Nurses’ Insights on TB Control Programs in Wales
The role of nurses in national TB control programs: qualitative insights from TB cohort review in Wales
Tamas D Barry¹²*, Yvonne Hester³, Philip Pallmann⁴, Emma Thomas-Jones⁴, Jonathan Underwood²⁵, Matthijs Backx⁵, Simon M Barry⁶
- Division of Population Medicine, Cardiff University, Cardiff, UK
- Division of Infection and Immunity, Cardiff University, Cardiff, UK
- Integrated TB Service, Cardiff and Vale University Health Board, Cardiff, UK
- Centre for Trials Research, Cardiff University, Cardiff, UK
- Department of Infectious Diseases, Cardiff and Vale University Health Board, Cardiff, UK
- Department of Respiratory Medicine, Cardiff and Vale University Health Board, Cardiff, UK
[email protected]
[email protected]
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: Barry, T.D., Hester, Y., et al., 2024. The role of nurses in national TB control programs: qualitative insights from TB cohort review in Wales. Medical Research Archives, [online] 12(12).
https://doi.org/10.18103/mra.v12i12.6063
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i12.6063
ISSN 2375-1924
Abstract
Background: Tuberculosis (TB) cohort review was implemented nationally in Wales in 2012 as a systematic process for reviewing all notified cases of TB and evaluating outcomes to improve service delivery. Local TB teams collect outcome data, and then all notified cases are presented for discussion and expert feedback at a multi-disciplinary, all-Wales CR meeting.
Aims: Nurses are crucial in national TB control programs in low-incidence countries, carrying out resource-intensive activities such as contact tracing. This qualitative study aims to explore nurses’ experiences of cohort review, identify successes, and explore barriers to improving TB care.
Methods: Questionnaires were developed using Microsoft Forms and distributed electronically to all nurses involved in TB care across Wales. They used a mixture of Likert-scale and open-ended questions. Qualitative data was analysed using reflexive thematic analysis.
Results: Questionnaire responses were collected from 19/23 (82.6%) nurses. Responses highlighted significant regional disparities in time and resource allocations to TB nursing teams. Thematic analysis results broadly aligned with the quantitative findings, identifying essential areas such as the lack of consultant support and the emotional impacts of presenting at meetings. Despite these challenges, nurses reported that the implementation of CR has improved TB care and fostered a stronger community of TB professionals across Wales.
Conclusion: These findings highlight the necessity of dedicated, well-resourced TB nursing teams in low-incidence countries to ensure the sustainability of high-quality TB care.
Introduction
Tuberculosis (TB) control in low-incidence countries such as Wales presents significant challenges as nations work toward achieving and maintaining elimination targets. TB cases are often complex because many of those at most significant risk belong to marginalised populations who face barriers to healthcare access¹. These include individuals experiencing homelessness, people with substance use disorders, incarcerated individuals, and migrants or asylum seekers from high-incidence countries². Managing these cases, therefore, requires significant input from multidisciplinary teams and imposes a substantial administrative and resource burden. The national TB cohort review (CR) program was implemented nationally in Wales in 2012 as a framework for addressing these challenges. This was part of a strategic approach to improve care coordination, enhance patient outcomes, and strengthen epidemiological surveillance nationwide.
Cohort review is a systematic process of case review and quality assurance. It involves the regular multidisciplinary discussion of all notified cases of active TB in Wales. Meetings involve all local TB teams based in six of Wales’ seven health boards and are attended by consultant physicians, TB clinical nurse specialists or respiratory nurses, public health professionals, and an external TB expert. Nurses typically present cases, with subsequent feedback on clinical case management and implications for the broader epidemiological context of TB in Wales. As nurses are central to the CR process, their experience and insights are vital to continue improving the service.
A qualitative study conducted by Wallis et al. (2016) investigated the experiences of healthcare professionals in TB cohort audit (TBCA) in England, a low-incidence setting. The study highlighted the significance of multidisciplinary collaboration and the development of a “community of practice” to enhance TB care³. Building on these findings, our study aims to examine the specific challenges faced by TB nurses in Wales, given that differences in resource availability and geographic contexts may affect their experiences of care delivery. Literature on national TB control strategies highlights the necessity of providing adequate training, staffing, and support for nurses, particularly in low-incidence countries. A lack of resources and varying levels of support can have a substantial impact on nurses’ ability to effectively perform their duties.
This study examines the experiences of nurses involved in TB CR in Wales, highlighting critical challenges such as resource allocation, time management, and professional support. By understanding these challenges, we aim to inform strategies to strengthen TB control programs, particularly in Wales and comparable low-incidence settings.
Methods
We followed the Standards for Reporting Qualitative Research (SRQR) guidelines when reporting this study⁴. In 2024, questionnaires were distributed to all nurses involved in TB care across Wales. This included clinical nurse specialists (CNS) and respiratory nurses with TB responsibilities. Local TB teams are based in six of Wales’ seven health boards (HBs). In the remaining HB without any major hospitals, patients with complex problems such as TB are managed in other Welsh HBs or England. Given this small cohort, total population sampling was used to ensure that the perspectives of as many nurses as possible were captured⁵.
This study followed a constructivist paradigm, using a narrative approach to explore the experiences of nurses involved in CR⁶. The questionnaires were developed using Microsoft (MS) Forms and included Likert scale questions and open-ended responses. To ensure clarity and relevance, pilot testing was conducted by sending the questionnaire to one nurse and a consultant physician involved in TB care⁷. Nurses were given six weeks to respond, and a reminder email was sent to non-responders after two weeks. All responses were anonymised to ensure confidentiality.
The primary researchers maintain professional relationships with many TB nurses across Wales.
While this may have offered advantages such as ease of access to participants and a deeper understanding of the clinical context, it also raises the possibility of bias⁸. Anonymisation partially mitigated this.
A mixed-methods approach was used for data analysis⁹. Data was manually transcribed from MS Forms to an MS Excel file for analysis. Quantitative data from Likert scale responses were analysed descriptively. The qualitative data, derived from open-ended responses, underwent Reflexive Thematic Analysis (RTA) following Braun and Clarke’s approach¹⁰,¹¹. This process involved several steps:
- Familiarisation: researchers (TDB, YH, SMB) familiarised themselves with the responses by repeatedly reading the data to understand key ideas and initial impressions.
- Initial coding: open-ended responses were systematically coded, with descriptive codes assigned to significant points and recurring ideas.
- Theme development: codes were reviewed and grouped into potential themes that captured broader patterns across the dataset. Themes and sub-themes were refined iteratively to ensure they reflected the nuances in nurses’ experiences.
- Review and refinement: themes were continuously refined to ensure coherence, and some were restructured or combined as the analysis progressed.
- Defining and naming themes: each theme was defined to encapsulate the key insights it represented, ensuring that the final themes accurately depicted the experiences and challenges of nurses in TB CR.
RTA was chosen for its flexibility in exploring nuanced, context-specific insights into TB nurses’ experiences. This approach allowed the researchers to engage reflexively with the data, particularly capturing anticipated and emergent themes, which aligned well with the study’s qualitative focus¹²,¹³.
To enhance the trustworthiness of the analysis, a member-checking process was undertaken¹⁴. One of the authors (YH), a TB nurse and participant in the study, reviewed a summary of the findings and provided feedback. This feedback was used to refine the analysis and ensure that the themes accurately represented the experiences and perspectives of TB nurses involved in CR. This step contributed to the credibility of the findings by attempting to align the analysis with participants’ intended meanings. As a participant in the study however, this had the potential to introduce bias.
This study received a favourable ethical opinion from the Central Bristol Research Ethics Committee (reference number 23/SW/0089) and was registered under IRAS project ID 321836.
Results
There are twenty-three nurses involved in TB care across Wales, and 19 responded to the questionnaire (82.6% response rate). Of these, four (17.4%) were TB CNS; the remainder worked primarily as respiratory nurses. Table 1 presents the distribution of respondents across the six included HBs.
Table 1: Distribution of nurses who responded to the questionnaire across health boards in Wales and time allocated each week for TB-specific work
| Health Board | No. of respondents | 1 Day or Less | 2 Days | 3 Days | 4 Days | 5 Days |
|---|---|---|---|---|---|---|
| 1 | 1 | 0 | 0 | 1 | 0 | 0 |
| 2 | 5 | 4 | 0 | 1 | 0 | 0 |
| 3 | 3 | 0 | 0 | 0 | 0 | 3 |
| 4 | 6 | 6 | 0 | 0 | 0 | 0 |
| 5 | 1 | 0 | 0 | 0 | 0 | 1 |
| 6 | 3 | 0 | 1 | 2 | 0 | 0 |
| Total (%) | 19 (100.0) | 10 (52.6) | 1 (5.3) | 4 (21.1) | 0 (0.0) | 4 (21.1) |
Abbreviations: TB = tuberculosis
Most respondents reported positive effects of CR on communication and collaboration. As shown in figure 1, 12/19 (63.2%) agreed or strongly agreed that CR improved communication within TB teams, and 16/19 (84.2%) felt or strongly felt that it improved communication across Wales. Despite these benefits, there was notable variability in responses, with some indicating mixed experiences.
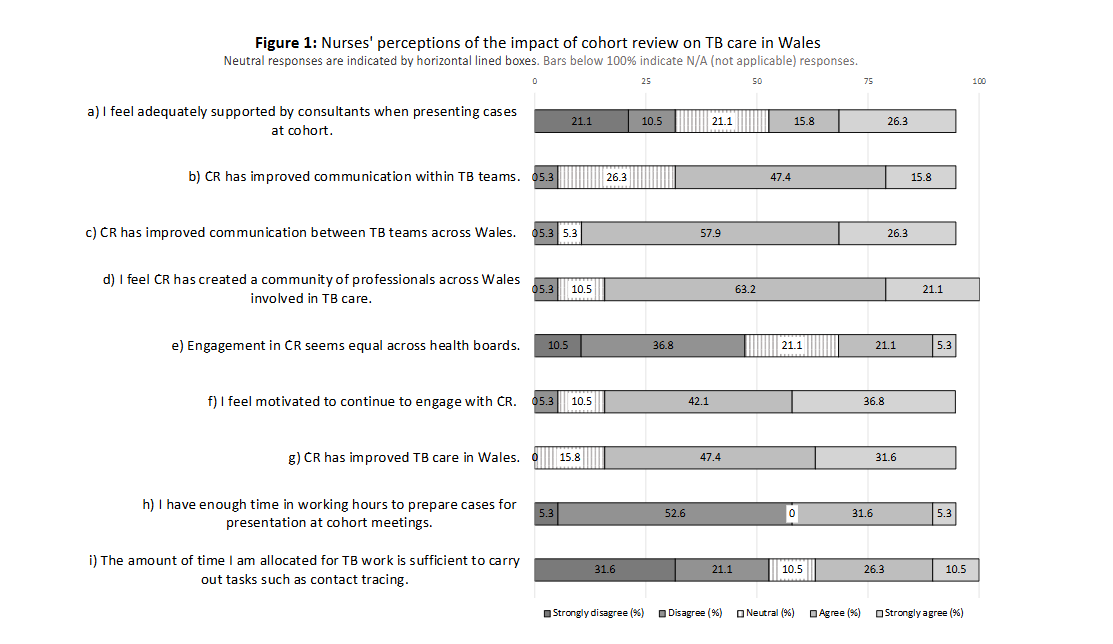
Most respondents reported positive effects of CR on communication and collaboration. As shown in figure 1, 12 (19.1) and 16 (19.1) strongly felt that CR improved communication within TB teams, while 16 (19.1) felt strongly that it improved communication across Wales. Despite these benefits, there was notable variability in responses, with some indicating mixed experiences.
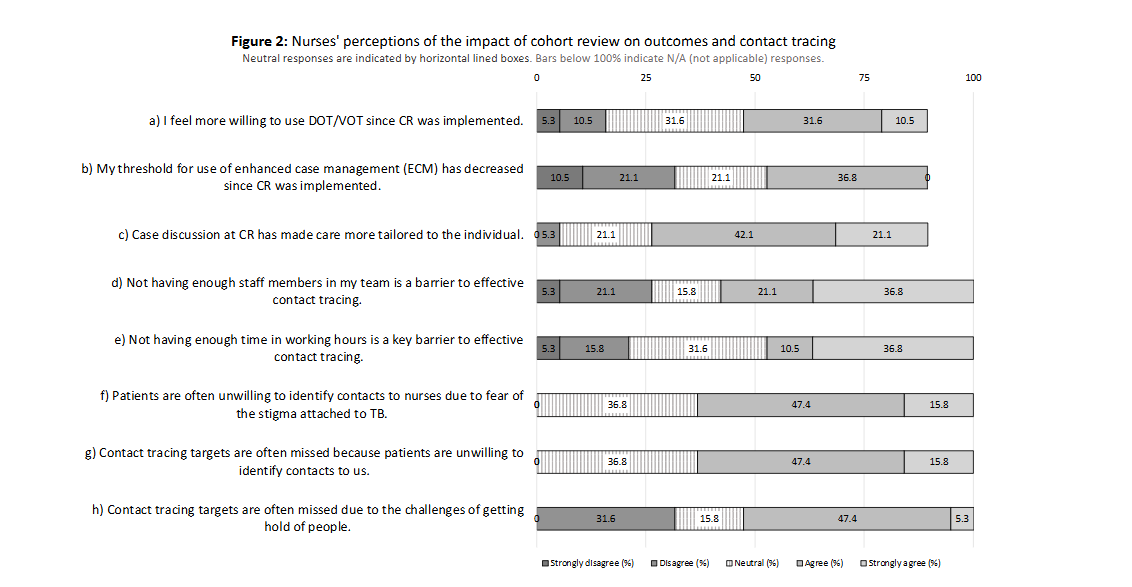
Figure 2 highlights that time constraints and patient communication are critical barriers to effective contact tracing. Some respondents, 11/19 (57.9%), agreed or strongly agreed that limited staffing hinders patient care, but only 9/19 (47.3%) viewed time constraints as a significant challenge. A further 12/19 (63.2%) felt that case discussion at CR had led to more individualised care.
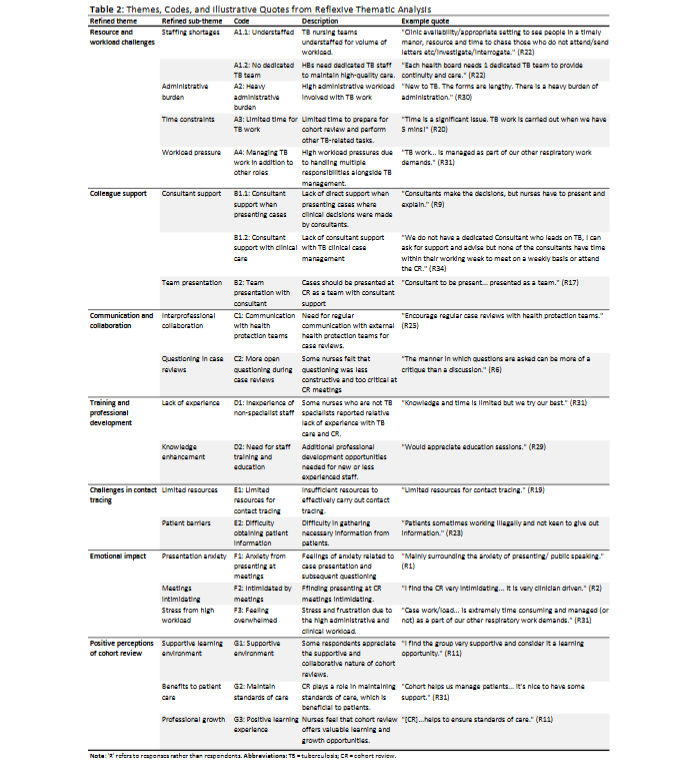
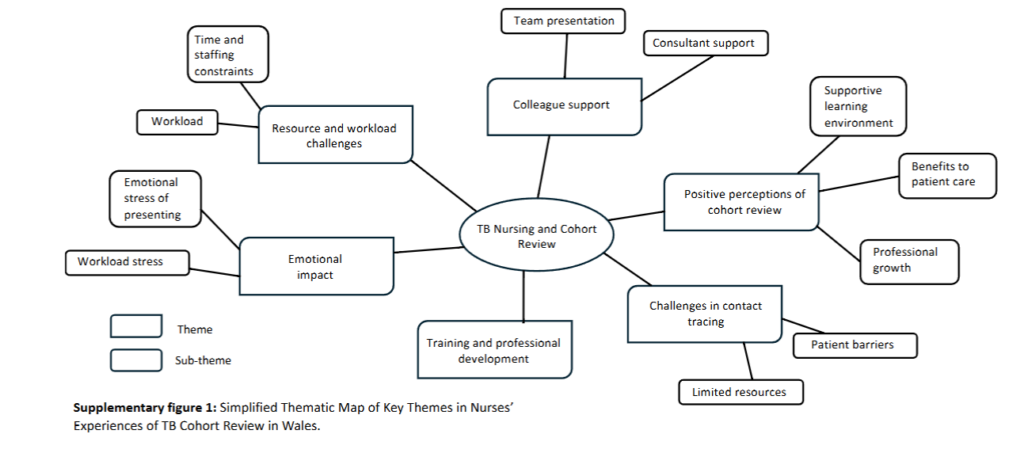
The full results of the RTA are shown in table 2. ‘R’ refers to responses rather than respondents. There were 34 open-ended responses in total (R1 – R34). The initial thematic analysis, including all responses to open-ended questions, can be found in supplementary tables 1a and 1b. A simplified schematic of the main themes and sub-themes involved in the analysis is shown in supplementary figure 1. The results reveal a significant thematic overlap between the quantitative and qualitative data, particularly around time and resource constraints as barriers to effective TB care. Time limitations (A3) and staffing shortages (A1.1) were consistently highlighted by respondents as key obstacles. Furthermore, the need for consultant support during case presentations (B1.1 and B1.2) was frequently mentioned, with nurses expressing the desire for more direct support in presenting cases where consultants made clinical decisions.
Table 2: Themes, Codes, and Illustrative Quotes from Reflexive Thematic Analysis
| Refined theme | Refined sub-theme | Code | Description | Example quote |
|---|---|---|---|---|
| Resource and workload challenges | Staffing shortages | A1.1 | Understaffed TB nursing teams for volume of workload. | “Clinic availability/appropriate setting to see people in a timely manor, resource and time to chase those who do not attend/send letters etc/investigate/interrogate.” (R22) |
| No dedicated TB team | A1.2 | HBs need dedicated TB staff to maintain high-quality care. | “Each health board needs 1 dedicated TB team to provide continuity and care.” (R22) | |
| Administrative burden | A2 | High administrative workload involved with TB work. | “New to TB. The forms are lengthy. There is a heavy burden of administration.” (R30) | |
| Time constraints | A3 | Limited time for TB work. | “Time is a significant issue. TB work is carried out when we have 5 mins!” (R20) | |
| Workload pressure | A4 | High workload pressures due to handling multiple responsibilities alongside TB management. | “TB work… is managed as part of our other respiratory work demands.” (R31) |
Note: ‘R’ refers to responses rather than respondents. Abbreviations: TB = tuberculosis; CR = cohort review.
Discussion
TB control programs in low-incidence countries have made progress in reducing TB incidence over recent decades, though the rate of decline has recently slowed in many areas¹⁵. Nurses, who undertake most of the work associated with TB care alongside health protection teams, are central to the success of these programs. This study highlights priority action areas, focussing on regional disparities, time pressures, and the evolving role of nurses in TB CR in Wales. It has implications for similar low-incidence settings.
Most respondents in this study acknowledged that TB CR had improved TB care in Wales and enhanced communication within and between teams (G1, G2). The process of CR was also seen as a positive learning experience (G3). However, the disparities in resource allocation, staffing, and time devoted to TB-specific care across HBs remain significant (A1.1, A3). While some HBs have dedicated nurses, others do not, and nurses are often required to undertake TB work in addition to their regular duties in respiratory medicine (A4). Several respondents highlighted the need for dedicated TB teams in all HBs (A1.2). Without dedicated TB teams, nurses are stretched thin, leading to variability in the quality of care. This is particularly important given the complexity of TB case management, where continuity and dedicated time are essential for successful outcomes¹⁶.
The resource and time constraints nurses report have broader implications for the effectiveness of TB control programs¹⁷,¹⁸. The frustration voiced by nurses over inadequate time allocation highlights the need for HBs to reassess how TB nursing roles are structured and supported. Ensuring that nurses have sufficient time to perform TB-related tasks enhances the quality of care. It also improves the effectiveness of contact tracing, which is critical for preventing outbreaks in low-incidence settings and arresting community transmission. This is a crucial aspect of many elimination strategies¹⁹. Compounding these challenges, the patient stigma around TB further hinders contact tracing, as patients are often reluctant to identify contacts, making it even more essential that nurses are given the time and resources needed to build trust and overcome these barriers (E2)²⁰.
Moreover, consultants’ lack of consistent support during CR meetings was a recurring theme (B1.1, B1.2). While nurses are responsible for much of the day-to-day management of TB cases, the critical clinical decisions ultimately rest with consultants. When coupled with time pressures and inadequate preparation, this dynamic can leave nurses feeling unsupported and potentially increase anxiety when presenting (F1, F2). To address this, there is a need for stronger collaboration between nurses and consultants, with consultants providing support for nurses presenting shared cases, thus ensuring that nurses feel more confident in presenting cases (F1)²¹,²². CR meetings offer an opportunity for continuous learning and professional development, but this is greatly helped by supportive consultant colleagues (D1, D2)²³.
The broader context of TB care in Wales reflects the struggles faced by many low-incidence countries in maintaining political and financial support for TB programs. As the incidence of TB declines, there is a risk of reduced commitment to these programs, a concept known as “Brown’s Law”²⁴,²⁵. This phenomenon, observed in other infectious disease control programs, highlights the danger of complacency. For TB control efforts to succeed in the long term, sustained investment and political will are essential, even as the disease becomes rarer²⁶,²⁷. The situation is further complicated by the UK National Health Service (NHS) context, where chronic underfunding has led to healthcare staff increasingly experiencing burnout due to rising workloads and resource constraints. This was particularly evident during the COVID-19 pandemic²⁸. This overburdened system makes it more difficult for healthcare workers to dedicate time and attention to TB care. Without sufficient investment, the risk of staff burnout could further erode the quality of care provided²⁹. The resurgence of diseases like syphilis, after political
support for active case finding waned, serves as a cautionary example of what could happen if TB control programs are not maintained²⁴.
There are several limitations to this study. Firstly, the sample size is small, which may limit generalisability to other settings, particularly countries with larger populations or different healthcare systems. Further, primary researchers’ professional relationships with study participants may have influenced responses, potentially leading to participants responding in a manner that they felt aligned with research expectations. This seems unlikely, though, as all responses were anonymous, and many respondents were candid in their open-ended feedback. Moreover, researchers were not present at the time of data collection.
Furthermore, while a study participant was involved in the RTA’s member-checking process, the research team felt that the value of having a nurse involved with TB care in Wales verify the identified themes outweighed the potential for bias. Given Wales’ small size and limited number of TB staff, this situation was challenging to avoid. Including an external reviewer may have reduced this bias, but it could have compromised the depth of understanding of the CR process and the nuances of TB care in Wales.
The reflexive approach to analysis allowed us to explore sensitive themes, such as the need for consultant support, with empathy and respect for the challenges described by participants. By recognising the power dynamics and pressures faced in CR meetings, we could delve into these issues in a way that remained mindful of nurses’ experiences, enhancing the depth of the analysis and supporting a respectful interpretation of the data. While this reflexive stance facilitated a deeper understanding of the data, it may also emphasised specific themes, such as time constraints and staffing shortages, reflecting the researchers’ professional awareness of these issues. Throughout the RTA process, we remained attentive to our own experiences and perspectives within the TB care setting, aiming to provide a nuanced understanding of participants’ experiences while acknowledging the potential influence of our perspectives on the analysis.
Therefore, our findings highlight three priority action areas for enhancing TB care in Wales and other low-incidence countries with sufficient resources. First, local health authorities should have dedicated nursing teams. The quality and consistency of TB case management could be improved by ensuring that nurses can focus exclusively on TB care without competing responsibilities. Second, consultants should be present at CR meetings to provide support. This will help build confidence among staff, ensure better decision-making, and strengthen the overall collaborative dynamic of CR. Finally, offering more targeted and frequent training to TB nurses – an actionable intervention now that doesn’t require significant resources – could empower staff when handling complex cases. Addressing these priorities requires immediate, practical actions and sustained investment in resources and staffing to create a resilient TB care system.
Conclusion
In this study, we identified several critical challenges faced by the national TB control program in Wales, particularly concerning resource allocation, staffing and consultant support. Our findings emphasise nurses’ vital contributions to the success of TB CR and broader TB control efforts. We have suggested priority areas for health services to enhance TB care, emphasising the need for dedicated nursing teams. Notably, despite the barriers identified, nurses reported that TB CR has positively impacted TB care in Wales, and they remain motivated to continue their involvement in the program. These findings are relevant to Wales and offer valuable insights that can be applied to other low-incidence countries.
Conflict of Interest Statement:
The authors declare no conflicts of interest.
Acknowledgement Statement:
We gratefully acknowledge the contributions of the nurses who participated in this research and the TB teams involved in CR across Wales. The lead author would also like to thank his PhD supervisors for their invaluable support and guidance.
References
[2] Villar-Hernández R, Ghodousi A, Konstantynovska O, Duarte R, Lange C, Raviglione M. Tuberculosis: current challenges and beyond. Breathe. 2023;19(1). doi:10.1183/20734735.0166-2022
[3] Wallis SK, Jehan K, Woodhead M, Cleary P, Dee K, Farrow S, et al. Health professionals’ experiences of tuberculosis cohort audit in the North West of England: a qualitative study. BMJ Open. 2016;6(3). doi:10.1136/bmjopen-2015-01053
[4] O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: A synthesis of recommendations. Acad Med. 2014;89(9):1245-1251. doi:10.1097/ACM.00 0000000000388
[5] Onwuegbuzie AJ, Leech NL. Sampling Designs in Qualitative Research: Making the Sampling Process More Public. Qual Rep. 2007;12 (2): 238-254. doi:10.46743/2160-3715/2007.1636
[6] Lee CJG. Reconsidering Constructivism in Qualitative Research. Educ Philos Theory. 2012;44 (4):403-412. doi:10.1111/j.1469-5812.2010.00720.x
[7] Malmqvist J, Hellberg K, Möllås G, Rose R, Shevlin M. Conducting the pilot study: A neglected part of the research process? methodological findings supporting the importance of piloting in qualitative research studies. Int J Qual Methods. 2019;18. doi:10.1177/1609406919878341
[8] Williams V, Boylan AM, Nunan D. Critical appraisal of qualitative research: Necessity, partialities and the issue of bias. BMJ Evid Based Med. 2020;25 (1):9-11. doi:10.1136/bmjebm-2018-111132
[9] Liamputtong P. Qualitative data analysis: Conceptual and practical considerations. Health Promot J Austr. 2009;20(2):133-139. doi:10.1071/ he09133
[10] Byrne D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual Quant. 2022;56(3):1391-1412. doi:10.1007/ s11135-021-01182-y
[11] Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4): 589-597. doi:10.1080/2159676X.2019.1628806
[12] Braun V, Clarke V. Is thematic analysis used well in health psychology? A critical review of published research, with recommendations for quality practice and reporting. Health Psychol Rev. 2023;17(4):695-718. doi:10.1080/17437199.2022.2161594
[13] Campbell KA, Orr E, Durepos P, Nguyen L, Li L, Whitmore C, et al. Reflexive thematic analysis for applied qualitative health research. Qual Rep. 2021 ;26(6):2011-2028. doi:10.46743/2160-3715/2021.5010
[14] Candela AG. Exploring the Function of Member Checking. Qual Rep. 2019;24(3), 619-628. doi: 10.46743/2160-3715/2019.3726
[15] European Centre for Disease Prevention and Control. Tuberculosis surveillance and monitoring in Europe 2024 – 2022 data. https://www.ecdc.europa.eu/en/publications-data/tuberculosis-surveillance-and-monitoring-europe-2024-2022-data. Published March 2024. Accessed November 28, 2024.
[16] Public Health England. Collaborative Tuberculosis Strategy for England 2015 to 2020. https://assets.publishing.service.gov.uk/media/5a755625e5274a3cb28699eb/Collaborative_TB_Strategy_for_England_2015_2020_.pdf. Published January 2015. Accessed November 28, 2024.
[17] D’Ambrosio L, Dara M, Tadolini M, Centis R, Sotgiu G, Van Der Werf MJ, et al. Tuberculosis elimination: Theory and practice in Europe. Eur Respir J. 2014;43(5):1410-1420. doi:10.1183/0903 1936.00198813
[18] Erkens CGM, Kamphorst M, Abubakar I, Bothamley GH, Chemtob D, Haas W, et al. Tuberculosis contact investigation in low prevalence countries: A European consensus. Eur Respir J. 2010;36(4):925-949. doi:10.1183/090319 36.00201609
[19] Matteelli A, Rendon A, Tiberi S, Al-Abri S, Voniatis C, Carvalho ACC, et al. Tuberculosis elimination: Where are we now? Eur Respir Rev. 2018;27(148). doi:10.1183/16000617.0035-2018
[20] Faccini M, Cantoni S, Ciconali G, Filipponi MT, Mainardi G, Marino AF, et al. Tuberculosis-related stigma leading to an incomplete contact investigation in a low-incidence country. Epidemiol Infect. 2015;143(13):2841-2848. doi:10.1017/S095 026881400394X
[21] Amudah P, Hamidah H, Annamma K, Ananth N. Effective communication between nurses and doctors: Barriers as perceived by nurses. J Nurs Care. 2018; 07(03). doi:10.4172/2167-1168.1000455
[22] Tabak N, Orit K. Relationship between how nurses resolve their conflicts with doctors, their stress and job satisfaction. J Nurs Manag. 2007;15 (3):321-331. doi:10.1111/j.1365-2834.2007.00665.x
[23] Snelgrove S, Hughes D. Interprofessional relations between doctors and nurses: Perspectives from South Wales. J Adv Nurs. 2000;31(3):661-667. doi:10.1046/j.1365-2648.2000.01321.x
[24] Williams LA, Klausner JD, Whittington WL, Handsfield HH, Celum C, Holmes KK. Elimination and reintroduction of primary and secondary syphilis. Am J Public Health. 1999;89(7):1093-1097. doi:10.2105/ajph.89.7.1093
[25] Valentine JA, Bolan GA. Syphilis Elimination: Lessons Learned Again. Sex Transm Dis. 2018;45(9 S):S80-S85. doi:10.1097/OLQ.0000000000000842
[26] Raviglione M, Marais B, Floyd K, et al. Scaling up interventions to achieve global tuberculosis control: Progress and new developments. The Lancet. 2012;379(9829):1902-1913. doi:10.1016/s 0140-6736(12)60727-2
[27] Reid MJA, Arinaminpathy N, Bloom A, Bloom BR, Boehme C, Chaisson R, et al. Building a tuberculosis-free world: The Lancet Commission on tuberculosis. The Lancet. 2019;393(10178): 1331-1384. doi:10.1016/S0140-6736(19)30024-8
[28] British Thoracic Society. Impact of COVID-19 on Tuberculosis Services in the UK – Survey Report April 2022. April, 2022. Accessed November 28, 2024. https://www.brit-thoracic.org.uk/quality-improvement/covid-19/impact-of-covid-19-on-tuberculosis-services-in-the-uk-survey-report/.
[29] Care Quality Commission (CQC). State of Care: The Health and Care Workforce. https://www.cqc.org.uk/publications/major-report/state-care/2022-2023/workforce. Published October 2023. Accessed October 6, 2024.
[30] UK Parliament. Workforce Burnout and Resilience in the NHS and Social Care: Second Report of Session 2021-22. https://committees.parliament.uk/work/494/workforce-burnout-and-resilience-in-the-nhs-and-social-care/publications/ .Published June 2021. Accessed October 6, 2024.
Supplementary Materials
Supplementary table 1a: Initial thematic coding of responses R1 – R17
| Response ID | Excerpt | Code | Theme |
|---|---|---|---|
| R1 | Mainly surrounding the anxiety of presenting/ public speaking. | Anxiety | Emotional impact of meetings |
| R2 | I find the CR very intimidating, I feel at times the cases are challenged and it is the nurses that are questioned with regard to management and treatment plans that is poorly directed. Maybe the doctors should present. It is very clinician driven and not particularly an open reflective session. | Intimidating, Lack of support, Communication | Emotional impact of meetings, Better consultant support, More open communication |
| R3 | Limited time to prep for meetings. | Time | Time constraints |
| R4 | New to disease area. | Inexperience | Lack of experience |
| R5 | Time to prepare. Time to attend. Feel a little intimidated (it’s not the only thing we do so knowledge base is not as up to date as others in the group). | Intimidating, Time, Inexperience, Training and development | Emotional impact of meetings, Time constraints, Lack of experience, Need for training/teaching |
Supplementary table 1b: Initial thematic coding of responses R18 – R34
| Response ID | Excerpt | Code | Theme |
|---|---|---|---|
| R18 | Not applicable – but from previous experience a TB consultant lead in Cwm Taf (RGH) would be beneficial. | Resource and staffing constraints, Consultant support | Lack of consultant support, Need for dedicated TB staff |
| R19 | It is clear that contact tracing is a challenge and as TB work is sporadic this is short staffed when needed. | Resource and staffing constraints, Contact tracing | Challenges in contact tracing, Lack of staff |
| R20 | Time is a significant issue. TB work is carried out when we have 5 mins! | Time constraints | Lack of time |
| R21 | It is not a funded service in Swansea. So we do the TB work out of Asthma hours. | Resource and staffing constraints | Lack of staff, Unfunded TB service |
| R22 | Clinic availability/appropriate setting to see people in a timely manor, resource and time to chase those who do not attend/send letters etc/investigate/interrogate. | Resource and staffing constraints, Time constraints, Heavy administrative burden | Lack of space, lack of time, lack of resources |
Supplementary figure 1: Simplified Thematic Map of Key Themes in Nurses’ Experiences of TB Cohort Review in Wales.