since imagery is linked to sensory information, memory, and perception, they suggested it might affect the emotional system. Second, recent evidence shows that images evoke stronger emotions than words. They also discussed how visualisation helps alleviate emotional disorders. Some researchers found that images arouse emotions more than words. Another study revealed imagery’s crucial but understudied function in several mental diseases like PTSD, agoraphobia, body dysmorphic disorder, psychosis, and mood disorders. Therapists utilise imaginal reliving to treat PTSD, not simply flashbacks.
Due to their strong emotional associations, images might cause certain disorders. For example, intrusive mental images can cause serious depression. The negative imagery and its vividness are handled by posterior cingulate gyrus (PCG), which is a part of the brain within the cerebral cortex. The vividness fluctuates with emotional intensity of images. It is metabolically active and linked to various structures in brain. Recent research suggests that PCG controls cognitions during focused tasks. Understanding PCG cognitive function in generating imagery outcome may be clinically relevant. The imagery relationship with a multifunctional brain area explains its importance beyond psychology. In a study it was found that mental imagery contributes to agoraphobia. Similarly, positive prospective imagery vividness was found linked with current and future optimism. The degree of optimism may possess predictive significance regarding the management of cardiovascular illnesses and depression. Another study confirmed the role of positive imagery in treating anxiety and serious depression. Ahsen predicted that understanding image’s function in psychopathology and its treatment will surpass psychology and psychotherapy into neuroscientific study. Following the same pattern neuroscience researchers are finding more evidence that imagery consolidates autobiographical (trauma) memory, involuntary recall, negative emotions, and attention hijacking in intrusive memory in those with PTSD.
In a nutshell imagery is now being considered as one of the key pathogenic and therapeutic factors as Ahsen theorised in 1960s. Ahsen has developed a well-established procedure of an applicable techniques of psychotherapy exploring the multidimensional potential of imagery.
1.3. THERAPEUTIC PROCEDURES
Eidetic Psychotherapy alters junctional behaviour, a term coined by Ahsen to describe the neuropsychological equilibrium underlying behavioural patterns, by repetitively and intensively activating eidetic imagery. Eidetic interrupts inflexible neurotic patterns and promotes life-affirming behaviours, healing emotions and changing cognition.
The first stage in Eidetic psychotherapy is to catalogue symptoms. The therapist uses a systematic interview to identify physical and psychological symptoms. The client is also asked about concerns in relation to symptoms related difficulties. Anxieties, concerns related to body part, and other worries are also noted. Symptoms are written in client’s verbatim. Significant biographical information is also collected. This historical and biographical data collection is done following Age Projection Test. This method usually reveals an event that created the illness in TDIs and leads to resurfacing a chain of events that led to symptoms composite. However, the process is especially simpler in people with ID. The client is instructed to repeatedly visualise themselves during this surfaced experience until it becomes clear. The visual, experiential, or eidetic image incorporates all sensory, physiological, and cognitive elements of the event. Syed and colleagues found that eidetic images can help PWID to lose the severity of symptoms and their debilitating nature.
The EMG detects and mitigates environmental, emotional, and developmental disturbances. It emphasises choice, planned activities, and meaningful interaction, which reduce tension and stimulate development beyond skill learning. In contrast to behaviouristic models, EMG relies on intrinsic motivation rather than reinforcement, which is stimulated by environmental interaction facilitated through eidetic imagery.
2. Eidetic Model of Growth (EMG) for people with intellectual disabilities
Intellectual disability research and policy advances reinforce the Eidetic Model of Growth theoretical emphasis. The EMG inherently includes the five AAIDD-recommended ideas to help PWID. In The Renaming of Mental Retardation: Understanding the Change to the Term Intellectual Disability, Schalock et al. explained the key changes. This document confirms that suitable individualised support over an extended duration, the life functioning of individuals with intellectual disabilities typically enhances.
Similar to Schalock et al, EMG stated that disability is no longer static and unchallengeable construct. Dual support is needed for intellectually disabled people. The support must help surmount the obstacles contributing to their learning deficiencies. Second, they need help with emotional and experiential challenges since they are more susceptible than TDIs.
Theoretically, the triple code model (ISM) of experience, eidetic theory refers to growth from the pathological complexes. Eidetics are normal subjective visual images (I) with significant vividness that are not necessarily prompted by an external stimuli or prior experiences of a real situation. The seeing is accompanied with a bodily response (S) and meaning (M) whether the individual is aware or not. All aspects of this experience preclude pathology. G. W. Allport developed a model that emphasised the healthful aspects of eidetic phenomena after a thorough literature review. Ahsen believes the eidetic includes all development and transition factors. Syed derived two inferences from this idea. One, the application of eidetic imagery is not confined to psychopathology. Second, past successes and failures shape our future. This helps the learning about the environment and its demands. Eidetic learning occurs organically during growth if emotional, experiential, or environmental elements do not obstruct it.
The EMG uses two methods to identify and correct developmental abnormalities in intellectually disabled people. One part detects contextual factors that cause dread and mistrust of the environment and a refusal to participate. The second arm addresses emotional and experiential issues like abuse and attachment difficulties.
2.1. ADAPTATION OF EIDETIC PSYCHOTHERAPY (EP) FOR INDIVIDUALS WITH INTELLECTUAL DISABILITIES
The EMG is a modified version of EP developed for PWID to help them grow and overcome emotional and experiential problems. This modification addressed two theoretical issues: how ISM might apply to cognitively impaired people and whether PWID can experience the eidetic image. These theoretical concerns were addressed theoretically and empirically.
2.1.1. ISM and intellectual disability
The ISM stands as a nucleus of eidetic theory, the M stands for the cognitive aspect. The theory of EMG acknowledges the restricted development of cognitive component in PWID. That is why the structure of ISM is depicted as ISm. Small-case m indicates limited cognitive development and functioning. This ISm model compares and contrasts PWID and the TIDs.
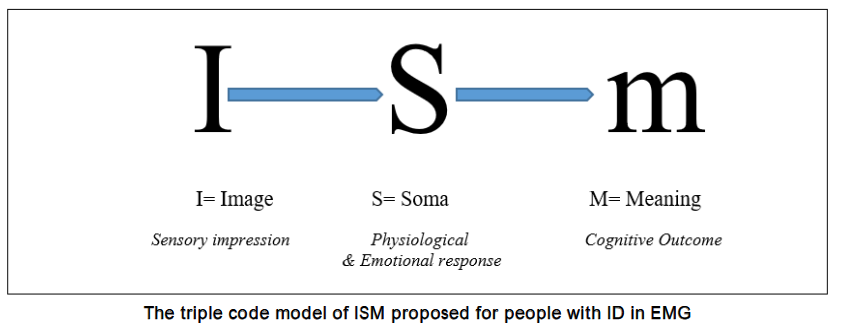
Eidetic theory states that PWID receive the sensory impression of their experiences and are affected physiologically and emotionally like typically developing individuals (TDIs). The only distinction they have is their inability to understand them owing to delayed cognitive development. Therapy in EMG is based on this formulation. Syed states that Eidetic Therapy is simpler, more successful, and less challenging for PWID than for TDIs. This claim, however, needs evidence that PWID with their cognitive deficit can experience eidetic imagery like TDIs do.
2.1.2. People with intellectual disability and Eidetic Imagery
Imagery was mostly deemed one of the high cognitive function in popular imagery literature. This widespread description raises questions about whether PWID due to their cognitive deficits can experience imagery or benefit from imagery-based therapy. It’s crucial to determine the viability and efficacy of imagery-based therapy (EMG). The study by Syed, Neelofur, Moran, and O’Reilly examined this subject. They compared mental and eidetic imagery vividness in people with mild, moderate, and severe ID with TIDs. Individuals with mild and moderate ID counterintuitively not only performed well on mental imagery and eidetic imagery vividness tests but the group was not significantly different from TIDs. However, people with severe ID performed lower than the rest of three groups, though they showed the ability to perform on both types of imagery tests. Furthermore, neurological findings confirmed that the vividness of imagery has nothing to do with individual ability. The studies employed fMRI to see brain activity during the visualisation, confirmed that vividness is a neurological construct and changes with objects and situations.
The second question was how eidetic imagery works for PWID. Syed, Neelofur, Moran, and O’Reilly examined the therapeutic utility of eidetic imagery-based psychotherapy (EMG) for ID. This study evaluated eidetic imagery-based therapy for people with mild and moderate ID. The study comprised thirty PWID who have long-term difficulties with experiential (abuse, trauma), emotional (bereavement, attachment disorders), mental health (anxiety, depression), and behavioural (anger, violence) issues. They received Eidetic Psychotherapy as suggested in EMG. The Anxiety Depression and Mood Scale (ADAMS) was used to measure their difficulties at the start, after every fifth session, and at the end. Their ADAMS scores showed significant improvement. The difference was statistically significant with a large effect size (d=1.54), while Tapp et al in the results of their meta-analysis reported the effect size for individually delivered therapy as small and non-significant. Average number of sessions until symptoms remission was 9.31. Furthermore, the study also reported the underlying experiential reasons for the presenting complaints. Predominantly, they were related to bereavement, attachment issues and traumas, which are frequently documented experiential reasons behind the onset of prevalent mental health issues like anxiety and depression in people with ID.
The results of this study are relevant in two respects. They demonstrate the presence of eidetic imagery in PWID and demonstrate the therapeutic efficacy of eidetic imagery-based treatment.
2.2. THERAPEUTIC PROCESS OF EMG
Eidetic Model of Growth offers a two-pronged therapeutic process for PWID. One aspect of EMG works to create a therapeutic environment. Based on theoretical tenets of Ahsen, this arm of EMG emphasises on the individual choices and predictability. Here the first goal is to enhance individual’s participation in meaningful and growth-oriented activities of choice.
The therapeutic emphasis is on the growth and development of PWID. Syed characterised growth as extending beyond the notion of skill acquisition. Growth, in this context, is a normative, organic process sustained through various developmental phases in human consciousness. According to the eidetic theory, growth processes are impeded when the individual is in conflict with nature or their environment. The individual is not a passive participant in their connection with nature and the surroundings. One component of the EMG seeks to address environmental concerns to create a more congenial and pleasant atmosphere, enabling individuals to actively participate in its development. A secondary component of EMG aims to tackle emotional issues, such as loss and attachment, as well as experiential concerns, including abuse and trauma, during individual sessions. For patients exhibiting diminished cognitive functioning and minimal or absent verbal capacity, therapies are implemented through indirect methods utilising principles of Eidetic Psychotherapy. The EMG emphasises the environment in which PWID reside and operate. The focus on individual activity selection and the regularity of activity structure enhances engagement in meaningful and productive endeavours while also reducing anxiety. Syed also proposed group interventions to tackle interpersonal issues.
The EMG processes entail the following steps. The process starts with formal and informal assessment of current functional status. The objective here is to ascertain the present degree of functioning and deficits. The individual’s functioning, skills, adjustment in various environments, and behavioural challenges are evaluated using updated assessment instruments. This establishes the direction of warranted interventions for the individual.
2.2.2. Eidetic Therapy for people with intellectual disability
Syed discovered that EP techniques for overcoming emotional and experiential challenges in PWID are not only similarly promising, but also more simple, straightforward, and uncomplicated than in TDIs. The explanation for this is that, unlike TDIs, PWID have no gap between image and word. That is why PWID cannot have an imageless recall, whereas TDIs can. The image of a traumatic experience can be flashed by a word, symbol, or revisiting a place. They typically do not require instruction for visualising an experience, as an EP practitioner does with TDIs. This finding prompted Syed to propose two plausible theoretical techniques; Telling is Visualisation, and Interaction is Revisiting. These two eidetic principles help bypassing the functional impediments of PWID in taking instructions to visualise an experience.
As the ISM in ID is described as ISm, which illustrates the similarities and differences between PWID and TDIs, according to eidetic theory. Individuals with ID share similarities in processing sensory input and experiencing its bodily effects; however, their ability to comprehend these experiences may be underdeveloped due to reduced cognitive functioning.
The second adaption of Eidetic Psychotherapy was implemented upon the realisation that an individual with ID concurrently verbalises an incident while visualising its images. The disparity between verbal description and visualisation is absent. The therapeutic premise Telling Is Visualisation is grounded in this clinical observation. The spontaneous “telling” process elicits the pertinent bodily responses and cognitive transformations that the EP seeks to accomplish. Nonetheless, when visualisation is feasible (in individuals with mild ID who possess the necessary language skills to follow therapeutic instructions), the therapeutic process unfolds similarly to that of TDIs. In instances, where the emotional difficulties are caused by a conflict with significant others (Case 5) the EMG principle Interaction Is Revisiting is employed. A predictable, regular, frequent, and brief interaction with the significant other is likely to overcome the conflict in interaction.
The EMG recommended a revised definition for the structure of activity planning to meet the needs of PWID. This new structure is founded on Ahsen’s idea of interactivity. This arm of EMG is meant to develop a therapeutic environment.
2.2.3. Therapeutic procedures
The emphasis of EMG extends beyond conventional remediation. However, here we are focused only on the therapeutic aspect of the EMG. In this section we will describe the therapeutic processes as they are administered.
The EMG has adapted/modified Ahsen therapeutic approach. In his approach Age projection Test is a therapeutic guide, which helps the therapist to track and treat the pathological experiences. The TDIs develop many intricate mechanism the way experience is stored in consciousness. Two mechanisms, which Ahsen has identified were; variation in the ISM structure, instead of ISM, they develop IMS, MIS, MSI, SIM, and SMI. The second intricacy is what Ahsen termed as Consciousness-Imagery Gap (CIG), that also challenges the therapeutic procedures and therapist is supposed to deal with it. Ahsen has identified a gap between an experience as revealed in eidetic image and an ordinary conscious understanding of it. This conscious understanding depends solely on the cognitive abilities of an individual. Syed made his observation that these difficulties, therapists do not have to deal with while working with ID group. The ISM variation and CIG exist mostly in TDIs.
The process of history taking most of the time is relatively simpler in people with ID. Particularly, in developed countries, all the important life events are easily traceable in the records. The important life milestones, stressful events, witnessing violence, abuse of various nature, deprivation of basic needs, traumas, deaths of significant others or moving out of family home to an institutional care are generally part of the record. That is a fact PWID can not give the subjective evaluation of life events as thoroughly, however, the physical and behavioural signs are enough, most of the time, to assess the nature and severity of impact of stressful events on them. Interviews with family members and staff aid this process further.
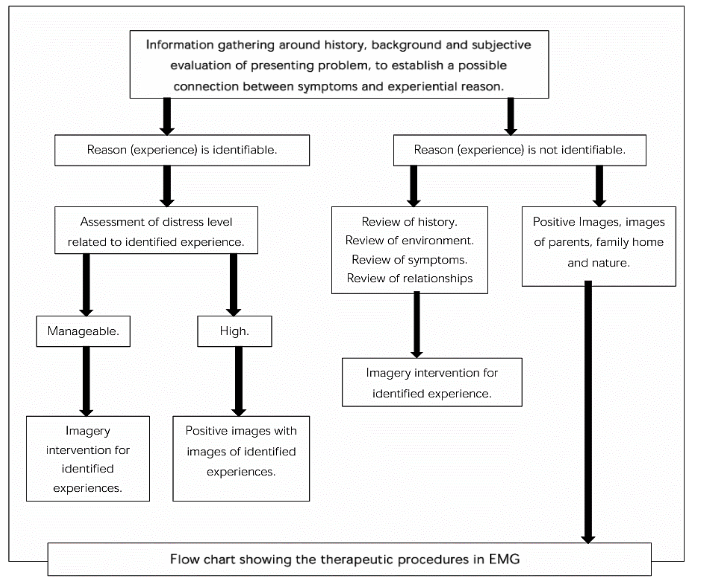
After finding (list of) significant stressful events the therapeutic process starts as shown in the figure. In case, the record does not reveal a clinically definable trauma, the financial difficulties in childhood, emotional and attachment related issues like parental separation, deaths in the family, departure from family home can also be investigated into. Different life issue, sometimes need to be approached somewhat differently. The therapeutic modus operandi depends predominantly on cognitive and verbal ability of individual and other support mechanisms available.
3. The application of eidetic imagery based therapeutic techniques for people with intellectual disability
In this section, therapeutic procedures employed in five cases of psychological, emotional, behavioural and experiential difficulties are presented. They highlight the EMG approach of identifying the underlying experiential difficulties and then addressing them through imagery. Another salient feature here to note is the involvement of lay therapists, which may help the therapeutic work where there is a dearth of trained psychotherapists.
3.1. TRAUMA IN CONFLICT REGIONS AND INDIVIDUALS WITH INTELLECTUAL DISABILITY
Research on trauma and how it affects the lives and mental health of PWID is a relatively recent development in psychology. Only a few studies published before 2000 were cited in a pilot study on PTSD in PWID. These studies brought attention to the existence of trauma in PWID. Different types of abuse by families or institutional setting were the source of the trauma in those researches. In the most recent evaluation of the literature, Starke, Larsson, and Punzi examined 26 studies, but again, the majority of them dealt with the mistreatment and abuse people with ID endured. Another review focused on the disregard for PWID in times of war or similar circumstances. Rohwerder emphasised how little is known about PTSD in PWID from the warzones. In a review, it has been described how the conflict in Ukraine affected PWID. But only the first three months of the conflict were covered in this review. Less is known about the literature from areas that are enduring decades of conflict, such as Afghanistan, Somalia, and Palestine. As a result, there is less data regarding the effects of the war and the therapeutic support for PWID.
In addition to demonstrating how EMG therapy can be used to treat the trauma experienced by PWID who have lived in conflict areas, Case 1 also suggests that PTSD symptoms may not manifest in PWID right away. Thus, it implies that a deeper understanding of the trauma experienced in warzones is crucial, necessitating in-depth professional analysis and dialogue.
3.2. SEXUAL ABUSE IN PEOPLE WITH INTELLECTUAL DISABILITY
According to several studies referenced by McNally, Taggart, and Shevlin, one of the main causes of PTSD in individuals with ID is sexual abuse. O’Malley et al. examined cases of sexually abused people with ID and determined that eidetic psychotherapy can be beneficial for them clinically. Case 2 provides an intense and complex presentation of a person with ID who struggled for a long time with aggressive and self-harming behaviours. He responded to eidetic imagery-based treatment despite having a severe speech impediment.
3.3. FINANCIAL DIFFICULTIES AND THEIR PSYCHOLOGICAL IMPACT
A risk factor that is frequently disregarded in relation to behavioural, emotional, and physical health issues among PWID is Adverse Childhood Experiences. The effects of early childhood need deprivation on the adult lives of individuals with ID are explained in Case 3. The behavioural presentation in Case 3 was uncharacteristic of an overall personal profile of the individual. Inaccurate theoretical framework can make it difficult to relate the behaviours that result from the ACEs to the current presentation. Such behavioural symptoms are considered as actual problems to address by behaviouristic and other symptom based therapeutic models. However, the system-based therapies, like the EMG interprets these behaviours as a sign of a deeply ingrained experience in the consciousness. As a result, it was simple and rapid to recognise and address the behaviour at the earliest stages of therapeutic encounters with the individual.
3.4. ATTACHMENT AND BEREAVEMENT RELATED ISSUES
After reviewing several studies, Ramsden et al. concluded that individuals with ID are more likely than other groups to develop insecure and disorganised attachment patterns, both in clinical and non-clinical settings. According to their research evaluation, there are a number of reasons why people with ID may experience attachment difficulties. Parents are not sensitive enough and caring when it comes to meeting the needs of children with ID because of communication problems. Parents who experience stress have mental health issues that affect their relationships and interactions with others. It is more difficult to establish secure attachment bonds when one is dependent on several care providers.
Doka coined the term disenfranchised grief to characterise the lack of knowledge around the death of a parent and to explain the often-overlooked emotional impact of death on PWID. According to several cases reported by Syed et al., the primary etiological experience driving complicated presentations ranging from aggression to self-harming conduct was bereavement. Case 4 describes the treatment procedure for an individual with chronic attachment and bereavement-related difficulties and their complex manifestation in behavioural symptoms.
3.5. DEINSTITUTIONALISATION AND EMG
According to Neelofur’s systematic review, there is no traceable literature on the psychological support given to individuals with ID during the deinstitutionalisation process. She conducted a qualitative analysis of the lives of individuals with ID who left institutions and had difficulty adjusting to life in a community home, specifically in the context of challenging behaviour, for her doctoral research. According to the literature examined by Neelofur, deinstitutionalisation does not address or even improve behavioural problems. She described how eidetic imagery-based EMG assisted recently deinstitutionalised individuals in overcoming extremely challenging behaviour, resulting in a rather normal life in community-based residential services.
4. Conclusion
For people with intellectual disabilities (PWID), the Eidetic Model of Growth (EMG) is an approach of psychology support based on eidetic imagery. This review examines EMG theory, practice, procedures and evidence. Hereby, the following key aspects of its theory and practice are highlighted. Imagery is now a recognised feature and function of human consciousness, supported by psychological and neurological research that demonstrates its biological existence, and psychological functions. In a nonpharmacological way, a psychotherapy model based on it easily links it to the biological underpinnings of behaviour and cognition. Despite the verbal and cognitive impairments, there is evidence that people with ID experience it in a similar way to typically developing individuals (TDIs), with just a few slight differences. Furthermore, PWID can also benefit from a therapeutic paradigm that is based on it.
In those with mild to moderate ID, empirical studies on EMG have demonstrated significant improvements in anxiety, depression, mood, and behavioural issues, requiring fewer therapy sessions than other models. This review confirms Ahsen’s original assertions on the broad applicability of eidetic imagery in psychological healing and growth by highlighting the potential clinical effectiveness of EMG techniques in addressing chronic experiential, emotional, mental, and behavioural problems. Furthermore, this review also indicates at the ease and speed with which EMG works. This aspect makes it a worthwhile option for services and schools for PWID.
References
- Syed, A. A., Neelofur, S., Moran, A. & O’Reilly, G. (2020). Investigating the potential clinical utility of therapeutic techniques based on eidetic imagery as adapted by the Eidetic Model of Growth (EMG) for people with intellectual disability (ID). Heliyon, 2020; 6, 10, 1-10.
- Malley, G., Irwin, L., Syed, A. A., & Guerin, S. (2019). The clinical approach used in supporting individuals with intellectual disability who have been sexually abused. British Journal of Learning Disability, 2019; 47, 105-115.
- Neelofur, S. Exploring Psychological Supports and the Potential Role and Contribution of Eidetic Model of Growth in Providing Psychological Supports to People with Intellectual Disabilities after Deinstitutionalization. An unpublished PhD thesis submitted to the University College Dublin, Ireland. 2019.
- Kosslyn, S. M. Image and brain. Cambridge: MIT Press: 1996.
- Jaensch, E.R. Eidetic imagery. (Oscar Oeser, Trans.). New York: Harcourt, Brace & Company: 1930.
- Hochman, J. The image psychology of Akhter Ahsen. Lahore: Dastavez: 1995.
- Ahsen, A. Eidetics: An overview. Journal of Mental Imagery, 2010; 34, 1 & 2, 11- 42.
- Kosslyn, S. M. (2005). Reflective thinking and mental imagery: A perspective on the development of posttraumatic stress disorder. Development and Psychopathology, 2005; 17. 851-863.
- Holmes, E. A, & Mathews, A. Mental imagery in emotion and emotional disorders. Clinical Psychology Review, 2010; 30, 349 362.
- Holmes, E. A., Mathews, A., Mackintosh, B., & Dalgleish, T. The causal effect of mental imagery on emotion assessed using picture-word cues. Emotion, 2008; 8, 3, 395 409.
- Mathews, A., Ridgeway, V., & Holmes, E. A. Feels like the real thing: Imagery is both more realistic and emotional than verbal thought. Cognition and Emotion, 2013; 27,2, 217-229.
- Holmes, E., & Hackmann, A. A healthy imagination? Editorial for the special issue of memory: Mental imagery and memory in psychopathology. Memory, 2004; 12, 4,, 387-388.
- Ehlers, A., Clark, D.M., Hackmann, A., McManus, F., & Fennell, M. Cognitive therapy for post-traumatic stress disorder: development and evaluation. Behaviour Research and Therapy. 2005; 43, 4, 413 431.
- Patel, T, Brewin, C. R, Wheatley, J, Wells, A., Fisher, P., & Myers, S. Intrusive images and memories in major depression. Behaviour Research and Therapy, 2007; 45, 2573 2580.
- Motoyama, H., & Hishitani, S. The brain mechanism that reduces the vividness of negative imagery. Consciousness and Cognition, 2016; 39, 59 69.
- Leech R, Sharp DJ. The role of the posterior cingulate cortex in cognition and disease. Brain. (1):12-32.
- Day, S. J., Holmes, E. A., & Hackman, A. (2004). Occurrence of imagery and its link with early memories in agoraphobia. Memory, 2004; 12(4), 416-427.
- Ji, J. L., Holmes, E, A., & Blackwella, S. E. Seeing light at the end of the tunnel: Positive prospective mental imagery and optimism in depression. Psychiatry Research, 2017; 247, 155 162.
- Morina, N., Deeprose, C., Pusowski, C, Schmid, M., & Holmes, E. A. (2011). Prospective mental imagery in patients with major depressive disorder or anxiety disorders. Journal of Anxiety Disorders, 2011; 25, 1032 1037.
- Dolan, A. T. Imagery treatment of phobias, anxiety states and other symptom complexes. New York: Brandon House: 1997.
- Clark, I.A., and Mackay, C.E. Mental imagery and post-traumatic stress disorder: a neuroimaging and experimental psychopathology approach to intrusive memories of trauma. Front. Psychiatry, 2015; 6:104.
- Borghus A, Dokkedahl S, Elklit A. Pilot study: undetected post-traumatic stress disorder symptoms among intellectually disabled. Int J Dev Disabil. 2018; 20;66(1):36-45.
- Starke, M., Anneli Larsson, A., and Punzi, E. (2024). People with intellectual disability and their risk of exposure to violence: Identification and prevention a literature review. Journal of Intellectual Disabilities, 2024; 0(0) 1 24.
- Grove, S., N. Grove, and T. Myerscough. Intellectual Disability and War: Issues for Consideration. Journal on Developmental Disabilities, 2010; 16 (1): 85 93.
- Rohwerder, B. Intellectual Disabilities, Violent Conflict and Humanitarian Assistance: Advocacy of the Forgotten. Disability & Society, 2013; 28 (6): 770 783.
- Vromans, L., Frielink, N., Noorlandt, H. W., Giesbers, S. A. H., & Embregts, P. J. C. M. The experiences of people with intellectual disabilities living in Ukraine during the first months of the Russian invasion: A lack of fulfilment of basic necessities and support and uncertainty towards reforms. Disability & Society, 2023; 39(11), 2920 2935.
- McNally, P., Taggart, L. and Shevlin, M. (2021), Trauma experiences of people with an intellectual disability and their implications: A scoping review. J Appl Res Intellect Disabil, 2021; 34: 927-949.
- Vervoort-Schel, J., Mercera, G., Wissink, I., Helm, P. V., Lindauer, R., & Moonen, X. Prevalence of and relationship between adverse childhood experiences and family context risk factors among children with intellectual disabilities and borderline intellectual functioning. Research in Developmental Disabilities, 2021; 113.
- Ramsden R, Reeves E, Whitwell E, Lane N, Fletcher HK. (2025) A systematic review of attachment interventions for people with intellectual disability and their caregivers. J Intellect Disabil, 2025; 29(2): 469-499.
- Doka, K., Disenfranchised Grief. 1989. Lexington, MA: Lexington Books: 1989.
- Runge, M. S., Cheung, M. W., & D Angiulli, A. Meta-analytic comparison of trial- versus questionnaire-based vividness reportability across behavioural, cognitive and neural measurements of imagery. Neuroscience of Consciousness; 2017 1 13.
- Dijkstra, D, Bosch, S. & Gerven, M. A. J. Vividness of visual imagery depends on the neural overlap with perception in visual areas. Journal of Neuroscience; 2017, 10, 6, 1-23.