





Challenges in Managing Congenital Conductive Hearing Loss
Conductive hearing loss – “Need to think out of the box”
Dr Hitha K¹, Dr Sunil Kumar K P², Dr Nambiar Sapna S³
- Senior resident, Department of Otorhinolaryngology, Government Medical College, Kozhikode
- Professor and Head of Department, Department of Otorhinolaryngology, Government Medical College, Kozhikode
- Professor (CAP), Department of Otorhinolaryngology, Government Medical College, Kozhikode
OPEN ACCESS
PUBLISHED: 30 December 2024
CITATION: Hitha, K., et al., 2024, Challenges of Clinical Pharmacogenomics Implementation in the Era of Precision Medicine. Medical Research Archives, [online] 12(12).
https://doi.org/10.18103/mra.v12i12.6192
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i12.6192
ISSN 2375-1924
ABSTRACT
Background:
Conductive hearing loss in children is usually acquired. However, congenital causes ranging from deformities of the external and middle ear to isolated malformations of the ossicular chain are noted. The incidence of congenital middle ear anomalies is 0.28 per 1,00,000 persons. The diagnosis and management are both not only challenging but demanding with respect to surgical expertise, to ensure optimum outcome in terms of hearing and thereby improved quality of life.
Case report:
Our patient, a 7-year-old boy, was referred with complaints of decreased hearing noticed for the past 2 years. The clinical examination was normal except for left preauricular sinus and skin tag. Audiological evaluation showed bilateral moderately severe conductive hearing loss with ‘Ad’ type tympanogram on left side. HRCT temporal bone showed agenesis of right stapes and dysplastic left stapes. Exploratory tympanotomy on left side under general anaesthesia revealed a deformed incus with only an arch of bone in the area of stapes and the facial nerve coursing through the arch. The intra-operative identification of the congenital anomaly was followed by appropriate ossicular reconstruction with aim to restore hearing and avoid facial palsy. A fenestra was created anterior to the arch and Teflon piston placed from malleus (Malleovestibulopexy). The post-operative hearing improvement was beneficial to the patient with an air-bone gap closure to 15 dB on pure tone audiometry.
Conclusion:
Congenital anomalies of middle ear are relatively rare. Early identification of anomalies and anatomical variants, through proper preoperative evaluation along with imaging techniques, is necessary to initiate appropriate treatment ensuring improved quality of life.
Keywords:
Congenital conductive hearing loss, tympanotomy, stapes anomaly, ossicular deformity
Introduction
Hearing loss is an enigmatic condition, which affects the day-to-day life of a person and constitutes a public health concern globally. Currently more than 1.5 billion people (approximately 20% of global population) live with hearing loss as per WHO statistics (7th March, 2023). The prevalence of hearing loss in general population in India varies between 6–26.9%.[1][2] In children, prevalence of hearing loss is 6.6–16.47%.[1] In children conductive hearing loss (CoHL) is mostly due to acquired causes like otitis media with effusion, cholesteatoma etc. The incidence of congenital CoHL due to deformities of middle ear is 1 in 15,000.[3]
Hearing, one of the basic 5 senses marking is gifted with is essential for communication, social existence and at times protection from perils. Hearing loss is detrimental to human development at all ages. However, children are more affected as their overall development depends on their ability to hear. The incidence of congenital CoHL is less which may be either due to delay in identifying the same by parents or timely diagnosing the condition by specialists. Early diagnosis and prompt intervention is necessary in such cases, which could make great differences in the quality of life of these children as well as their family. This case report highlights the clinical profile with need for appropriate diagnosis and treatment in a child with congenital CoHL.
Case Report
7-year-old boy, preterm delivery, born out of a non-consanguineous marriage was referred with the complaints of decreased hearing and poor scholastic performance over 2 years. The child had a history of congenital heart disease (small atrial septal defect) diagnosed at 1 year of age and evaluation revealed ectopic kidney on right side, for which he was on follow up. Pediatric evaluation ruled out any syndromic association.
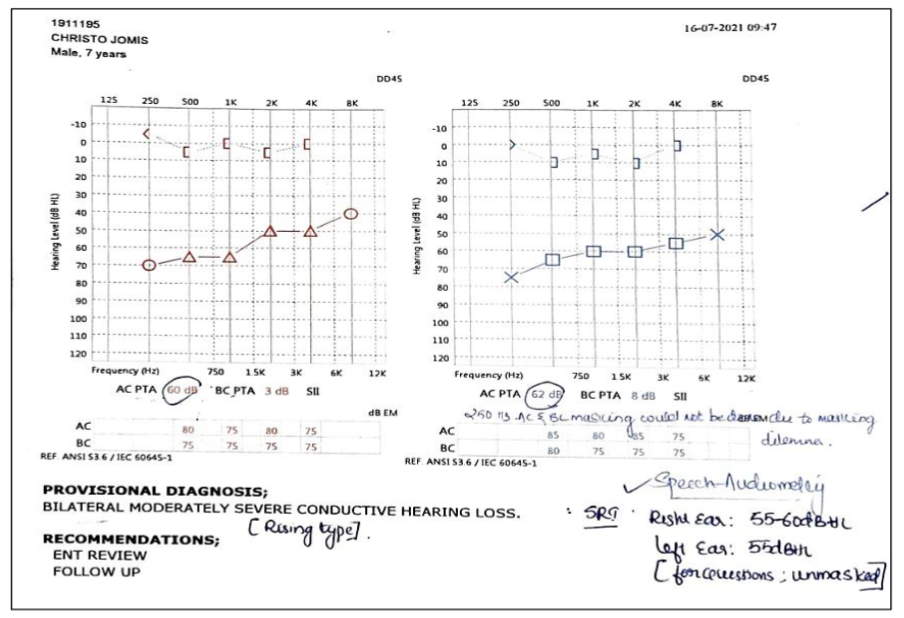
On examination left ear showed preauricular sinus and skin tag. (Fig.1) External auditory canal and tympanic membrane were normal bilaterally. Tuning fork tests showed bilateral CoHL with the same confirmed on pure tone audiometry (PTA) wherein both ears had an air-bone gap of 40–50 dB. (Fig.2) The tympanometry findings revealed ‘Ad’ curve in the left ear and ‘A’ curve in the right ear.
Fig.1. Left pre auricular skin tag

Fig.2. Pure tone audiogram (PTA) showing bilateral moderately severe CoHL
Otoendoscopy and diagnostic nasal endoscopy were normal. High resolution computed tomography (HRCT) of temporal bone showed agenesis of right stapes and dysplastic left stapes with aberrant course of facial nerve (Fig. 3, 4 & 5).
The parents were explained the treatment options with need for exploratory tympanotomy. The patient was then posted for the surgery of left ear with intraoperative findings revealing deformed incus, with only an arch of bone of stapes with fixed footplate.
(Fig.6). Facial nerve was seen traversing through the stapes arch. The need to preserve the facial nerve and improve the hearing was the felt need for optimum outcome. Therefore, a fenestra was made in the footplate of stapes anterior to the deformed remnant of the supra structure of stapes and a Teflon piston (0.4 × 6 mm) was used to bridge the gap from the footplate to the neck of malleus (Malleovestibulopexy). (Fig.7)
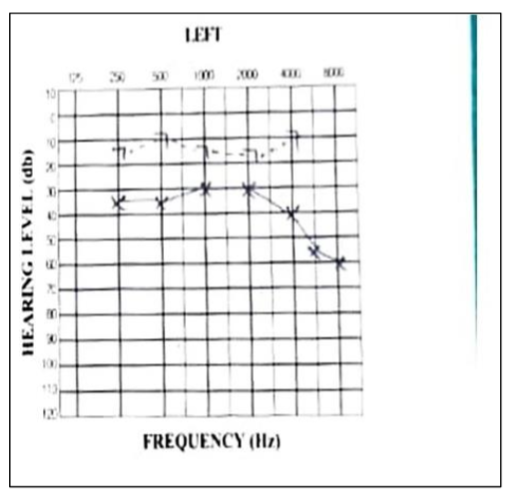
Post operative period was uneventful. Hearing recovery showed an improvement with closure of air-bone gap to 15 dB, 4 weeks post surgery. (Fig.8)
Fig.3. HRCT temporal bone – Coronal section left side showing facial nerve escaping the facial canal
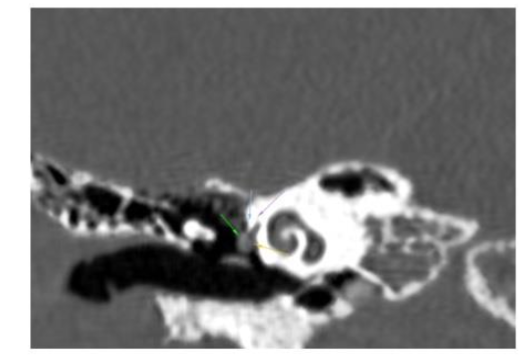
Fig.4. HRCT temporal bone – coronal section left side showing only ossicular status
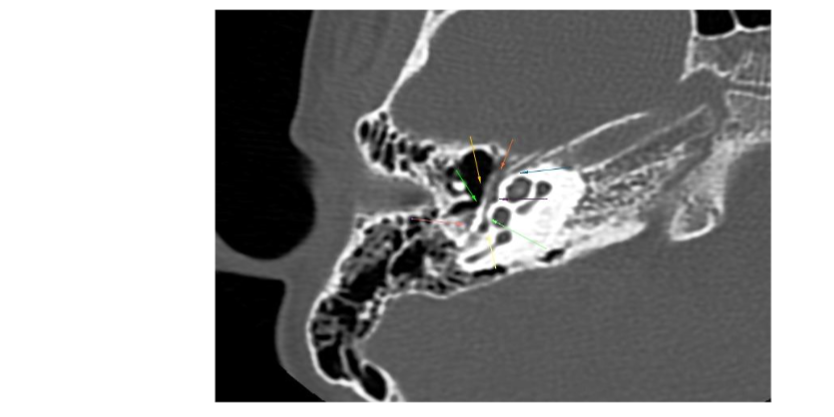
Fig.5. HRCT temporal bone – left side axial section showing facial nerve escaping through facial canal and coursing the promontory, through the deformed stapes

Fig.6. Intraoperative microscopic picture left ear showing an arch of bone at the level of oval window with the facial nerve traversing the arch
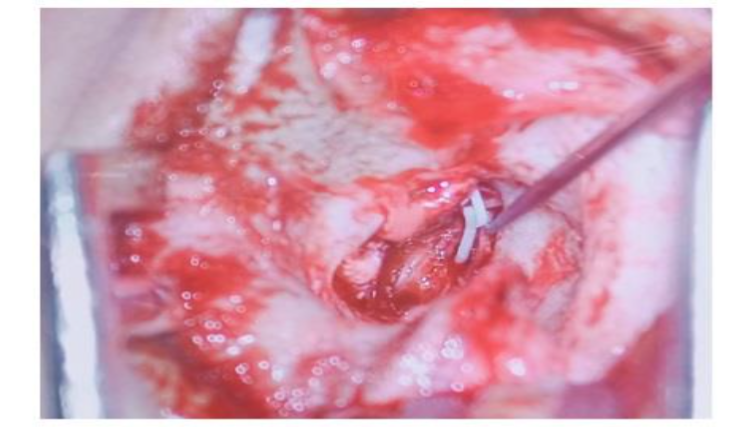
Fig.7. Intraoperative microscopic image left ear showing insertion of Teflon piston (0.4 × 6 mm) from the fenestra in the footplate of stapes hooked to the neck of malleus
Fig.8(a) Pre op PTA of left ear
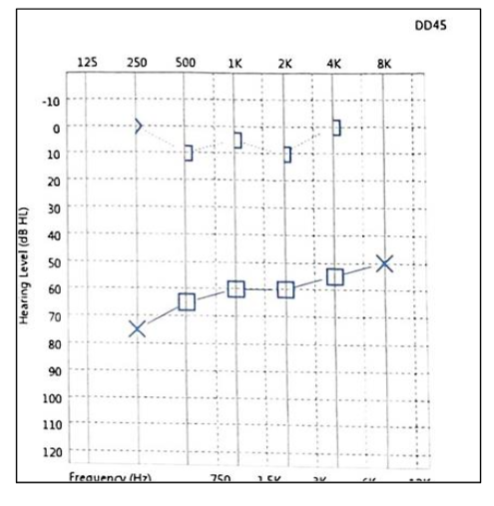
Fig.8(b) Post op PTA in left ear showing improvement
Discussion
CoHL is treatable, but congenital CoHL is an entity that calls for detailed evaluation and timely treatment. Congenital CoHL resulting from pathology of middle ear represents a rare cause of hearing impairment even at tertiary referral centers[3][4] and this entity discusses hearing loss caused by congenital malformations of middle ear with an intact tympanic membrane. Incidence among children with conductive hearing impairment is between 0.5 and 1.2%.[5][6]
The most common causes for CoHL were stapes fixation (33%) and malleus fixation (33%). It can also be associated with syndromes like Apert syndrome. Congenital CoHL due to ossicular deformities can be treated by either rehabilitation with hearing aid or surgical reconstruction.[3]
Development of stapes footplate, oval window and facial nerve canal are interrelated. Stapes develops between the fifth and sixth week of embryonic development from second branchial arch (Reichert’s cartilage).
cartilage) and from otic capsule. Facial nerve also emerges from otic capsule and Reichert’s cartilage during a similar time as that of stapes. So, any abnormality in development of either of these will affect one another.[7]
The decision to operate on ear with congenital ossicular malformation is controversial. Indications for treating congenital conductive hearing loss are diverse and no uniform criteria are universally accepted. Teunissen and Cremers proposed a classification system in 1993, that employs 4 major classes of minor anomalies of middle ear. (Table 1) This classification is a recent one developed mainly from surgical viewpoint to categorize surgical finding and to further analyse the outcomes of interventions.[8][9]
Table 1. Teunissen and Cremers classification
CLASS 1
Anomaly: Isolated stapes ankylosis
Treatment option: Stapedotomy
CLASS 2
Anomaly: Stapes ankylosis associated with other ossicular malformations
Treatment option: Stapedotomy
CLASS 3
Anomaly: Deformity of ossicular chain with mobile stapes footplate
Treatment option: Tympanoplasty with ossicular reconstruction
CLASS 4
Anomaly: Aplasia or severe dysplasia of oval window or round window
Treatment option: Auditory rehabilitation with conventional or BAHA (bone anchored hearing aid) prosthesis
As per the above classification, our patient belongs to class 2, but with an aberrant course of facial nerve. Though we made a stapedotomy for this patient, owing to the deformed incus we had to modify ossiculoplasty to place the prosthesis on to the handle of malleus. This technique, also known as malleovestibulopexy, is utilized when the incus is absent or unsuitable for prosthesis attachment. The technique involves connecting the malleus directly to the vestibule (via the oval window) using a prosthesis, bypassing the missing or defective incus improving the sound conduction.[1]
A sound radiological knowledge with study of the HRCT on the console helps in being prepared for the surgery, which may be beneficial in correcting the deformity benefitting the patient. The principal role of the radiologist in case of exploratory tympanotomy is to guide the surgeon by predicting difficulties which may be encountered during surgery. High resolution computed tomography (HRCT) of the temporal bone is the investigation of choice before surgery, but it is not performed on a routine basis for uncomplicated cases. In a study, Zeifer et al. reported that HRCT enables preoperative diagnosis of anomalous course of the facial nerve as well as absence of the oval window. This is likely due to advancements in CT imaging, allowing high spatial resolution and image quality.[10]
The decision to operate on congenital middle ear anomalies is made individually based on the estimated short and long-term benefit in patients after surgery, and is weighed against the possible risks during and after surgery (hearing deterioration, inner ear damage and chorda tympani or facial nerve injury).[11] During surgery the identification of the anomalies called for meticulous dissection to reconstruct the hearing mechanism with preservation of the facial nerve. Surgical expertise is also the need of the hour in treating congenital ossicular malformations. In a study by Kisilevsky et al., better hearing outcomes with surgery was achieved in class 1 to 3 anomaly, compared to poor or mixed outcome in class 4 anomaly.[12]
The malleovestibulopexy done in our case helped restore the hearing with significant improvement in the patient who was able to attend school and do his daily chores much better than his pre-operative status.
This outcome highlights the potential benefits of tailored surgical interventions in managing congenital CoHL due to ossicular malformations.
Conclusion
Hearing is a special sense that needs due care at the right time. Conductive hearing loss is common in children, of which congenital CoHL can be challenging with respect to diagnosis and treatment. In our patient with congenital CoHL an appropriate clinico-radiological co-relation helped in identifying the pathology which was in the region of development of 2nd branchial arch for which an exploratory tympanotomy with ossicular reconstruction was done with significant improvement in hearing. The meticulous evaluation, early diagnosis and appropriate surgical intervention is decisive in providing an optimum outcome and avoiding complications.
Conflict of Interest:
None
Acknowledgements:
We would like to acknowledge the contributions from the Department of Radiology, Government Medical College Kozhikode. Prof (Dr) Devarajan E, Professor & Head of the Department of Radiology and his entire team including the faculty and residents have been very helpful in the work-up of this patient.
References
1. Verma RR, Konkimalla A, Thakar A, Sikka K, Singh AC, Khanna T. Prevalence of hearing loss in India. Natl Med J India 2021; 34:216–22.
2. Garg S, Kohli C, Mangla V, Chadha S, Singh MM, Dahiya N. An Epidemiological Study on Burden of Hearing Loss and Its Associated Factors in Delhi, India. Ann Otol Rhinol Laryngol. 2018 Sep;127(9): 614-619
3. Miller, S.M., Mikulec, A.A. (2013). Congenital Conductive Hearing Loss. In: Kountakis, S.E. (eds) Encyclopedia of Otolaryngology, Head and Neck Surgery. Springer, Berlin, Heidelberg. 2013;539-543
4. Thomeer HG, Kunst HP, Cremers CW. Congenital stapes ankylosis associated with another ossicular chain anomaly: surgical results in 30 ears. Arch Otolaryngol Head Neck Surg. 2011 Sep;137 (9):935-41.
5. Briggs RJ, Luxford WM. Correction of conductive hearing loss in children. OtolaryngolClin North Am. 1994;27(3):607
6. Stewart JM, Downs MP. Congenital conductive hearing loss: the need for early identification and intervention. Pediatrics. 1993;91(2):355-359.
7. Esteves SDS, Silva AP, Coutinho MB, Abrunhosa JM, Sousa CA. Congenital defects of the middle ear – uncommon cause of pediatric hearing loss. Braz J Otorhinolaryngol. 2014;80:251-6.
8. Charachon R, Barthez M, Lavieille JP. Minor malformations of the ear ossicles: new classification and therapeutic results. Ann OtolaryngolChirCervicofac. 1994;111(2):69-74.
9. Teunissen EB, Cremers WR. Classification of congenital middle ear anomalies: report on 144 ears. Ann OtolRhinolLaryngol. 1993;102(8, pt 1): 606-612.
10. Zeifer B,Sabini P, Sanne J.Congenital absence of oval window:radiologic diagnosis and associated anomalies.AJNR Am J Neuroradiol. 2000;21(1):171-4
11. Sara E Henkemans , Adriana L Smit,Robert J Stokroos ,Hans GXM Thomeer. Congenital Anomalies of the Ossicular Chain: Surgical and Audiological Outcomes Ann Otol Rhinol Laryngol. 2021 Jun 11;131(4):388–396.
12. Kisilevsky V E, Bailie N A, Dutt S N, Halik J J. Hearing results of stapedotomy and malleovestibulopexy in congenital hearing loss. Int J Ped Otorhinolaryngol; 2009; Sep 30; p135-151.
13. Gargule S,Daval M,Arej N,Veyrat M,Corre A, Ayache D. Malleostapedotomy for otosclerosis, our experience of nitinol piston on twelve patients. J Otol.2020(5):129-132.