






Salt Taste Perception and Blood Pressure Screening Insights
Evaluation of Salt Taste Perception Threshold as an Additional Screening Tool across a Spectrum of Blood Pressure Levels
Ms. Hiranya S. Deore¹, Dr. Vidya Ganji², Dr. Madhuri Taranikanti³, Dr. Nitin Ashok John⁴, Dr. Kalpana M³, Dr. Madhusudhan U², Dr. Archana Gaur²*
- MBBS Final Year Student, All India Institute of Medical Sciences, Bibinagar.
- Associate Professor, Physiology, All India Institute of Medical Sciences, Bibinagar.
- Additional Professor, Physiology, All India Institute of Medical Sciences, Bibinagar.
- Professor, Physiology, All India Institute of Medical Sciences, Bibinagar.
OPEN ACCESS
PUBLISHED 30 November 2024
CITATION Deore, HS., Ganji, V., et al., 2024. Evaluation of Salt Taste Perception Threshold as an Additional Screening Tool across a Spectrum of Blood Pressure levels. Medical Research Archives, [online] 12(11).
https://doi.org/10.18103/mra.v12i11.5941
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5941
ISSN 2375-1924
ABSTRACT
Hypertension is one of the most common multi-factorial conditions with largest contribution to cardiovascular diseases. The development of hypertension is secondary to complex interaction between genetic, environmental and lifestyle factors. It is undisputed that hypertension is one of the important and independent risk factors for cardiovascular disease, stroke, peripheral arterial disease. Despite efforts of public health education, awareness on hypertension and their control remains problematic with only third of adults and elderly population aware of their hypertension status. The study aimed to evaluate a predictable burden of hypertension and identify salt taste perception threshold (SPT) as an additional screening tool for hypertension. The study results indicated that the salt taste perception threshold was significantly higher in hypertensive individuals when compared to normotensive individuals. The findings suggest that SPT can be used as an additional screening tool.
Keywords
- Hypertension
- Salt Taste Perception
- Screening Tool
- Blood Pressure
Introduction
Hypertension is one of the major multifactorial conditions having significant burden on healthcare system in India. In 2016, 1.63 million deaths were attributed to hypertension(1). It is undisputable that hypertension is one of the important and independent risk factors for cardiovascular disease, stroke, peripheral arterial disease(2). Despite efforts of public health education, awareness on hypertension and diet control remains problematic with only two-thirds of adult and elderly population aware of their hypertension status(3). Improved awareness and detection of hypertension would reduce a preventable burden of cardiac diseases related to hypertension. The development of elevated blood pressure and hypertension is secondary to complex interaction between environmental factors like high dietary salt intake, obesity and genes. Salt is the main source of sodium in our diet which is added primarily for palatability taste preferences and for preservation and processing of food. Processed food comprises 75% of salt intake. A small amount of sodium (500mg) is required to conduct nerve impulses, contraction and relaxation of muscles and maintenance of proper electrolyte balance. However, most people take more sodium than is needed. Salt consumption varies in different countries and an average Indian consumes 9 to 12 gm of salt per day which is almost double the amount of salt recommended by WHO (5 gm/day per adult)(4,5). Excessive salt intake >5g/day has shown a significant increase in blood pressure and has been linked with onset of hypertension(6). The role of genetic and environmental factors on sodium consumption and consequently the relationship between hypertension and salt intake is widely supported by individual and population-based studies(7,8).
Elevated blood pressure (a new BP category) defined as systolic BP of 120-139 mmHg or diastolic BP of 70-89 mmHg is an early condition that can develop into hypertension. The risk of cardiovascular diseases including atherosclerosis is higher in individuals with elevated blood pressure(9). The high sodium intake and increase in blood pressure may lead to water retention, increase in systemic peripheral resistance, alterations in endothelial function and modification in cardiovascular system. JNC7 recommendations for lowering blood pressure include reduced sodium intake to no more than 100mmol/day (2.4 g of sodium or 6 g of sodium chloride)(10). A meta-analysis showed that modest reduction in salt intake from 10 gm to 5 gm/day for 4 or more weeks would reduce the blood pressure in both hypertensive and normotensive individuals irrespective of sex and ethnicity(11). Hence, limited intake of salt plays an important role in dietary guidelines for prevention and proper management of hypertension which would contribute to substantial decline in mortality from cardiovascular diseases(12,13).
Salt sensitivity of blood pressure in which BP changes >10% in response to change in salt consumption accounts to approx. 57% to 80% of essential hypertension. Salt perception threshold (SPT) refers to lowest concentration of sodium at which an individual is able to perceive the taste of salt. Recent evidence suggested that salt taste perception is related to total sodium intake(14) and some studies have suggested higher salt taste perception thresholds in hypertensives(15). The adoption of lifestyle interventions is limited in Indian population and large number of individuals with pre-hypertension progress to hypertension within few years. Although 24-hr urine collection method is considered as the gold standard for assessing salt intake, collecting urine over a whole day is laborious and inconvenient for the individuals involved. Thus, in the present study, we tried to evaluate the salt perception threshold which measures salt taste sensitivity of an individual and its relationship with dietary salt intake across a spectrum of blood pressure levels so that it can be used as an additional screening tool to take appropriate measures to decrease morbidity and mortality from cardiovascular disease.
OBJECTIVES: To evaluate the salt taste perception threshold in normotensives, individuals with elevated blood pressure and hypertensive individuals.
Methodology
STUDY DESIGN – CROSS-SECTIONAL STUDY:
The study was carried out at All India Institute of Medical Sciences (AIIMS), Bibinagar in Department of Physiology and General Medicine OPD between July 2023 and January 2024 after obtaining approval from Institute Ethical Committee (IEC. No. AIIMS/BBN/IEC/MAR/2023/267)
INCLUSION CRITERIA:
Men and women in the age group of 18–50 years from urban and rural areas of Bibinagar.
EXCLUSION CRITERIA:
Subjects with history of smoking, history of active drug or chronic alcohol use, patients with diabetes mellitus, pregnancy, impaired renal function tests, hyper-aldosteronism, those having blocked nose and other conditions that might alter salt taste perception were excluded.
Dietary intake in the subjects was assessed using a validated food frequency questionnaire (FFQ) (reporting the types and quantities of salt consumption in last 24 hr) based on recall, demography, other eating practices and family history of hypertension. Height and weight of the subjects were measured using a standard anthropometric scale and the body mass index was calculated as weight divided by height square (kg/m²). The blood pressure was measured using standard clinically validated mercury sphygmomanometers by a single examiner with the subject in relaxed sitting position after 5 minutes rest. The blood pressure was measured with the subject’s arm at level of the heart with the palm of the hand facing up and elbow slightly flexed (16). Three consecutive readings were made at 5 minutes interval and the average of last 2 BP measurements was used for classification of study participants into 3 groups based on blood pressure as per the 2024 guidelines by European Society of Cardiology (ESC) (17).
-
Group I (normotensives / controls): Individuals with SBP <120 mmHg and DBP <70 mmHg
-
Group II: Individuals with elevated blood pressure (SBP 120–139 mmHg and DBP 70–89 mmHg)
-
Group III (Hypertensives; HTN): Individuals with SBP ≥140 mmHg and DBP ≥90 mmHg.
For assessment of salt perception threshold (SPT), the subjects were warned not to smoke, eat, or brush their teeth over a period of at least 2 hrs prior to the test. The room temperature was kept at 26°C. The subject’s mouth was washed with distilled water before doing the test to remove any taste. Salt taste perception threshold was determined by commercially available salt impregnated taste strips with sodium chloride in closed bottles (Burkhart Odofin salt strips, MediSense, Germany) at 5 concentrations of 0 g/ml (labelled as M), 0.016 g/ml (labelled as L), 0.04 g/ml (labelled as K) and 0.1 g/ml (labelled as J), and 0.25 g/ml (labelled as I). The salt strips were placed and stored in closed containers in a dry environment at room temperature. The salt strip was held at the subject’s mouth for 3 sec and the subject was asked whether he or she experienced no taste or some taste or salt taste. Salt strips with increasing concentrations were applied until the subject recognized “salty taste” for 2 consecutive concentrations. The lowest concentration of salt which is detected by the subject is defined as the salt perception threshold (SPT). Based on the SPT, the individuals were identified as those with normal SPT (individuals who identified the salt taste with L and K strips as they had low (0.016 g/ml) to normal (0.04 g/ml) NaCl conc.), while individuals with high SPT were those who identified the salt taste with J and I strips which had high concentrations of NaCl (0.1 g/ml) and (0.25 g/ml).
The data was entered into excel sheet and the continuous variables were presented as mean values and standard deviations. The data of thresholds of salt perception were presented as median detection and recognition categories in each category. The data was analyzed using SPSS software version 23 and for comparison of means student’s t-test was used all the probability values for statistical tests. Analysis of variance was used to investigate association between SPT and mean blood pressure values. The P value <0.05 were regarded as statistically significant.
Results:
We analyzed the data of 400 individuals in the age group of 18–50 years who were included in the study. 67% (n=268) of the study participants were females and 33% were males (n=132). The subjects were divided into 3 groups based on the blood pressure levels:
-
Group I (n=120): controls / normotensives
-
Group II (n=120): individuals with elevated blood pressure
-
Group III (n=160): hypertensives
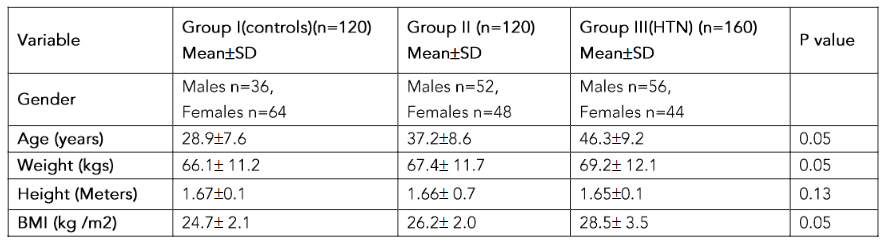
The details of mean age of the study participants are given in table 1. The number of males with elevated blood pressure (52%) (group II) and hypertension (group III) (56%) were more than the number of females in the corresponding groups but however we observed that the awareness of hypertension and importance of sodium restriction in diet was found in 54% of women when compared to 47% in men.
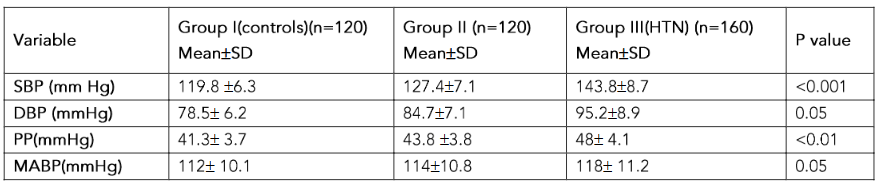
The mean BMI was significantly high in group II (26.2 ± 2.0) (elevated blood pressure) and higher in group III (28.5 ± 3.5) (HTN) individuals compared to controls (group I) (24.7 ± 2.14) (p<0.05). The mean values of systolic blood pressure (SBP) (p<0.001) and diastolic blood pressure (p<0.05) were significantly higher in group II and III individuals compared to group I individuals. There was significant increase in pulse pressure in group II and III (p<0.01).
The mean salt intake/day was significantly higher in males compared to females in the corresponding groups. The mean salt intake in group I males was 10.4 ± 1.9 g/day and 11.7 ± 2.1 g/day in group II males and 13.4 ± 2.4 g/day in group III males while in females the mean salt intake was 7.8 ± 1.2 g/day (table 2).
It was observed that 77% of the group I (normotensives) individuals presented normal SPT as they identified the salty taste with salt strips labelled as L (conc. of NaCl 0.016 g/ml), K (conc of NaCl 0.04 g/ml) whereas rest of 23% presented high SPT as they identified the salty taste with salt strips labelled as J (conc. of NaCl 0.1 g/ml) and I (conc. of NaCl 0.25 g/ml). On the other hand, 64% of the group II individuals (elevated blood pressure) with high SPT and 36% presented with normal SPT. In addition, 71% of group III individuals (hypertensives) presented with high SPT and rest of 29% presented normal SPT (table 2).
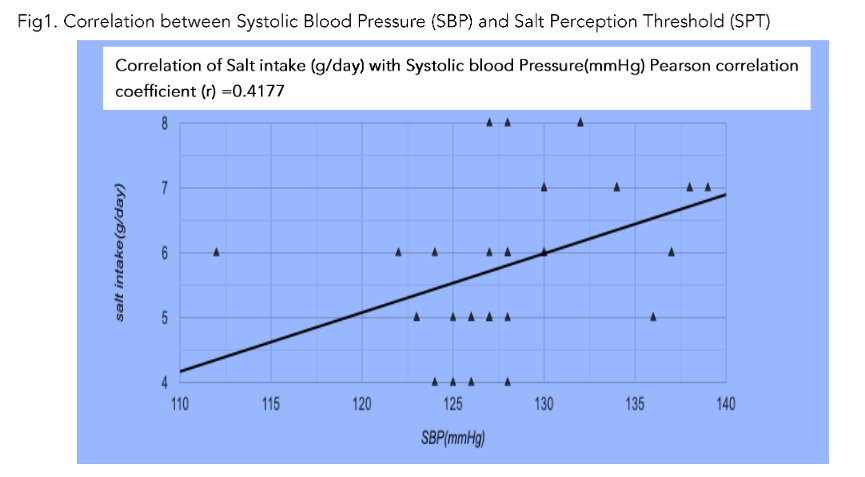
The salt intake of the individuals with high SPT was significantly higher (p<0.01). This shows that the mean salt intake/day is higher in individuals with elevated blood pressure and hypertension. The SPT were also higher significantly in individuals with elevated blood pressure and much higher in hypertensive subjects compared to normotensive subjects suggesting that an association existed between salt intake, salt taste perception and BP levels. It was observed that the SPT were higher in individuals with family history of hypertension. The BMI of the individuals with high SPT was also significantly higher (p<0.05) than that of the individuals with normal SPT. It was observed that systolic blood pressure values were high among individuals presented with high SPT.
There is a positive correlation between systemic systolic blood pressure and mean salt intake (Fig 1) (r = 0.77).
We analyzed the data of 400 individuals in the age group of 18-50 years who were included in the study. 67% (n=268) of the study participants were females and 33% were males (n=132). The subjects were divided into 3 groups based on the blood pressure levels: Group I (n=120): controls/normotensives; Group II (n=160): individuals with elevated blood pressure and Group III (n=120): hypertensives. The details of mean age of the study participants are given in table 1. The number of males with elevated blood pressure and hypertension are shown in table 1. The BMI was significantly higher in group III compared to group I (p<0.05) (Table 1).
We found that the salt intake/day and salt perception threshold (SPT) among groups I (controls), Group II (Elevated BP) and group III (hypertensive subjects) were significantly different (Table 2).
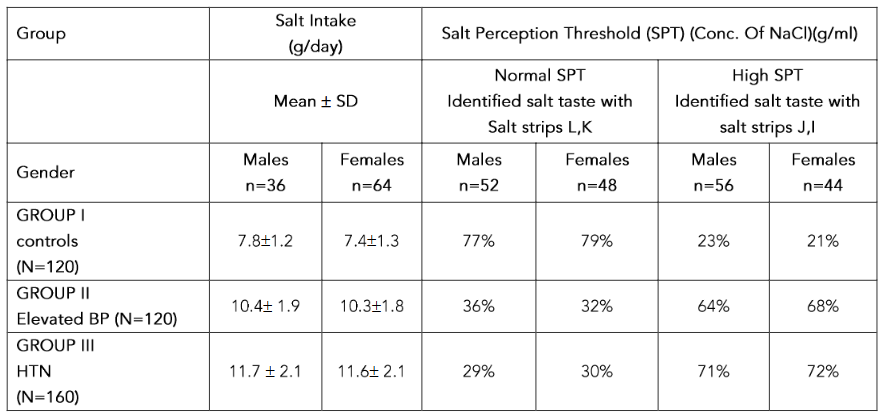 Table 2: Salt Intake/day and salt perception threshold (SPT) among groups
Table 2: Salt Intake/day and salt perception threshold (SPT) among groups
Discussion
Prevalence rates of hypertension are increasing over the last several decades among the young and elderly adults in India. In our study, we examined the gender differences in prevalence and awareness of elevated blood pressure and hypertension awareness in the study population and our results showed that the number of males with elevated blood pressure and hypertension are more than the number of females. However, the awareness on hypertension was lower in male subjects compared to women. Several other studies also have shown similar results that men younger than 65 years have higher risk of hypertension compared to women of the same age group(17,18). In contrast to this, females in a study conducted in Bangladesh demonstrated a higher prevalence and awareness of hypertension compared to males(17). Few studies have demonstrated a higher prevalence of hypertension in women by 6th decade of life compared to males(19,20). Our study shows that gender differences in hypertension are due to both biological and behavioral factors like sex hormones, chromosomal differences that are protective against hypertension in women(21). Behavioral risk factors like body mass index are found to be higher in men with elevated blood pressure compared to women leading to gender gap. These differences highlight the need for sex and region-specific health interventions through regular medical visits for improving awareness on hypertension and potentially preventable cardiac disability.
In our study, we observed high intake of salt among individuals with high SPT had high BMI. Some studies have shown a similar positive association between high salt intake and changes in body composition in Caucasian population(22). Few studies have shown that with ingestion of additional each 1 gm of salt, the chance of developing obesity is 26% regardless of ethnicity and energy intake(23).
The mean salt taste perception threshold was significantly lower in females than that of males of the same group. The salt perception threshold was found to be significantly high in individuals with elevated blood pressure and higher in hypertensive subjects when compared to normotensives. A high SPT suggests that the individual have low salt sensitivity and is more likely to have excessive salt intake to achieve nice tastes. High salt consumption will further decrease the sensitivity which would lead to more consumption of salt. Some studies have shown similar results with high salt perception threshold in hypertensive patients(24,25). In another study done on Indian adolescents, higher SPT and higher blood pressure values were observed in individuals with a family history of hypertension(26). There is genetic predisposition associated with salt taste perception and that certain populations are genetically more susceptible to development of hypertension(27). However, in contrast to this, some studies concluded that there was no difference in salt perception threshold among pregnant women or any higher sensitivity(28,29). In contrary, some people are salt sensitive and this salt sensitivity defines that the individual is more likely to have low salt intake. Studies and literature evaluating associations between salt perception threshold, salt intake and blood pressure are still scarce.
In correlation with the above hypothesis, we observed that the salt intake was higher by 2.6 g/day in individuals with elevated blood pressure and 3.9 g/day in hypertensive subjects when compared to controls. It was also observed that the salt intake was slightly higher in males compared to females of the same group. Several studies have concluded that with greater intakes of sodium, mean pressure is higher with age(30,31). High salt intake plays a crucial role in transition from elevated blood pressure to hypertension. Excessive sodium consumption >5 g/day (defined by WHO) has been shown to produce significant increase in BP and linked to onset of hypertension and its cardiovascular complications(4,11). Several studies indicate that Women are more salt sensitive than men are thereby at a higher risk of developing salt sensitive hypertension. The results of the INTERSALT study revealed a significantly higher
association of BP and sodium excretion in women than in men(32).
The mechanisms that link high salt intake and hypertension are:
-
Sodium and chloride being osmotically active, cause water retention leading to expansion of extracellular fluid volume, increase in cardiac output and rise in renal perfusion pressure leading to increased glomerular filteration rate and increased sodium excretion aiming to restore the fluid balance in the body called pressure natriuresis mechanism(31).
-
High salt intake can modulate the activity of autonomic nervous system, especially greater sympathetic nervous system activation.
-
Increase in systemic peripheral resistance as sodium triggers remodelling of small resistance arteries.
-
Endothelial dysfunction: high salt intake can cause marked reduction in endothelial nitric oxide which is responsible for endothelial dependent vascular dilatation. When the endothelium excretory ability of the kidneys is compromised, hypertension develops.
Reducing dietary salt intake in individuals with elevated blood pressure lowers the CVD event rates. The health benefits of salt reduction are mediated through BP lowering effects(33). A linear relationship has been described in a dose-response meta-analysis between sodium intake ranging from 0.4 to 0.7 g/day and reduction of systolic and diastolic blood pressure(34,35). It is recommended to restrict total dietary sodium intake of 5g/day including added salt. It needs to be emphasized that large parts of the daily sodium intake occurred in the subjects by means of sodium consumption contained in processed foods.
Conclusion:
This study shows that the mean salt intake/day was high in individuals with elevated blood pressures and higher in those with hypertension. An association existed between salt intake, salt perception threshold and blood pressure regardless of other risk factors. Hence, evaluation of the salt taste perception threshold would help in estimating the salt intake and can be used as an additional screening tool. The study results emphasize that reduction in salt consumption is recommended to prevent progression of those with elevated blood pressure to hypertension. Salt restriction in diet and awareness of hypertension should be a public health priority at community level to prevent the progression of individuals with elevated blood pressure to hypertension and prevent risk from cardiovascular diseases.
Competing interests:
The authors declare that they have no competing interests.
Funding:
The project was supported by AIIMS, Bibinagar under intramural STS -2023 project (Project no: AIIMS/BBN/Res/ IM-F/2022-23/S-04)
Acknowledgements:
Not Applicable.
Study design: Cross sectional study
In the present study, we tried to evaluate the salt perception threshold which measures salt taste sensitivity of an individual and its relationship with dietary salt intake across a spectrum of blood pressure levels.
Ethics approval and consent to participate:
This study was approved by Institutional Ethics Committee (IEC). (IEC. No. AIIMS/BBN/IEC/ MAR/2023/267) and written informed consent to participate was obtained from all the participants.
Availability of data and materials:
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Author’s contributions
All authors contributed to this work. HSD: data collection of blood pressure levels and determination of salt perception thresholds; NA: data analysis; correlation of blood pressure levels with SPT; KM: drafting and data collection; MU: data interpretation; MC: final manuscript revision.
Abbreviations
- HTN: Hypertension
- SPT: Salt Perception Threshold
- Pre-HTN: Pre-hypertension
- BMI: Body Mass Index
- DBP: Diastolic Blood Pressure
- SBP: Systolic Blood Pressure
- MABP: Mean Arterial Blood Pressure
References
1. Indian council of medical research, public health foundation of India and Indian institute for health metrics and evaluation. India: Health of the nation’s states- The India state-level disease and burden initiative. New Delhi, India. https://phfi.org/the-work/research/the-india-state-level-disease-burden-initiative/(2017).
2. Karmali KN, Ning H, Goff DC, Lloyd-jones DM. Identifying individuals at risk for cardiovascular events across the spectrum of blood pressure levels. J Am Heart Assoc 2015;4e002126.
3. Ostchega Y, Yoon SS, Hughes J, Louis T et al. hypertension awareness, treatment, and control -continued disparities in adults: United states,2005-2006. NCHS Data brief.2008;3: 1-8.
4. World health organization. Guideline: sodium intake for adults and children. World health organization; Geneva, Switzerland: 2012.
5. Johnson C. Santos JA, Sparks E, Raj TS et al. Sources of dietary salt in North and south India estimated from 24 hour dietary recall. Nutrients. 2019;11(2):318.
6. Gleiberman L. Blood pressure and dietary salt in human populations. Ecol Food Nutr.1973; 2(2): 143-156.
7. He FJ, Nirmala DM, Mc Gregor GA. Modest salt reduction lowers blood pressure in isolated systolic hypertension and combined hypertension: A meta-analysis of randomized trials. Implications for public health. Hypertension.2005; 44: 66-70.
8. Zhang H, Thijs L, Kuznetsova T, Fagard RH, Li X et al. Progression to hypertension in the non-hypertensive participants in the Flemish study on environment, genes and health outcomes. J Hypertens.2006;24(9):1719-27.
9. John William McEvoy, Cian P Mc Carthy, Rosa Maria Bruno, Sofie Brouwers et al. ESC Scientific document group,2024 ESC Guidelines for the management of elevated blood pressure and hypertension: developed by task force on the management of elevated blood pressure and hypertension of the European society of cardiology (ESC) and endorsed by the European society of endocrinology and European society stroke organisation(ESO), European heart journal,2024; 45(38):3912-4018.
10. World health organization. Salt reduction. https://www.who.int/news-room/fact-sheets/detail/salt-reduction.
11. Strazzullo P, D’Elia L, Kandala NB, Cappuccio FP. Salt intake, stroke and cardiovascular disease: meta-analysis of prospective studies. BMJ.2009; 339:b4567.
12. He FJ, Li J, Macgregor GA. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials.BMJ.2013;346:f1325.
13. Hayes JE, Sullivian BS, Duffy VB. Explaining variability in sodium intake through oral sensory phenotype, salt sensation and liking. Physiol Behav.2010; 100(4): 369-380.
14. Geleijnse JM, Kok FJ, Grobbee DE. Blood pressure response to changes in sodium and potassium intake: A meta regression analysis of randomized trials. J Human Hypertens. 2003; 17(7):471-480.
15. Michikawa T, Nishiwaki Y, Okamura T, Asakura K et al. The taste of salt measured by a simple test and blood pressure in Japanese women and men. Hypertens Res. 2009 May; 32(5):399-403. doi: 10.1038/hr.2009.31. E pub 2009 Apr 3. PMID: 19343036.
16. Stergiou GS, Alpert B, Mieke S, Asmar R et al. A universal standard for validation of blood pressure measuring devices: Association for the advancement of medical instrumentation /European Society of Hypertension /International organisation for Standardisation (AAMI/ESH/ISO) collaboration statement. J Hypertens.2018;36(3): 71:472-478.
17. Reckelhoff JF. Mechanisms of sex and gender differences in hypertension. J Hum Hypertens 2023; 37(8); 596-601.
18. Islam JY, Zaman MM, Ahmed JU, Chaudhury SR et al. Sex differences in prevalence and determinants of hypertension among adults: A cross-sectional survey of one rural village in Bangladesh. BMJ open.2020; 10(9) e 037546.
19. Ji H, Kim A, Ebinger JE, Niiranen TJ et al. Sex differences in blood pressure trajectories over the life course. JAMA cardiol.2020;5(3): 19-26.
20. Sandberg K, Ji H. Sex differences in primary hypertension. Biol Sex Differ. 2012;3(1):7.
21. Everett B, Zajacova A. Gender differences in hypertension and hypertension awareness among young adults. Biodemography Soc Biol.2015; 61(1): 1-17.
22. Larsen SC, Angquist L, Sorensen TI, Heitmann BL. 24 hr urinary sodium excretion and subsequent change in weight, waist circumference and body composition. PLos One. 2013;8(7):e69689.
23. Ma Y, He FJ, MacGregor GA. High salt intake: independent risk factor for obesity? Hypertension. 2015;66(4):843-9.
24. Antonello VS, Antonello IC, Santos CA. Salt taste threshold, 24 hr natriuresis and blood pressure variation in normotensive individuals. Rev Assoc Med Bras.2007;53 (2):142-6.
25. Martinelli J, Conde SR, Araujo AR, Marcadenti A. Association between salt taste sensitivity threshold and blood pressure in healthy individuals : A cross sectional study. Sao Paulo Med J.2020; 138(1):4-10.
26. Nikam LH. Salt taste threshold and its relation to blood pressure in normotensive offspring of hypertensive parents amongst Indian adolescents. Indian J Physiol Pharmacol.2015;59(1):34-40.
27. Pilic L, Mavrommatis Y. Genetic predisposition to salt-sensitive normotension and its effects on salt taste perception and intake. Br J Nutr.2018; 120(7):721-731.
28. Kim CY, Ye MK, Lee YS. The salt taste threshold in untreated hypertensive patients. Clin Hypertens.2017; 23: 22.
29. Kudo A, Kitamura A et al. Salt taste perception and blood pressures levels in population based samples: the circulatory risk in community study (CIRCS).Br J Nutr.2021. 125(2):203-211.
30. Schechter PJ, Horwitz D, Henkin RI. Salt preference in patients with untreated and treated essential hypertension. Am J Med Sci. 1974; 267 (6):320-6.
31. Grillo A, Salvi L, Coruzzi P, Salvi P, Parati G. Sodium intake and hypertension. Nutrients. 2019;11(9):1970.
32. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. Intersalt cooperative research group. BMJ.1988; 297(6644): 319-28.
33. Chung J, Lee S. Relationship between taste perception for salt and blood pressure in normotensives and hypertensive Korean adults: Curr Dev Nutr: 2019:3(1); 12-27.
34. Huang L, Trieu K, Yoshimura S, M Woodward, N Campbell, D Lackland et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials.BMJ 2020;368:M315.
35. Graudal NA, Hubeck-Graudal T, Jurgens G, Taylor RS. Dose response relation between dietary sodium and blood pressure: a meta-regression analysis of 133 randomised controlled trials. Am J Clin Nutr 2019;109(5):1273-1278.