






Utility of LSAS in Understanding Stuttering and Anxiety
Utility of the Liebowitz Social Anxiety Scale in Understanding Stuttering Issues
Yoshikazu Kikuchi¹, Gerald A Maguire²˒³, Daisuke Murakami¹, Yumi Yamaguchi¹, Takashi Nakagawa¹, and Toshiro Umezaki⁴˒⁵
- Department of Otorhinolaryngology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan.
- CenExel CIT Research, Riverside, California, USA.
- College Medical Center, Long Beach, California, USA.
- Voice and Swallowing Center, Fukuoka Sanno Hospital, Fukuoka, Japan.
- International University of Health and Welfare, Fukuoka, Japan.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Kikuchi, Y., Maguire, GA., et al., 2024. Utility of the Liebowitz Social Anxiety Scale in Understanding Stuttering Issues. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.5898
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5898
ISSN 2375-1924
ABSTRACT
Background: Stuttering is a speech fluency disorder that can significantly affect quality of life. Among adults who seek consultations for stuttering, 40–60% have comorbid social anxiety disorder (SAD). The Liebowitz Social Anxiety Scale (LSAS) has been developed to assess the severity of SAD, while the overall assessment of the speaker’s experience of stuttering for adults (OASES-A) questionnaire can measure the broader impact of stuttering. However, some medical professionals lack knowledge of such questionnaires.
Aims: Here, we aimed to investigate the correlation between the severity of stuttering and the OASES-A, and between the OASES-A and the LSAS.
Methods: Overall, 51 adults who stutter were included in this study. Stuttering frequency was assessed using a Japanese test, whereas the OASES-A questionnaire captured the comprehensive impact of stuttering on the participants’ lives. The LSAS was used to measure the severity of social anxiety. Pearson’s correlation analysis was used to determine the relationship between the variables.
Results: The average stuttering frequency was 10%, and the mean OASES-A total score was 2.86. The mean total LSAS score was 51.5. While no significant correlation was found between stuttering frequency and OASES-A total scores, a significant correlation was noted between LSAS and OASES-A total scores.
Conclusion: This study found that stuttering frequency did not correlate with the OASES-A. Notably, a novel moderate correlation was identified between OASES-A and LSAS total scores. The LSAS may help to evaluate the challenges faced by people who stutter when the OASES-A is unavailable.
Keywords
stuttering, childhood-onset fluency disorder, OASES, LSAS, social anxiety disorder.
INTRODUCTION
Stuttering is a speech fluency disorder and is referred to as a childhood-onset fluency disorder in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Many instances of stuttering in early childhood recover spontaneously. However, if stuttering persists until the age of 8, there is a high likelihood that it will continue into adolescence. Stuttering negatively impacts the quality of life (QOL), school attendance, social status, and wages, thereby emphasizing the need for support.
To assess stuttering, the English-speaking community uses the stuttering severity instrument 4th Edition, whereas the stuttering test method is used in Japan. However, the issue of people who stutter is likened to an “iceberg,” and addressing only the visible stutter is insufficient. Several questionnaires have been developed to understand the full scope of this problem. Notably, the overall assessment of the speaker’s experience of stuttering for adults (OASES-A) is popular among clinicians and researchers worldwide and has been adapted to languages such as Dutch, Brazilian Portuguese, Japanese, Hebrew, Swedish, Chinese, Polish, and Kannada, with standard data for the Australian population.
Among adults who seek consultations for stuttering, 40–60% experience comorbid social anxiety disorder (SAD). The co-occurrence of SAD and major depressive disorder is approximately 20%. When SAD is comorbid with depression, the suicide attempt rate increases to 7%. Therefore, comprehensive support from multiple professionals, including physicians, is necessary for adults who stutter. Physicians have long used the well-established Liebowitz Social Anxiety Scale (LSAS) to assess the severity of SAD; however, many physicians lack knowledge of questionnaires such as the OASES-A, which holistically assess the issues of those who stutter. Therefore, this study aimed to investigate whether the severity of stuttering correlates with the OASES-A, which measures the QOL of those who stutter. Subsequently, the correlation between the OASES-A and the LSAS, a medically established test for SAD, was examined.
METHODS
PARTICIPANTS
This study included 51 Japanese adults who stutter (43 males and 8 females). The average age was 26.3 years (range: 18–55 years). Nine participants had a history of psychiatric treatment, and none had participated in a stuttering self-help group.
STUTTERING FREQUENCY
Stuttering frequency was assessed using the Japanese Standardized Test for Stuttering and was calculated by dividing the number of core stuttering symptoms by the total number of utterances and multiplying the result by 100.
OVERALL ASSESSMENT OF THE SPEAKER’S EXPERIENCE OF STUTTERING
The OASES has been released in three different English versions as follows: the OASES-A, intended for adults (aged ≥18 years); the OASES-T, designed for teenagers (aged 13–17 years); and the OASES-S, tailored for school-age children (aged 7–12 years). The OASES-A comprises 100 items divided into four separate sections, each exploring different aspects of the stuttering condition. Section I, “General Information” (20 items), evaluates the overall perspective on stuttering, such as perceived fluency, the naturalness of spoken language, knowledge about stuttering, treatment options, and self-help groups. This section also includes an assessment of the speaker’s speaking ability and self-perception as a person who stutters. Section II, “Reactions to Stuttering” (30 items), evaluates the emotional, behavioral, and cognitive responses experienced by speakers resulting from stuttering. For instance, the items include questions on how frequently the speaker feels anxiety or frustration about stuttering, how often they experience physical tension during stuttering, and whether the speaker is worried about speaking or stuttering. Section III, “Communication in Everyday Situations” (25 items), assesses the difficulties the speaker faces when communicating in everyday settings, such as at home, at work, or in social contexts. Section IV, “QOL” (25 items), measures the negative impact of stuttering on an individual’s overall QOL by investigating factors, such as the speaker’s satisfaction with communication and whether stuttering interferes with their relationships with others. All items were rated on a 1–5 Likert scale, with higher scores indicating higher levels of adverse effects. The impact rating comprises the following five levels: mild (1.00–1.49), mild to moderate (1.50–2.24), moderate (2.25–2.99), moderate to severe (3.00–3.74), and severe (3.75–5.00).
LIEBOWITZ SOCIAL ANXIETY SCALE
The LSAS is a 24-item self-report questionnaire designed to measure social anxiety in various social interactions and performance situations that individuals with social phobia fear and avoid. The LSAS is categorized into the following two sections: one addressing social interaction situations (11 items) and the other addressing performance situations (13 items). Participants rated their level of fear over the past week using a 4-point Likert scale (0 = none, 1 = mild, 2 = moderate, and 3 = severe) and their level of avoidance (0 = never (0%), 1 = occasionally (10%), 2 = often (33–67%), and 3 = usually (67–100%). The responses for each scale were summed, resulting in a total LSAS score ranging from 0 to 144. Higher scores indicate more severe social anxiety. Additionally, six sub-scores were calculated as follows: Overall Fear, Performance Fear, Social Interaction Fear, Overall Avoidance, Performance Avoidance, and Social Interaction Avoidance. A Japanese version of the LSAS is available, and has shown high internal consistency, reliability, and convergent validity.
STATISTICAL ANALYSIS
We examined the relationships among the following three variables: stuttering frequency, OASES-A total score, and LSAS total score. Pearson’s product-moment correlation analysis was used to explore pairwise linear relationships among these variables. This method was selected because it offers a quantitative assessment of the association between any two of the three variables. The normality of the data was confirmed before correlation analysis. The specific analytical procedure was as follows: First, the values for stuttering frequency, OASES-A total scores, and LSAS total scores were input as a dataset. Subsequently, using JMP Pro 17 software (SAS Institute Inc., Cary, NC, USA), we chose the “Analyze > Multivariate Methods > Multivariate” option for the correlation analysis. The resulting correlation matrix displayed Pearson’s correlation coefficients, representing pairwise associations among the three variables. Bonferroni correction for multiple comparisons was performed, and the significance level was set at p<0.016. This study was approved by the Institutional Review Board of Kyushu University (2020-809) and conducted in compliance with the Declaration of Helsinki.
RESULTS
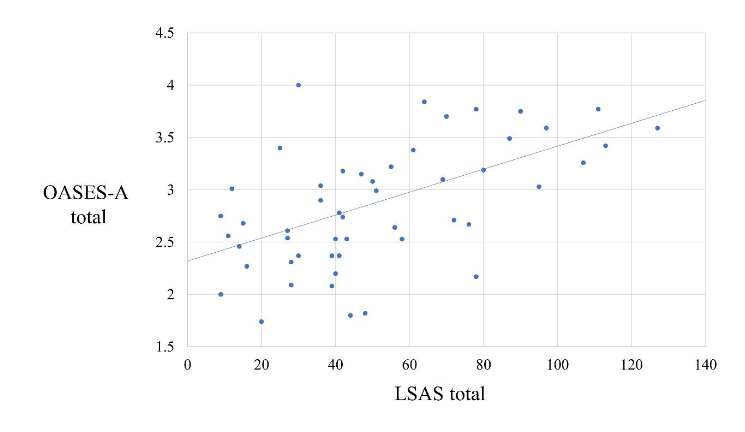
The average stuttering frequency (standard deviation) was 10% (1.1%). The mean total OASES-A score (standard deviation) was 2.86 (0.08). The average score (standard deviation) for the total LSAS was 51.5 (4.2). No statistically significant correlation was noted between stuttering frequency and total scores on either the OASES-A (r = -0.11, p = 0.46) or LSAS (r = 0.13, p = 0.41). The correlation between the total LSAS and OASES-A total scores was statistically significant (r = 0.56, p < 0.0001).
DISCUSSION
The results of this study indicate that the total OASES-A score did not correlate with the frequency of stuttering. This lack of correlation between stuttering frequency and the OASES-A aligns with other research findings, suggesting that stuttering frequency does not comprehensively represent the psychological and social impacts experienced by individuals who stutter. Even those with a low stuttering frequency might feel deeply affected by the fear and anxiety of stuttering and the restrictions it imposes on their daily lives.
Next, we confirmed that the OASES-A total score was moderately correlated with the total score on the social anxiety scale LSAS. Previous studies have shown correlations between the OASES-A and other social anxiety scales but not specifically with the LSAS. The correlation between the OASES-A and LSAS observed here is a novel finding of this study. The LSAS is a familiar index for healthcare professionals that is frequently used to assess the therapeutic effects of cognitive-behavioral therapy for SAD, and pharmacologic therapy. If adults who stutter visit a physician or clinical psychologist and the OASES-A is unavailable, the LSAS could serve as a substitute to help understand the challenges faced by people who stutter and monitor the effectiveness of treatment.
There is a growing need to develop evidence-based treatments for stuttering accompanied by SAD. Cognitive behavioral therapy has proven effective for SADs that co-occur in adults who stutter, with randomized controlled trials of this therapy being reported. Randomized controlled trials have been conducted on pharmacotherapy treatments for stuttering, including risperidone, olanzapine, and pagoclone. However, no Food and Drug Administration-approved medications are currently available for stuttering. Three Food and Drug Administration-approved medications are available for SAD as follows: venlafaxine, paroxetine, and sertraline. With the establishment of evidence-based treatments for SAD through cognitive-behavioral therapy and pharmacotherapy, physicians might play a vital role in the treatment of patients who stutter.
This study had some limitations. First, while the OASES-A offers a detailed analysis across four categories, the LSAS only assesses anxiety, fear in specific situations, and degree of avoidance. Although it can only assess a fraction of the speaking experiences of individuals who stutter, it may be useful in preventing the challenges faced by adults who stutter from being overlooked. Second, we did not verify the correlations based on sex. Females who stutter were one-quarter as common as males, and in this study, we had only eight females who stutter. Therefore, correlations were calculated for both sexes. Third, owing to the small number of participants with a history of psychiatric treatment, this factor was not used for differentiation, and the data were analyzed collectively. Two participants had a history of depression; however, the Beck Depression Inventory was not administered.
CONCLUSIONS
The LSAS showed a moderate correlation with the OASES, suggesting that in the absence of the OASES-A, the LSAS might be useful in evaluating the challenges faced by people who stutter.
CONFLICT OF INTEREST STATEMENT
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest. Dr. Maguire received a research grant and consulting fees from Noema; however, these were not utilized in this research study.
FUNDING
This work was supported by JSPS KAKENHI, Grant Numbers JP21KK0238, JP21K02688, and JP20K02299.
ACKNOWLEDGMENTS
We would like to thank Editage (www.editage.com) for the English language editing.
AUTHOR CONTRIBUTIONS
YK, DM, and YY contributed to the conception and design, investigation, data analysis, and interpretation and drafted the manuscript. GAM contributed to the conception and design, data curation, methodology, and critical revision of the manuscript. MS and MT contributed to the investigation and data curation. XY contributed to the investigation and critically revised the manuscript. TN and TU critically revised the manuscript. All authors contributed to the manuscript and approved the submitted version.
ETHICS STATEMENT
The studies involving human participants were reviewed and approved by the Institutional Review Board of Kyushu University. Informed consent was obtained from all participants.
DATA AVAILABILITY STATEMENT
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
REFERENCES
- Battle DE. Diagnostic and statistical manual of mental disorders (DSM). Codas. 2013;25(2):191-192. doi: 10.1590/s2317-17822013000200017.
- Ambrose NG, Cox NJ, Yairi E. The genetic basis of persistence and recovery in stuttering. J Speech Lang Hear Res. 1997;40(3):567-580. doi: 10.1044/jslhr.4003.567.
- Yairi E, Ambrose NG. Early childhood stuttering I: persistency and recovery rates. J Speech Lang Hear Res. 1999;42(5):1097-1112. doi: 10.1044/jslhr.4205.1097.
- Kefalianos E, Onslow M, Packman A, et al. The history of stuttering by 7 years of age: follow-up of a prospective community cohort. J Speech Lang Hear Res. 2017;60(10):2828-2839. doi:10.1044/2017_JSLHR-S-16-0205.
- Howell P, Davis S. Predicting persistence of and recovery from stuttering by the teenage years based on information gathered at age 8 years. J Dev Behav Pediatr. 2011;32(3):196-205. doi:10.1097/DBP.0b013e31820fd4a9.
- Craig A, Blumgart E, Tran Y. The impact of stuttering on the quality of life in adults who stutter. J Fluency Disord. 2009;34(2):61-71. doi:10.1016/j.jfludis.2009.05.002.
- Kikuchi Y, Kenjo M, Yoshida E, et al. Social anxiety disorder in adolescents who stutter: a risk for school refusal. Pediatr Int. 2023;65(1):e15622.
- McAllister J, Collier J, Shepstone L. The impact of adolescent stuttering on educational and employment outcomes: evidence from a birth cohort study. J Fluency Disord. 2012;37(2):106-21. doi:10.1016/j.jfludis.2012.01.002.
- Gerlach H, Totty E, Subramanian A, Zebrowski P. Stuttering and labor market outcomes in the United States. J Speech Lang Hear Res. 2018;61(7):1649-1663. doi: 10.1044/2018_JSLHR-S-17-0353.
- Riley G. Stuttering severity instrument. 4th ed. Austin, Tex.: Pro-Ed. 2009.
- Ozawa E, Hara Y, Suzuki N, Moriyama H, Ohashi Y, Kensaho K. Standardized test for stuttering. Gakuensha. 2013.
- Sheehan JG. Stuttering: research and therapy. New York: Harper & Row. 1970.
- Yaruss JS, Quesal RW. Overall assessment of the speaker’s experience of stuttering (OASES): documenting multiple outcomes in stuttering treatment. J Fluency Disord. 2006;31(2):90-115. doi:10.1016/j.jfludis.2006.02.002.
- Yaruss JS. Assessing quality of life in stuttering treatment outcomes research. J Fluency Disord. 2010;35(3):190-202. doi:10.1016/j.jfludis.2010.05.010.
- Ammons R, Johnson W. Studies in the psychology of stuttering: XVIII. The construction and application of a test of attitude toward stuttering. J Speech Disord. 1944;9:39-49. doi: 10.1044/jshd.0901.39.
- Andrews G, Cutler J. Stuttering therapy: the relation between changes in symptom level and attitudes. J Speech Hear Disord. 1974;39(3):312-319. doi: 10.1044/jshd.3903.312.
- Brutten G, Shoemaker D. Speech situation checklist. Carbondale, IL: Speech Clinic. Southern Illinois University. 1974.
- Crowe TA, Di Lollo A, Crowe BT. Crowe’s protocols: a comprehensive guide to stuttering assessment. San Antonio, Tex.: The Psychological Corporation. 2000.
- Erickson RL. Assessing communication attitudes among stutterers. J Speech Hear Res. 1969;12(4):711-724. doi: 10.1044/jshr.1204.711.
- Lanyon RI. The measurement of stuttering severity. J Speech Hear Res. 1967;10(4):836-843. doi:10.1044/jshr.1004.836.
- Ornstein AF, Manning WH. Self-efficacy scaling by adult stutterers. J Commun Disord. 1985;18(4):313-320. doi: 10.1016/0021-9924(85)90008-5.
- Riley J, Riley G, Maguire G. Subjective screening of stuttering severity, locus of control and avoidance: research edition. J Fluency Disord. 2004;29(1):51-62. doi: 10.1016/j.jfludis.2003.12.001.
- Watson JB. A comparison of stutterers’ and nonstutterers’ affective, cognitive, and behavioral self-reports. J Speech Hear Res. 1988;31(3):377-385. doi:10.1044/jshr.3103.377.
- Woolf G. The assessment of stuttering as struggle, avoidance, and expectancy. Br J Disord Commun. 1967;2(2):158-171. doi:10.3109/13682826709031315.
- Wright L, Ayre A. The Wright & Ayre Stuttering Self Rating Profile (WASSP). Bicester: Winslow Press. 2000.
- Koedoot C, Versteegh M, Yaruss JS. Psychometric evaluation of the Dutch translation of the overall assessment of the speaker’s experience of stuttering for adults (OASES-A-D). J Fluency Disord. 2011;36(3):222-230. doi:10.1016/j.jfludis.2011.03.002.
- Bragatto EL, Osborn E, Yaruss JS, Quesal R, Schiefer AM, Chiari BM. Brazilian version of the overall assessment of the speaker’s experience of stuttering – adults protocol (OASES-A). J Soc Bras Fonoaudiol. 2012;24(2):145-151. doi:10.1590/s2179-64912012000200010.
- Sakai N, Chu SY, Mori K, Yaruss JS. The Japanese version of the overall assessment of the speaker’s experience of stuttering for adults (OASES-A-J): translation and psychometric evaluation. J Fluency Disord. 2017;51:50-59. doi: 10.1016/j.jfludis.2016.11.002.
- Freud D, Kichin-Brin M, Ezrati-Vinacour R, Roziner I, Amir O. The relationship between the experience of stuttering and demographic characteristics of adults who stutter. J Fluency Disord. 2017;52:53-63. doi: 10.1016/j.jfludis.2017.03.008.
- Lindström E, Nilsson E, Nilsson J, et al. Swedish outcomes of the overall assessment of the speaker’s experience of stuttering in an international perspective. Logoped Phoniatr Vocol. 2020;45(4):181-189. doi:10.1080/14015439.2019.1695930.
- Ma Y, Oxley JD, Yaruss JS, Tetnowski JA. Stuttering experience of people in China: a cross-cultural perspective. J Fluency Disord. 2023;77:105994. doi: 10.1016/j.jfludis.2023.105994.
- Węsierska K, Yaruss JS, Kosacka K, Kowalczyk Ł, Boroń A. The experience of Polish individuals who stutter based on the OASES outcomes. J Fluency Disord. 2023;77:105991. doi:10.1016/j.jfludis.2023.105991.
- Mahesh S, Pushpavathi M, Seth D, Saravanan S, Yaruss JS. Adaptation and validation of overall assessment of the speaker’s experience of stuttering for adults in Kannada (OASES-A-K). Folia Phoniatr Logop. 2024;76(1):30-38. doi:10.1159/000531048.
- Blumgart E, Tran Y, Yaruss JS, Craig A. Australian normative data for the overall assessment of the speaker’s experience of stuttering. J Fluency Disord. 2012;37(2):83-90. doi:10.1016/j.jfludis.2011.12.002.
- Blumgart E, Tran Y, Craig A. Social anxiety disorder in adults who stutter. Depress Anxiety. 2010;27(7):687-692. doi: 10.1002/da.20657.
- Menzies RG, O’Brian S, Onslow M, Packman A, St Clare T, Block S. An experimental clinical trial of a cognitive-behavior therapy package for chronic stuttering. J Speech Lang Hear Res. 2008;51(6):1451-1464. doi: 10.1044/1092-4388(2008/07-0070).
- Stein MB, Baird A, Walker JR. Social phobia in adults with stuttering. Am J Psychiatry. 1996;153(2):278-280. doi: 10.1176/ajp.153.2.278.
- Ohayon MM, Schatzberg AF. Social phobia and depression: prevalence and comorbidity. J Psychosom Res. 2010;68(3):235-243. doi:10.1016/j.jpsychores.2009.07.018.
- Stein MB, Fuetsch M, Müller N, Höfler M, Lieb R, Wittchen HU. Social anxiety disorder and the risk of depression: a prospective community study of adolescents and young adults. Arch Gen Psychiatry. 2001;58(3):251-256. doi:10.1001/archpsyc.58.3.251.
- Costa D, Kroll R. Stuttering: an update for physicians. CMAJ. 2000;162(13):1849-1855.
- Kalinowski J, Saltuklaroglu T. The road to efficient and effective stuttering management: information for physicians. Curr Med Res Opin. 2004;20(4):509-515. doi:10.1185/030079904125003287.
- Liebowitz MR. Social phobia. Anxiety. Karger Publishers. 1987; 22:141-173.
- Asakura S, Inoue S, Sasaki F, et al. Reliability and validity of the Japanese version of the Liebowitz Social Anxiety Scale. Seishin-Igaku (Psychiatry). 2002;44:1077-1084.
- Fresco DM, Coles ME, Heimberg RG, et al. The Liebowitz Social Anxiety Scale: a comparison of the psychometric properties of self-report and clinician-administered formats. Psychol Med. 2001;31(6):1025-1035. doi:10.1017/s0033291701004056.
- Heimberg RG, Horner KJ, Juster HR, et al. Psychometric properties of the Liebowitz Social Anxiety Scale. Psychol Med 1999;29(1):199-212. doi: 10.1017/s0033291798007879.
- Masia-Warner C, Storch EA, Pincus DB, Klein RG, Heimberg RG, Liebowitz MR. The Liebowitz Social Anxiety Scale for children and adolescents: an initial psychometric investigation. J Am Acad Child Adolesc Psychiatry. 2003;42(9):1076-1084. doi:10.1097/01.CHI.0000070249.24125.89.
- Chu SY, Sakai N, Lee J, Harrison E, Tang KP, Mori K. Comparison of social anxiety between Japanese adults who stutter and non-stuttering controls. J Fluency Disord. 2020;65:105767. doi:10.1016/j.jfludis.2020.105767.
- Constantino CD, Leslie P, Quesal RW, Yaruss JS. A preliminary investigation of daily variability of stuttering in adults. J Commun Disord. 2016;60:39-50. doi: 10.1016/j.jcomdis.2016.02.001.
- Manning W, Gayle Beck J. The role of psychological processes in estimates of stuttering severity. J Fluency Disord. 2013;38(4):356-367. doi:10.1016/j.jfludis.2013.08.002.
- Sønsterud H, Howells K, Ward, D. Covert and overt stuttering: concepts and comparative findings. J Commun Disord. 2022;99:106246. doi:10.1016/j.jcomdis.2022.106246.
- Davidow JH, Scott KA. Intrajudge and interjudge reliability of the stuttering severity instrument-fourth edition. Am J Speech Lang Pathol. 2017;26(4):1105-1119. doi:10.1044/2017_AJSLP-16-0079.
- Bricker-Katz G, Lincoln M, McCabe P. A life-time of stuttering: how emotional reactions to stuttering impact activities and participation in older people. Disabil Rehabil. 2009;31(2):1742-1752. doi:10.1080/09638280902738672.
- Tichenor SE, Gerwin KL, Walsh B. Repetitive negative thinking in adolescents who stutter. J Speech Lang Hear Res. 2023;66(9):3290-3306. doi:10.1044/2023_JSLHR-23-00147.
- Scholten W, Seldenrijk A, Hoogendoorn A, et al. Baseline severity as a moderator of the waiting list-controlled association of cognitive behavioral therapy with symptom change in social anxiety disorder: a systematic review and individual patient data meta-analysis. JAMA Psychiatry. 2023;80(8):822-831. doi:10.1001/jamapsychiatry.2023.1291.
- Singh P, Samantaray NN. Brief cognitive behavioral group therapy and verbal-exposure-augmented cognitive behavioral therapy for social anxiety disorder in university students: a randomized controlled feasibility trial. Indian J Psychol Med. 2022;44(6):552-557. doi:10.1177/02537176211026250.
- Thew GR, Kwok APL, Lissillour Chan MH, et al. Internet-delivered cognitive therapy for social anxiety disorder in Hong Kong: a randomized controlled trial. Internet Interv. 2022;28:100539. doi:10.1016/j.invent.2022.100539.
- Mitsui N, Fujii Y, Asakura S, et al. Antidepressants for social anxiety disorder: a systematic review and meta-analysis. Neuropsychopharmacol Rep. 2022;42(4):398-409. doi: 10.1002/npr2.12275.
- Danforth AL, Grob CS, Struble C, et al. Reduction in social anxiety after MDMA-assisted psychotherapy with autistic adults: a randomized, double-blind, placebo-controlled pilot study. Psychopharmacol (Berl). 2018;235(11):3137-3148. doi: 10.1007/s00213-018-5010-9.
- Iverach L, Rapee RM. Social anxiety disorder and stuttering: current status and future directions. J Fluency Disord. 2014;40:69-82. doi: 10.1016/j.jfludis.2013.08.003.
- Lowe R, Menzies R, Onslow M, Packman A, O’Brian S. Speech and anxiety management with persistent stuttering: current status and essential research. J Speech Lang Hear Res. 2021;64(1):59-74. doi: 10.1044/2020_JSLHR-20-00144.
- Menzies RG, Onslow M, Packman A, O’Brian S. Cognitive behavior therapy for adults who stutter: a tutorial for speech-language pathologists. J Fluency Disord. 2009;34(3):187-200. doi:10.1016/j.jfludis.2009.09.002.
- McAllister J, Gascoine S, Carroll A, et al. Cognitive bias modification for social anxiety in adults who stutter: a feasibility study of a randomised controlled trial. BMJ Open. 2017;7(10):e015601. doi:10.1136/bmjopen-2016-015601.
- Menzies RG, Packman A, Onslow M, O’Brian S, Jones M, Helgadóttir FD. In-clinic and standalone Internet cognitive behavior therapy treatment for social anxiety in stuttering: a randomized trial of iGlebe. J Speech Lang Hear Res. 2019;62(6):1614-1624. doi: 10.1044/2019_JSLHR-S-18-0340.
- Chard I, Van Zalk N, Picinali L. Virtual reality exposure therapy for reducing social anxiety in stuttering: a randomized controlled pilot trial. Front Digit Health. 2023;5:1061323. doi:10.3389/fdgth.2023.1061323.
- Maguire GA, Gottschalk LA, Riley GD, Franklin DL, Bechtel RJ, Ashurst J. Stuttering: neuropsychiatric features measured by content analysis of speech and the effect of risperidone on stuttering severity. Compr Psychiatry. 1999;40(4):308-314. doi:10.1016/s0010-440x(99)90132-3.
- Maguire GA, Riley GD, Franklin DL, Gottschalk LA. Risperidone for the treatment of stuttering. J Clin Psychopharmacol. 2000;20(4):479-482. doi: 10.1097/00004714-200008000-00013.
- Maguire GA, Riley GD, Franklin DL, Maguire ME, Nguyen CT, Brojeni PH. Olanzapine in the treatment of developmental stuttering: a double-blind, placebo-controlled trial. Ann Clin Psychiatry. 2004;16(2):63-67. doi: 10.1080/10401230490452834.
- Maguire G, Franklin D, Vatakis NG, Morgenshtern E, Denko T, Yaruss JS, et al. Exploratory randomized clinical study of pagoclone in persistent developmental stuttering: the EXamining Pagoclone for peRsistent dEvelopmental Stuttering Study. J Clin Psychopharmacol. 2010;30(1):48-56. doi: 10.1097/JCP.0b013e3181caebbe.
- Schneier FR. Clinical practice. Social anxiety disorder. N Engl J Med. 2006;355(10):1029-1036. doi:10.1056/NEJMcp060145.
- Yairi E, Ambrose N. Epidemiology of stuttering: 21st century advances. J Fluency Disord. 2013;38(2):66-87. doi: 10.1016/j.jfludis.2012.11.002.