

Minimally Invasive Osteosynthesis for Distal Humerus Fracture
Minimally invasive osteosynthesis of distal humerus fracture with commercially available pre-contoured plate using an anterolateral fixation: mid to long-term results
Oscar Alejandro Mejía, MD.¹, Jaime Valencia, MD.², Carlos Eduardo Afanador, MD.², Sebastián Calle Díaz, MD.³, German Alejandro Jaramillo, MD.⁴, Ana Milena Herrera, MD. Ph.D⁵
- Orthopedic surgeon. Shoulder and elbow orthopedics. Clínica del Campestre and Clínica Universitaria Bolivariana. Medellín, Colombia
- Orthopedic surgeon. Shoulder and elbow orthopedics. Hospital Pablo Tobón Uribe, Clínica Universitaria Bolivariana and Clínica del Campestre. Medellín, Colombia
- Orthopedic surgery resident. Facultad de Medicina, Universidad de Antioquia. Medellín, Colombia
- Orthopedic surgeon. Shoulder and elbow orthopedics. Clínica del Campestre and Clínica del Norte. Medellín, Colombia
- Epidemiology Unit, Clínica del Campestre. Medellín, Colombia
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: Mejía, OA., et al., 2025. Minimally invasive osteosynthesis of distal humerus fracture with commercially available pre-contoured plate using an anterolateral fixation: mid to long-term results. Medical Research Archives, [online] 13(3).
https://doi.org/10.18103/mra.v13i3.6425
COPYRIGHT:© 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6425
ISSN 2375-1924
ABSTRACT
Background:
Surgical treatment of distal diaphyseal humerus fractures (DDHF) minimally invasive plate osteosynthesis (MIPO) has gained popularity among orthopedic surgeons as it causes less soft-tissue disruption associated with other open approaches; however, the iatrogenic radial nerve injury is still a concern. Recently, a novel technique for a MIPO through anterior approach and anterolateral fixation was proposed as an alternative to reduce the risk of radial nerve damage.
Aims:
To determine the mid-to-long-term functional results and safety of a MIPO through an anterior approach and anterolateral fixation using a pre-contoured locking plate modified to adjust to the anatomical surface of the lateral column of the humerus.
Methods:
A prospective longitudinal follow-up of patients treated for a DDHF with MIPO through an anterior approach and anterolateral fixation using a pre-contoured locking plate modified to adjust to the anatomical surface of the lateral column of the humerus. Clinical evaluations included the active range of movement (AROM), functional assessment through the Mayo Elbow Performance Score (MEPS), and pain and complications. Radiographic evaluation included assessment of consolidation, residual angulations, and the optimal plate’s position.
Results:
This series included ten patients with 12A, 12B, and 12C fractures. Patients were followed for a median of 36.9 months (9.5 – 62.5 months). At the last evaluation, the median pain level was 1.5, the median elbow flexion was 125 degrees, and the median MEPS was 85. Two patients presented radial nerve praxia, which resolved with physical therapy. Residual angulations were minimal and within the range of acceptable alignment in the osteosynthesis of a distal diaphyseal fracture of the humerus.
Conclusion:
This MIPO technique with an anterior approach and anterolateral fixation for metaphyseal and distal diaphyseal extra-articular humerus fractures produced a stable reduction and fixation with satisfactory mid-to-long-term clinical and functional outcomes and low complication rates.
Keywords:
Humeral Fractures, Distal; Fracture Fixation, Internal; Bone Plates; Minimally Invasive Surgical Procedures
Introduction
Treatment of distal diaphyseal humerus fractures (DDHF) represents a challenge in orthopedic surgery owing to the complex elbow anatomy and proximity of neurovascular structures¹⁴. These fractures have a bimodal distribution, mainly caused by high-energy traumas in the young population and by low-energy traumas or falls in older people²,³,⁵.
Restoration of elbow function amid a stable fixation of all bone fragments is critical in managing DDHF. Although there is no consensus on the best alternative for surgical treatment, for a while, open reduction and internal fixation (ORIF) with dual plates has been the treatment of choice, especially for more distal meta-diaphyseal fractures³,⁵,⁸. However, sometimes, to have sufficient articular exposure for dual plating, a posterior approach with extensive soft tissue trauma is usually performed, carrying a high risk of iatrogenic neurovascular injury. Additionally, revision surgery is frequently needed secondary to olecranon osteotomy, leading to non-union, malunion, and hardware irritation¹–⁵,⁹–¹¹.
On the other hand, ORIF with medial or lateral approaches facilitates exposure of the joint’s anterior surface, radial nerve visualization and exploration, and rigid fixation of the more distal fracture fragments, allowing prompt rehabilitation and functional recovery¹¹–¹⁴. Still, the soft tissue trauma and scar are extensive with these methods.
To minimize soft tissue disruption while achieving a stable fixation of DDHF, minimally invasive plate osteosynthesis (MIPO) through different approaches has been proposed by several authors¹⁵,²⁰. However, the complex anatomy of the elbow makes plating and fixation extremely difficult, often leading to complications such as permanent neurovascular damages and joint stiffness²¹.
Cañada-Oya et al.¹⁶, and Yang et al.¹⁷, have proposed a MIPO through an anteromedial approach, a technically difficult method as the neurovascular structures are at risk; it requires a vast knowledge of the anatomical structures and high expertise of the trauma surgeon¹⁶,¹⁷. Nevertheless, Yang et al.¹⁷ reported satisfactory results in fracture healing and functional recovery with no complications in twelve patients using this technique. More recently, Mejía et al.²² published an anatomical study proposing a MIPO technique with an anterior approach with two incisions and fixation using a modified locking plate on the lateral column of the humerus. In this technique, a small distal incision permits accessing the fracture site by medially retracting the biceps brachii muscle and dissecting the brachialis muscle. A second proximal incision allows submuscular communication for retrograde plate slipping from distal to proximal. The extra-articular distal humerus plate is manually molded to fit the bone surface on the lateral column and distally fixed with 5 five locking screws conferring maximum stability to the distal segment²². In the distal region, the radial nerve runs lateral to the lateral edge of the plate at about 10 to 11 mm. With this anatomical study, the authors showed that this technique permits better exposure of the fracture focus and radial nerve observation and protection while minimizing soft tissue damage²². However, whether the molding of the plate could lead to fatigue of the material and consequently loosening or failure, and whether the stability of fixation would persist through time is still unknown.
This study presents the mid-to-long-term clinical and functional outcomes of a series of patients with DDHF treated with the MIPO with anterior approach and anterolateral fixation technique described by Mejía et al.²².
Methods
PATIENTS
The study was approved by our Institutional Review Board (IRB); all methods were carried out following local and international guidelines and regulations. Between March 2019 and May 2023, ten consecutive patients were treated for a DDHF with MIPO through an anterior approach and anterolateral fixation using a pre-contoured locking plate modified to adjust to the anatomical surface of the lateral column of the humerus. Data concerning the procedures and follow-ups were gathered from March 2019 to June 2024. All procedures were carried out in Clínica del Campestre and Clínica Universitaria Bolivariana in Colombia.
Adult patients (≥18 years) were eligible for the procedure if presented with an extraarticular type 12A to 12C DDHF. Patients with less than 12 months of follow-up after the surgery were excluded from the study.
After the procedure, all patients were scheduled for routine follow-ups of 15 days and 3 and 6 months, according to our clinical protocol. Clinical evaluations during follow-ups consisted of the active range of movement (AROM) and functional assessment through the Mayo Elbow Performance Score (MEPS)²³, and the presence of pain and complications. Data was extracted from clinical records. Due to restrictions from the paying insurers, radiographic evaluations were not performed during all follow-ups unless clinical evaluation indicated the need for it.
For one last follow-up, additional efforts were made to reach all patients and update their clinical and radiological assessments. At the last radiographic evaluation, consolidation, varus or valgus deformity, recurvatum or antecurvatum, and the optimal plate’s position were assessed.
SURGICAL TECHNIQUE
The surgical technique follows the steps described by Mejía et al.²². In brief, the patient’s arm is placed in a supine position. An anterior 3 cm incision is performed at the midpoint of the distal third of the arm, 2 cm proximal to the antecubital fold. Then, the biceps muscle is rejected medially, exposing the brachialis muscle and the lateral antebrachial cutaneous nerve (Figure 1).
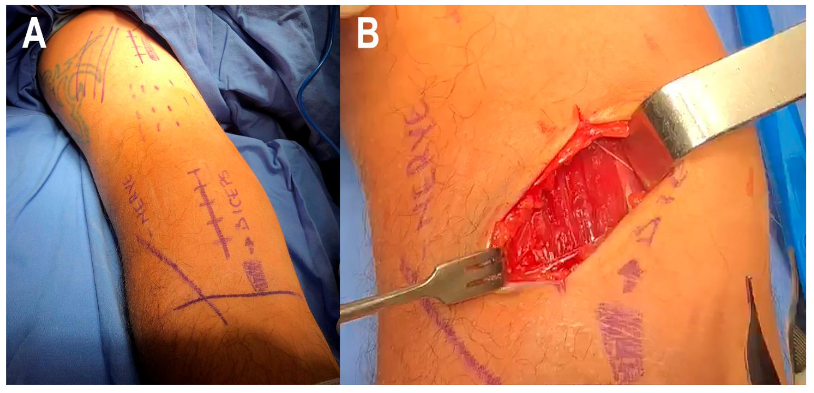
The images show the position of the initial distal incision (A) and the exposure of the brachialis muscle and the lateral antebrachial cutaneous nerve (B).
The brachialis muscle is dissected to expose the distal third of the humeral shaft; the coronoid fossa and distal lateral column are observed here. A second and proximal 4 to 5 cm skin incision is performed on the proximal third of the arm, exposing the humeral shaft (Figure 2).
The fracture is reduced with elbow traction movements, at 60-degree shoulder abduction and 90-degree elbow flexion with forearm supination. Then, the distal and proximal approaches are communicated sub-muscularly sliding the previously molded contralateral, LCP® Extra-articular Distal Humerus Plate (DePuy Synthes, Johnson & Johnson) from distal to proximal. The plate should be positioned 1 cm proximal to the most proximal part of the capitellum (Figure 3).
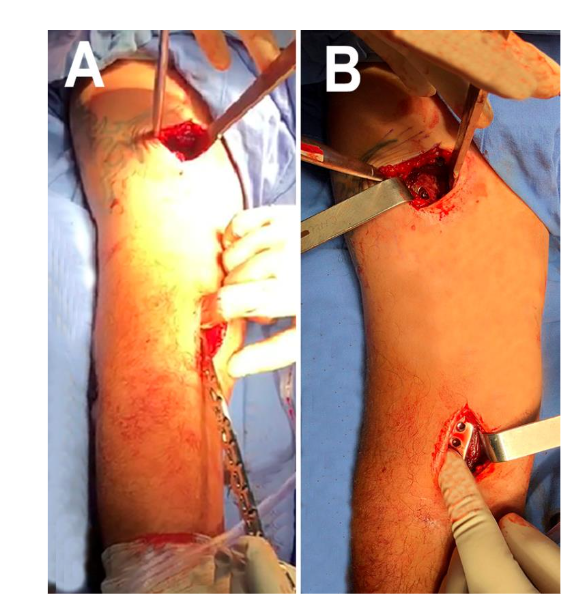
The images display the exposure of the lateral column of the distal humerus (A) and the location of the second and proximal incisions (B).
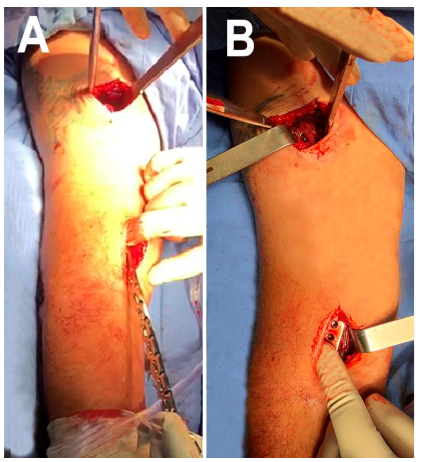
Figure 3. Plate sliding and positioning.
The pictures depict the molded plate sliding in from distal to proximal over the humeral lateral surface (A) and the position of the distal end 1 cm proximal to the most proximal edge of the capitellum (B).
A temporary proximal fixation is performed (Figure 4), followed by plate fixation with five locked screws distally and three screws proximally. The correct reduction with the plate’s position and fixation are confirmed with the image intensifier. The anatomical relations of the plate are depicted in Figure 5²².

A temporary proximal fixation is performed (Figure 4), followed by plate fixation with five locked screws distally and three screws proximally. The correct reduction with the plate’s position and fixation are confirmed with the image intensifier. The anatomical relations of the plate are depicted in Figure 5²².

Figure 5. Anatomical relations. The illustrations depict the optimal position of the plate and the relationship of the plate with the capitellum and the radial nerve (Extracted with permission from Mejía et al. 2024²²).
The rehabilitation protocol involved passively assisted elbow movements for the first 30 days, followed by active movements. Gradual strengthening begins after 6 to 8 weeks. Non-competitive physical activities were allowed in the fifth month.
STATISTICAL ANALYSIS
Unless otherwise specified, data are expressed as medians and ranges (minimum and maximum) for continuous variables and absolute frequencies (number) for categorical variables. The elbow flexion of the operated arm was expressed as a percentage of the non-affected arm. Nonparametric statistics were used for the bivariate analysis of the relation of the distal segment length. AROM and MEPS were obtained at the latest follow-up using the chi-square, Kruskal-Wallis, and Spearman correlation tests. The two-sided statistical tests were considered statistically significant with a p-value ≤0.05. The analysis was.
conducted using SPSS statistical software (version 25.0; IBM Corp, Armonk, NY, USA).
Results
The cohort included six males and four females with a median age of 28.5 years (range 19 – 61 years) at the time of the procedure. Seven right and three left arms underwent the procedure, and in seven of the ten patients, the arm on the dominant side was intervened. The most frequent mechanism of the fracture was a motorcycle accident in nine patients (Table 1).
Three patients had fractures type 12A, five type 12B, and two 12C. The median distal segment length was 85.5 mm (49 – 103 mm) (Table 1). None of the patients presented a neurovascular compromise.
Table 1. Patients’ characteristics and their preoperative assessment details
| Patient # | Sex | Age (years) | Affected side | Dominant side affected | Trauma mechanism | Type of fracture | Distal segment length (mm) |
|---|---|---|---|---|---|---|---|
| 1 | Male | 61 | Right | Yes | Motorcycle accident | 12-A3 | 92 |
| 2 | Male | 25 | Right | Yes | Motorcycle accident | 12-B3 | 99 |
| 3 | Male | 23 | Right | Yes | Motorcycle accident | 12-B2 | 103 |
| 4 | Female | 32 | Right | Yes | Motorcycle accident | 12-C3 | 74 |
| 5 | Male | 19 | Left | No | Motorcycle accident | 12-B2 | 98 |
| 6 | Female | 24 | Right | Yes | Motorcycle accident | 12-B2 | 58 |
| 7 | Male | 40 | Right | Yes | Motorcycle accident | 12-A1 | 62 |
| 8 | Male | 32 | Left | No | Motorcycle accident | 12-C3 | 88 |
| 9 | Female | 25 | Left | No | Motorcycle accident | 12-B2 |
49
|
| 10 | Female | 37 | Right | Si | Car accident | 12-A2 | 83 |
The surgical procedure was performed at a median of 11.5 days (range, 3 – 17 days) after the trauma. The procedure went without complications in all cases. Only two patients presented radial nerve praxia, which quickly resolved with physical therapy.
The AROM and MEPS steadily and significantly changed through follow-ups (p = 0.000) (Figure 6).
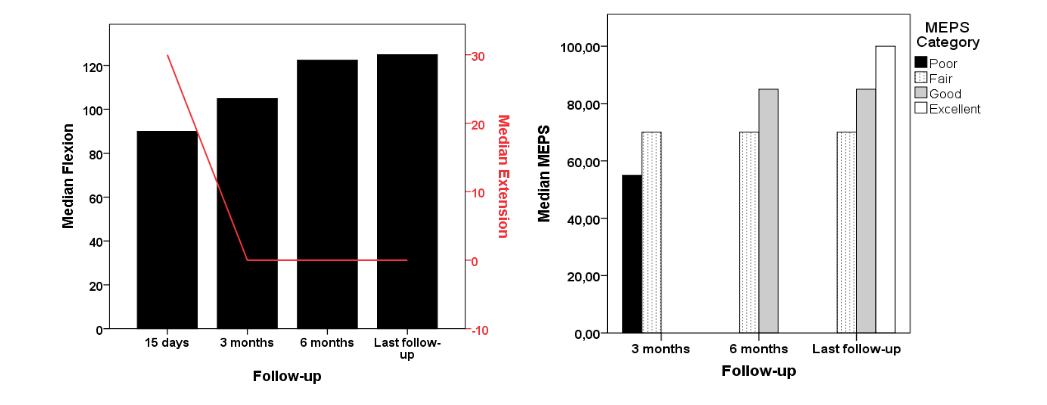
Figure 6. AROM and MEPS changes.
The figures show steady changes in the median flexion and extension (A) and the MEPS (B) through follow-ups.
The last follow-up was carried out in a median of 36.9 months (9.5 – 62.5 months). During the last follow-up, the median pain level (VAS) was 1.5 (range, 0 – 3), median elbow flexion was 125 degrees (range, 110 – 130 degrees), and median MEPS was 85 (range, 70 – 100) (Table 2).
Table 2. Patients’ follow-ups, complications, and their most recent assessment details
| Patient # | Complications | 3 months AROM | % | MEPS | 6 months AROM | % | MEPS | Last follow-up POP time | AROM | % | MEPS | VAS | Residual angulations |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 10–95° | 73.1 | 55 | 0–120° | 92.3 | 70 | 40.3 | 0–125° | 96.1 | 85 | 1 | ||
| 2 | Radial n. praxia | 10–110° | 88 | 70 | 0–125° | 100 | 85 | 40 | 0–125° | 100 | 100 | 0 | 7° antecurvatum |
| 3 | 0–100° | 80 | 70 | 0–120° | 96 | 85 | 39.4 | 0–125° | 100 | 100 | 0 | 4° varus | |
| 4 | Radial n. praxia | 20–100° | 80 | 55 | 0–110° | 91.7 | 70 | 12 | 0–110° | 91.7 | 85 | 2 | 6° antecurvatum |
| 5 | 0–95° | 79.2 | 40 | 0–100° | 80 | 85 | 62.5 | 0–110° | 91.7 | 100 | 0 | 4° varus / 3° recurvatum | |
| 6 | 0–130° | 84.6 | 55 | 0–130° | 100 | 85 | 34.4 | 0–130° | 100 | 100 | 2 | 5° valgus / 6° recurvatum | |
| 7 | 0–100° | 76.9 | 40 | 0–120° | 92.3 | 60 | 25.3 | 0–125° | 96.1 | 70 | 2 | 4° recurvatum | |
| 8 | 0–130° | 100 | 50 | 0–130° | 100 | 70 | 14.5 | 0–130° | 100 | 85 | 2 | 2° varus | |
| 9 | 0–125° | 100 | 55 | 0–125° | 100 | 70 | 22.9 | 0–125° | 100 | 85 | 1 | 7° antecurvatum | |
| 10 | 0–120° | 96 | 55 | 0–125° | 100 | 70 | 62.2 | 0–125° | 100 | 85 | 3 | 3° recurvatum |
AROM*: Active range of movement expressed in degrees
%: indicated the percentage of operated arms concerning the contralateral
POP time: Postoperative time is expressed in months
The bivariate analysis showed no relation between the distal segment length and the AROM and MEPS assessed during the last follow-up (p = 0.934 and 0.521, respectively) (Figure 7)
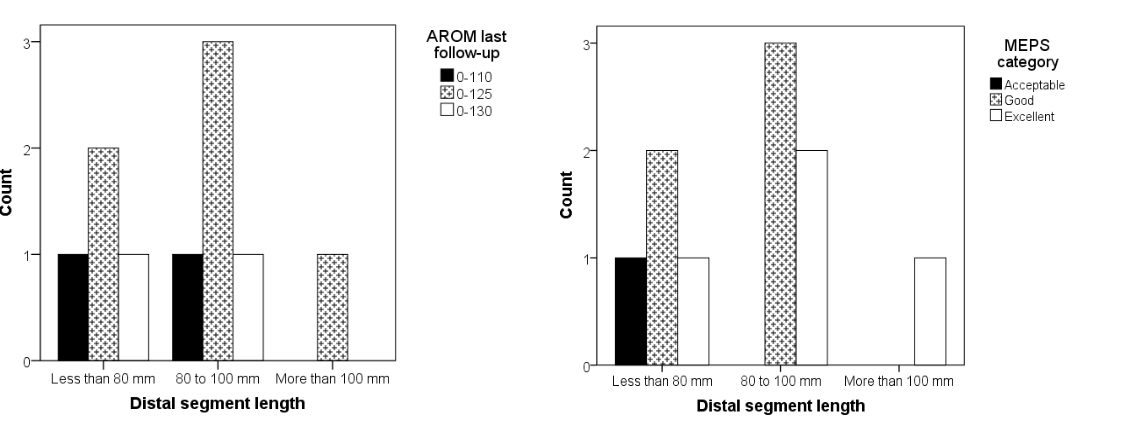 Figure 7. AROM and MEPS according to distal segment length.
Figure 7. AROM and MEPS according to distal segment length.
Three patients had a varus deformity, and one had a valgus deformity of less than 5 degrees. Three patients presented antecurvatum and four recurvatum with less than 7 degrees. All patients demonstrated evidence of consolidation during the last assessment and radiographic follow-up (Table 2).
One patient required removal of the osteosynthesis material due to pain with elbow flexion. All patients reported being satisfied with the functional outcome of the surgery.
Two cases of the series are shown in Figures 8 and 9.
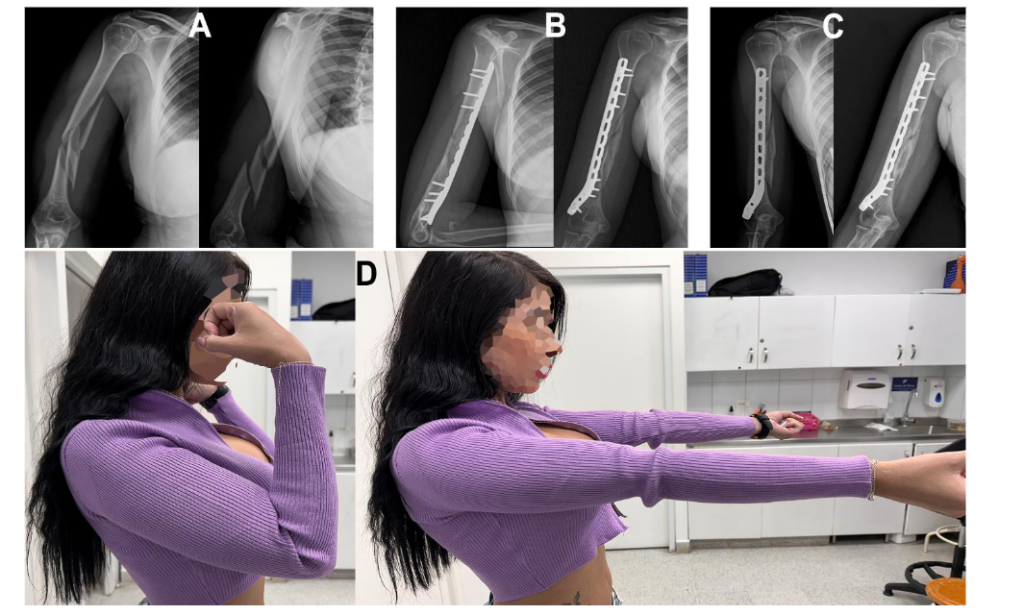
Figure 8. Case 1.
A. Female 32 years old, with a right 12-C3 fracture.
B. Three months’ follow-up.
C. Six- and ten-month radiographic follow-up.
D. AROM at ten months after surgery.
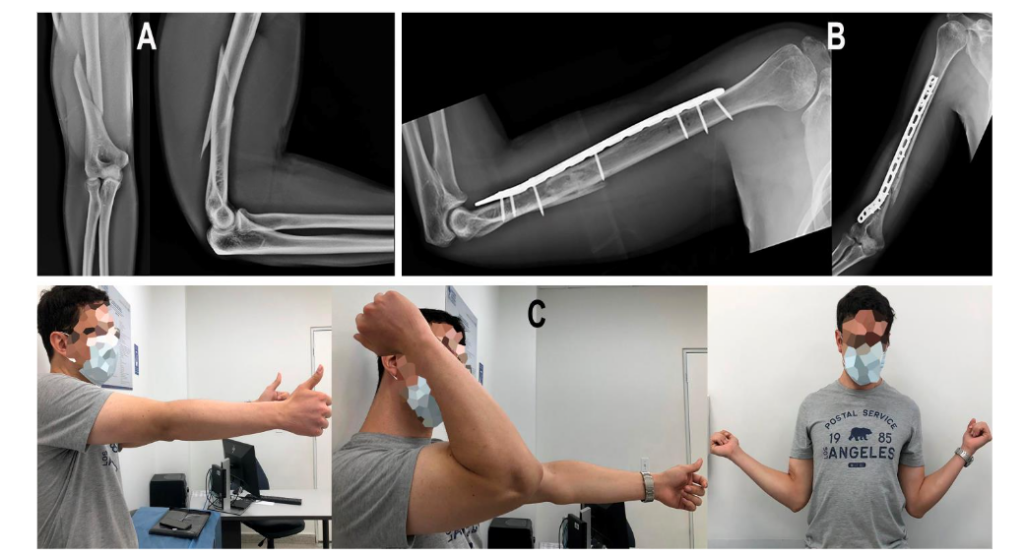
Figure 9. Case 2.
A. Male, 32 years old, with a right 12-C3 fracture.
B. Three months’ follow-up.
C. AROM at three months after surgery.
Discussion
The current study showed satisfactory mid-to-long-term clinical and functional outcomes and low complication rates in patients with DDHF treated with a MIPO with anterior approach and anterolateral fixation following the technique described by Mejía et al.²². In our series of ten patients, 80% had recovered the AROM, and 60% functionally recuperated after six- and twelve-months post-surgery, respectively. Only two patients presented radial nerve praxia, which resolved without long-term consequences. Fifty percent of the patients had follow-ups more than 36 months after the procedure, showing a stable fixation and long-lasting functional results in the mid-to-long term.
ORIF is probably the most used surgical treatment for extra-articular DDHF¹–⁵; however, MIPO, through different approaches, has been gaining more acceptance among the most experienced surgeons as an alternative for achieving a stable fixation while minimizing soft-tissue disruption¹⁶,²⁰,²⁴. Nonetheless, the risk of iatrogenic injury to the neurovascular structures while reaching the fracture site and plating is still a significant concern, especially in MIPO techniques where the dissection field is reduced¹²,¹⁷,²⁵–²⁸.
Despite the critical closeness of the radial nerve to the plate when performing a MIPO shown by Livani et al.²⁹ in their study, performing ultrasound evaluations, the incidence of transient radial nerve palsy is still lower compared to ORIF as demonstrated in the meta-analysis by Beerens et al.²⁵. However, to overcome this non-negligible risk, several surgical approaches for performing MIPO have been proposed¹⁶,²⁰,²⁴.
Jitprapaikulsarn et al.¹⁹ reported results of a MIPO with a posterior approach in 18 patients with type B or C DDHF. Even though this approach allows sufficient visualization and exposure of the fracture site, it still poses a significant risk of iatrogenic injury of the radial nerve. Yet, the authors showed that only two of their patients presented transient radial nerve palsy that fully recovered within three months¹⁹.
Anterior or anteromedial approach to the humerus could also lead to iatrogenic injury to any of the main nerves in the forearm. However, in different anatomical and clinical studies, it has been shown that this injury could be prevented if the fracture-to-coronoid distance (FCD) is >2 cm, keeping the fixing plate at a tolerable distance from these neural structures¹⁶,¹⁷,¹⁹,²⁰.
Cañada-Oya et al.¹⁶ performed an anatomical study proposing a minimally invasive anteromedial and distal approach with plate fixation on the medial column of the humerus. To avoid damaging the medial and ulnar nerves or the brachial artery, the technique requires surgical expertise during plate insertion, as this must be done through an incision in the pronator teres muscle¹⁶. Although promising, to our knowledge, no clinical data have been published using this specific technique. Yang et al.¹⁷ described a similar technique in a cadaveric study and the outcomes of a series of 12 patients using the anteromedial approach but inserting the plate through a soft tissue tunnel under the brachialis, fixing it on the anteromedial surface of the humerus. The authors found a satisfactory functional recovery at 12 months of follow-up without iatrogenic neurovascular injuries¹⁷.
On the other hand, using an anterolateral approach through only one distal incision at the fracture site in 28 patients with DDHF, Zhao et al.²⁴ showed satisfactory results without cases of iatrogenic neuropraxia²⁴. The authors proposed that the anterolateral approach allowed clear visualization and exposure of the radial nerve between the brachialis and brachioradialis muscles, permitting safe manipulation and plate insertion without damaging the nerve²⁴.
Recently, our group proposed an alternative MIPO technique using an anterior approach with plate fixation in the anterolateral column of the humerus that, according to the cadaveric study, is anatomically safe and allows the management of distal diaphyseal and meta-diaphyseal humerus fractures²².
anatomical analysis of the technique showed that the risk of damaging the radial nerve when performing the lateral separation of the intermuscular septum could be averted by performing blunt longitudinal dissection and separation without tension of the brachialis muscle. It was also shown that with this technique, the average distance between the lateral edge of the plate after fixation on the lateral column of the humerus and the radial nerve was 10.9 ± 0.6 mm. Additionally, contrary to the technique described by Zhao et al.²⁴, in our method, the radial nerve is neither explored nor neurolysed, which hypothetically could diminish accidental nerve injury. Also, by making two incisions, one distal and one proximal, a better visualization and handling of the plate can be achieved.
In this series of ten patients, using the anterior approach and anterolateral fixation, only two transient neuropraxia of the radial nerve occurred, which resolved adequately with physiotherapy, showing that, if the technique is followed as described using a blunt separator for the radial nerve, there should not be significant nerve injuries.
In the anatomical study by Mejía et al.²², it was argued that by placing more distal blocked screws, there would be better stability of the fixation that would be maintained in the long-term²². Zhao et al.²⁴ utilized a locking compression plate of 10–14 holes molded to fit the anterior surface of the humerus, fixing it to the lateral or medial columns with only 2 or 3 distal screws that could cause less stability to the distal segment. Yet, the results after follow-ups ranging from 12 to 36 months were satisfactory without the occurrence of nonunions or implant failures²⁴. With our technique, the molded locking plate could be distally fixed with five cortical or blocked screws providing good stability to even the most distal diaphyseal fractures relatively close to the coronoid fossa. After a median of 36.9 months follow-up (min 9.5 – max 62.5), there were no cases of nonunions, malunions, or failures, showing that the reductions and fixation stability were preserved in the mid-and-long term. Additionally, the residual radiographic angulations observed in our series are within the range of acceptable alignment in the osteosynthesis of a distal diaphyseal fracture of the humerus, as has been previously reported by other authors¹⁸,¹⁹,²¹.
One of the possible drawbacks of fixating the locking plate immediately proximal to the coronoid fossa in the most distal fractures with a high density of distal screws placing is the compromise of the elbow’s flexion. Mejía et al.²² suggested that, for optimal functional results, the minimum distance from the most distal edge of the plate to the most proximal part of the capitellum or the FCD should be close to 1 cm²². Given the thinner profile in the distal end of the locking plate, which would allow for closer proximity to the capitellum without interfering with the elbow flexion, we included patients with distal segments ranging from 0.49 to 1.03 cm. Our results showed that even in patients with short segments, the active range of movement and functional score were as satisfactory as those with longer segments. There was only one case in which the patient required the removal of the osteosynthesis material as the patient complained of pain with elbow flexion. However, the patient had complete AROM and excellent MEPS, and after removal around 40 months after the procedure, the patient continued with satisfactory evolution and a stable reduction.
Another concern with the technique proposed by Mejía et al.²² was the possibility of implant failure or loosening secondary to material fatigue caused by the molding needed for adapting to the anatomy of the anterior surface of the humerus. Some of our patients had follow-ups longer than 40 months; still, in all our patients, the implant was intact, in place, and without signs of failure, demonstrating that the modification performed to the plate did not alter its cycling.
The study has some limitations. First, it has a limited sample size and is not powered to prove any hypothesis regarding function improvement or complications. Second, it lacked a control or comparison group that could prove the superiority or no inferiority of the technique concerning other previously published methods. Third, most patients were younger than 40, skewing the results towards the younger population. However, at this time, we can show satisfactory results in ten cases in the mid-to-long term, indicating this technique is a promising alternative of MIPO for patients with distal diaphyseal and meta-diaphyseal humerus fractures.
Conclusion
For meta-diaphyseal and distal diaphyseal extra-articular humerus fractures, a MIPO technique with an anterior approach and anterolateral fixation produced a stable reduction and fixation with satisfactory mid-to-long-term clinical and functional outcomes, low complication rates, and early return of patients to daily life activities that did not involve weight bearing. The technique represents a safe surgical alternative that allows for good visualization of the fracture site with minimal soft tissue disruption and a low risk of radial iatrogenic injury.
Conflicts of Interest Statement:
The authors have no conflicts of interest to declare.
Acknowledgments:
None
Institutional Review Board (IRB):
The IRB approved this study on March 18, 2024 (Universidad Pontificia Bolivariana, file 5 of 2024)
References
1. Mighell MA, Stephens B, Stone GP, Cottrell BJ. Distal Humerus Fractures. Hand Clin [Internet]. 2015 Nov 1;31(4):591–604. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0749071215000736
2. Nowak LL, Dehghan N, McKee MD, Schemitsch EH. Plate fixation for management of humerus fractures. Injury. 2018 Jun 1;49:S33–8.
3. Morrey ME, Morrey BF, Sanchez-Sotelo J, Barlow JD, O’Driscoll S. A review of the surgical management of distal humerus fractures and nonunions: From fixation to arthroplasty. J Clin Orthop Trauma. 2021 Sep 1;20.
4. Beazley JC, Baraza N, Jordan R, Modi CS. Distal Humeral Fractures-Current Concepts. Open Orthop J. 2017 Nov 30;11(1):1353–63.
5. Savvidou OD, Zampeli F, Koutsouradis P, Chloros GD, Kaspiris A, Sourmelis S, et al. Complications of open reduction and internal fixation of distal humerus fractures. Vol. 3, EFORT Open Reviews. British Editorial Society of Bone and Joint Surgery; 2018. p. 558–67.
6. Helfet DL, Kloen P, Anand N, Rosen HS. Open reduction and internal fixation of delayed unions and nonunions of fractures of the distal part of the humerus. The Journal of Bone and Joint Surgery-American Volume. 2003 Jan;85(1):33–40.
7. Vauclair F, Goetti P, Nguyen NT V., Sanchez-Sotelo J. Distal humerus nonunion: evaluation and management. EFORT Open Rev. 2020 May;5(5): 289–98.
8. Piekarczyk P, Kwiatkowski K, Piątkowski K, Gołos J, Kuczmera P. Outcomes after Open Reduction and Plate Fixation of Distal Humerus Fractures. Ortop Traumatol Rehabil. 2015;17(6):627–36.
9. Han SH, Park JS, Baek JH, Kim S, Ku KH. Complications associated with open reduction and internal fixation for adult distal humerus fractures: a multicenter retrospective study. J Orthop Surg Res. 2022 Dec 1;17(1).
10. Jain D, Goyal GS, Garg R, Mahindra P, Yamin M, Selhi HS. Outcome of anatomic locking plate in extraarticular distal humeral shaft fractures. Indian J Orthop. 2017 Jan 1;51(1):86–92.
11. Saracco M, Smimmo A, De Marco D, Palmacci O, Malerba G, Vitiello R, et al. Surgical approach for fracture of distal humerus: Posterior vs lateral. Vol. 12, Orthopedic Reviews. Page Press Publications; 2020. p. 52–7.
12. Teng L, Zhong G, Li HB, Cen S qiang, Liu DH, Li L. Combined Medial and Lateral Approach Versus Paratricipital Approach in Open Reduction and Internal Fixation for Type C Distal Humerus Fracture: A Randomized Controlled Study. Orthop Surg. 2023 Aug 1;15(8):2062–73.
13. Lee TJ, Kwon DG, Na SI, Cha S Do. Modified combined approach for distal humerus shaft fracture: Anterolateral and lateral bimodal approach. Clin Orthop Surg. 2013 Sep;5(3):209–15.
14. Parmaksizoglu A, Ozkaya U, Bilgili F, Mutlu H, Cetin U. Fixation of extra-articular distal humeral fractures with a lateral approach and a locked plate: an alternative method. Acta Orthop Traumatol Turc [Internet]. 2016;2(50):132–8. Available from: https://www.aott.org.tr/en/fixation-of-extraarticular-distal-humeral-fractures-with-a-lateral-approach-and-a-locked-plate-an-alternative-method-133749
15. Benninger E, Meier C. Minimally invasive lateral plate placement for metadiaphyseal fractures of the humerus and its implications for the distal deltoid insertion- it is not only about the radial nerve. A cadaveric study. Injury. 2017 Mar 1;48(3): 615–20.
16. Cañada-Oya H, Cañada-Oya S, Zarzuela-Jiménez C, Delgado-Martinez AD. New, Minimally Invasive, Anteromedial-Distal Approach for Plate Osteosynthesis of Distal-Third Humeral Shaft Fractures An Anatomical Study. JBJS Open Access. 2020 Jan 1;5(1).
17. Yang J, Yang Z, Liu D, Lu Z, Tao C, Liu T. Is an anteromedial minimally invasive approach for middle and distal third humeral fractures feasible? A cadaveric study and clinical case series. Journal of Orthopaedics and Traumatology. 2023 Dec 1;24(1).
18. Jitprapaikulsarn S, Neti N, Thremthakanpon W, Gromprasit A. Anterior minimally invasive plating osteosynthesis using reversed proximal humeral internal locking system plate for distal humeral shaft fractures. European Journal of Orthopaedic Surgery and Traumatology. 2020 Dec 1;30(8):1515–21.
19. Jitprapaikulsarn S, Gromprasit A, Sukha K, Patamamongkonchai C, Jiamton C. Minimally invasive plate osteosynthesis via posterior approach for type B and C fractures of distal humeral shaft: surgical tactics and a clinical series. European Journal of Orthopaedic Surgery and Traumatology. 2023 May 1;33(4):1431–7.
20. Zhiquan A, Bingfang Z, Yeming W, Chi Z, Peiyan H. Minimally Invasive Plating Osteosynthesis (MIPO) of Middle and Distal Third Humeral Shaft Fractures.
21. Tetsworth K, Hohmann E, Glatt V. Minimally Invasive Plate Osteosynthesis of Humeral Shaft Fractures: Current State of the Art. Journal of the American Academy of Orthopaedic Surgeons. 2018 Sep 15;26(18):652–61.
22. Mejía O, Valencia J, Márquez W, Jaramillo J, Ordoñez S, Monsalve F, et al. Minimally invasive osteosynthesis of distal humerus fracture with commercially available pre-contoured plate using an anterolateral fixation: a cadaveric studyMinimally invasive osteosynthesis of distal humerus fracture with commercially available pre-con. Med Res Arch. 2024 Oct;12(10).
23. Cusick MC, Bonnaig NS, Azar FM, Mauck BM, Smith RA, Throckmorton TW. Accuracy and reliability of the Mayo Elbow Performance Score. J Hand Surg Am. 2014 Jun;39(6):1146–50.
24. Zhao W, Qu W, Fu C, Jiang H, Liu S, Cheng C. Antero-lateral minimally invasive plate osteosynthesis (MIPO) with the radial nerve exploration for extra-articular distal-third diaphyseal fractures of the humerus. Int Orthop. 2017 Sep 1;41(9):1757–62.
25. Beeres FJ, Diwersi N, Houwert MR, Link BC, Heng M, Knobe M, et al. ORIF versus MIPO for humeral shaft fractures: a meta-analysis and systematic review of randomized clinical trials and observational studies. Vol. 52, Injury. Elsevier Ltd; 2021. p. 653–63.
26. Rosenlund AMN, Søreide E, Madsen JE, Flugsrud GB, Douglass BW, Midtgaard KS. Outcomes and complications after open reduction and internal fixation of distal humeral fractures with precontoured locking plates. OTA Int. 2022 Dec; 5(4):e220.
27. Shimamoto Y, Tokutake K, Takegami Y, Asami Y, Sato K, Ueno H, et al. Comparative Outcomes of Anterior and Posterior Plating for Distal-Third Humerus Shaft Fractures. Journal of Hand Surgery. 2023;
28. Huang Q, Lu Y, Wang ZM, Sun L, Ma T, Wang Q, et al. Anterolateral approach with two incisions versus posterior median approach in the treatment of middle- and distal-third humeral shaft fractures. J Orthop Surg Res. 2021 Dec 1;16(1).
29. Livani B, Belangero W, Andrade K, Zuiani G, Pratali R. Is MIPO in humeral shaft fractures really safe? Postoperative ultrasonographic evaluation. Int Orthop. 2009 Dec;33(6):1719–23.