






Clinical Features of Migraine in Mangalore: A Study
Clinical characteristics and disability of subjects with migraine in a tertiary Centre in Mangalore: A Cross-Sectional Study
Shubham Bhusari1, Deepthi Saka2, Rohit Pai3
- MBBS Student, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India.
- Senior Resident, Department of Psychiatry, Maharajah Institute of Medical Sciences, Vizianagaram, Andhra Pradesh, India.
- Associate Professor of Neurology, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Bhusari, S., Saka, D., et al., 2024. Clinical characteristics and disability of subjects with migraine in a tertiary Centre in Mangalore: A Cross-Sectional Study. Medical Research Archives, [online] 12(11).
https://doi.org/10.18103/mra.v12i11.6022
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i11.6022
ISSN 2375-1924
Introduction
Headache is the most common neurological disorder¹⁵ and is broadly classified into migraine headache and tension headache. Migraine is a primary headache characterized by a set of specific clinical features. It is the most common headache related neurological disability in the world¹. In terms of disability-adjusted life years (DALY)¹⁶, Migraine headache ranks second globally and has been considered as one among the ten most debilitating diseases globally¹⁵. The diagnosis of migraine is based on the criteria given by the second edition of the International Classification of Headache Disorders (ICHD-2)². It affects around 15% of women and 6% of men over 1 year period.¹ Owing to the inadequacy in diagnosis and treatment, there has been a rise in levels of disability leading to a poor quality of life³. It affects multiple domains of functioning including social, occupational, academic, personal, and particularly psychological domains. Particularly of note, migraine has been associated with a broad range of psychiatric comorbidities⁴. There has been a reported increase in the prevalence of migraine-related disability in patients who develop mood disorders due to migraine⁵. Considering the paucity in literature and limited work that has been done in migraine leading to mood disorders and other psychiatric comorbidities, leading to overall poor quality of life¹⁷.
Hence, the present study was conducted to study the clinical characteristics of migraine, identify and treat patients adequately to prevent the disability and correlate mood disorders¹³ in patients with migraine, and assess mood-related disability.
Materials and Methods:
The cross-sectional observation prospective clinical study was begun after getting approval from Institutional Ethics Committee of Father Muller Medical College, Mangalore, Karnataka, India and written informed consent from the study subjects. Subjects with migraine amongst those aged 14-64 years diagnosed with migraine based on ICHD were recruited by consecutive sampling at Neurology outpatient department of Father Muller Medical college and hospital, Mangalore, Karnataka during one month between March and April 2017.
Consecutive/Universal sampling method was adopted for the data collection, all the migraine patients visiting the Neurology outpatient department and satisfying the inclusion criteria during the study period were recruited for the study.
Data was collected based on questionnaire which had 3 sections. Section A includes identification data of the study participants. Section B focuses on collecting comprehensive socio-demographic information. This section includes details on age, gender, education level, current occupation, marital status, socio-economic status and assess some of its clinical features, namely duration, frequency, character, localization, type, severity, associated symptoms, family history, and questions related migraine disability assessment (MIDAS)⁷. The questionnaire was prepared after thorough review of literature of published articles.
Operational definition of migraine encompasses headache attacks lasting for 4-72 hours without treatment or failure of treatment which fulfills at least two of the following characteristics: moderate or severe pain intensity, aggravation by or avoidance of routine physical activity, unilateral headache, feelings of pulsation. During migraine, at least nausea and/or vomiting or photophobia and phonophobia is experienced.
SPSS Version 21.0 was used for entering and analyzing the data. Descriptive statistics like proportion, mean and standard deviation were used to express the results.
Results
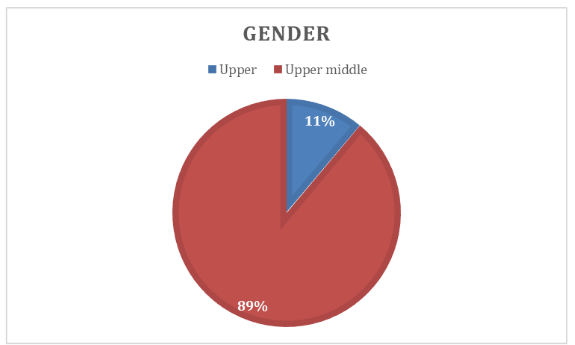
The study included 50 participants with a median age of 34.14 years (±12.22). The majority were female (37) as depicted in Figure 1.
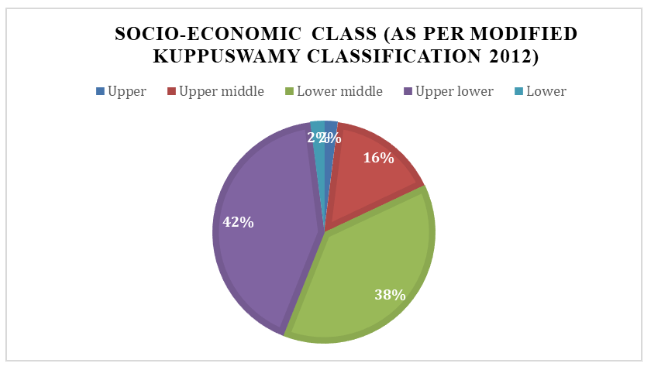
Among 50 subjects with migraine, a larger proportion belonged to lower socio-economic class, with 42% classified as class IV (6-10) as depicted in Figure 2.
Baseline Characteristics of Study Participants (N=50)
| Characteristic | Number | Percentage (%) |
|---|---|---|
| Education | 6 – middle school | 5 |
| 7 – primary school | 4 | |
| 8 – unskilled work | 6 | |
| 9 – skilled work | 4 | |
| 10 – professional | 2 | |
| Marital Status | Single | 13 |
| Married | 31 | |
| Residence | Urban | 29 |
Headache Characteristics
Out of 50 study participants 84% (n=42) of them reported having migraine without aura, 56% (n=28) had a family history of headaches as depicted in Table 3.
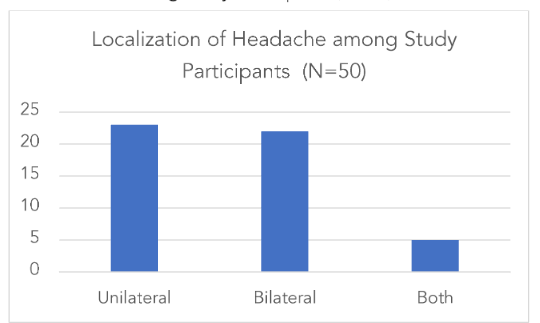
Among 50 subjects with migraine who had headache, 23 subjects (46%) had unilateral headache, 22 subjects (44%) reported bilateral headaches as depicted in Figure 4.
Figure 5: Presence of Associated Symptoms (N=50)
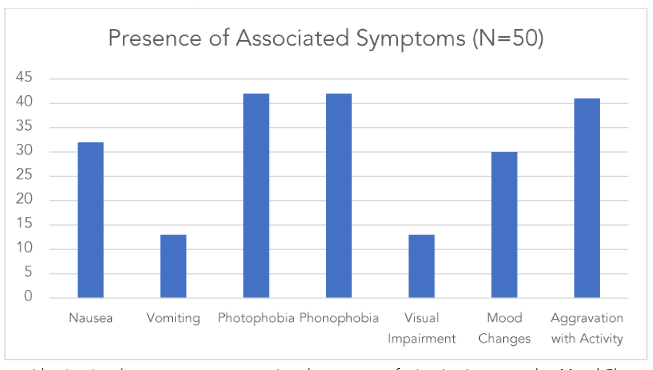
Presence of Associated Symptoms (N=50)
| Associated Symptoms | Number of Participants |
|---|---|
| Nausea | 42 |
| Vomiting | 28 |
| Photophobia | 30 |
| Visual impairment | 10 |
Disability associated with headache as per MIDAS score
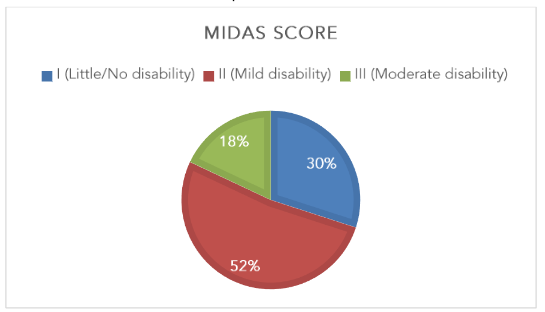
The study focused on the clinical characteristics of migraine, and the MIDAS score indicated that 52.0% (n=26) had MIDAS Grade I (little/no disability) and 14.0% (n=7) MIDAS Grade III (moderate disability) as depicted in Figure 5.
Statistical Correlation: Cross-Tabulation
Table 3: Cross-tabulation of Age at Onset of Headache and Family History of Headache
| Age at onset (in years) | Family History Present n (%) | Family History Absent n (%) | Total |
|---|---|---|---|
| 14 – 34 | 9 (26%) | 25 (74%) | 34 |
| 34 – 49 | 1 (7%) | 13 (93%) | 14 |
| 50 – 64 | 1 (50%) | 1 (50%) | 2 |
| Total | 11 (22%) | 39 (78%) | 50 |
There is no association between age at onset of headache and family history of headache (Chi Square Value: 1.1, p-value: 0.2943) as depicted in Table 3.
Table 4: Cross-tabulation of Gender of Subject with Migraine and Family History of Headache
| Gender | Family History Present n (%) | Family History Absent n (%) | Total |
|---|---|---|---|
| Male | 0 | 13 (100%) | 13 |
| Female | 11 (30%) | 26 (70%) | 37 |
| Total | 11 (22%) | 39 (78%) | 50 |
There is an association between gender of subjects with migraine and family history of headache (p<0.05, Chi Square Value: 4.955, p-value: 0.026) as depicted in Table 4.
Table 5: Cross-tabulation of Gender of Subject with Migraine and Age at Onset of Headache
| Gender | 14 – 34 n (%) | 35 – 49 n (%) | 50 – 64 n (%) | Total |
|---|---|---|---|---|
| Male | 7 (54%) | 4 (31%) | 2 (15%) | 13 |
| Female | 27 (73%) | 10 (27%) | 0 | 37 |
| Total | 34 (68%) | 14 (28%) | 2 (4%) | 50 |
There is an association between gender of subjects with migraine and age at onset of headache (p<0.05, Chi Square Value: 6.258, p-value: 0.044) as depicted in Table 5.
Table 6: Cross-tabulation of Duration of Attack (in hours) and Localization of Headache
| Duration of Headache (in hours) | U/L n (%) | B/L n (%) | Both n (%) | Total |
|---|---|---|---|---|
| < 6 | 5 (50%) | 4 (40%) | 1 (10%) | 10 |
| 6 – 24 | 9 (39%) | 12 (52%) | 2 (9%) | 23 |
| 24 – 72 | 7 (50%) | 6 (43%) | 1 (7%) | 14 |
| > 72 | 2 (66%) | 0 | 1 (33%) | 3 |
| Total | 23 (46%) | 22 (44%) | 5 (10%) | 50 |
There is no association between duration of attack in hours and localization of headache (p>0.05, Chi Square Value: 4.095, p-value: 0.664) as depicted in Table 6.
| Associated symptoms | MIDAS | Pearson chi-square value | P-value | |||
|---|---|---|---|---|---|---|
| I (Little/No disability) n (%) | II (Mild disability) n (%) | III (Moderate disability) n (%) | Total | |||
| Character | 10.487 | 0.106 | ||||
| Pulsating/throbbing | 11 (69%) | 9 (36%) | 5 (56%) | |||
| Sharp | 3 (19%) | 10 (40%) | 2 (22%) | |||
| Dull | 2 (12%) | 2 (8%) | 2 (22%) | |||
| Others | 0 | 4 (16%) | 0 | |||
| Total | 16 | 25 | 9 | 50 |
| Monthly Frequency (in days) | I n (%) | II n (%) | III n (%) | Total | Pearson chi-square value | P-value |
|---|---|---|---|---|---|---|
| 0–4 | 5 (31%) | 1 (4%) | 0 | 1.335 | 0.855 | |
| 5–9 | 3 (19%) | 13 (52%) | 0 | |||
| >10 | 8 (50%) | 11 (44%) | 9 (100%) | |||
| Total | 16 | 25 | 9 | 50 |
| Education | I n (%) | II n (%) | III n (%) | Total | Pearson chi-square value | P-value |
|---|---|---|---|---|---|---|
| Professional or Honors | 0 | 0 | 1 (11%) | 6.381 | 0.896 | |
| Graduate or Post graduate | 3 (19%) | 3 (12%) | 0 | |||
| Intermediate or post high school diploma | 2 (12.5%) | 4 (16%) | 1 (11%) | |||
| High school | 6 (37.5%) | 10 (40%) | 6 (67%) | |||
| Middle school | 1 (6%) | 3 (12%) | 1 (11%) | |||
| Primary school | 2 (12.5%) | 3 (12%) | 0 | |||
| Illiterate | 2 (12.5%) | 2 (8%) | 0 | |||
| Total | 16 | 25 | 9 | 50 |
| Gender | I n (%) | II n (%) | III n (%) | Total | Pearson chi-square value | P-value |
|---|---|---|---|---|---|---|
| Male | 4 (25%) | 8 (32%) | 1 (11%) | 0.601 | 0.740 | |
| Female | 12 (75%) | 17 (68%) | 8 (99%) | |||
| Total | 16 | 25 | 9 | 50 |
Discussion
Migraine is a wide spectrum of disease characterized by a variable number of episodes, associated with variable intensities of pain, causing implications in the migraine treatment.
The current study focused on the clinical characteristics of migraine, assessed the disability associated with migraine, and correlated clinical profile with the socio-demographic factors. The current study has a special focus on migraine-related disability associated with mood disorders affecting the health-related quality of life⁸, considering the inadequacy of diagnosis and treatment amongst migraine patients.
The findings of the current study which involved 50 subjects with migraine are in accordance with similar research specific to the disability and demographic parameters of patients with migraine. The current study shows a female preponderance of 74.0%. The Majority of about 52.0% belonged to the age group of 14-34. 42.0% belonged to the middle IVth socio-economic class, and 40% had attained atleast high school education. Demographic variables are in accordance with studies done by Renjith V10, Steiner TJ11, both studies emphasize on the significant burden of migraine as a disabling condition, however they focus on different populations. Study conducted by Renjith V10 in Karnataka, India, surveyed 60 patients, revealing a female preponderance (70%) and a mean age of 35.22 years. It documented high rates of associated symptoms such as throbbing pain (90%) and moderate to severe functional disability in 73.3% of participants. Conversely, study conducted by Steiner TJ11 estimated the one-year prevalence of migraine in England through a large sample (n = 4007), finding that 7.6% of males and 18.3% of females reported migraines, with a significant decline in prevalence after the age of 40. The study emphasized substantial productivity loss, averaging 5.7 working days lost per year for migraineurs, particularly among the most disabled individuals. Together, these studies underscore the pervasive impact of migraine across different demographics, emphasizing the need for targeted healthcare strategies to address this significant public health issue.
A family history of migraine was present in 78% of subjects. The family history of migraine is associated with a lower age-at-onset. The various symptoms experienced by patients include throbbing pain (50.0%), mood changes (60.0%), nausea (65.0%), photophobia (84.0%), and phonophobia (84.0%).
The duration and frequency of headaches were found to correlate with the presence of mood disorders in 60.0% of the patients. Moreover, a higher migraine-related disability was noted in patients with comorbid mood disorders.
Numerous studies have highlighted that individuals with migraines who also experience mood disorders tend to face a lower quality of life. This includes increased activity limitations, more frequent job absences, greater use of healthcare services, and a higher likelihood of needing assistance with personal or instrumental daily activities. These findings are consistent with the worse disability scores observed in our study.
Most of the subjects (52.0%) under the study belonged to mild levels of functional disability based on MIDAS. MIDAS questionnaire can be used as an effective clinical measure to identify the severity of illness and can be an inevitable tool in planning treatment for migraine.
We would like to acknowledge the limitations of our study. Firstly, the small and specific sample size restricts the generalizability of our findings to a broader population. Secondly, being a cross-sectional study, it does not allow the effect of medication on disability levels over time. Additionally, the relatively short duration of the study limits our ability to assess long-term outcomes and changes in disability. However, one of the primary strengths of our study is its prospective design, which allows for the observation and analysis of outcomes over time, reducing biases associated with retrospective studies. Additionally, the assessment was conducted using standard international criteria and standardized tools, ensuring that the measurements and evaluations were both reliable and valid. Another, strength of our study is that we have carefully excluded other causes of headache especially tension type and medication overuse headaches which could potentially change the clinical and psychological picture of the individuals or any subjects with acute illnesses.
Hence, we contend that this study provides a pure and undistorted picture of Clinical characteristics and disability of subjects with migraine along with a correlation amongst associated symptoms like mood changes with duration and frequency of headaches.
Conclusion
Migraine headache is a common neurological disorder¹⁴ affecting the younger female population leading to significant mood disorders with rising migraine-related disability. An early diagnosis and optimum treatment of these individuals can prevent these impairments and lead to a better quality of life in these individuals. Moreover, patients with migraine must be screened for mood disorders using questionnaires like the Hospital Anxiety and Depression Scale (HADS)⁹ to rule out comorbid mood disorders. A prospective longitudinal study, larger sample size, and effectiveness of treatment and quality of life with adequate treatment could be targets for future epidemiological and clinical studies on migraine.
Conflict of Interest:
There are no conflicts of interest.
Funding Statement:
None.
Acknowledgements:
The authors would like to express their sincere gratitude to Dr. Mithun, Assistant Professor, Department of Community Medicine, Kasturba Medical College, Mangalore for his support and guidance in thorough review of the manuscript. We also extend our thanks to the anonymous reviewers for their insightful comments, which significantly enhanced the quality of this article.
Corresponding Author:
Dr. Rohit Pai
Associate Professor of Neurology Kasturba Medical College
Mangalore, Karnataka, India.
Email Address: [email protected]
References
1. Peter J. Goadsby, Neil H. Raskin, Migraine and Other Primary Headache Disorders Harrison’s Principles Of Internal Medicine. 19th ed. New York: mcgraw-Hill, 2015.
2. Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004;24(1):1e160
3. Steiner TJ, Scher AI, Stewart WF, Kolodner K, Liberman J, Lipton RB. The prevalence and disability burden of adult migraine in England and their relationships to age, gender and ethnicity. Cephalalgia 2003;23(7):519e27
4. Mccracken HT, Thaxter LY, Smitherman TA. Psychiatric comorbidities of migraine. Handbook of clinical neurology. Published online January 1, 2024:505-516. Doi: https://doi.org/10.1016/b978-0-12-823357-3.00013-6
5. Rammohan K, Mundayadan SM, Das S, Shaji CV. Migraine and Mood Disorders: Prevalence, Clinical Correlations and Disability. Journal of Neurosciences in Rural Practice. 2019;10(01):28-33. Doi: https://doi.org/10.4103/jnrp.jnrp_146_18
6. Kumar N, Gupta N, Kishore J. Kuppuswamy’s socioeconomic scale: Updating income ranges for the year 2012.Indian J Public Health 2012;56:1034.
7. Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache related disability. Neurology 2001;56(6 Suppl. 1):S20e8.
8. Monzon MJ, Lainez MJ. Quality of life in migraine and chronic daily headache patients. Cephalalgia 1998;18(9):638e43.
9. Snaith RP. The Hospital Anxiety And Depression Scale. Health and Quality of Life Outcomes. 2003;1(1):29. Doi:https://doi.org/10.1186/1477-7525-1-29
10. Renjith V, Pai MS, Castelino F, Pai A, George A. Clinical profile and functional disability of patients with migraine. J Neurosci Rural Pract 2016;7:250
11. Steiner TJ, Scher AI, Stewart WF, Kolodner K, Liberman J, Lipton RB. The prevalence and disability burden of adult migraine in England and their relationships to age, gender and ethnicity. Cephalalgia 2003;23(7):519e27.
12. Stewart WF, Linet MS, Van Celentano DDNM, Ziegler D. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol 1991; 134: 1111–20.
13. Breslau N, Davis GC, Andreski P. Migraine, psychiatric disorders, and suicide attempts: an epidemiologic study of young adults. Psychiat Res 1991; 37: 11–23.
14. Chen, D., Willis-Parker, M., & Lundberg, G. P. (2019). Migraine headache: Is it only a neurological disorder? Links between migraine and cardiovascular disorders. Trends in Cardiovascular Medicine, 30(7), 424–430. https://doi.org/10.1016/j.tcm.2019.10.005
15. Ahmed, F. (2012). Headache disorders: differentiating and managing the common subtypes. British Journal of Pain, 6(3), 124–132. https://doi.org/10.1177/2049463712459691
16. Grosse, S. D., Lollar, D. J., Campbell, V. A., & Chamie, M. (2009). Disability and Disability-Adjusted Life Years: Not the Same. Public Health Reports, 124(2), 197–202. https://doi.org/10.1177/003335490912400206
17. Pistoia, F., Salfi, F., Saporito, G. et al. Behavioral and psychological factors in individuals with migraine without psychiatric comorbidities. J Headache Pain 23, 110 (2022). https://doi.org/10.1186/s10194-022-01485-x