






Comparative Study of Needles in Auriculotherapy for Pain
Comparative retrospective analysis of auriculotherapy with mechanical needles and cryogenic needles for pain treatment
David Alimi 1,2 Sarah Dauchy 2, Isabelle Nègre 3, Christophe Gueguen 4
- Department of Anesthesiology, University of Pittsburgh, Pittsburgh, PA.
- Institut Gustave Roussy, DISSPO, Department of Psycho-oncology, Villejuif, France.
- Kremlin Bicêtre Hospital, Villejuif, France. Evaluation and Pain treatment.
- Medical Practice, 176 Rue De Lille, 62400 Bethune, France.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Alimi, D., Dauchy, S., et al., 2024. Comparative retrospective analysis of auriculotherapy with mechanical needles and cryogenic needles for pain treatment. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.6081
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.6081
ISSN 2375-1924
ABSTRACT
To compare the effects of so-called semi-permanent needles and cryogenic needles in auriculotherapy performed at a hospital or independently. We analyzed the auriculotherapy consultation records of Gustave Roussy and Kremlin Bicêtre hospitals, and of the medical practices of Drs. D. Alimi and C. Gueguen, from November 2010 to February 2012. Results on pain intensity were compared according to whether patients had received auriculotherapy with semi-permanent needles or cryogenic needles, in different pathologies.
A total of 2,147 patient records were analyzed, of which 90% suffered from chronic pain and 10% from acute pain. 79% of patients had been treated in the practices of Drs. D. Alimi and C. Gueguen, and 21% in Gustave Roussy and Kremlin Bicêtre hospitals (with participation of Dr. D. Alimi). 1,355 patients were familiar with auriculotherapy, of which 652 were treated with semi-permanent needles and 703 with cryogenic needles. 792 patients were not familiar with AT and were treated with cryogenic needles. In those already familiar with auriculotherapy, 75% of patients treated with semi-permanent needles were relieved of their pain compared to 80% of those treated with cryogenic needles; while among patients not familiar with auriculotherapy, 72% of those treated with semi-permanent needles and 79% of those treated with cryogenic needles were relieved of their pain.
Positive results were obtained with both semi-permanent and cryogenic needles, with slight superiority for the latter, knowing that these results were not from a randomized controlled trial.
Keywords
auriculotherapy, semi-permanent needles, cryogenic needles, pain treatment, retrospective analysis
Introduction
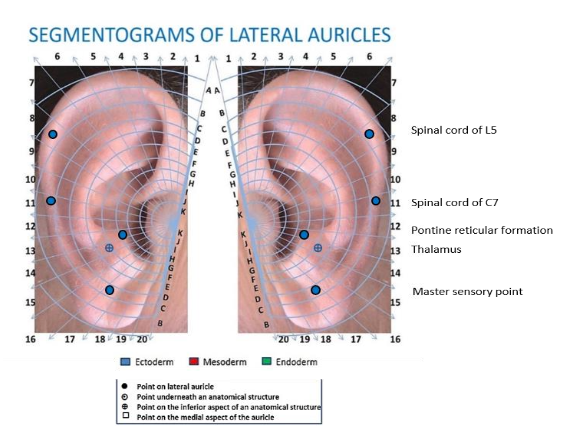
Auricular acupuncture or auriculotherapy is a therapeutic technique for treating sick people, in many indications, using certain points of the ear, which have precise electrical and electrochemical properties. It works by exploiting the embryogenetic laws underlying the formation of the ear pavilions and the neurophysiological laws regulating information management.
The auriculotherapy zones (or points) are a characterization of the focal connective tissue containing “nodes”, made of vascular, nervous and more or less cellular elements, intercalated on the “ordinary” path of the skin structure with a diameter of approximately 2 to 3 mm, creating “neurovascular complexes” (NVC). The latter have electrical properties, combining thyristor and diode effects, allowing the activation of the central, peripheral, enteric and autonomic nervous systems.
The technique consists of soliciting these points in order to induce a central and peripheral neurophysiological homeostatic rebalancing, tending to return to the last known good configuration, respecting Otto Kahler’s law. These actions induce a temporary and reversible invalidation of the auricular somatotopic representation zones, in reciprocal echo with the cerebral somatotopic maps.
There are 2 types of needles commonly used in auricular acupuncture (auriculotherapy): either extemporaneous needles (EN) for single use, inserted in the auricles at the levels of the presumed therapeutic sites; or so-called “semi-permanent” needles (SPN), also for single use, inserted at the same sites and which fall out by themselves after a few days, after the end of their therapeutic action.

At the Pain Center of the Gustave Roussy Cancer Institute, we provided auriculotherapy consultations. We very frequently had complaints from cancer specialists who were bothered by the presence of semi-permanent needles, which we had stuck into our patients’ ears, to effectively relieve their pain. These needles often represented various inconveniences during the necessary care of patients (surgery, radiotherapy, chemotherapy). Because these needles may have a number of disadvantages (accidental contact, consequent discomfort for certain professions, diabetics, patients on anticoagulants, immune-compromised patients, hearing aid wearers, etc.). About ten years ago, we decided to try to find new therapeutic tools to continue to relieve these patients through auriculotherapy.
During an experiment studying the action of liquid nitrogen cryosprays on the auricular skin, it became clear to us that these could have a temporary invalidation effect on the auriculotherapy zones. Thermoreceptors are distributed throughout the skin with different densities. The skin of the face, including the ears, has the highest density of cold receptors: 16 to 20/cm2 compared to 1.5/cm2 for hot receptors. Each mm2 of epidermis contains approximately 60 to 70 nerve endings, including 1 thermosensitive fiber and 59 polymodal sensitivity fibers.
The rapid injection of a cold source into healthy or pathological skin, generally liquid nitrogen, creates a real thermal shock (by succession of vasoconstriction and vasodilation: Hunting reaction or Lewis reaction), which causes a crystallization of intracellular water, affecting the membrane and cellular structures; temporarily invalidating, during the reconstruction, the functions supported by the affected cells.
The coldest areas of the head studied in the cold laboratory, at 0 degrees Celsius, appear clearly at the ears, nose and chin. This is how we imagined and discovered CryoAuriculoTherapy (CAT).
The SPN may have a number of disadvantages (accidental contact, consequent discomfort for certain professions, diabetics, patients on anticoagulants, immune-compromised patients, hearing aid wearers, etc.). To overcome these disadvantages, in 2011, Alimi D. developed so-called “cryogenic” needles (CN) by adapting the “CryoAlfa” system to auriculotherapy, which has already been used in dermatology, gynecology, stomatology, vascular pathology and anesthesiology. This liquid nitrogen spray injected at the auricular point(s) to be treated temporarily numbs the therapeutic zone, as does the semi-permanent needle; without leading to scarring or sclerogenic lesions, by freezing, in a few seconds the point in depth, over 2 to 3 mm, respecting the constitutional proteins (collagen fibers, cartilages), without any limitation of age, repetition of the sessions or without any constraint. These cryogenic needles allow a risk-free, non-bloody, odorless, colorless, almost painless auriculotherapy. They eliminate all the disadvantages of the mechanical needles and their constraints, while maintaining their effectiveness.

Recently, in terms of economic management of hospitals and private healthcare costs, financial decision-makers have been asked to reduce hospital costs in terms of healthcare equipment costs. The effectiveness of semi-permanent needles has been studied, but to our knowledge, no studies have been done to compare the action of semi-permanent needles and cryogenic needles. We therefore decided to carry out a retrospective observational analysis of patient records, having been treated for pain of different etiologies. We randomly selected a 10-year period (September 2010 to June 2022), in which we randomly selected a sufficiently broad analysis period (November 2010 to February 2012).
Methods
STUDY DESIGN
We selected, regardless of age and sex, in each painful pathology, patients who had been treated with ASP needles and those who had been treated with cryogenic needles; the latter having a lower financial cost than semi-permanent needles. We did a retrospective analysis of 2,147 files of patients treated for pain, either with SPN or with CN. Recruitment was done in 4 pain consultations, in 2 hospitals and 2 medical practices. 14% of patients were part of the auriculotherapy consultation at Gustave Roussy hospital, 7% were at the Bicêtre hospital, and 79% were monitored at the practices of Drs. David Alimi and Christophe Gueguen.
SETTING
All the patients were treated using localization of area zones of the International Nomenclature of Auriculotherapy, as agreed upon by the World Federation of Chinese Medicine Societies. To treat patients’ pain, the same auricular therapeutic strategies have been performed, both with SPN and with CN.
PARTICIPANTS
The eligibility criteria were the patients who came to consult the pain centers of the above-mentioned centers, and who had completed an evaluation of their pain on a visual analogue scale, graduated from 0 to 10.
VARIABLES
Patient follow-up was performed monthly by an algologist, and the results were recorded in the files of each patient. The eligibility criteria were the patients, regardless of gender, regardless of age, who came to consult the pain centers of the above-mentioned centers, and who had completed an evaluation of their pain on a visual analogue scale, graduated from 0 to 10. Compared to the initial value of the EVA estimated by each patient: very good results were considered to be decreases in the VAS pain score of 5 points, good results were considered to be decreases of 4 points, satisfactory results were considered to be decreases of 3 points, insufficient results were considered to be decreases of 2 points, null results were considered to be no change, results with worsening, any increase in the VAS pain score were considered to be.
DATA SOURCES MEASUREMENT
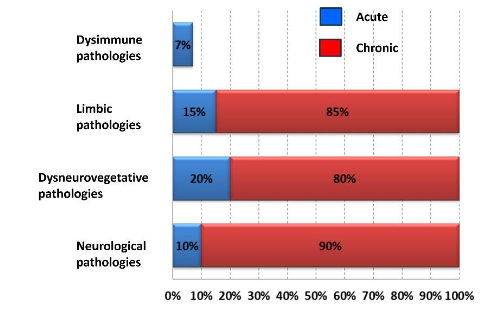
The selected files were those who had come consult as part of their analgesic follow-up. All types of pain were retained, which was important to us, was to compare the effects on the intensity of the pain, either ASP or CN. Regarding the etiologies generating pain, 7% concerned acute pain caused by dysimmune pathologies, limbic pathologies had caused 15% of acute pain and 85% of chronic pain, dyneurovegetative pathologies had caused 20% of acute pain and 80% of chronic pain, and finally neurological pathologies had caused 10% of acute pain and 90% of chronic pain.
BIAS
We keep only the complete files of the patients who came regularly to consult and did not change their treatment during the entire period considered. Records mentioning the occurrence of an interfering pathology have been eliminated. Only complete and correctly completed files were retained, patients lost to follow-up were removed from the analysis, and a check of the last VAS was performed by the host nurse.
STUDY SIZE
Having considered all the factors of inclusion and exclusion mentioned above, we were able to consider 2147 files of patients treated for pain out of 2200, in the period stretching from November 2010 to February 2012.
QUANTITATIVE VARIABLES
The VAS survey and analysis was assigned to each center participating in this retrospective analysis, to the same consultation and treatment team.
STATISTICAL METHODS
The results were assessed by measuring the estimated intensity of the improvement of pain treated, on a VAS, at levels 0 D, 30 D, 60 D and 90 D, by averaging the arrhythmic weekly VAS. Patients were classified according to the pathologies generating their pain and between those who knew auriculotherapy or not, those who had already been treated with SPN or not, and finally those who had already been treated with CN or not. Assessment charts have been developed to measure potential variations in pain intensity EVA in these different groups.
Results
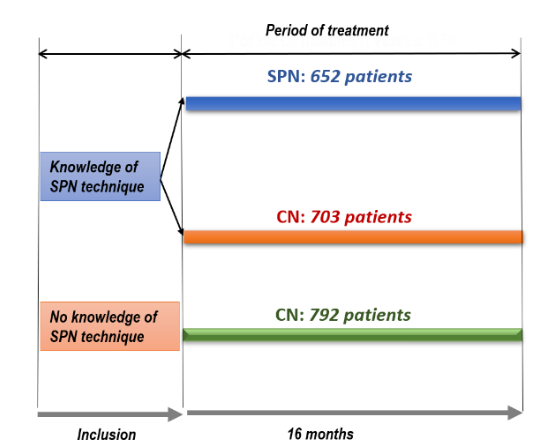
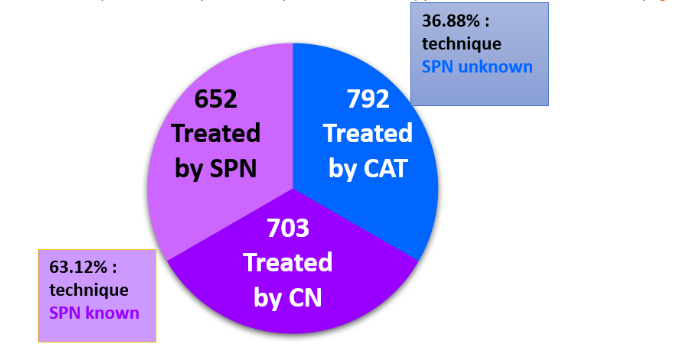
We were able to consider 2147 files of patients treated for pain out of 2200, in the period stretching from November 2010 to February 2012. 90% of the pain was chronic in nature and 10% acute in nature. Among 1,355 patients, 3 more or less equal groups of patients were identified: the first group (652 patients) benefited from SPN treatments and was already familiar with auriculotherapy using SPN; the second group (703 patients) benefited from CN treatments and was also familiar with the auricular therapeutic technique using SPN. The third group (792 patients) benefited from CN treatments and was not familiar with the auricular therapeutic technique, and thus were considered naive patients.
Among all the patients: 63.12 % was familiar with the therapeutic technique using SPN, and 36.88% had not.
Patients who were already familiar with auriculotherapy with SPN were given the choice to either continue being treated with SPN (only 1% made this choice), or to be treated with the new therapeutic tool consisting of the CN. The other patients benefited from auriculotherapy with cryogenic needles. No side effects were noted in both SPN and CN patients.
By adding up the very good, good, and satisfying results, the scores show: respectively, for patients treated with SPN and those treated with CN: 75% and 80% were positive responses. Among the patients who had never been treated with auriculotherapy: the scores show, respectively, for the patients treated with SPN and those treated with CN: 72% and 79% were positive responses.
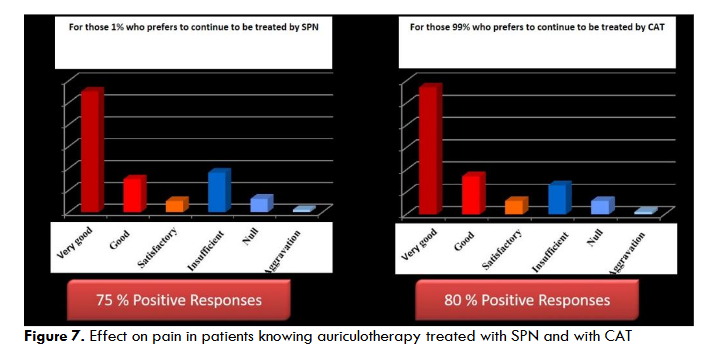
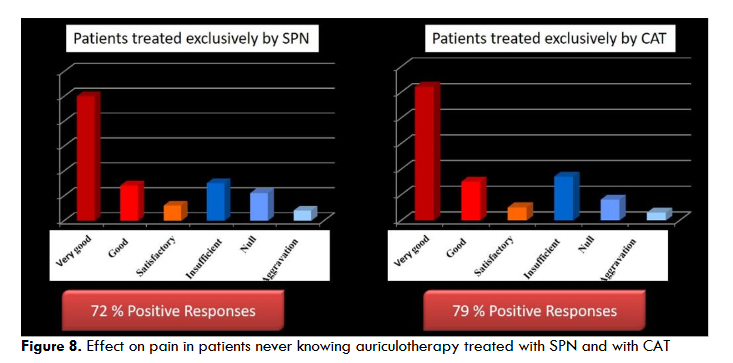
Therapeutic gain is noted when CNs were used; both for patients who have already been treated with SPN (+ 7%) and for patients who were not familiar with auriculotherapy, who have never been treated with SPN (+ 5%). The average percentage of positive therapeutic responses, when CNs were used, finally amounts to + 6% in painful conditions treated.
Discussion
This retrospective analysis performed on a sample of 2147 patients from auriculotherapy consultations in 2 hospitals and 2 medical practices, compared the results on pain intensity, after auriculotherapy by Semi Permanent Needles or by Cryogenic Needles; would have been more meaningful if it could have been performed as a double-blind against placebo for both types of auriculotherapy. But it’s a retrospective analysis and in the painful pathologies studied, the patients concluded to an equal therapeutic effectiveness during the use of the SPN as well as the CNs. We could have conducted a double-blind study comparing the effectiveness against pain of the use of SPN and CN in auriculotherapy, but our Institute needed a quick response to make its health-saving decisions. It is not excluded that we could form the project of conducting this type of study later?
Conclusion
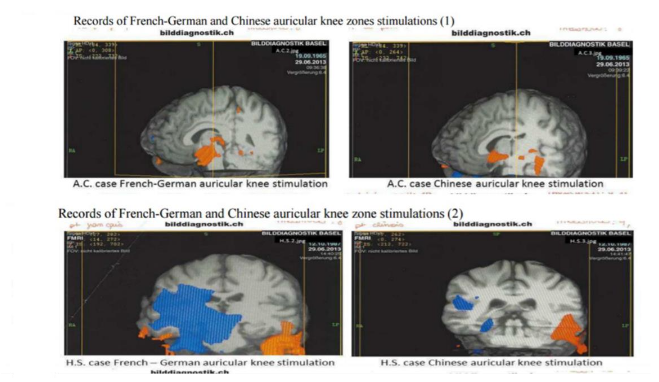
This finding leads to a relative estimate of the effectiveness of the two types of needles. In addition, the demonstration of the action of CNs using fMRI, in the same way as the SPN puts the possible placebo action of these 2 auricular therapeutic tools at the same level. This retrospective analysis gained credibility if it could have been conducted from the outset in intention to treat and double-blind against double placebo. But the positive results in both cases make it possible to affirm the effectiveness of auriculotherapy, and allows to give the patients the free choice of the tool to treat them.
Conflicts of Interest Statement
No competing interests.
Funding Statement
This retrospective analysis received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements
The authors would like to thank all the staff who were involved in data collection, intervention implementation, data management, and data analysis. The authors especially thank Debborah Guez and Sylvie Emmanuel.
References
- Rabischong P. Med Acupunct. 26(2):84-96. doi:101089/acu.2014.1038.
- Larsen WJ. Human embryology. De Boeck; 2011.
- Hockfield S, Kalb RG. Activity-dependent structural changes during neuronal development. Curr Opin Neurobiol. 1993;3(1):87-92.
- Onteniente B, Peschanski M, Prochiantz A, Ollat H. Functional neuroanatomy. Volume 3: development and plasticity. ANPP; 1996.
- Auziech O. Acupuncture et auriculothérapie. Essai d’analyse histologique de quelques structures cutanées impliquées dans ces deux techniques. Sauramps; 1984
- Terral C. Douleur et acupuncture. De la recherche à la Clinique. Sauramps Medical; 2009.
- Bossy J. Bases neurobiologiques des réflexothérapies. 3e éd. Masson; 1983.
- Vnitr L. Pavel Cech. 2019;65 (5):379-389. PMID: 31163973.
- Alimi D, Gessmann A, Gardeur D. Auricular acupuncture stimulation measured on functional magnetic resonance imaging. Med Acup. 2002;13:18-21.
- Liboni W, Romoli M, Allais G, et al. The fMRI for the auricular acupuncture validation: Experimental protocol [presentation; in Italian]. Acti XXII Congresso Nationale Soc Ital Rifles Ago Auri (SIRAA). 2007;November16–17
- Okorie EC, Santosa H, Alter BJ, Chelly JE, et al. Ipsilateral stimulation shows somatotopy of thumb and shoulder auricular points on the left primary somatosensory cortex using high-density fNIRS. bioRxiv [Preprint]. 2024 Sep 16:2024.09.16.612477. doi:10.1101/2024.09.16.612477.PMID: 3934559
- Eric Kandel, John D. Koester, Sarah H. Mack, Steven Siegelbaum. Principles of Neural Science. April 2021.
- Carter R. The Brain Book. Human Body Guides. Dorling Kindersley Ltd; 2019
- David E, Presti W, et al. Foundational Concepts in Neuroscience: A Brain-Mind Odyssey. January 2016.
- Steegmann Jr. AT. Human facial temperatures in natural and laboratory cold. 1979; 50(3):227-32 PMID: 45432.
- Sliosberg A. Cryopuncture in current medical practice. Press Med. 1952.20.60(81:1730
- Vanggard L. Physiological reactions to wet-cold. Aviation, Space and Environmental Medicine. 1975;January33-36
- Zeveke AV, Efes ED, Malysheva GI et al. Analysis of activity in A and C fibers under mechanical and thermal stimulation in the skin receptor field. Program Brain research. 1976;43:151-157
- Evans PJD. Cryoanalgesia: the application of low temperature to nerves to produce anesthesia or analgesia. Anesthesia. 1981;36:1003-1013
- Lecroart Jl, Deklunder G, Houdas Y. Dynamique de refroidissement sous cryothérapie par azote liquid vaporisé et par glace. Laboratoire de physiologie de la faculté de médecine de Lille. 1990; rapport JETCOOL
- Alimi D , Rubino F, Lewandowski EP et al. Analgesic Effect of Auricular Acupuncture for Cancer Pain. Journal of Pain and Symptom Management. 2000;19:81-82
- Alimi D. Xerostomia induced by radiotherapy. Therapeutics and Clinical Risk Management. Dovepress. 2015;11:1-4
- Alimi D, Chelly J.E. Auriculotherapy in anesthesia and pain treatment. Praticien en Anesthesie Reanimation. 2016;20,2,1:97–100
- Nomenclature Normative Internationale. ISBN: 978-2-220-06330-0. Desclée de Brouwer Edition: Sept. 2011;372-375.
- Alimi D, Chelly J.E. New Universal Nomenclature in Auriculotherapy. J Altern Complement Med. 2018;24:7-14.