






Perioperative Medication Management for Surgical Patients
Practice Recommendations in the Perioperative Chronic Medication Management in the Surgical Patient
García-Miguel FJ, MD, PhD, DESA1; Valencia Castillo, SL, MD, PhD2
- Anaesthesia and Reanimation Chief of Department, Complejo Hospitalario Segovia, Spain.
- Specialist Haematologist, Complejo Hospitalario Segovia, Spain.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: García-Miguel, FJ., and Valencia Castillo, SL., 2024. TITLEHERE. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.6070
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI ps://doi.org/10.18103/mra.v12i11.6070
ISSN 237 5-1924
ABSTRACT
At least 50 percent of patients undergoing surgery take medications on a regular basis. Anesthesiologists in the preoperative assessment of the surgical patient often must decide if chronic medications should be continued in the perioperative period. Unfortunately, there are few outcome data about the majority of medications taken in the perioperative period. The evidenced-based medical literature shows great variability in the attitude taken by different centers regarding the patient`s taking of chronic preoperative medication. This lack of medical evidence is reflected by the large variation in perioperative management recommendations. This topic will focus on medications known to have perioperative effects, those known to interact with anesthetic agents, and those in common use. The present article aims to provide an evidenced-based review of perioperative chronic medication management. Emphasis is placed on the importance of specific recommendations for medication management by different categories of therapeutic agents: cardiovascular, gastrointestinal, pulmonary and endocrine agents. Medications affecting kidney function, psychotropic agents, chronic opioid therapy, rheumatologic and neurologic agents, medications for benign prostatic hypertrophy, herbal medications, and antiretroviral agents have been reviewed. The management of patients taking glucocorticoids, oral diabetic agents and insulin preoperatively and agents affecting hemostasis is complex and should not be discussed in this paper because probably they should need and specific protocol en each center. The recommendations in this review are to a large degree expert opinion, based on information from other review and textbooks, along with clinical experience and theoretic considerations.
Keywords
perioperative management, chronic medications, anesthetic agents, cardiovascular agents, gastrointestinal agents, pulmonary agents, endocrine agents, psychotropic agents
INTRODUCTION
Currently the demand for surgical and anaesthetic procedures is increasing. More than 50 percent of the interventions are carried as major outpatient surgery, and at least 50% of the patients take regularly a pharmacological treatment. Medication errors and their side effects are a major cause of morbidity with clinical and economic consequences for both patients and society. More than half of these errors originate in the processes of care transition, that is, when there is a change in the professional responsible for the patient throughout the therapeutic process. If we are also dealing with surgical patients, the problem is aggravated, since it is essential to manage chronic medication during hospitalization and upon discharge from hospital, making an individualized assessment of the benefit/risk of maintaining or suspending the medication in each case, depending on the surgical procedure to be performed.
The following principles inform the management of chronic medications in the perioperative period:
- A complete medication history should be obtained, and all clinicians involved in patient management (eg, surgeon, anesthesiologist, medical consultants) should review the medication history. Medication use reported by the patient should be verified (medication reconciliation) to address accuracy of drugs and doses. This should include all over-the-counter and herbal/complementary medications, as well as prescription drugs. In addition, substance use information (including alcohol, nicotine, and illicit drugs) should be elicited.
- Medications associated with known medical morbidity if withdrawn abruptly should be continued in the perioperative period or tapered if feasible. Intravenous, transdermal, or transmucosal medicines should be substituted when absorption will be impaired because of loss of gastrointestinal function or restrictions on oral intake. Medications thought to increase the risk of anesthetic or surgical complications and not essential for the short-term should be held through the perioperative period. Other medications can be discontinued or continued based upon clinician judgment.
- The many medications administered perioperatively during a relatively short period increase the potential for drug-drug interactions.
- The metabolism and elimination of medications and their metabolites may be altered during the perioperative period. In particular, gastrointestinal absorption of oral medications may be impaired due to changes in splanchnic blood flow and edema.
- The majority of medications can be resumed once the patient is able to tolerate oral intake. The main exceptions to this are medications that impact the bleeding or thromboembolic risk and are discussed in detail in the relevant medication sections below.
This article is an update on recent management issues in perioperative chronic medication management. Evidence is synthesized from different resources: Continuous review of journals, electronic searching of databases (including Medline and Cochrane Library), as well as other sources of information based in a large degree expert opinion, based on information from other review and textbooks, along with clinical experience and theoretic considerations.
1. Cardiovascular Medications
For elective surgery, preoperative planning and care should be optimized to reduce risk and minimize the need for acute changes in medication management perioperatively. For example, we have to suggest control of clinical signs of heart failure (HF) for one week or longer preoperatively if time permits. Although the optimum intraoperative blood pressure target is unclear, episodes of either hypotension or hypertension should be avoided or promptly treated to minimize the potential for adverse cardiovascular and cerebrovascular outcomes.
Beta blockers
Benefit/risk: Beta blockers have a number of potential beneficial effects when taken perioperatively. Beta blockers reduce ischemia by decreasing myocardial oxygen demand due to increased catecholamine release. They may also help prevent or control arrhythmias. Patients who take beta blockers chronically for management of angina are at risk of ischemia with withdrawal of beta blockade. Acute withdrawal of a beta blocker pre- or postoperatively can lead to substantial morbidity and even mortality. Withdrawal issues are of less concern when beta blockers are used for hypertension or migraine prophylaxis.
Whether to initiate beta blockers as prophylaxis for ischemia in the perioperative period in patients at increased risk for coronary disease is complex and it is not discussed in this paper. Potential adverse effects of perioperative beta blockade include bradycardia and hypotension. Nonselective beta blockers can interact with epinephrine, used for infiltration anesthesia or management of intraoperative anaphylaxis.
Continue/discontinue: In light of the potential benefits of perioperative beta blockade, minimal adverse effects, and consequences of acute withdrawal, beta blockers should be continued in the perioperative period and continued throughout the hospital stay. The dose of the beta blocker should be closely regulated throughout the perioperative period to maintain the blood pressure and heart rate (rate-pressure product) below the patient’s ischemic threshold. Since adequate beta blockade can take weeks to achieve safely in patients with systolic heart failure, initiation of beta blockade in the preoperative period only should be initiated if acute decompensated heart failure is not present and surgery can be substantially delayed. If surgery is urgent, it is better postponing beta blockade until a later date.
Alpha 2 agonists
Benefit/risk: Although earlier smaller randomized trials suggested that centrally acting sympatholytic drugs such as clonidine may improve perioperative outcomes, the larger POISE-2 randomized trial in 10,010 patients undergoing noncardiac surgery found that preoperative initiation of low-dose clonidine resulted in increased harm (no change in mortality or myocardial infarction but increase in clinically significant hypotension and nonfatal cardiac arrest). A sub study of the trial also found no benefit of perioperatively administered clonidine in reducing the risk of acute kidney injury.
For patients already taking clonidine, abrupt withdrawal of clonidine can precipitate rebound hypertension. This usually occurs after abrupt cessation of fairly large oral doses (eg, greater than 0.8 mg/day) but has also been noted in patients using transdermal clonidine.
Continue/discontinue: Given the possible negative consequences of withdrawal, alpha 2 agonist drugs should be continued in the perioperative period, but not initiated.
Calcium channel blockers
Benefit/risk: Data are limited regarding the risks and benefits of calcium channel blockers in the perioperative setting. Small trials have shown a more stable intraoperative hemodynamic profile in patients treated with continuous diltiazem, compared with placebo, during coronary bypass surgery, but these studies are not large enough to demonstrate improved outcomes. Wijeysundera et al. in an observational study, continued use of calcium channel blockers was associated with reduced mortality for patients undergoing cardiac surgery. A meta-analysis found that use of calcium channel blockers was associated with reduced ischemia and atrial arrhythmia in patients undergoing noncardiac surgery.
There are no serious interactions between calcium channel blockers and anesthetic agents. A withdrawal syndrome is not typical of calcium channel blockers, although abrupt discontinuation of these drugs has been reported to cause severe vasospasm in patients undergoing coronary revascularization. Concerns have been raised about a possible association between calcium channel blockers and an increased risk of bleeding. A randomized trial in valvular surgery patients found that, compared with placebo, patients receiving nimodipine had increased bleeding. Reports conflict on whether there is a greater incidence of anemia in patients receiving calcium channel blockers after hip surgery. Two large trials in cardiac surgery patients did not find any association between bleeding risk and use of calcium channel blockers.
Continue/discontinue: Despite little data regarding calcium channel blockers during the perioperative period, these agents appear safe and have theoretic benefit; data regarding bleeding risk are contradictory. Thus, calcium channel blockers are recommend to be continued in patients who are already taking them preoperatively.
Angiotensin-Converting enzyme inhibitors and angiotensin II receptor blockers
Benefit/risk: The management of patients taking angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) preoperatively is controversial. ACE inhibitors and ARBs can theoretically blunt the compensatory activation of the renin-angiotensin system during surgery and result in prolonged hypotension. Also, the effect of these drugs may be different in noncardiac and cardiac surgery as well as with general and neuraxial anesthesia.
Data regarding use of ACE inhibitors and ARBs in the perioperative period are inconsistent, with many studies indicating some increased risk for peri- and postoperative hypotensive episodes but variable adverse effect on cardiovascular outcomes or respiratory outcomes when the medications are continued.
Continue/discontinue: We should individualize the decision to continue or discontinue ACE inhibitors based on the indications for the drug, the patient’s blood pressure, and the type of surgery and anesthesia planned. For most patients, we usually withhold them on the morning of surgery. However, when the indication is for heart failure or poorly controlled hypertension, we continue them to avoid further exacerbation of these conditions. Many anesthesiologists may prefer to withhold these medications on the morning of surgery based on concerns about possible hypotension, and in such cases when we favor continuation, we inform the anesthesiologist of our justification.
We recommend resuming these agents as soon as possible postoperatively, as failure to restart ARBs within 48 hours after surgery has been associated with increased 30-day mortality. As above, most findings suggest that continuing ACE inhibitors up to the time of surgery increases perioperative hypotension but possibly reduces the incidence of postoperative hypertension.
Diuretics
Benefit/risk: The two major physiologic effects of concern of loop and thiazide-type diuretics are hypokalemia and hypovolemia. Hypokalemia can theoretically increase the risk of perioperative arrhythmia, although observational studies of patients with structural heart disease have failed to find such a relationship. Additionally, hypokalemia might potentiate the effects of muscle relaxants used during anesthesia, as well as provoke paralytic ileus.
Systemic vasodilatation induced by anesthetic agents may cause hypotension in patients who are intravascularly depleted from diuretics. However, in a study of elective, noncardiac surgeries in patients chronically treated with furosemide, the administration of furosemide on the day of surgery did not significantly increase the risk for intraoperative hypotension.
Continue/discontinue: There is no consensus on whether diuretics should be discontinued prior to elective surgery. Our approach depends upon the reason for diuretic use and on an individual patient’s history:
- We advise patients who are taking diuretics for hypertension to hold the medication on the morning of surgery. Diuretics may theoretically increase the risk of intraoperative hypotension, and although unlikely to occur in patients on chronic therapy, it is reasonable to hold the medication for this reason.
- For patients receiving diuretic therapy to treat heart failure, diuretic continuation is based upon assessment of volume status, which should be evaluated and optimized preoperatively whenever possible. For patients with well-controlled heart failure and stable volume status, we generally recommend holding the morning dose of diuretic on the day of surgery. For patients with heart failure in whom fluid balance has historically been more difficult to control, we recommend continuing the diuretic without interruption.
If diuretics are held the morning of surgery and volume overload develops, a quick diuresis can be initiated by intravenous administration perioperatively. For patients who require perioperative diuretics, clinicians should pay close attention to potassium replacement.
Non-statin hypolipidemic agents
Benefit/risk: Niacin and fibric acid derivatives (gemfibrozil, fenofibrate) cause myopathy and rhabdomyolysis. The risk is higher when these agents are used in combination with statins, and surgery may also increase the risk of myopathy. Lipid-lowering agents that are bile sequestrants (cholestyramine and colestipol) interfere with bowel absorption of multiple medications that may be required perioperatively. The benefits or risks of ezetimibe in the perioperative period are unknown.
Continue/discontinue: The most appropriate is a temporary discontinuation of niacin, fibric acid derivatives, bile sequestrants, and ezetimibe perioperatively. Discontinuation is likely to be safe since these agents are given for the goal of long-term reduction in vascular morbidity. The optimal interval to discontinue these agents before surgery is unknown. They should be stopped the day before surgery to allow for drug elimination.
Digoxin
Benefit/risk – Studies on digoxin in the perioperative period are limited. The two indications for digoxin are to prevent hospitalization and readmission in patients with reduced left ventricular function and to control ventricular response in atrial fibrillation. One study found perioperative use of digoxin to be a predictor of postoperative ischemia, but this was probably because it was a marker of underlying cardiac disease. A subgroup analysis of patients undergoing intrathoracic surgery found that digoxin decreased the incidence of postoperative supraventricular arrhythmias.
Continue/discontinue – Digoxin should be continuing perioperatively. Obtaining a drug level preoperatively is not usually required.
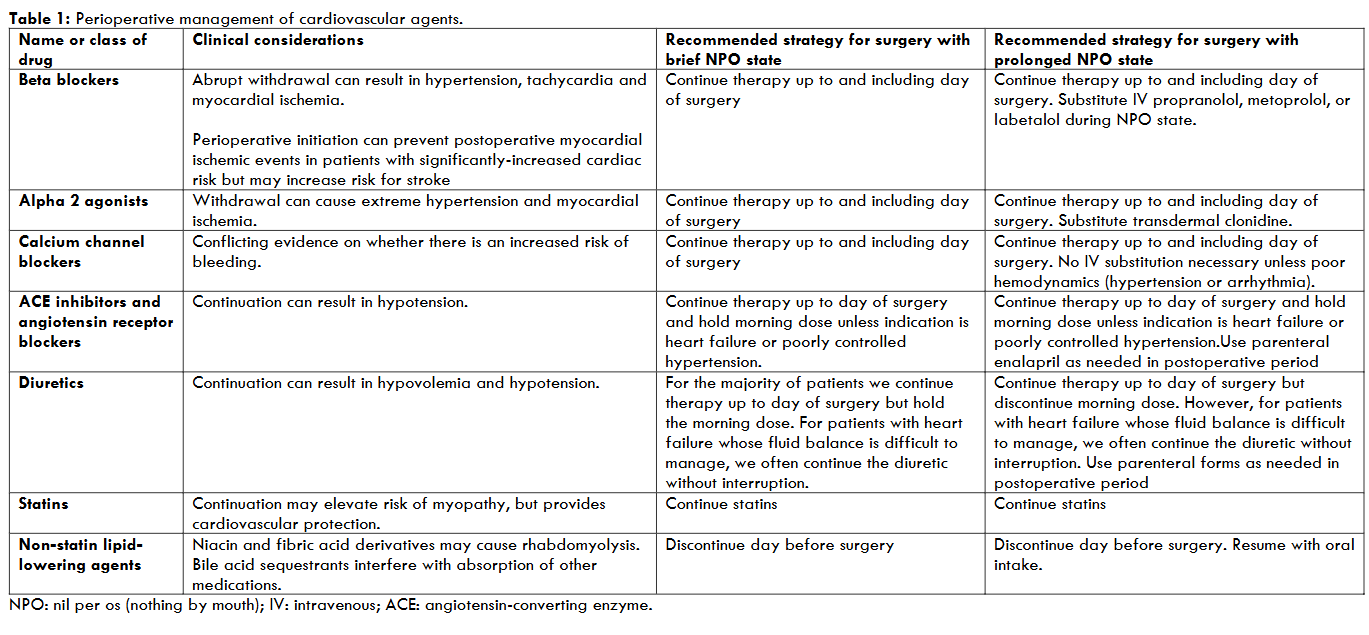
Recommendations for perioperative management of cardiovascular agents are summarized in the table 1.
2. Gastrointestinal Agents
H2 blockers and proton pump inhibitors
Benefit/risk: There are several potential advantages of continuing H2 blockers or proton pump inhibitors perioperatively. The stress of surgery and other conditions (eg, mechanical ventilation and intensive care unit stay) can increase the risk of stress-related mucosal damage, which may be minimized by administration of these drugs. In addition, gastric aspiration during anesthesia, though rare, can lead to severe pulmonary injury. Both H2 blockers and proton pump inhibitors decrease gastric volume and raise gastric fluid pH, thereby reducing the risk of chemical pneumonitis from aspiration.
Although H2 blocker therapy is generally safe, rare central nervous system (CNS) reactions including confusion and delirium are associated with the use of intravenous H2 blockers in critically ill postoperative patients. Patient risk factors for CNS reactions include advanced age, organ dysfunction, and preexisting cognitive impairment. It is uncertain whether any H2 blocker is less likely to cause CNS effects than others.
An increased risk of Clostridioides difficile infection has been associated with proton pump inhibitor use. Neither H2 blockers nor proton pump inhibitors have been shown to interact with common anesthetic agents, although cimetidine can alter the metabolism of several drugs.
Continue/discontinue: Based upon the potential benefits and lack of contraindications, patients who are taking either H2 blockers or proton pump inhibitors should remain on these medications in the perioperative period.
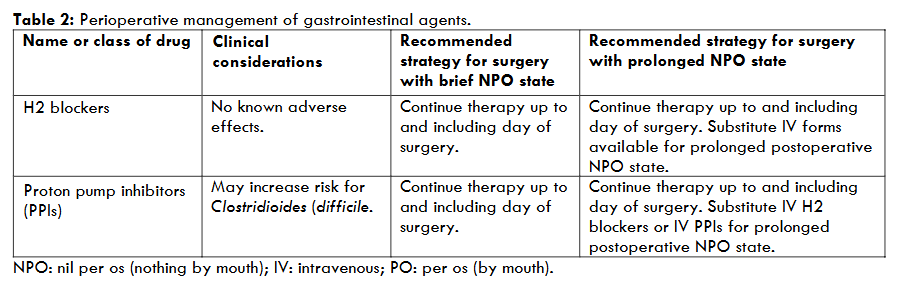
Recommendations for perioperative management of these agents are summarized in the table 2.
3. Pulmonary Agents
Inhaled beta agonists and anticholinergics
Benefit/risk: Inhaled medications used to control obstructive pulmonary disease, such as beta agonists (albuterol, salmeterol, formoterol) and anticholinergics (ipratropium, tiotropium), have been found to reduce the incidence of postoperative pulmonary complications in patients with asthma and chronic obstructive pulmonary disease and should be continued perioperatively.
Continue/discontinue: Beta agonists should be continuing in the perioperative period, including the day of surgery. The drugs can be administered through a nebulizer or in the circuit of the ventilator when use of metered-dose inhalers is not possible.
Theophylline
Benefit/risk: There are no data indicating whether continuation of theophylline in the perioperative period decreases pulmonary complications. Theophylline has the potential to cause serious arrhythmias and neurotoxicity at a level just beyond the therapeutic range, and theophylline metabolism is affected by many common perioperative medications.
Continue/discontinue: Theophylline medication should be discontinued the evening before surgery.
Inhaled corticosteroids
Benefit/risk: Patients with pulmonary disease who are maintained on corticosteroids are at risk of adrenal insufficiency if steroids are abruptly withdrawn, particularly in the face of increased stress related to surgery. Additionally, glucocorticoids in such patients may be necessary to maintain optimal lung functions. The risk of possible perioperative complications related to glucocorticoids, including wound infections, is low.
Continue/discontinue: Both inhaled and systemic glucocorticoids should be continued during the perioperative period.
Leukotriene inhibitors
Benefit/risk: The leukotriene inhibitors zafirlukast and montelukast help maintain asthma control but are not used for acute therapy. The elimination half-life of these agents is relatively short, but their effect on asthma symptoms and pulmonary function continues for up to three weeks after cessation of treatment. There is no evidence of a withdrawal syndrome with abrupt stoppage of these agents. We are aware of no evidence of harmful interactions of these drugs with anesthetics.
Continue/discontinue: Leukotriene inhibitors should be given on the morning of surgery and resumed when the patient is tolerating oral medications.
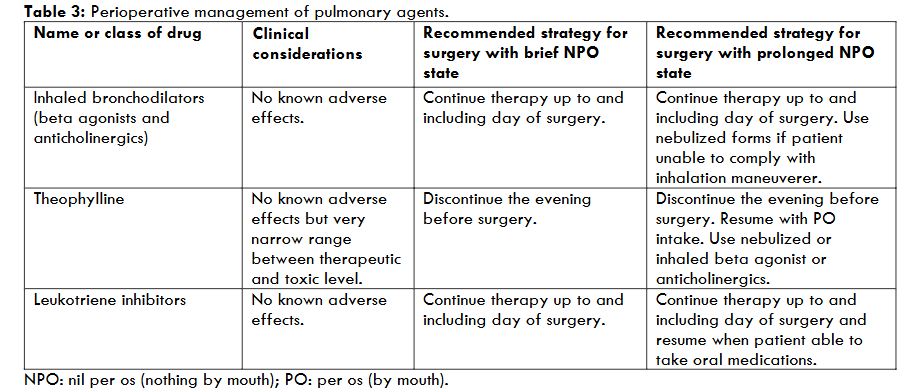
Recommendations for perioperative management of these agents are summarized in the table 3.
4. Endocrine Medications
As we comment on above, the management of patients taking glucocorticoids, oral diabetic agents, insulin preoperatively, and other antidiabetic therapy (GLP-1 receptor agonists, Sodium-glucose cotransporter 2 inhibitors) is complex and should not be discussed in this paper.
Oral contraceptives
Benefit/risk: Oral contraceptives (OCs) are statistically the most frequent cause of thrombosis in young women due to their widespread use. The risk of thrombosis increases within four months of initiation and decreases to previous levels within three months of stopping treatment. Surgery itself is a risk factor for thrombosis and compounds the risk associated with oral contraceptive use.
OCs with higher estrogen content (≥35 mcg) have a greater risk of thromboembolism compared with those with lower estrogen content (≤30 mcg). Nevertheless, even the lower estrogen content pills are associated with an increased risk of thrombosis. Estrogen/progestin patches also increase thrombosis risk. Risk also varies with type of progestin.
Continue/discontinue: In general, OCs should be continued and provision of appropriate perioperative thromboprophylaxis. In patients at higher risk for venous thromboembolism (VTE) who are undergoing high-risk surgery, discontinuation of OCs may be reasonable to mitigate the additional VTE risk; if the decision is made to discontinue, OCs should be stopped four weeks prior to surgery. Women who discontinue OCs that are used for contraceptive purposes should use an alternative method of birth control, which should be continued for the first week after resuming OCs postoperatively. If they cannot or prefer not to use an alternative method, continuing the OC is appropriate (with appropriate perioperative thromboprophylaxis). Prevention of thromboembolic disease in the surgical patient is discussed elsewhere.
We recommend a serum pregnancy test prior to surgery in all women of childbearing age.
Estrogen-based hormone therapy. Postmenopausal hormone therapy
Benefit/risk: The estrogen content of preparations used for postmenopausal hormone therapy (HT) is much lower than in oral contraceptive pills. However, use of oral HT, with estrogen alone or estrogen plus a progestin, still appears to increase the risk of VTE. Although a case-control study did not find an increased risk of thromboembolism in those undergoing arthroplasty who received oral HT, the results may have been confounded by patients at lower risk for thromboembolism being more likely to be prescribed HT. Transdermal estrogen does not appear to increase risk for VTE in the general population, even among those with an elevated baseline risk for VTE; however, no data exist for surgical patients. The risks associated with temporary discontinuation of hormone therapy are mainly discomfort from hot flashes and other menopausal symptoms.
Continue/discontinue: Usually it should be individualizing the decision to continue HT perioperatively based on the VTE risk of the procedure and the patient’s preference, but overall we feel the risk of continuing HT is relatively low. Ideally, individuals undergoing procedures associated with moderate to high risk for VTE should stop hormone therapy at least two weeks prior to elective surgery and resume treatment postoperatively once the period of elevated risk for VTE has resolved. HT can be continued uninterrupted for surgical procedures associated with a low risk of VTE.
Selective estrogen receptor modulators
Benefit/risk: The indications for use of selective estrogen receptor modulators (SERMs) such as tamoxifen and raloxifene include breast cancer treatment, breast cancer chemoprevention, and, at least for raloxifene, the prevention and treatment of osteoporosis. Both tamoxifen and raloxifene increase the risk of VTE. Brief discontinuation of SERMs used for the prevention/treatment of osteoporosis or the prevention of breast cancer is unlikely to result in harm. For patients with breast cancer who are being treated with SERMs, the risk of disease progression with preoperative cessation of treatment is a consideration.
Continue/discontinue: SERMs can be continued without interruption for low- and moderate-risk surgeries while providing appropriate VTE prophylaxis. For surgeries with a high-risk of VTE, our approach depends upon the specific SERM and the indication for its use:
- For patients taking raloxifene for osteoporosis treatment/prevention or breast cancer prevention, we suggest discontinuing the medication three days prior to a surgical procedure associated with a high risk of VTE. The raloxifene can be resumed as soon as the period of elevated VTE risk is resolved. However, if the patient has taken the medication within three days of the procedure, we do not recommend postponing the surgery for this reason; the procedure can be done as planned and appropriate VTE prophylaxis provided.
- For patients taking tamoxifen for breast cancer prevention (eg, in women without a history of breast cancer), we suggest discontinuing the medication two weeks prior to a surgical procedure associated with a high risk of VTE. The tamoxifen can be resumed as soon as the period of elevated VTE risk has resolved. However, if the patient has taken the medication within two weeks of the procedure, do not be postponing the surgery for this reason; the procedure can be done as planned and appropriate VTE prophylaxis provided.
- For patients taking a SERM (eg, tamoxifen) for breast cancer treatment, the decision to discontinue is more difficult, and consultation with an oncologist is recommended. We typically recommend continuing SERMs in this setting while providing appropriate VTE prophylaxis.
The package insert for tamoxifen states that in the case of surgery and immobility, the medication should only be stopped if the risk of tamoxifen-induced thrombosis clearly outweighs the risks associated with interrupting treatment. If continued, all patients should receive appropriate thrombosis prophylactic measures. The manufacturers of raloxifene, however, recommend stopping it at least three days before surgery.
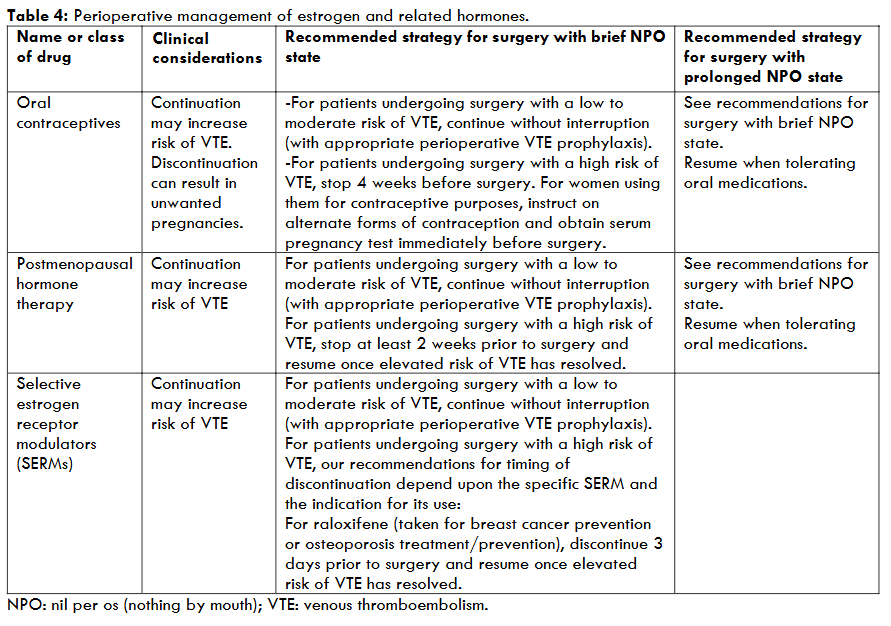
Recommendations for perioperative management of these agents are summarized in the table 4.
Drugs used for thyroid
Continue/discontinue: Perioperative therapy for both hyperthyroidism and hypothyroidism should be continued. In the case that a patient cannot take oral medications for several days, the approach depends upon the thyroid medication:
- Thyroxine (T4) has a long half-life, and patients on chronic T4 therapy who are unable to take oral medication for several days do not need parenteral T4. If oral T4 cannot be resumed within five to seven days, it should then be administered parenterally (intravenously or intramuscularly).
- The antithyroid thionamide medications (methimazole and propylthiouracil) have a very short half-life. The decision on how long to hold antithyroid medications for a patient who is unable to take oral medications must be individualized based upon several factors, including the patient’s history of thyroid disease and length of previous treatment with antithyroid medications.
Drugs used for osteoporosis/osteopenia
Benefit/risk: Bisphosphonate use, especially in malignancy, has been associated with osteonecrosis of the jaw in patients undergoing dental surgery. The absolute risk is very low, but osteonecrosis is difficult to manage. The duration of effect of bisphosphonates on bone remodeling is long, and the discontinuation of these agents for weeks or even months before surgery has not been shown to decrease the risk of osteonecrosis. Likewise, there is no evidence that short-term discontinuation of these agents results in reduction in treatment efficacy for prevention of osteoporotic bone fractures.
Continue/discontinue: We recommend withholding bisphosphonates only on the morning of surgery, as they are typically taken with at least 100 mL of water and the patient is supposed to remain upright for at least 30 minutes and until after eating a meal. Guidelines from the American Association of Oral and Maxillofacial Surgeons recommend proceeding as usual with dental surgery in patients who have been treated with oral bisphosphonates for less than four years and have no clinical risk factors. They suggest discontinuing bisphosphonates for two months prior to performing the dental surgery if a patient has been treated for more than four years or has taken concomitant glucocorticoids. Bisphosphonates are restarted when the bone has healed.
We generally agree with these guidelines and advise that, for patients undergoing dental surgery, bisphosphonates not be held in advance of the procedure nor dental surgery delayed since the absolute risk of jaw osteonecrosis is low and the benefit of holding the medication in advance is not clear. For patients believed to be at very high risk due to need for extensive bony surgery, concomitant glucocorticoid or chemotherapy, or long-term bisphosphonate use, a delay of surgery for two months is reasonable, although these cases are uncommon.
5. Medications Affecting Kidney Function
Acute kidney injury (AKI) is defined by a rise in the serum creatinine concentration or a decline in urine output that develops within hours to days. AKI is commonly, though not always, caused by acute tubular necrosis (ATN), particularly among postoperative patients and critically ill hospitalized patients. Several medications and agents used during the perioperative period may lead to acute kidney injury, including nonsteroidal antiinflammatory drugs (NSAIDs), ACE inhibitors, angiotensin II receptor blockers (ARBs), diuretics, antibiotics (eg, aminoglycosides, vancomycin), and intravenous contrast agents. The benefits and risks vary based on each drug. Patients who are at high risk for ischemic ATN should have interventions to prevent AKI. Interventions include optimizing volume status and avoiding or stopping nephrotoxins, if possible. There is not consensus to administer any pharmacologic agent (such as diuretics or dopamine) for the prevention of ischemic ATN.
6. Psychotropic Medications
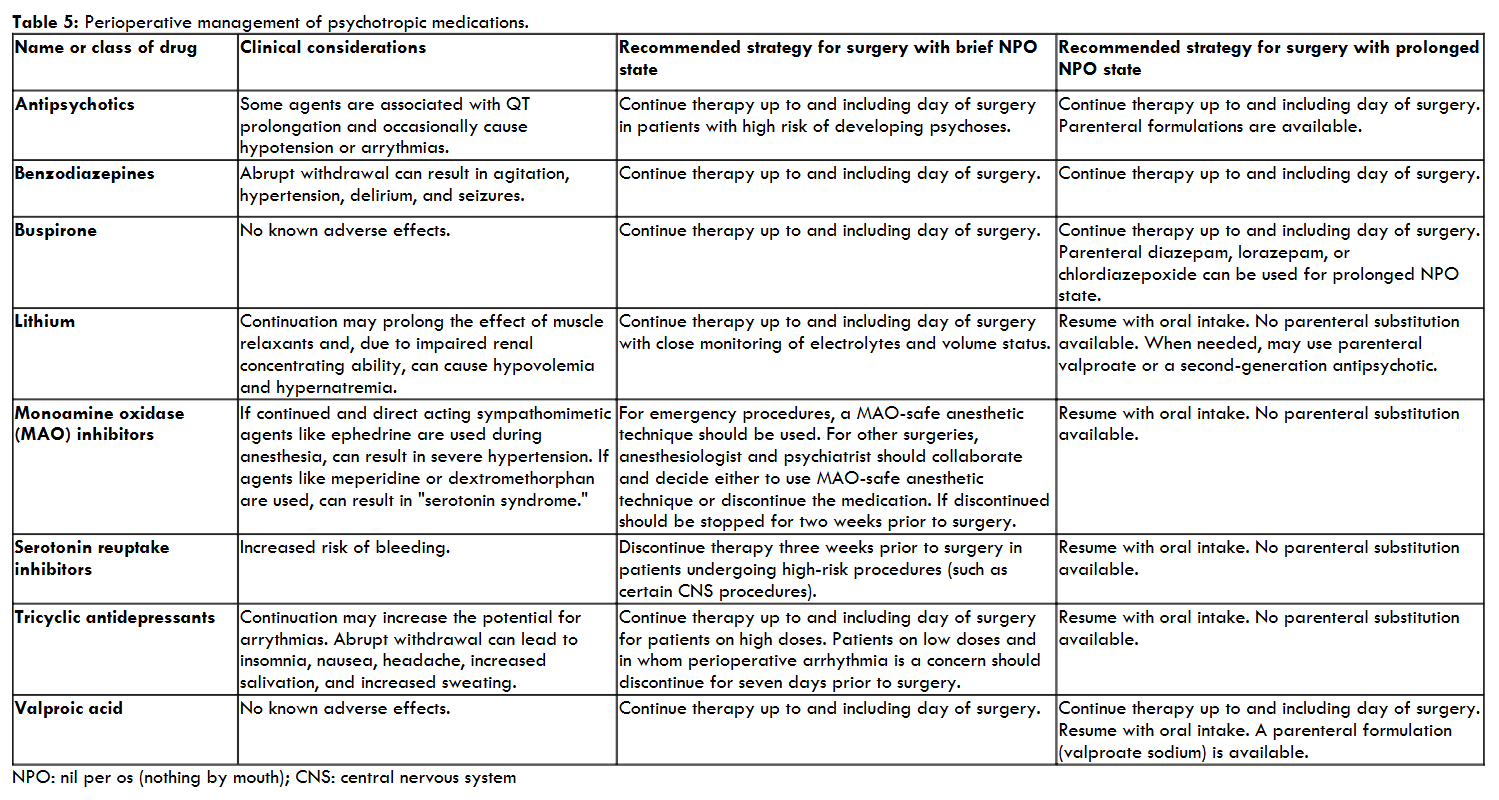
The perioperative management of patients taking psychotropic agents varies with the class of drugs used and severity of mental illness. Evidence-based guidelines for these drugs are lacking; data are primarily derived from case reports and open trials. Perioperative decisions about use of these drugs must balance their potential for side effects and interaction with anesthetic agents with psychiatric and physiologic consequences of withdrawal of these agents. In general, psychotropic medications for treatment of patients with serious or unstable mental illness should be continued throughout the perioperative period to avoid psychiatric decompensation. However, the optimal choice of anesthesia and analgesia in combination with many psychotropic agents is unknown. Other than antipsychotics, many psychotropic agents do not have a parenteral delivery mode. Appropriate pharmacologic management includes consideration of parenteral alternatives of the same or different class to maintain mood and behavior stability.
Tricyclic and tetracyclic antidepressants
Benefit/risk: Cyclic antidepressants inhibit the uptake of norepinephrine and serotonin at the synaptic cleft. Unlike most newer antidepressants, cyclic antidepressants lower the seizure threshold and possess significant anticholinergic, antihistaminic, and alpha-1 blocking properties. These agents delay gastric emptying, prolong the QTc interval, and may increase the risk for arrhythmias in combination with some volatile anesthetics or sympathomimetic agents, although literature to support this concern is scant. Abrupt withdrawal of tricyclic antidepressants can lead to insomnia, nausea, headache, increased salivation, and sweating and should be avoided if feasible.
Cyclic antidepressants can amplify the systemic pressor effects of norepinephrine and epinephrine; however, use with epinephrine-containing local anesthesia is generally safe. Use with atropine or scopolamine may increase postoperative confusion.
Continue/discontinue: The US Food and Drug Administration (FDA) and some experts advise that tricyclic antidepressants (imipramine, amitriptyline, nortriptyline, desipramine, and clomipramine) be discontinued prior to elective surgery, when possible, and this information is provided in package labelling for these medications. The stability of the patient’s depression should be considered prior to tapering or discontinuing the medication to avoid worsening of depression. If depression is moderate or severe, best practice would be to continue the antidepressant and notify the anesthesia team to monitor for cardiac arrhythmias in the perioperative period. If depression is mild, the antidepressant is not felt to be essential for short-term quality of life, and if arrhythmias are of concern, the agent should be tapered to minimize the chance of withdrawal.
Continuations of cyclic agents throughout the perioperative period, in particular for patients on high doses without cardiac disease is generally recommend. For patients on low doses or in whom the risk of perioperative arrhythmia is increased, the agents should be tapered off over a period of 7 to 14 days before surgery. The elimination half-life of various cyclic antidepressants ranges from one to three days or more.
Selective serotonin reuptake inhibitors
Benefit/risk: Selective serotonin reuptake inhibitors (SSRIs) may increase bleeding risk and the consequent need for transfusion with surgery, perhaps because of their effects on platelet aggregation. Bleeding risk with SSRIs has been documented primarily in association with antiplatelet or nonsteroidal antiinflammatory drug (NSAID) use.
Stopping SSRIs could lead to exacerbation of mood and other disorders. The washout period for SSRIs may be as long as three weeks, and reinitiation may not lead to clinical benefit for several weeks. Half-life varies widely from 15 hours (ie, paroxetine, fluvoxamine, sertraline) up to seven days (fluoxetine). Abrupt withdrawal of short-acting SSRIs should be avoided, as it can cause a discontinuation syndrome including dizziness, chills, muscle aches, and anxiety. Determining whether perioperative continuation or withdrawal of SSRIs produces a net clinical benefit requires randomized controlled trials.
Continue/discontinue: For most patients, we recommend continuing SSRI therapy through the perioperative period. The decision to withhold SSRIs perioperatively should balance the consequences of bleeding with the severity of the underlying psychiatric disorder.
For patients undergoing surgical procedures with substantial risks of postoperative bleeding that could lead to significant morbidity (such as CNS procedures), or in patients requiring ongoing antiplatelet therapy for secondary prevention (eg, aspirin and thienopyridine for a drug-eluting cardiac stent), consider discontinuing SSRIs by tapering several weeks prior to surgery and starting an alternative antidepressant regimen, in consultation with a psychiatrist if possible. Patients with severe mood disorders and those undergoing surgery with low to moderate risks of abnormal bleeding should generally be maintained on SSRIs through surgery.
Antiplatelet agents should be discontinued preoperatively if at all possible, in patients taking SSRIs. If aspirin or thienopyridine therapy is required for secondary prevention through surgery (eg, presence of a drug-eluting cardiac stent), then the SSRI should be discontinued in advance of surgery and an alternative antidepressant regimen considered, in consultation with a psychiatrist if possible.
Selective norepinephrine reuptake inhibitors and bupropion
Benefit/risk: There are limited data regarding selective norepinephrine reuptake inhibitor (SNRI) agents in the perioperative period. Tully PG et al. in a retrospective study of 4136 patients undergoing coronary artery bypass graft surgery showed that SNRI use was associated with an increased risk of renal dysfunction and prolonged ventilation but not bleeding events or long-term mortality. This has not been replicated in other studies.
No literature exists regarding perioperative considerations with bupropion.
Continue/discontinue: Considerations regarding cessation versus continuation in the perioperative period should be similar as with SSRIs.
Monoamine oxidase inhibitors
Benefit/risk: Nonselective irreversible monoamine oxidase (MAO) inhibitors for use as antidepressants (isocarboxazid, pargyline, phenelzine, and tranylcypromine) are prescribed far less commonly than other antidepressants but are used in patients with refractory mood disorders in whom withdrawal and recurrent depression may be problematic. MAO inhibitors are also used for treatment of conditions other than depression.
Use of nonselective MAO inhibitors results in the accumulation of biogenic amines in central and autonomic system neurons. Concomitant administration of sympathomimetic agents, like ephedrine during anesthesia, can result in massive release of stored norepinephrine and severe hypertensive crisis. In addition, two types of CNS reactions may occur relevant to surgery and anesthesia. The “Type I” reaction occurs with the administration of anticholinergics (such as dextromethorphan) and meperidine with MAO inhibitors, leading to a serotonin syndrome (agitation, headache, fever, and seizures, with possibility of coma and death). The “Type II” reaction occurs when the MAO inhibitor inhibits hepatic microsomal enzymes involved in opiate metabolism, subsequently leading to accumulation of free narcotic, sedation, respiratory depression, and cardiovascular collapse. It is a good choice the use of lower-risk opioids, including morphine, codeine, buprenorphine, oxymorphone, or hydromorphone, to mitigate risk for a Type I reaction. Patients continuing MAO inhibitors requiring opioid therapy with higher-risk agents (fentanyl, oxycodone or methadone should be monitored closely for CNS depressive effects. Phenelzine may prolong the effect of succinylcholine. Use with epinephrine-containing local anesthetics is generally safe.
Continue/discontinue: The decision to continue or withhold nonselective MAO inhibitors before surgery requires close collaboration with the anesthesiologist and psychiatrist. MAO inhibitors generally should be continued when two criteria are met: the anesthesiologist is comfortable with use of MAO-safe procedures and the psychiatrist believes temporary withdrawal of the agent will exacerbate or precipitate a depressive syndrome. In the absence of either criteria, we recommend discontinuing MAO inhibitors before surgery. Many MAO inhibitors are irreversible antagonists, and recovery of MAO function requires two weeks after discontinuation of the drug. Thus, patients should taper and discontinue MAO inhibitors two weeks before elective surgery. An alternative drug regimen for depression, such as tricyclic antidepressant or SSRI therapy, may be used for the perioperative period.
If MAO inhibitors are continued perioperatively, the patient must be prescribed a diet that excludes foods containing high amounts of tyramine while an inpatient to avoid precipitating a hypertensive crisis. Intraoperative and perioperative drug interactions must be closely monitored.
Mood stabilizing agents (lithium and valproate)
Benefit/risk: Lithium has a number of physiologic effects that may be important perioperatively. Lithium decreases release of neurotransmitters and may prolong the effect of neuromuscular blockers. Lithium has a narrow therapeutic index, is highly dependent upon maintained renal function for clearance, and is subject to drug interactions with diuretics, NSAIDs, angiotensin-converting enzyme (ACE) inhibitors, and serotoninergic drugs (eg, meperidine, methylene blue, tramadol). Chronic lithium use has a multitude of effects on the thyroid. In addition, arginine vasopressin resistance (previously called nephrogenic diabetes insipidus) has been described in up to 20 percent of patients taking lithium. Patients who have impaired renal concentrating ability maintain euvolemia and normal serum sodium through polydipsia. Access to free water may be impaired during the perioperative period and lead to volume depletion and hypernatremia.
Valproate (valproic acid) is another mood stabilizer used in patients with bipolar disorder. Valproate drug interactions include NSAIDs and some antibiotics. There are no reports demonstrating problems in patients continuing valproic acid perioperatively.
Continue/discontinue: Lithium and valproate are used for treatment of serious mental illness. We therefore recommend continuation of lithium perioperatively with increased attention to fluid and electrolyte monitoring and a low threshold to check thyroid function tests before surgery. We recommend that valproic acid should be continued too.
Serum levels of lithium and valproate should be monitored regularly. Serum lithium levels are affected by medications that affect sodium and fluid balance.
Antipsychotics
Benefit/risk: Antipsychotics are effective in controlling psychoses that may become problematic in the perioperative period in patients with underlying psychiatric illness. However, findings from a large observational study indicate that use of antipsychotics, both typical and atypical, is associated with an increased risk for sudden death. Both typical and atypical antipsychotics may prolong the QT interval and cause arrhythmia, particularly when co-administered with volatile anesthetic agents or drugs such as erythromycin, quinolones, amiodarone, and sotalol.
Continue/discontinue: Antipsychotics should be used cautiously in patients at risk for exacerbation of psychoses. These agents should be withheld in patients whose baseline or follow-up electrocardiogram demonstrates prolongation of the QT interval. Shorter-acting and low-dose antipsychotics should be considered, and complete discontinuation may be preferable after consultation with a psychiatrist. The half-life of antipsychotics varies widely. Rarely, withdrawal symptoms (eg, nausea, vomiting, insomnia) or rebound psychoses can occur following abrupt discontinuation. Antipsychotics may potentiate sedative and hypotensive effects of anesthetics and opiate analgesics. They variably cause extrapyramidal side effects and, rarely, neuroleptic malignant syndrome. Several antipsychotics undergo or inhibit CYP2D6 and/or CYP3A4 drug metabolism and thereby can interact with other drugs used perioperatively (eg, antibiotics, midazolam, ketamine). Parenteral administration of antipsychotics seems to increase the perioperative risk of additive sedation, hypotension, or QTc prolongation with other drugs.
Antianxiety agents
Benefit/risk: Abrupt withdrawal of chronic benzodiazepines can lead to an excitatory state with hypertension, agitation, delirium, and seizures. Many of these agents have active metabolites, and withdrawal can occur several days to weeks after discontinuation. Withdrawal symptoms can occur in less than 24 hours following abrupt discontinuation of chronic alprazolam use. Conversion to an extended release preparation of alprazolam prior to surgery may be useful for delaying the need for postoperative re-dosing.
Benzodiazepines are commonly used short-term to relieve preoperative anxiety and are generally safe, with proper monitoring, in the perioperative period. Additive sedation or increased tolerance to perioperative anesthetic and sedative agents may be observed.
Buspirone is felt to be safe in the perioperative period; it has been reported to reduce the shivering threshold intraoperatively in conjunction with dexmedetomidine with minimal sedation and no respiratory depression. It has a slow onset of effect (ie, weeks) and does not prevent withdrawal reactions due to discontinuation of benzodiazepines.
Continue/discontinue: Benzodiazepines or buspirone used chronically for antianxiety or sedative effects should be continued perioperatively.
Psychostimulants
Psychostimulant medications, used in the treatment of attention deficit hyperactivity disorder, may increase risk for hypertension and arrhythmias, lower the seizure threshold, and interact with medications that could be needed in the perioperative period (eg, vasopressors). There is a risk of sudden blood pressure increase when halogenated anesthetics are used in conjunction with methylphenidate, and, per drug labeling, the stimulant should be withheld on the day of surgery.
Benefit/risk: Psychostimulants are not associated with adverse effects when discontinued in the non-abusing patient. Patients generally do not need to be concerned about alertness on the day of surgery.
Continue/discontinue: Data are limited but risks are low of temporarily discontinuing psychostimulant medications. We recommend they be withheld on the day of surgery and resumed when the patient is stable.
Recommendations for perioperative management of these agents are summarized in the table 5.
7. Chronic Opioid Therapy
Peri- and postoperative pain management in opioid dependent patients is not discussed in this paper.
Naltrexone, methadone
Benefit/risk: Naltrexone is a derivative of oxymorphone that acts as a competitive antagonist at opioid receptor sites, showing the highest affinity for mu receptors. It decreases cravings and helps maintain abstinence in opioid addicted patients and is also used for the treatment of alcoholism. As with buprenorphine, chronic naltrexone use may increase CNS opioid receptor concentration, potentially resulting in a transient exaggerated response to agonists in an acute pain situation.
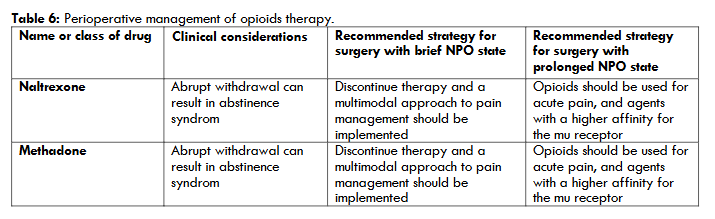
Continue/discontinue: Naltrexone should be discontinued (or the intramuscular dose held) in anticipation of surgery, and a multimodal approach to pain management should be implemented, including the use of local anesthetics with or without sedation, nonsteroidal antiinflammatory drugs (NSAIDs), acetaminophen, corticosteroids, tricyclic antidepressants, or nerve stabilizers such as gabapentin. Opioids should be used for acute pain, and agents with a higher affinity for the mu receptor (such as morphine, fentanyl, or hydromorphone) are recommended. In addition, a “reverse ladder” approach has been suggested to de-escalate opioid agonist therapy in the postoperative period, utilizing nonopioid alternatives for pain control in conjunction with resumption of the antagonist agent.
Recommendations for perioperative management of these agents are summarized in the table 6.
8. Perioperative Management Of Patients With Rheumatic Disease
All patients with rheumatic disease should have a careful preoperative history and physical examination. Preoperative laboratory and imaging studies should be based on patient-specific factors and the planned surgical procedure. Perioperative care in patients with rheumatic disease requires special attention to the following issues to minimize both risk of disease flare and surgical complications:
- Assessing disease activity and optimizing the medication regimen.
- Recognizing the increased cardiovascular risk associated with rheumatic diseases.
- Addressing states of altered coagulation in patients with antiphospholipid syndrome.
- Minimizing risk of surgical site infections in the setting of immunosuppressive medications.
Perioperative management of immunosuppressive therapy is largely based on low-quality evidence and expert opinion. A rheumatologist should be involved in perioperative medication management. Disease severity must be considered in perioperative immunosuppression for patients with some diseases, such as systemic lupus erythematosus.
Glucocorticoids
Benefit/risk: The major concerns regarding glucocorticoid use in the setting of surgery are risks of surgical site infections and hemodynamic instability (secondary to glucocorticoid-induced adrenal insufficiency). Ideally, the lowest possible dose of glucocorticoids should be used in the perioperative setting in order to minimize these risks.
Nonsteroidal antiinflammatory drugs
Benefit/risk: Aspirin and other nonsteroidal antiinflammatory drugs (NSAIDs) may need to be stopped prior to surgery to avoid bleeding and kidney damage, depending on the type of NSAID, type of surgery, and other patient factors.
Nonbiologic disease-modifying antirheumatic drugs
We continue current doses of nonbiologic disease-modifying antirheumatic drugs (DMARDs) including methotrexate, leflunomide, hydroxychloroquine, apremilast, and/or sulfasalazine throughout the perioperative period.
Biologic disease-modifying antirheumatic drugs
We withhold biologic DMARDs and plan elective surgery at the end of the dosing cycle for that specific medication. These agents (abatacept, adalimumab, etanercept, infliximab, rituximab and tocilizumab) should not be restarted until external wound healing is complete, which is typically around two weeks.
Janus kinase inhibitors
We withhold Janus kinase inhibitors (tofacitinib, baricitinib and upadacitinib) for at least three days prior to surgery.
Recommendations for perioperative management of biologic disease modifying antirheumatic drugs are summarized in the table 7.
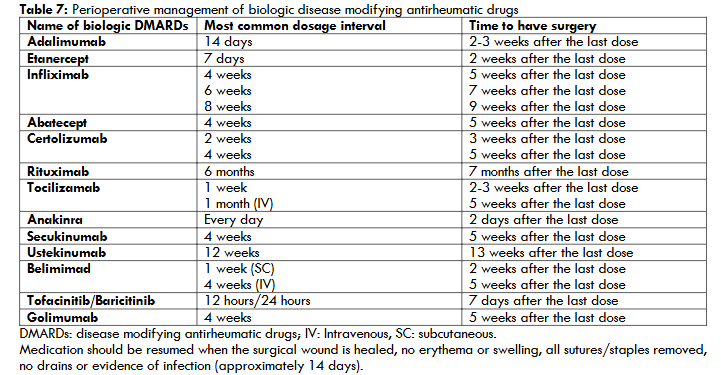
Medication should be resumed when the surgical wound is healed, no erythema or swelling, all sutures/staples removed, no drains or evidence of infection (approximately 14 days).
9. Perioperative Management Of Patients With Neurologic Disease
Important considerations for the perioperative care of patients with neurologic disease are the management of medications used to treat neurologic disorders, an understanding of the pathophysiologic mechanism of these disorders, prevention of adverse intraoperative events, and evaluation of new neurologic changes that occur perioperatively. Anesthesiologists are additionally concerned with understanding the impact of the neurologic disorder on anesthetic management, as well as minimizing perioperative physiologic changes that can impact the neurologic disorder and lead to an adverse perioperative event. The more commonly encountered neurologic disorders and their perioperative management are reviewed here. Perioperative management of patients with traumatic brain injury, patients who undergo craniotomy and spine surgery, and patients with spinal cord injury are not discussed.
Seizures disorders
Seizures that occur during the perioperative period may be due to metabolic derangements, drug and alcohol withdrawal, or intracranial surgery, or rarely may be anesthetic related. They may also arise from premorbid epilepsy, particularly when antiseizure medication therapy has been disrupted. Seizures that occur during a surgical procedure can increase morbidity and mortality.
Patients with preexisting seizure disorders generally need to have antiseizure medications continued perioperatively, with as little disruption as possible. Other patients with new-onset perioperative seizures should probably be treated with antiseizure medication therapy while the underlying cause is evaluated.
Parkinson disease
The major perioperative issues in patients with Parkinson disease are impaired swallowing and pulmonary function potentially leading to pneumonia. The use of meperidine (for postoperative analgesia) should be avoided in patients taking monoamine oxidase type B (MAO-B) inhibitors (selegiline, rasagiline). Patients may also be at increased risk of postoperative delirium and other medical and surgical complications.
Cerebrovascular disease
Patients with cerebrovascular disease are at risk for perioperative stroke and for major adverse cardiac events.
Postoperative delirium
Postoperative delirium may develop in the immediate postoperative period as the patient emerges from anesthesia, or it may follow lucid intervals for several days. Postoperative delirium may be caused by sepsis, medications, and a number of metabolic derangements. Delirium in hospitalized patients increases the length of stay, risk of complications, mortality, and postdischarge institutionalization.
Myasthenia gravis
For patients with myasthenia gravis, myasthenic crisis with respiratory failure is the most concerning complication in the perioperative period. The medication regimen should be disrupted as little as possible and medications that can exacerbate myasthenia should be avoided.
Neuromuscular disorders (Multiple sclerosis, Amyotrophic lateral sclerosis and Guillain-Barré syndrome)
For patients with denervating neuromuscular disorders and neurologic disorders associated with muscle weakness, the depolarizing neuromuscular blocking agent (NMBA) succinylcholine should be avoided during anesthesia because of an increased risk of severe hyperkalemia. These patients may have a variable response to nondepolarizing NMBAs (eg, rocuronium, vecuronium, cisatracurium).
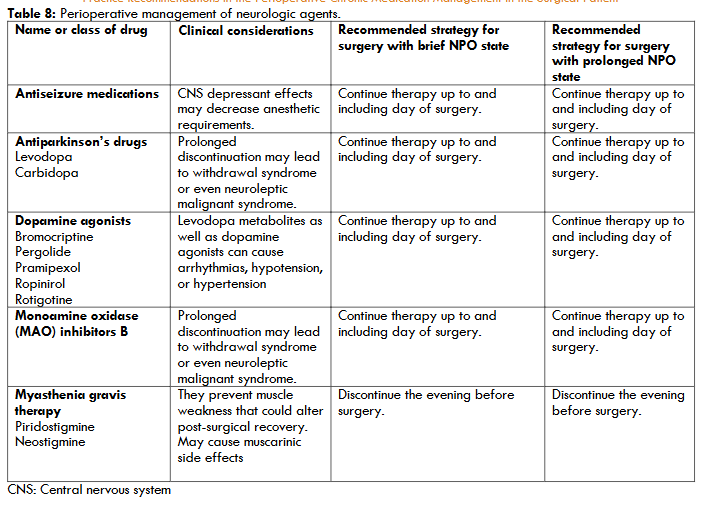
Recommendations for perioperative management of these agents are summarized in the table 8.
10. Perioperative Management of Medications for Benign Prostatic Hypertrophy
Alpha-adrenergic receptor blockers
Benefit/risk: Hypotension is an important potential side effect. Blood pressure should be monitored in patients who are started on alpha-adrenergic receptor blockers due to the risk of hypotension. Doses are titrated over several weeks. Terazosin and doxazosin carry a higher risk of hypotension; for these medications, bedtime dosing may reduce the impact of postural lightheadedness.
Intraoperative floppy iris syndrome – Alpha-1 antagonists, particularly tamsulosin, have been associated with intraoperative floppy iris syndrome (IFIS) with cataract surgery. So, in patients with planned cataract surgery, it should be delaying the initiation of alpha-1 antagonists until after surgery is completed. Alpha-1 antagonists, particularly tamsulosin, have been associated with IFIS. IFIS is a surgical condition associated with cataract operations, characterized by a triad of findings: intraoperative miosis despite preoperative dilation; iris prolapse; and a billowing, flaccid iris. Although a causal relation between the use of alpha-1 adrenergic blockers and IFIS remains controversial, IFIS is associated with increased rates of iris trauma and posterior capsular rupture during cataract surgery. In patients already on alpha-1 antagonists, there are insufficient data to recommend withholding or discontinuing the medication if the need for cataract surgery arises. In such patients, preoperative alpha-1 antagonist use should be discussed in advance with the ophthalmologist, as perioperative precautions may be taken to reduce the risk of IFIS complications.
Cardiovascular risk – An association between alpha-1 adrenergic receptor antagonists and adverse cardiovascular events has been reported. Following the landmark Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial, in which patients receiving doxazosin had a 25 percent increased risk of cardiovascular events, guidelines no longer recommend alpha-1 adrenergic blockers as initial therapy for hypertension.
11. Antiretroviral Agents
Surgical morbidity and mortality: With widespread use of antiretroviral therapy (ART), generally favourable surgical outcomes have been reported among patients with HIV undergoing a wide range of surgical procedures. Most studies have shown slightly greater morbidity and mortality compared with uninfected populations, especially in patients who have AIDS-related complications or lower CD4 cell counts. A CD4 cell count and HIV viral load should be performed if not available within the preceding three months. A review of potential drug interactions with antiretroviral medications should be performed in preparation for induction of sedation and anesthesia.
Perioperative management: When altered mental status or gastrointestinal tract dysfunction interferes with the ability of the patient to take oral medications, all antiretroviral drugs should be held. In the patient with AIDS, parenteral alternatives should be sought for agents used for prophylaxis against opportunistic infections if a prolonged duration of poor oral intake is anticipated.
12. Herbal Medications
Herbal medications, used frequently, may have effects that could be deleterious in the perioperative period, including clotting abnormalities and interactions with anesthetics. Clinicians should specifically inquire about herbal medication use in presurgical patients, as patients often do not readily disclose use.
A review that examined eight commonly used herbal remedies found the following:
- Ephedra (ma huang) may increase the risk of heart attack and stroke and should be discontinued at least 24 hours prior to surgery.
- Garlic may increase bleeding risk and should be discontinued at least seven days prior to surgery.
- Ginkgo may increase bleeding risk and should be discontinued at least 36 hours prior to surgery.
- Ginseng lowers blood sugar and may increase bleeding risk and should be discontinued at least seven days prior to surgery.
- Kava may increase the sedative effect of anesthetics and should be discontinued at least 24 hours prior to surgery. An association between kava use and fatal hepatotoxicity has been reported.
- St. John’s wort may diminish the effects of several drugs by induction of cytochrome P450 enzymes and should be discontinued at least five days prior to surgery.
- Valerian may increase the sedative effect of anesthetics and is associated with benzodiazepine-like withdrawal. There are no data on preoperative discontinuation. Ideally it is tapered weeks before surgery; if not, withdrawal is treated with benzodiazepines.
- Echinacea is associated with allergic reactions and immune stimulation. There are no data on preoperative discontinuation.
There is no evidence that herbal medications improve surgical outcomes, and there are theoretic reasons that these agents may increase perioperative morbidity. For simplicity and because the purity and nature of some herbal medications is unclear, we recommend stopping herbal agents at least one week before surgery.
Conclusions
Anesthesiologists must often decide if chronic medications should be continued in the perioperative period, although there are few outcome data about most medications. The following general principles inform the perioperative management of chronic medications:
- A complete medication history (including all over-the-counter and herbal/complementary medications) should be obtained, and all clinicians involved in patient management should review the medication history.
- Medications associated with known morbidity if withdrawn abruptly should be continued or tapered if feasible. Intravenous, transdermal, or transmucosal medicines should be substituted when absorption will be impaired because of loss of gastrointestinal function or restrictions on oral intake. Medications thought to increase the risk of anesthetic or surgical complications and not essential for the short term should be held through the perioperative period.
- The many medications administered perioperatively during a relatively short period increase the potential for drug-drug interactions.
- The metabolism and elimination of medications and their metabolites may be altered during the perioperative period.
- The majority of medications can be resumed once the patient is able to tolerate oral intake, with the exception of medications that impact the bleeding or thromboembolic risk.
Specific recommendations by medication category/class are reviewed in tables 1-8 and in text above.
References
1. Kennedy JM, van Rij AM, Spears GF, Pettigrew RA, Tucker IG. Polypharmacy in a general surgical unit and consequences of drug withdrawal. Br J Clin Pharmacol 2000; 49:353-362. Doi:10.1046/j.1365-2125.2000.00145.x
2. Kroenke K, Gooby-Toedt D, Jackson JL. Chronic medications in the perioperative period. South Med J 1998;91:358-364. Doi:10.1097/00007611-199804000-00009.
3. Spell NO 3rd. Stopping and restarting medications in the perioperative period. Med Clin North Am. 2001 Sep;85(5):1117-1128. Doi:10.1016/s0025-7125(05)70367-9.
4. Smith MS, Muir H, Hall R. Perioperative management of drug therapy, clinical considerations. Drugs 1996;Feb;51(2):238-59. Doi:10.2165/00003495-199651020-00005.
5. Clay BJ, Halasyamani L, Stucky ER, Greenwald JL, Williams MV. Results of a medication reconciliation survey from the 2006 Society of Hospital Medicine national meeting. J Hosp Med 2008; 3:465-472. PMID: 19084896 DOI: 10.1002/jhm.370
6. Marcucci M, Painter TW, Conen D, et al. Hypotension-Avoidance Versus Hypertension-Avoidance Strategies in Noncardiac Surgery: An International Randomized Controlled Trial. Ann Intern Med.2023 May;176(5):605-614. Doi:10.7326/M22-3157
7. Shammash JB, Trost JC, Gold JM, Sessler DI, Chan MTV, Borges FK, et al. Perioperative beta-blocker withdrawal and mortality in vascular surgical patients. Am Heart J 2001; 141:148.
8. Wallace AW, Au S, Cason BA. Association of the pattern of use of perioperative β-blockade and postoperative mortality. Anesthesiology 2010; 113:794-805. Doi:10.1097/ALN.0b013e3181f1c061.
9. Kertai MD, Cooter M, Pollard RJ, Buhrman W, Aronson S, Mathew JP, et al. Is Compliance with Surgical Care Improvement Project Cardiac (SCIP-Card-2) Measures for Perioperative β-Blockers Associated With Reduced Incidence of Mortality and Cardiovascular-Related Critical Quality Indicators After Noncardiac Surgery? Anesth Analg 2018; 126:1829-1838. Doi:10.1213/ANE.0000000000002577.
10. American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines, American Society of Echocardiography, American Society of Nuclear Cardiology, et al. 2009 ACCF/AHA focused update on perioperative beta blockade. J Am Coll Cardiol 2009; 54:2102-2128. DOI:10.1016/j.jacc.2009.07.004.
11. Hoffman BB. Therapy of hypertension. In: Goodman and Gilman’s The Pharmacological Basis of Therapeutics, 11th ed, Brunton LB, Lazo JS, Parker KL (Eds), McGraw-Hill, New York 2006.
12. Stühmeier KD, Mainzer B, Cierpka J, Cierpka J, Sandman W, Tarnow J. Small, oral dose of clonidine reduces the incidence of intraoperative myocardial ischemia in patients having vascular surgery. Anesthesiology 1996; 85:706-712 Doi:10.1097/00000542-199610000-00004.
13. Oliver MF, Goldman L, Julian DG, Holme I. Effect of mivazerol on perioperative cardiac complications during non-cardiac surgery in patients with coronary heart disease: the European Mivazerol Trial (EMIT). Anesthesiology 1999; 91:951-961. Doi:10.1097/00000542-199910000-00014.
14. Wallace AW, Galindez D, Salahieh A, Layug EL, Lazo EA, Haratonik KA, et al. Effect of clonidine on cardiovascular morbidity and mortality after noncardiac surgery. Anesthesiology 2004; 101:284-293. DOI:10.1097/00000542-200408000-00007.
15. Devereaux PJ, Sessler DI, Leslie K, Kurz A, Mrkobrada M, Alonso-Coello P, et al. Clonidine in patients undergoing noncardiac surgery. N Engl J Med 2014; 370:1504-1513. Doi:10.1056/NEJMoa1401106. Epub 2014 Mar 31.
16. Garg AX, Kurz A, Sessler DI, Mrkobrada M, Parikh C, Mizera R, et al. Aspirin and clonidine in non-cardiac surgery: acute kidney injury substudy protocol of the Perioperative Ischaemic Evaluation (POISE) 2 randomised controlled trial. BMJ Open 2014; 4: e004886. Doi:10.1136/bmjopen-2014-004886.
17. Lilja M, Jounela AJ, Juustila H. Withdrawal syndromes and the cessation of antihypertensive therapy. Arch Intern Med 1982; 142:839-840. PMID:6122433.
18. Metz S, Klein C, Morton N. Rebound hypertension after discontinuation of transdermal clonidine therapy. Am J Med 1987; 82:17-19. Doi:10.1016/0002-9343(87)90371-8.
19. Colson P, Médioni P, Saussine M, Séguin JR, Cuchet D, Grolleau D, et al. Hemodynamic effect of calcium channel blockade during anesthesia for coronary artery surgery. J Cardiothorac Vasc Anesth 1992; 6:424-428. DOI:10.1016/1053-0770(92)90007-t.
20. Wijeysundera DN, Beattie WS, Rao V, Ivanov J, Karkouti K. Calcium antagonists are associated with reduced mortality after cardiac surgery: a propensity analysis. J Thorac Cardiovasc Surg 2004; 127:755-762. Doi:10.1016/s0022-5223(03)00695-0.
21. Wijeysundera DN, Beattie WS. Calcium channel blockers for reducing cardiac morbidity after noncardiac surgery: a meta-analysis. Anesth Analg 2003; 97:634-641. Doi:10.1213/01.ane.0000081732.51871.D2
22. Reves JG, Kissin I, Lell WA, Tosone S. Calcium entry blockers: uses and implications for anesthesiologists. Anesthesiology 1982; 57:504-518. Doi:10.1097/00000542-198212000-00013.
23. Engelman RM, Hadji-Rousou I, Breyer RH, Whittredge P,Harbison W,R V Chircop. Rebound vasospasm after coronary revascularization in association with calcium antagonist withdrawal. Ann Thorac Surg 1984; 37:469-472. Doi:10.1016/s0003-4975(10)61133-2.
24. Kizer JR, Kimmel SE. Epidemiologic review of the calcium channel blocker drugs. An up-to-date perspective on the proposed hazards. Arch Intern Med 2001; 161:1145-1158. Doi:10.1001/archinte.161.9.1145.
25. Legault C, Furberg CD, Wagenknecht LE, Rogers AT, Stump DA, Coker L, et al. Nimodipine neuroprotection in cardiac valve replacement: report of an early terminated trial. Stroke 1996; 27:593-598. Doi:10.1161/01.str.27.4.593.
26. Zuccalá G, Pahor M, Landi F, Gasparini G, Pagano F, Carbonin P, et al. Use of calcium antagonists and need for perioperative transfusion in older patients with hip fracture: observational study. BMJ 1997; 314:643-644. Doi:10.1136/bmj.314.7081.643.
27. No authors listed. Effects of calcium antagonists on the risks of coronary heart disease, cancer and bleeding. Ad Hoc Subcommittee of the Liaison Committee of the World Health Organisation and the International Society of Hypertension. J Hypertens 1997; 15:105-115. PMID:9469785.
28. Grodecki-DeFranco P, Steinhubl S, Taylor P, et al. Calcium antagonist use and perioperative bleeding complications: an analysis of 5,157 patients. Circulation 1996; 94(suppl):I.
29. Finegan BA, Hussain MD, Tam YK. Pharmacokinetics of diltiazem in patients undergoing coronary artery bypass grafting. Ther Drug Monit 1992; 14:485-492. Doi:10.1097/00007691-199212000-00009.
30. Kheterpal S, Khodaparast O, Shanks A, Michael O’Reilly,Kevin K Tremper. Chronic angiotensin-converting enzyme inhibitor or angiotensin receptor blocker therapy combined with diuretic therapy is associated with increased episodes of hypotension in noncardiac surgery. J Cardiothorac Vasc Anesth 2008; 22:180-186. DOI:10.1053/j.jvca.2007.12.020.
31. Turan A, You J, Shiba A, Kurz A, Saager L, Sessler DI. Angiotensin converting enzyme inhibitors are not associated with respiratory complications or mortality after noncardiac surgery. Anesth Analg 2012; 114:552-560. doi:10.1213/ANE.0b013e318241f6af.
32. Shiffermiller JF, Monson BJ, Vokoun CW, Beachy MW, Smith MP, Sullivan JM, et al. Prospective Randomized Evaluation of Preoperative Angiotensin-Converting Enzyme Inhibition (PREOP-ACEI). J Hosp Med 2018; 13:661-667. Doi:10.12788/jhm.3036.
33. Hollmann C, Fernandes NL, Biccard BM. A Systematic Review of Outcomes Associated with Withholding or Continuing Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Before Noncardiac Surgery. Anesth Analg 2018; 127:678-687. Doi:10.1213/ANE.0000000000002837.
34. Roshanov PS, Rochwerg B, Patel A, Salehiam O, Duceppe E, Belley-Côté EP, et al. Withholding versus Continuing Angiotensin-converting Enzyme Inhibitors or Angiotensin II Receptor Blockers before Noncardiac Surgery: An Analysis of the Vascular events In noncardiac Surgery patIents cOhort evaluatioN Prospective Cohort. Anesthesiology 2017; 126:16-27. Doi:10.1097/ALN.0000000000001404.
35. Hirsch IA, Tomlinson DL, Slogoff S, Keats AS. The overstated risk of preoperative hypokalemia. Anesth Analg 1988; 67:131-136. PMID:3341565.
36. Nally BR, Dunbar SB, Zellinger M, Davis A. Supraventricular tachycardia after coronary artery bypass grafting surgery and fluid and electrolyte variables. Heart Lung 1996; 25:31-36. Doi:10.1016/s0147-9563(96)80009-4.
37. Khan NA, Campbell NR, Frost SD, Gilbert K, Michota FA, Usmani A, et al. Risk of intraoperative hypotension with loop diuretics: a randomized controlled trial. Am J Med 2010; 123:1059.e1. Doi:10.1016/j.amjmed.2010.07.019.
38. Farmer JA, Gotto AM. Dyslipidemia and the vulnerable plaque. Prog Cardiovasc Dis. 2002;44(6):415-428. Doi:10.1053/pcad.2002.123474.
39. Hollenberg M, Mangano DT, Browner WS, London MJ, Tubau JF, Tateo IM. Predictors of postoperative myocardial ischemia in patients undergoing noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA 1992; 268:205-209. PMID:1535109.
40. Polanczyk CA, Goldman L, Marcantonio ER, Orav EJ, Lee TH. Supraventricular arrhythmia in patients having noncardiac surgery: clinical correlates and effect on length of stay. Ann Intern Med 1998; 129:279-285. Doi:10.7326/0003-4819-129-4-199808150-00003.
41. Nishina K, Mikawa K, Takao Y, Shiga M, Maekawa N, Obara H. A comparison of rabeprazole, lansoprazole, and ranitidine for improving preoperative gastric fluid property in adults undergoing elective surgery. Anesth Analg 2000; 90:717-721. Doi:10.1097/00000539-200003000-00038.
42. Cruickshank RH, Morrison DA, Bamber PA, Nimmo WS. Effect of i.v. omeprazole on the pH and volume of gastric contents before surgery. Br J Anaesth 1989; 63:536-540. DOI:10.1093/bja/63.5.536.
43. Cantú TG, Korek JS. Central nervous system reactions to histamine-2 receptor blockers. Ann Intern Med 1991; 114:1027-1034. Doi:10.7326/0003-4819-114-12-1027.
44. Su FW, Beckman DB, Yarnold PA, Grammer LC. Low incidence of complications in asthmatic patients treated with preoperative corticosteroids. Allergy Asthma Proc 2004; 25:327-333. PMID:15603206.
45. Reiss TF, Chervinsky P, Dockhorn RJ, Shingo S, Seidenberg B, Edwards TB. Montelukast, a once-daily leukotriene receptor antagonist, in the treatment of chronic asthma: a multicenter, randomized, double-blind trial. Montelukast Clinical Research Study Group. Arch Intern Med 1998; 158:1213-1220. Doi:10.1001/archinte.158.11.1213.
46. Vandenbroucke JP, Rosing J, Bloemenkamp KW, Middeldorp S, Helmerhorst FM, Bouma BN, et al. Oral contraceptives and the risk of venous thrombosis. N Engl J Med 2001; 344:1527-1535. Doi:10.1056/NEJM200105173442007.
47. Grady D, Wenger NK, Herrington D, Khan S, Furberg C, Hunninghake D, et al. Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study. Ann Intern Med 2000; 132:689-696. Doi:10.7326/0003-4819-132-9-200005020-00002.
48. Miller J, Chan BK, Nelson HD. Postmenopausal estrogen replacement and risk for venous thromboembolism: a systematic review and meta-analysis for the U.S. Preventive Services Task Force. Ann Intern Med 2002; 136:680-690. DOI:10.7326/0003-4819-136-9-200205070-00011.
49. Hurbanek JG, Jaffer AK, Morra N, Karafa M, Brotman DJ. Postmenopausal hormone replacement and venous thromboembolism following hip and knee arthroplasty. Thromb Haemost 2004; 92:337-343. Doi:10.1160/TH04-03-0165.
50. Canonico M, Oger E, Plu-Bureau G, Conard J, Meyer G, Lévesque H, et al. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation 2007; 115:840-845. Doi:10.1161/circulationaha.106.642280.
51. Renoux C, Dell’Aniello S, Suissa S. Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. J Thromb Haemost 2010; 8:979-986. Doi:10.1111/j.1538-7836.2010.03839.x.
52. Canonico M, Fournier A, Carcaillon L, OliÉ V, Plu-Bureau G, Oger E, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol 2010; 30:340-345. Doi:10.1161/ATVBAHA.109.196022.
53. Cummings SR, Eckert S, Krueger KA, Grady D, Powles TJ, Cauley JA, et al. The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. Multiple Outcomes of Raloxifene Evaluation. JAMA 1999; 281:2189-2197. Doi:10.1001/jama.281.23.2189.
54. Fisher B, Costantino JP, Wickerham DL, Redmond CK, Kavanah M, Cronin WM et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst 1998; 90:1371-1388. Doi:10.1093/jnci/90.18.1371.
55. American Association of Oral and Maxillofacial Surgeons.Position paper: Medication-related osteonecrosis of the jaw – 2014 update http://www.aaoms.org/docs/position_papers/mronj_position_paper.pdf?pdf=MRONJ-Position-Paper (Accessed on October 01, 2024).
56. Borthwick E, Ferguson A. Perioperative acute kidney injury: risk factors, recognition, management, and outcomes. BMJ 2010; 341:c3365. Doi:10.1136/bmj.c3365.
57. Huyse FJ, Touw DJ, van Schijndel RS, de Lange JJ, Slaets JPJ. Psychotropic drugs and the perioperative period: a proposal for a guideline in elective surgery. Psychosomatics 2006; 47:8-22. Doi:10.1176/appi.psy.47.1.8.
58. Depaulo JR, Barker LR. Affective disorders. In: Principles of Ambulatory Medicine, Barker LR, Burton JR, Zieve PD (Eds), Williams and Wilkins, Baltimore 1995. p.166.
59. Labos C, Dasgupta K, Nedjar H, Turecki G, Rahme E. Risk of bleeding associated with combined use of selective serotonin reuptake inhibitors and antiplatelet therapy following acute myocardial infarction. CMAJ 2011; 183:1835-1843. Doi:10.1503/cmaj.100912.
60. Ziegelstein RC, Meuchel J, Kim TJ, Latif M, Alvarez W, Dasgupta M, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med 2007; 120:525-530. Doi:10.1016/j.amjmed.2006.10.026.
61. Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GI bleeding: confusion or confounding? Am J Med 2006; 119:719-727. Doi:10.1016/j.amjmed.2005.11.006.
62. Tully PJ, Cardinal T, Bennetts JS, Baker RA. Selective serotonin reuptake inhibitors, venlafaxine and duloxetine are associated with in hospital morbidity but not bleeding or late mortality after coronary artery bypass graft surgery. Heart Lung Circ 2012; 21:206-214. Doi:10.1016/j.hlc.2011.12.002.
63. Mason PJ, Morris VA, Balcezak TJ. Serotonin syndrome. Presentation of 2 cases and review of the literature. Medicine (Baltimore) 2000; 79:201-209. Doi:10.1097/00005792-200007000-00001.
64. Stack CG, Rogers P, Linter SP. Monoamine oxidase inhibitors and anaesthesia. A review. Br J Anaesth 1988; 60:222-227. Doi:10.1093/bja/60.2.222.
65. Ray WA, Chung CP, Murray KT, Hall K, Stein CM. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med 2009; 360:225-235. Doi:10.1056/NEJMoa0806994.
66. Ward N, Roth JS, Lester CC, Mutiso L, Lommel KM, Davenport DL. Anxiolytic medication is an independent risk factor for 30-day morbidity or mortality after surgery. Surgery 2015; 158:420-427. Doi:10.1016/j.surg.2015.03.050.
67. Lenhardt R, Orhan-Sungur M, Komatsu R, Govinda R, Kasuya Y, Sessler DI, et al. Suppression of shivering during hypothermia using a novel drug combination in healthy volunteers. Anesthesiology 2009; 111:110-115. Doi:10.1097/ALN.0b013e3181a979a3.
68. Fischer SP, Schmiesing CA, Guta CG, Brock-Utne JG. General anesthesia and chronic amphetamine use: should the drug be stopped preoperatively? Anesth Analg 2006; 103:203-206. Doi:10.1213/01.ane.0000221451.24482.11.
69. Kohan L, Potru S, Barreveld AM, Sprintz M, Lane O, Aryal A, et al. Buprenorphine management in the perioperative period: educational review and recommendations from a multisociety expert panel. Reg Anesth Pain Med 2021; 46:840-859. Doi:10.1136/rapm-2021-103007.
70. Bentzley BS, Barth KS, Back SE, Book SW. Discontinuation of buprenorphine maintenance therapy: perspectives and outcomes. J Subst Abuse Treat 2015; 52:48-57. Doi:10.1016/j.jsat.2014.12.011.
71. Pharmacology of Opiod Analgesics. In: Anesthesiology, Longnecker DE (Ed), McGraw-Hill, New York 2012.
72. Huxtable CA, Roberts LJ, Somogyi AA, MacIntyre PE. Acute pain management in opioid-tolerant patients: a growing challenge. Anaesth Intensive Care 2011; 39:804-823. Doi:10.1177/0310057X1103900505.
73. Rosandich PA, Kelley 3rd JT, Doyt LC. Perioperative management of patients with rheumatoid arthritis in the era of biologic response modifiers. Curr Opin Rheumatol 2004;16-192-198. Doi:10.1097/00002281-200405000-00005.
74. Goodman SM, Springer BD, Chen AF, Davis M, Fernandez DR, Figgie M et al. 2022 American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication in Patients With Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty. Arthritis Care Res (Hoboken) 2022; 74:1399-1408. Doi:10.1002/acr.24893.
75. George MD, Baker JF, Winthrop K, Alemao E, Chen L, Connolly S, et al. Risk of Biologics and Glucocorticoids in Patients with Rheumatoid Arthritis Undergoing Arthroplasty: A Cohort Study. Ann Intern Med 2019; 170:825-836. Doi:10.7326/M18-2217.
76. Jain A, Maini R, Nanchahal J. Disease modifying treatment and elective surgery in rheumatoid arthritis: the need for more data. Ann Rheum Dis 2004; 63:602-603. Doi:10.1136/ard.2003.017640.
77. Loza E, Martinez-Lopez JA, Carmona L. A systematic review on the optimum management of the use of methotrexate in rheumatoid arthritis patients in the perioperative period to minimize perioperative morbidity and maintain disease control. Clin Exp Rheumatol 2009; 27:856-862. PMID:19917174.
78. Mushtaq S, Goodman SM, Scanzello CR. Perioperative management of biologic agents used in treatment of rheumatoid arthritis. Am J Ther 2011; 18:426-434. Doi:10.1097/MJT.0b013e3181cb4042.
79. Goodman SM. Rheumatoid arthritis: Perioperative management of biologics and DMARDs. Semin Arthritis Rheum 2015; 44:627-632. Doi:10.1016/j.semarthrit.2015.01.008.
80. Merli GJ, Bell RD. Perioperative care of the surgical patient with neurologic disease. (Up To date Review). Up To Date 2024. http:www.uptodate.com. Accessed Sept 23, 2024.
81. Chang CC, Hu CJ, Lam F, Chang H, Liao CC, Chen TL. Postoperative adverse outcomes in surgical patients with epilepsy: a population-based study. Epilepsia 2012; 53:987-994. Doi:10.1111/j.1528-1167.2012.03448.x.
82. Kofke WA. Anesthetic management of the patient with epilepsy or prior seizures. Curr Opin Anaesthesiol 2010; 23:391-399. 10.1097/ACO.0b013e328339250b.
83. Newman JM, Sodhi N, Dalton SE, Khlopas A, Newman RP, Higuera CA, et al. Does Parkinson Disease Increase the Risk of Perioperative Complications After Total Hip Arthroplasty? A Nationwide Database Study. J Arthroplasty 2018; 33:S162-S166. Doi:10.1016/j.arth.2018.01.006.
84. Marchand KB, Vakharia R, Sodhi N, Anis H, Salem HS, Scuderi GR, et al. Impact of Parkinson’s Disease on Complications, Readmission Rates, and Costs of Care following Primary Total Knee Arthroplasty. J Knee Surg 2022; 35:21-25. Doi:10.1055/s-0040-1710546.
85. Abel M, Eisenkraft JB. Anesthetic implications of myasthenia gravis. Mt Sinai J Med 2002; 69:31-37. PMID:11832968.
86. Dempsey ZS, Rowell S, McRobert R. The role of regional and neuroaxial anesthesia in patients with systemic sclerosis. Local Reg Anesth 2011; 4:47-56. Doi:10.2147/LRA.S23808.
87. Chang DF, Osher RH, Wang L, Koch DD. Prospective multicenter evaluation of cataract surgery in patients taking tamsulosin (Flomax). Ophthalmology 2007; 114:957-964. Doi:10.1016/j.ophtha.2007.01.011.
88. Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin. J Cataract Refract Surg 2005; 31:664-673. Doi:10.1016/j.jcrs.2005.02.027.
89. Oshika T, Ohashi Y, Inamura M, Ohki K, Okamoto S, Koyama T, et al. Incidence of intraoperative floppy iris syndrome in patients on either systemic or topical alpha(1)-adrenoceptor antagonist. Am J Ophthalmol 2007; 143:150-151. Doi:10.1016/j.ajo.2006.07.046.
90. Bell CM, Hatch WV, Fischer HD, Cernat G, Paterson JM, Gruneir A, et al. Association between tamsulosin and serious ophthalmic adverse events in older men following cataract surgery. JAMA 2009; 301:1991-1996. Doi:10.1001/jama.2009.683.
91. Neff KD, Sandoval HP, Fernández de Castro LE, Nowacki AS, Vroman DT, Solomon KD. Factors associated with intraoperative floppy iris syndrome. Ophthalmology 2009; 116:658-663. Doi:10.1016/j.ophtha.2008.12.037.
92. Chatziralli IP, Sergentanis TN. Risk factors for intraoperative floppy iris syndrome: a meta-analysis. Ophthalmology 2011; 118:730-735. Doi:10.1016/j.ophtha.2010.08.039.
93. No authors listed. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). ALLHAT Collaborative Research Group. JAMA 2000; 283:1967-1975. PMID:10789664.
94. Libman H, Gandhi R, Bogorodskaya M. Surgical issues in HIV infection. (Up To date Review). Up To Date 2024. http:www.uptodate.com. Accessed Oct 1, 2024.
95. Kaye AD, Clarke RC, Sabar R, Vig S, Dhawan KP, Hofbauer R, et al. Herbal medicines: current trends in anesthesiology practice-a hospital survey. J Clin Anesth 2000; 12:468-471. Doi:10.1016/s0952-8180(00)00195-1.
96. Ang-Lee MK, Moss J, Yuan CS. Herbal medicines and perioperative care. JAMA 2001; 286:208-216. Doi:10.1001/jama.286.2.208.