






Efficacy of Community-Based Cardiac Rehab in Older Adults
Efficacy of a Community-Based Phase III Cardiac Rehabilitation Program in Improving Function in Older Adults
Konrad J. Dias, PT, DPT, PhD¹*, Henry George Peterson, BS, SPT², Dan Nguyen, BS, SPT², Linda Paumer, MA³, Dustin R. Nadler, PhD⁴
- Professor of Physical Therapy, Department of Physical Therapy, College of Health and Human Services, California State University, Sacramento. 6000 J Street, Sacramento CA 95819 (USA).
- Graduate Student Doctor of Physical Therapy, Department of Physical Therapy, College of Health and Human Services, California State University, Sacramento. 6000 J Street, Sacramento CA 95819 (USA).
- Program Coordinator, Cardiovascular Wellness Program, California State University, Sacramento. 6000 J Street, Sacramento CA 95819 (USA).
- Associate Professor of Psychology and Associate Director, Center for Access and Achievement. Maryville University of St. Louis, 650 Maryville University Drive. St. Louis, MO 63021 (USA).
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Dias, KJ., Peterson, HG., et al., 2025. Efficacy of a Community-Based Phase III Cardiac Rehabilitation Program in Improving Function in Older Adults. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i10.7023
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i10.7023
ISSN 2375-1924
ABSTRACT
Purpose and Hypothesis: The purpose of this investigation was to analyze objective measures of endurance, balance, and strength following 4 and 12 weeks of participation in a combined volunteer and student run Phase III cardiovascular wellness program at a public university. It was hypothesized that improvements in objective tests of balance, strength, and endurance will be noted following completion of one month and three months of the program.
Methods: A prospective observational longitudinal design explored changes in function in 51 ambulatory patients attending a Phase III community-based cardiac rehabilitation clinic. Functional measures assessed including 3 minutes of stepping, 6-minute walk test, gait speed test, Timed Up and Go test, 30 second chair rise test, along with assessment of absolute and relative quadricep strength using a handheld dynamometer. Measurements were collected by two designated data collectors at enrollment into the study (data visit 1), after 4-weeks (data visit 2) and after 12-weeks (data visit 3). All subjects received routine Phase III cardiac rehabilitation that combined monitored aerobic exercise and strengthening exercises during the 12-week participation period. Subjects voluntarily participated in the program and attended on average 2 sessions per week.
Results: 33 females and 18 males with mean age 74 + 9 years, mean weight 76 + 14 kg. who were registered participants in the community clinic, participated in this study. A repeated measures ANOVA revealed statistically significant differences over the course of 12 weeks in 6-minute walk scores (F=10.98, p<0.01); absolute strength scores (F=4.07, p=0.02) and relative strength scores (F=3.15, p=0.04). Changes in 30 second chair rise scores neared significance (F=2.80, p=0.06). No statistically significant differences were noted from baseline to 12 weeks for gait speed, timed up and go test, and 3-minute step test scores. (p> 0.05)
Conclusion: With the growing number of patients in the community with heart disease, it is imperative to investigate new delivery models including the use of a community-based wellness program that may be effective in improving patient outcomes. This investigation reports meaningful improvements in 6-minute walk test and quadricep strength scores in individuals receiving Phase III cardiac rehabilitation within a community-based clinic. Standardized care was not provided during the course of the intervention. Future studies should examine the use of a standardized intervention to further validate the effectiveness of community-based programs in improving functional outcomes in older individuals with heart disease.
Keywords
Cardiac rehabilitation, community-based program, endurance, balance, strength, older adults
Introduction
An increased risk of chronic disease has been associated with aging, which overwhelmingly affects the independence, mobility, and quality of life of older adults. Cardiovascular disease (CVD) is ubiquitous in older adults and conditions related to CVD pose a substantial burden within society. In 2023, approximately 20.5 million deaths around the world were attributed to CVDs. The latest 2025 American Heart Association’s Heart Disease and Stroke Statistics report that between 2017 and 2020, 127.9 million adults in the United States had some form of CVD.
Cardiac rehabilitation is a multi-disciplinary program that focuses on improving physical function, and preventing secondary cardiac events, hospitalizations, and disability in individuals with established CVD. The benefits of formal cardiac rehabilitation conducted in a hospital setting are numerous and include reduced risk of death, heart attack recurrence, reduced hospital readmissions, along with improvements in physical strength, quality of life, mood, and medication adherence. Further, a compelling position paper indicates that secondary prevention through comprehensive and ongoing cardiac rehabilitation is one of the most cost-effective interventions to ensure favorable outcomes across a wide spectrum of cardiovascular disease.
Phase III cardiac rehabilitation, conducted in an outpatient setting, focuses on long-term maintenance of cardiovascular health through structured programming and encourages independent exercise and lifestyle management. The Agency for Healthcare Policy and Research (AHCPR) and the American Heart Association delineate current and explicit evidence on the importance of regular exercise and activity for primary and secondary prevention of CVD.
Despite an overwhelming body of evidence that support the benefits of cardiac rehabilitation, patient participation is unusually low. The American Heart Association indicates that improving participation rates in cardiac rehabilitation is a national priority. There are documented reasons for inequities in CR utilization including geographic inaccessibility to cardiac rehabilitation, physician bias in referral decisions, and lack of adequate education, funds and resources. Cost-prohibitive copayments or coinsurance prevent patients from seeking rehabilitation services beyond the subacute phase and into the chronic phases of their disease. Despite the emphasis that continued exercise training is required to sustain improved exercise tolerance, a large percentage of patients are not seeking out services to improve long physical activity. In a national analysis, participation in cardiac rehabilitation ranges only from 19% to 34% across the 50 states. Additionally, data shows that 41.5% of patients with known cardiac disease have subsequent cardiac events within a five-year follow-up. These statistics along with the known barriers in CR utilization, highlight the importance for promoting community-based CR that provides patients with opportunities to receive post-event cardiac care.
With these thoughts in mind, a Cardiovascular Wellness Program (CWP) developed at a Northern California public university was been developed to provide equitable and accessible care to patients who are interested in improving/maintaining health status following prior cardiac events. This interdisciplinary program run by volunteers and students strives to improve cardiac wellness in patients, and fulfills Phase III maintenance goals. As very few universities run community-based Phase III cardiac rehabilitation programs in the United States, there exists a paucity of research investigating the efficacy of such programs in improving patient’s physical function. Therefore, the purpose of this investigation was to explore the efficacy of a combined volunteer and student run program at a public university in improving objective measures of endurance, balance, and strength following 4 and 12 weeks of participation in a community-based Phase III cardiac rehabilitation program. It was hypothesized that improvements in objective tests of balance, strength, and endurance will be noted following completion of one month and three months of the program.
Methods
DESIGN
This study utilized a prospective observational longitudinal design. The study was conducted within the CWP. The CWP is as a community pro bono program housed within a northern California public university. Data collection for this study occurred from March 2024- October 2024.
PARTICIPANTS
Subjects were recruited in collaboration with enrolled patients that were participating in the CWP. Eligibility criteria included subjects that were currently enrolled in the CWP after receiving a formal referral or approval from their physician for participation in Phase III cardiac rehabilitation. In order to be recruited into the study, subjects were screened by a student physical therapist to ensure they were ambulatory and able to ambulate with or without the use of an assistive device with no more than contact guard assistance. In addition, subjects were assessed to assure they were able to follow basic commands and instructions. All subjects recruited into the study were over the age of 65. Individuals that were medically unstable with resting systolic blood pressure greater than 250 mm of Hg, or diastolic blood pressure greater than 115 mm Hg, or reported the need for a medical procedure were excluded from the study. All participants reviewed and signed an informed consent document approved by the Sacramento State University Institutional Review Board.
DATA COLLECTION
Data collection for each participant occurred at three distinct points. The three data collection visits for the outcome measures occurred at the onset of the study, at the end of week 4 and at the end of week 12. Two designated student physical therapists completed all data collection by assessing each participant’s functional outcome measurements on all three occasions during the course of the study.
This study involved collecting data on six outcomes that aimed at measuring changes in endurance, balance and strength. Participants completed two tests that evaluated changes in endurance including a six-minute walk test (6MWT) and a three-minute step test (3MST). Additionally, two tests of balance were conducted including an assessment of Gait Speed (GS), and a timed up and go test (TUG). Finally, strength was assessed by having the students complete a 30 second chair rise test (30CRT) and handheld dynamometry testing of bilateral quadriceps muscle. At each of the three visits, participants were randomly assigned an order to perform the six assessments. Participants were instructed to consecutively draw six folded slips of paper from a container. Each slip of paper delineated the name of the assessment. The order of slips picked up by the participant determined their unique order for completion of each of the six tests. A standardized rest interval of 5 minutes was provided between each assessment to allow the subject to rest and recover. The paragraphs below provides information on the procedures used to complete each of the six assessments used in this investigation.
Gait speed (GS) was assessed by having the subject walk for a distance of 14 meters. Time to complete the intermediate 10 meters was measured to obtain walking speed. Markers were placed at 2 meters and 12 meters from where the subject was initially seated. The first and last 2-meter distance was provided to allow for acceleration and deceleration. The data collector started timing when the toes of the leading foot crossed the first 2-meter mark. Timing was stopped when the toes of the leading foot crossed the 12-meter mark. Subjects were asked to ambulate with or without the use of their assistive device at the subject’s preferred walking speed. The data collector utilized a stop watch for measuring the time to complete the 10-meter distance. Gait speed was calculated and recorded in meters/ second.
For the Timed Up and Go Test (TUG), the participant began in a seated position in a standard chair with his/her back against the back of the chair. On the command “Go”, the subject was asked to rise from the chair, walk 3 meters at a comfortable and safe pace, turn, walk back to the chair and sit down. The data collector utilized a stop watch and began timing at the “Go” command and stopped timing when the patient was seated in their chair. The data collector was asked to ensure that the subject was provided with the same assistive device each time he/she was tested to be able to compare scores. The equipment required for this test included a standard height chair, a stop watch and a tape measure. The stop watch and tape measure were provided to the data collector in a data collection kit. The data recorded the total time to complete the timed up and go task.
The Six Minute Walk Test (6MWT) involved having the subject walk for 6 minutes. The total distance covered in 6 minutes was measured. The subject was allowed to use assistive devices when performing the test. The subject was instructed to walk at a safe and comfortable pace along a pre-measured distance of 100 feet that was free of obstacles. No verbal cues are provided during the test other than a notification of the number of minutes completed at the end of each minute. The following instructions were provided to the patient, “Cover as much ground as possible over 6 minutes. Walk continuously, if possible, but do not be concerned if you need to slow down or stop to rest. The goal of this test is to feel that no more ground can be covered at the end of 6 minutes.”
The Three Minute Step Test (3MST) involved stepping onto a 12-inch step for 3 minutes at a self-determined pace. The participant began by standing in front of a 12’’ step. A researcher demonstrated the stepping procedure. The four-step pattern for this test involved the subject stepping up onto the step with the right foot, followed by bringing the left foot up, subsequently lowering the body down by bringing the right foot down to the floor, and finally placing the left foot down to the floor. Completion of all four steps counted as one step. On the command “Go” the timer was started and the participant continued stepping for the three-minute duration. The participant was allowed to switch the leading leg if necessary and stop if needed. A clicker was used to count the number of steps completed during the 3-minute period.
The 30 Second Chair Rise Test (30 CRT) was utilized to assess the strength of the lower body. The subject was instructed to sit in the middle of a standard chair and place hands crossed over the chest. On hearing the command “Go,” the subject was asked to rise to a full stand position and then sit back down again. The subject was asked to repeat these sits to stand maneuvers for 30 seconds. The data collector placed the rear legs of the chair against a wall to ensure that the chair does not slide backwards. If the subject could not stand even once, then the subject scored a zero. The data collector stood in close proximity to the subject, ready to catch the participant should they lose balance. The participant was allowed to stop and rest if they become tired; however, the time continued until 30 seconds was completed. The data recorder recorded the total number of sit to stand transfers completed in 30 seconds. If a subject completed more than half the ascent at the 30 second mark, the data recorder recorded this last ascent as an additional sit to stand maneuver.
A handheld dynamometer was used to objectively measure the strength of the right and leg quadriceps muscle. For this test, the subject was asked to sit at the edge of a table with feet dangling off the table, and arms crossed across the chest. The researcher obtained the midpoint between the patella and the ankle and placed the dynamometer at this position. The subject was then asked to extend the knee and perform a maximal voluntary contraction for 3-5 seconds. A break test methodology was utilized by providing resistance and prevent motion. The maximum force obtained from the dynamometer was recorded. A total of three trials were performed for each leg and the average of the three trials was utilized to record the absolute strength of the quadriceps muscle of each leg. Subsequently relative strength values were also calculated by dividing the mean absolute strength of the quadriceps muscle of each leg by the body weight of the participant.
EXERCISE INTERVENTION
During the course of the 12 weeks subjects participated in their routine Phase III cardiac rehabilitation program. On average, the participants attended two sessions per week of in person cardiac rehabilitation. A log was maintained to document participant attendance. External activity and exercise conducted outside the CWP was not monitored during the course of the investigation. The exercise component of cardiac rehabilitation intervention included a variety of aerobic activities including treadmill walking, bicycling and use of the elliptical machine. Additionally, participants engaged in strengthening exercises using body weight and dumbbells. The intensity of the intervention was variable between subjects. In general subjects exercised at a moderate intensity. Each session lasted for approximately 45 minutes.
STATISTICAL ANALYSIS
Data was entered for storage into Microsoft Excel which was then imported into the statistical package Jamovi (Version 1. 2. 27). Descriptive statistics including mean, median, mode, and standard deviation were calculated for demographic variables including age, gender, height and weight. Additionally, descriptive statistics were calculated for all outcome measures at each of the three data collection point. A within-subjects repeated measures analysis of variance (ANOVA) test was used to assess main effects for each dependent variable. Significance was set at a p value of 0.05 for all statistical tests. A Bonferroni adjustment was utilized in the statistical analysis to determine where statistical differences existed between each of the three time periods.
Results
Data was analyzed consisted using a pool of 51 subjects that participated in this study. The demographic data for the 51 participants is shown in Table 1. The participant pool consisted of 18 males and 33 females. These were community dwelling older adults with a mean age of 74.12 ± 9.1 years. Participants recorded a body mass index in the overweight category with a mean weight of 76.16 ± 14.5 kilograms and a mean height of 1.65 ± 0.09 meters. Subjects recorded normal hemodynamic responses at rest with mean resting heart rate values of 74.43 + 11.1 beats per minute and mean blood pressure values 120/65 mm of Hg.
| Variable | Mean (SD) |
|---|---|
| Age (years) | 74.12 (9.1) |
| Height (meters) | 1.65 (0.09) |
| Weight (kilograms) | 76.16 (14.5) |
| Body Mass Index (kg/m2) | 27.8 (4.3) |
| Resting Heart Rate (beats/minute) | 74.43 (11.1) |
| Resting Systolic Blood Pressure (mm Hg) | 120.29 (13.8) |
| Resting Diastolic Blood Pressure (mm Hg) | 65.60 (11.84) |
| Gender | 33 Female, 18 Male |
Table 2 outlines mean and standard deviation, values for each outcome measure collected at baseline, after 4-weeks and 12 weeks for all participants. Additionally, the table reports the results of the within-subjects repeated measures ANOVA for each outcome variable. It is important to appreciate that all 51 subjects did not complete all 6 assessments at each of the 3 points in time. As indicated in the table, only 40 and 38 subjects completed assessments at the 4-week and 12-week period respectively.
| Test | Visit 1 Mean ± Std. Dev | Visit 2 Mean ± Std. Dev | Visit 3 Mean ± Std. Dev | F score; p value |
|---|---|---|---|---|
| Subjects(N) | 51 | 40 | 38 | |
| Gait Speed (meters/second) | 1.26 ± 0.25 | 1.33 ± 0.22 | 1.29 ± 0.19 | 1.28; 0.28 |
| Timed Up and Go (seconds) | 9.18 ± 2.17 | 8.41 ± 2.33 | 8.10 ± 1.12 | 2.23; 0.16 |
| Six Minute Walk Test (meters) | 411.7 ± 84.33 | 452.79 ± 80.27 | 461.83 ± 73.31 | 10.98; <0.01 |
| 3 Minute Step Test (steps) | 48.47 ± 13.46 | 54.23 ± 14.19 | 51.93 ± 12.42 | 1.88; 0.16 |
| 30 Second Chair Rise (chair rises) | 12.94 ± 4.14 | 14.20 ± 3.62 | 14.68 ± 3.99 | 2.80; 0.06 |
| Absolute Quad Strength (lbs.) | 39.63 ± 12.52 | 43.18 ± 14.18 | 43.89 ± 13.28 | 4.07; 0.02 |
| Relative Quad Strength (lbs/kg) | 0.53 ± 0.18 | 0.59 ± 0.20 | 0.59 ± 0.17 | 3.15; 0.04 |
RESULTS FOR GAIT SPEED: GS values collected at baseline, 4-weeks and 12-weeks were analyzed for differences using a within-subjects repeated measures ANOVA. The mean ± SD values for the GS at baseline, 4-weeks and 12-weeks were recorded as 1.26 ± 0.25, 1.33 ± 0.22, and 1.29 ± 0.19 meters per second respectively. The results of the within subjects repeated measures ANOVA revealed no statistically significant differences F(2,66)=1.28, p=0.285. As depicted in Figure 1, GS values did improve at the 4-week time period but not improve at the 12-week time period resulting in no statistically significant differences in GS from baseline to the 12-week period.

RESULTS FOR TIMED UP AND GO TEST: The mean ± SD scores for the TUG test recorded at baseline, after 4-weeks and after 12-weeks were 9.18 ± 2.17, 8.41 ± 2.33, and 8.10 ± 1.12 seconds respectively. The results of a within subjects repeated measures ANOVA comparing TUG scores at the three time periods revealed no statistically significant differences F(2,66)=2.23, p=0.16. As indicated in Figure 1, TUG values did improve more from baseline to the 4-week time point, and less from the 4-week to the 12-week period, resulting in no statistically significant differences in TUG scores from baseline to the 12-week period.
RESULTS FOR SIX MINUTE WALK TEST: As indicated in Table 2, mean ± SD scores for the 6MWT scores at baseline, after 4-weeks and after 12-weeks were 411.7 ± 84.33, 452.79 ± 80.27, and 461.83 ± 73.31 meters respectively. The results of a within subjects repeated measures ANOVA comparing 6MWT scores at the three time periods revealed statistically significant differences F(2,66)=10.98, p<0.01. Further, 6MWT scores progressively improved from baseline to the 4-week time point and from the 4-week to the 12-week period as shown in Figure 2. Results of the Bonferroni post hoc t-test analyses indicated statistically significant differences between baseline and the 4-week period as well as between the 4-week and 12-week time point. 6MWT scores measured at the 4-week period were significantly higher baseline 6MWT values t(33) = 2.75, p=0.02. Additionally, 6MWT scores at 12 weeks were significantly higher than scores measured at the 4-week period t(33) = 4.19, p<.001.

RESULTS FOR THREE MINUTE STEP TEST: The mean ± SD scores for the 3MST recorded at baseline, after 4-weeks and after 12-weeks were 48.47 ± 13.46, 54.23 ± 14.19, and 51.93 ± 12.42 steps respectively. The results of a within subjects repeated measures ANOVA comparing 3MST scores at the three time periods, revealed no statistically significant differences F(2,50)=1.88, p=0.16. As indicated in Figure 2, 3MST values did improve more from baseline to the 4-week time point, but decreased from the 4-week to the 12-week period, resulting in no statistically significant differences in 3MST scores from baseline to the 12-week period.
RESULTS FOR 30 SECOND CHAIR RISE TEST: The mean ± SD values for the 30CRT measured at baseline, 4-weeks and 12-weeks were 12.94 ± 4.14, 14.20 ± 3.62, and 14.68 ± 3.99 chair rises respectively. The values approached statistical significance F(2,66)=2.80, p=0.06. Additionally, as depicted in Figure 3, 30CRT scores progressively improved from baseline to the 4-week time point and from the 4-week to the 12-week period. These improvements were small and therefore did not reveal true statistical significance from baseline to the 12-week time point.
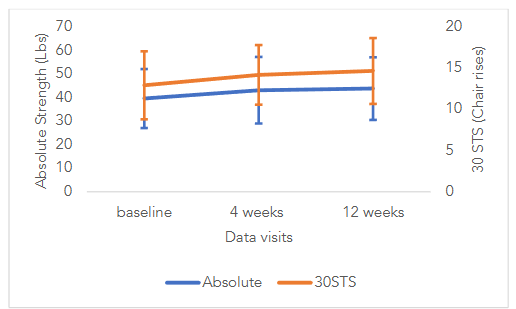
RESULTS FOR ABSOLUTE QUADRICEPS STRENGTH: Data was recorded for 3 trials of maximum voluntary contraction for the quadriceps muscle on the right leg and left leg. There were no statistical differences between strength values on the right leg compared to the left leg for each of the three trials, measured at baseline, after 4-weeks and 12-weeks of the program. Since no statistical differences were found between right and left quadriceps strength, strength scores on the right leg were used for the analysis. The mean ± SD values for handheld dynamometry of the right quadriceps muscle measured at baseline, 4-weeks and 12-weeks were 39.63 ± 12.52, 43.18 ± 14.18, and 43.89 ± 13.28 lbs. respectively. The results of a within subjects repeated measures ANOVA comparing absolute quadriceps strength scores at the three time periods revealed statistically significant differences F(2,64)=4.07, p=0.02. Additionally, as depicted in Figure 3, absolute quadriceps strength scores progressively improved from baseline to the 4-week time point and from the 4-week to the 12-week period. Results of the Bonferroni post hoc t-test analyses indicated no statistically significant differences between baseline and the 4-week period t(32) = 1.47, p=0.46., but statistically significant differences from baseline to the 12-week time point t(32) = 2.66, p=0.03.
RESULTS FOR RELATIVE QUADRICEPS STRENGTH: Relative strength was calculated by dividing the absolute strength by the participants body weight. The mean ± SD values for relative strength of the right quadriceps muscle measured at baseline, 4-weeks and 12-weeks were 0.53 ± 0.18, 0.59 ± 0.20, and 0.59 ± 0.17 lbs/kg body weight respectively. The results of a within subjects repeated measures ANOVA comparing relative quadriceps strength scores at the three time periods revealed statistically significant differences F(2,64)=3.15, p=0.04. Results of the Bonferroni post hoc t-test analyses indicated no statistically significant differences between baseline and the 4-week period t(32) = 1.38, p=0.53., but statistically significant differences from baseline to the 12-week time point t(32) = 2.4, p=0.05.
Discussion
The overall objective of this study was to compare the efficacy of a university run community-based Phase III cardiac rehabilitation in improving objective measures of endurance, strength and balance. Within the context of this investigation, community participants who were part of CWP volunteered to participate and have their endurance, strength and balance assessed at baseline, after 4-week and 12-weeks of participation in the program. The CWP offered participants monitored exercise on various modes including the treadmill, stationary bike and elliptical machine. Additionally, group exercise classes focused on strength training. Volunteers and students assisted patients in their exercise plans at each session. On average, participants attended 2 sessions per week during the course of this investigation.
There exists a dearth of evidence on the role of community-based Phase III CR programs in improving exercise and function. Although much research has looked at improvements with exercise training after acute heart disease, no research to date has specifically investigated improvements in endurance, balance and strength achieved during the maintenance phase of cardiac rehabilitation. Most of the available evidence focuses on patients who receive exercise interventions in the early stages following their cardiac event. However, individuals living in the community years after their acute event are also unique as they may not have the knowledge or resources to avail of community-based programs to help reduce their risk of cardiovascular mortality, morbidity, disability, and increase their quality of life. For this reason, this study provides meaningful evidence on improvements in function that can be achieved through participation in a community-based wellness program.
As the science related to cardiac rehabilitation has progressed over the years, the 2024 cardiac rehabilitation scientific statement from the American Heart Association advocates for the use of community resources to promote wellness and cardiovascular health. However, this paper does not specifically address the efficacy of community-based programs. The findings of this investigation report improvements in function that can be noted at 4-weeks and 12-weeks following participation in a community-based wellness program. For all outcome measures, participants revealed improvements in all outcomes from baseline to the end of the study. In addition, change scores were found to be higher in the first four weeks of participation in program. Although improvements were not observed in all outcome measures in the last 8 weeks, all subjects were able to maintain scores at or above baseline values. As noted in prior research, regular participation in aerobic and strength training is important in maintaining muscle mass and function with age.
MEANINGFUL IMPROVEMENTS IN FUNCTION
Steffen et al. report normative data on the 6MWT for community dwelling older adults. These investigators report septuagenarian men and women to have 6-minute walk distances of 527metres and 471 meters respectively. The mean age of participants in our investigation was 74 years of age and recorded a baseline mean 6-minute walk distance of 412 meters. This indicates that the sample in this study potentially presented with an endurance impairment with 6MWT values below normative data. In regards to meaningful change in 6WMT scores, Perera et al report a change of 50 meters as the minimally clinically important difference in older adults. In looking at our results, participants increased 6MWT scores by 50 meters over the 12-week period from 411 meters at baseline to 461 meters at the end of the intervention.
Our study utilized two outcomes to measure patients balance and fall risk. These two outcomes included the TUG test and the GS test. Shumway-Cook et al. report TUG scores greater than 13.5 seconds to indicate increased risk of falls in community dwelling older adults. Further, Montero-Odasso et al. indicate GS scores of less than 0.70 meters/second as a cut off score that increases an older adult’s risk for falls and adverse events. In this investigation, TUG tests at baseline were under 10 seconds, and GS scores were at 1.26 meters/second. These values depict that the sample of participants in this investigation did not have an underlying balance and fall risk impairment. Participants in this study were active in the community, driving and attending community events. As bassline TUG and GS scores were better than reported normative data, no statistically significant improvements were noted in TUG through participation in the CWP. However, the continued involvement within the exercise program allowed participants to maintain TUG and GS scores, and not worsen their balance and fall risk.
Improvements in lower extremity strength were captured through 30CRT and strength testing of the quadriceps muscle using a handheld dynamometer. Rikli and Jones present data on criterion fitness standards needed to maintain physical independence. These researchers report 13 and 15 chair rises in 30 seconds to be scores that facilitate physical independence in community dwelling septuagenarians. The results of our investigation report similar values over the 12-week period. The mean 30CRT score at baseline was recorded as 12.9 sit to stand maneuvers. This value increased to a mean value of 14.68 chair rises after 12 weeks. Additionally, the findings from our investigation report statistically significant improvements in absolute and relative strength over the 12-week period. These findings collectively suggest that participation in the CWP was efficacious in improving strength in community dwelling older adults with cardiac disease.
STRENGTHS AND LIMITATIONS
The study included a number of features to improve internal validity and minimize bias. The investigation followed a prospective design and a pragmatic approach in observing improvements in function without a formalized exercise plan. In addition, the procedures of the study utilized randomization of tests and two designated data collectors to conduct all assessments. The use of only two individuals for all data collection increased the reliability of scores obtained on each dependent variable.
There were several limitations of this study. Firstly, the use of a single-center threatens the external validity and the ability to generalize the findings over various settings. Secondly, the study did not call for a formal plan of activities and progressive exercises to include at each visit. It would be ideal if the study utilized a standardized plan of treatment interventions that was progressively increased over the course of 12-weeks. Thirdly, the study did not call for a methodology to log treatment activities and exercises that were completed outside the CWP.
RECOMMENDATIONS FOR FUTURE RESEARCH
An important suggestion for future research would be to utilize a formalized plan of activities and interventions along with a formalized progression of exercise during the course of the trial. A major limitation of the current investigation was its failure to control for the type and progression of intervention provided to participants during the 12-week period. Additionally, it may be useful for future research to include an economic analysis to assess the cost-effectiveness of a community-based cardiac rehabilitation program. An analysis of cost-effectiveness will be important to help institutions and organizations understand the economic value their program offers to the community.
Conclusion
Maintaining or increasing exercise capacity and function in community dwelling older adults with cardiac disease is a subject of substantial interest. With the growing number of patients in the community with heart disease, it is imperative to investigate new delivery models including the use of a community-based wellness program that may be effective in improving patient outcomes. Currently, little is known about the efficacy of a university-based community wellness program in improving patient’s physical function. This is the first study to report meaningful improvements in function in individuals who participated in a 12-week Phase III cardiac wellness program. Significant treatment effect differences were found for the 6MWT and strength scores. Standardized care was not provided during the course of the intervention. Future studies should examine the use of a standardized intervention to further validate the effectiveness of community-based programs in improving functional outcomes in older individuals with heart disease.
Conflict of Interest Statement:
None declared.
Funding Statement:
None.
Acknowledgements:
None.
References:
- Maresova P, Javanmardi E, Barakovic S, et al. Consequences of chronic diseases and other limitations associated with old age – A scoping review. BMC Public Health. 2019;19(1). doi:10.1186/S12889-019-7762-5
- Martin SS, Aday AW, Allen NB, et al. 2025 Heart Disease and Stroke Statistics: A Report of US and Global Data from the American Heart Association. Circulation. 2025;151(8):e41-e660. doi:10.1161/CIR.0000000000001303/SUPPL_FILE/SUB-SAHARAN
- Beatty AL, Beckie TM, Dodson J, et al. A New Era in Cardiac Rehabilitation Delivery: Research Gaps, Questions, Strategies, and Priorities. Circulation. 2023;147(3):254-266. doi:10.1161/CIRCULATIONAHA.122.061046/ASSET/5439B984-B96D-4553-B4E6-F27670B9BD6E/ASSETS/GRAPHIC/CIRCULATIONAHA.122.061046.FIG02.JPG
- Taylor RS, Walker S, Ciani O, et al. Exercise-based cardiac rehabilitation for chronic heart failure: The EXTRAMATCH II individual participant data meta-analysis. Health Technol Assess (Rockv). 2019;23(25):1-97. doi:10.3310/HTA23250
- Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: A systematic review and meta-analysis of randomized controlled trials. Am Heart J. 2011;162(4). doi:10.1016/J.AHJ.2011.07.017
- Oldridge N, Pakosh M, Grace SL. A systematic review of recent cardiac rehabilitation meta-analyses in patients with coronary heart disease or heart failure. Taylor & Francis. 2019;15(3):227-250. doi:10.2217/FCA-2018-0085
- Goel K, Pack QR, Lahr B, et al. Cardiac rehabilitation is associated with reduced long-term mortality in patients undergoing combined heart valve and CABG surgery. European Journal of Preventive Cardiology. 2015;22(2):159-168. doi:10.1177/2047487313512219
- Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2021;28(5):460-495. doi:10.1177/2047487320913379
- Thompson PD, Buchner D, Piña IL, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A statement from the council on clinical cardiology (subcommittee on exercise, rehabilitation, and prevention) and the council on nutrition, physical activity, and metabolism (subcommittee on physical activity). Circulation. 2003;107(24):3109-3116. doi:10.1161/01.CIR.0000075572.40158.77
- Brown TM, Pack QR, Aberegg E, et al. Core Components of Cardiac Rehabilitation Programs: 2024 Update: A Scientific Statement from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2024;150(18):e328-e347. doi:10.1161/CIR.0000000000001289/SUPPL_FILE/BROWN_SUPPLEMENTAL_MATERIAL.PDF
- Ritchey MD, Maresh S, McNeely J, et al. Tracking cardiac rehabilitation participation and completion among Medicare beneficiaries to inform the efforts of a national initiative. Circ Cardiovasc Qual Outcomes. Published online 2020. doi:10.1161/CIRCOUTCOMES.119.005902
- Patel RS, Tragante V, Schmidt AF, et al. Subsequent Event Risk in Individuals With Established Coronary Heart Disease. Circ Genom Precis Med. 2019;12(4):e002470. doi:10.1161/CIRCGEN.119.002470
- Salzwedel A, Jensen K, Rauch B, et al. Effectiveness of comprehensive cardiac rehabilitation in coronary artery disease patients treated according to contemporary evidence based medicine: Update of the. European Journal of Preventive Cardiology. 2020;27(16):1756-1774. doi:10.1177/2047487320905719
- Abraham LN, Sibilitz KL, Berg SK, et al. Exercise-based cardiac rehabilitation for adults after heart valve surgery. Cochrane Database of Systematic Reviews. 2021;2021(5). doi:10.1002/14651858.CD010876.PUB3/FULL/ID
- Fuertes-Kenneally L, Blasco-Peris C, Casanova-Lizón A, et al. Effects of high-intensity interval training on vascular function in patients with cardiovascular disease: a systematic review and meta-analysis. Front Physiol. 2023;14. doi:10.3389/FPHYS.2023.1196665
- O’Connor CM, Whellan DJ, Lee KL, et al. Efficacy and Safety of Exercise Training in Patients With Chronic Heart Failure: HF-ACTION Randomized Controlled Trial. JAMA : the journal of the American Medical Association. 2009;301(14):1439. doi:10.1001/JAMA.2009.454
- Dibben G, Faulkner J, Oldridge N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database of Systematic Reviews. 2021;2021(11). doi:10.1002/14651858.CD001800.PUB4/MEDIA/CDSR/CD001800/IMAGE_T/TCD001800-CMP-001.10.PNG
- Laurin JL, Reid JJ, Lawrence MM, Miller BF. Long-term aerobic exercise preserves muscle mass and function with age. Curr Opin Physiol. 2019;10:70-74. doi:10.1016/J.COPHYS.2019.04.019
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys Ther. 2000;80(9):896-903. doi:10.1093/PTJ/80.9.896
- Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743-749. doi:10.1111/J.1532-5415.2006.00701.X
- Montero-Odasso M, Schapira M, Soriano ER, et al. Gait velocity as a single predictor of adverse events in healthy seniors aged 75 years and older. Journals of Gerontology – Series A Biological Sciences and Medical Sciences. 2005;60(10):1304-1309. doi:10.1093/GERONA/60.10.1304
- Rikli RE, Jones CJ. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist. 2013;53(2):255-267. doi:10.1093/GERONT/GNS071