






Metacognitive Therapy for Bipolar Disorder: A Case Study
Metacognitive therapy for bipolar disorder. A clinical case report from Denmark
Dr. Pia Callesen¹, Tina Bihal¹ (HCPC approved Clinical Psychologist)*
- Cektos – Center for Metakognitiv terapi, Borgergade 28, 4 sal, 1300 Copenhagen, Denmark.
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Callesen, P., 2024. Metacognitive therapy for bipolar disorder. A clinical case report from Denmark. Medical Research Archives, [online] 12(10).
https://doi.org/10.18103/mra.v12i10.5777
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5777
ISSN 2375-1924
ABSTRACT
Bipolar disorder is one of the most serious psychiatric disorders that has recurrent and sometimes chronic nature. Metacognitive therapy is a new treatment for this population with promising results from the previous studies reported. A clinical case report referring to a 35-year old male suffering from bipolar disorder is presented describing the stages of metacognitive therapy. Firstly, a case formulation is produced evaluating strategies and how they backfire and maintain symptoms. Afterwards, the patients’ negative and positive metacognitive beliefs about uncontrollability and the usefulness of worrying and ruminating are restructured. Further larger scale investigations are needed to further document the effect of metacognitive therapy for bipolar disorder.
Introduction
Bipolar disorder (BD) is a serious mental illness that has a high mortality rate and a significant impact on quality of life¹. When including all types of bipolar disorders, the lifelong prevalence rate can reach 7.8%² and is defined by a markedly unbalanced fluctuation in mood, activity levels, and self-perception³. BD is characterised by a person experiencing altering episodic emotional states ranging from elevated mood or mania to lower mood or depression. The condition manifests in cycles or episodes and is typically regarded as chronic. Although manic and depressive episodes are usually included, mixed episodes can also occasionally happen¹.
Cognitive behavioural therapy (CBT) has been the most researched psychological treatment for bipolar disorder (BD)¹¹. However, research indicates that CBT recovery rates frequently lead to small to moderate effect sizes⁵. Furthermore, a recent meta-analysis by Chiang et al.⁶ emphasises that combining medication and CBT improves recovery rates and lowers relapse rates, especially for BD I. However, modest to moderate effect sizes were also routinely seen in these studies. Consequently, to improve treatment outcomes and lower recurrence rates in this patient population, it is necessary to investigate an alternative and more efficient treatment approach to BD.
The S-REF model and the CAS
In recent years, there has been a surge of interest in metacognition and metacognitive therapy as a new approach to understanding and treating mental disorders. Metacognitive therapy (MCT), developed by Wells in 2007⁷, is based on the Self-Regulatory Executive Function (S-REF) model, a transdiagnostic model of emotional disorders. The model explains how negative thinking perpetuates mental illnesses such as depression and bipolar disorder⁸.
According to Wells⁷, the Cognitive-Attentional Syndrome (CAS) is crucial for the onset and progression of these disorders. The CAS consists of perseverative thinking, threat monitoring and maladaptive coping strategies. For mood disorders such as depression the CAS typically shows as ruminative thinking patterns, focusing the attention on internal states such as low mood and energy. This overthinking and internal focus is accompanied by avoidance, reduced activity levels and lack of interest in social interactions⁷.
The CAS is perpetuated by negative and positive metacognitive beliefs about worry and rumination. Negative beliefs, such as “rumination is uncontrollable,” is central to depression and is also seen in several other conditions when there is uncontrollability over concern, danger assessment, or perseverative thinking. On the other hand, positive beliefs are presumptions about the benefits of thinking things through such as “rumination helps me find solutions”⁷. Restructuring of these underlying metacognitive beliefs, both positive and negative reduces the CAS. MCT addresses CAS by altering underlying metacognitive beliefs, yielding high efficacy rates of 70–80% for anxiety and depression¹⁰,¹¹,¹².
The significance of metacognitive beliefs in bipolar disorder
Østefjells et al.¹³ conducted a study that compared metacognitive beliefs and thought control strategies in individuals with bipolar disorder (n=80) and control subjects (n=166). The results showed that individuals with bipolar disorder had higher levels of unhelpful metacognitive beliefs and thought control strategies than the control group. Depression and age at onset of affective disorders were factors that may influence these metacognitive patterns in individuals with bipolar disorder¹³.
A recent study conducted by Palmer et al.¹⁴ examined the link between unhelpful cognitions and mood symptoms in individuals with bipolar disorder (n = 331) over time (3 months), as well as the potential mediating effect of self-compassion across sections. Results showed that inappropriate metacognitions were the only significant predictor of depression at 3-month follow-up (β = 0.31, p < .001), with no relationship to mania over time. Thus, longitudinally, baseline unhelpful metacognitions significantly predicted depression at 3-month follow-up. Unhelpful metacognitions were predictive of future depression severity, and therefore further exploration of metacognitive therapy for bipolar disorder should be considered.
Reinholdt-Dunne et al.¹⁵ compared patients with bipolar disorder in remission (n=28) with healthy controls (n=31) and found that patients had higher levels of inappropriate metacognitive beliefs and reduced attentional control as well as cognitive impairments. The results indicate that these metacognitive beliefs may be associated with persistent anxiety in patients with bipolar disorder in remission. Therapies targeting maladaptive metacognitive beliefs may help reduce anxiety and improve functional recovery and quality of life in these patients.
Aim of the article
CEKTOS is specialised in delivering metacognitive therapy to patients with various mental health problems and is also a pioneer in investigating cutting-edge methods of treating mood disorders¹⁶,¹⁷. We therefore seek to present a thorough demonstration of the bipolar disorder treatment strategy used by CEKTOS, with a focus on the application of metacognitive therapy to address maladaptive thought processes, patterns and coping mechanisms that exacerbate symptoms and impede functioning in persons with BD.
This article includes a review of relevant literature, expanding upon Callesen et al.’s (2020) seminal work, to explore the role of metacognition and metacognitive therapy in bipolar disorder treatment. By integrating clinical insights from CEKTOS with findings from wider literature, we aim to deepen understanding of the potential benefits of incorporating metacognitive principles into treatment. Ultimately, our objective is to inform clinical practice and inspire further research to enhance treatment outcome for individuals with bipolar disorder.
This case report delineates the application of metacognitive therapy at CEKTOS, Center for Metacognitive Therapy, Denmark, in the treatment of Daniel (Daniel is a false name):
Daniel is a 35-year-old unemployed male. He arrives at the clinic with complaints of excessive sadness and hopelessness. He has experienced this multiple times over the last decade, each time with great intensity. He has attempted suicide once, which led to psychiatric hospitalization. What he describes as in the dark periods, he uses most of his time examining why he feels this way, and tries to mentally retrace where it could all stem from. His mother was emotionally unavailable for much of his life as she dealt with mood issues similar to his. Daniel thinks this is where it all came from. When his mood is low, he spends most of the day in bed, trying to sleep it away. These periods are also the cause of his unemployment as he has no energy to keep up a job when he feels this way. Daniel explains another difficulty which has caused problems for him in the past. He has periods, occasionally, lasting anywhere from a couple of days to a couple of weeks, where he has a lot of energy and has all the confidence in the world, however this causes him to do things he would not normally do. In the past he has bought plane tickets to different countries without any plan or ideas of what to do there, or he has become highly promiscuous, which is highly unlike him. In these periods, he also sleeps very little as he does not need it as much. After a period like this, he spends a lot of time thinking about why he did, and he is highly
ashamed of his behavior. After hours of inner focus he ends up concluding that his future is hopeless. He is currently on antidepressants and has previously tried CBT where he was instructed in restructuring dysfunctional thinking to more rational or realistic thoughts, but it has not helped. He has read a bit about MCT, and he has therefore tried to reduce thinking as much, but he cannot seem to stop. Daniel hopes to become happier and more stable moods as a result of treatment.
Case formulation and socialisation
In the first stage of treatment Daniel and his therapist fill out a case formulation to begin to understand how Daniel is dealing with his trigger thoughts in various maladaptive ways. After one of his manic episodes Daniel has thoughts of regret e.g. “Why did I do so many stupid things?” (trigger thoughts). He does not leave these thoughts alone but instead has a tendency to regret his actions not just for a couple of minutes but for several days (CAS). This long-term regret results in depressive symptoms and he ends up concluding that “he is a loser” and that “the future is hopeless”. In addition, he tries to avoid his trigger thoughts by sleeping more which backfires and prolongs his low energy and low mood. Mostly, these depressive episodes last for weeks until he feels a bit better. On better days he wakes up with a lot of energy and ideas. Where his trigger thoughts in contrast consist of a lot of ideas and an omnipotent state of self-worth e.g. “I want to fly to Australia!” or “I want to have sex with a woman now!”, “I’m a cool guy!”. Daniel does not leave his positive thoughts alone. He dwells and acts on his ideas and thereby uses the CAS to drag himself up from the depression and prolongs his manic state. Below is a short case formulation using the A-M-C model both in a depressive and manic period.
Fig. 1: Daniels A-M-C case formulation on his depression:
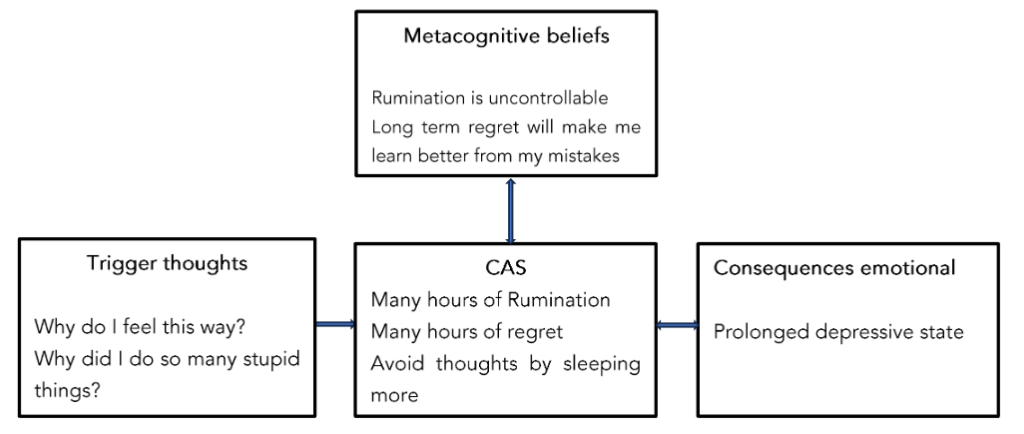
Fig. 2: Daniels A-M-C case formulation model in a manic state
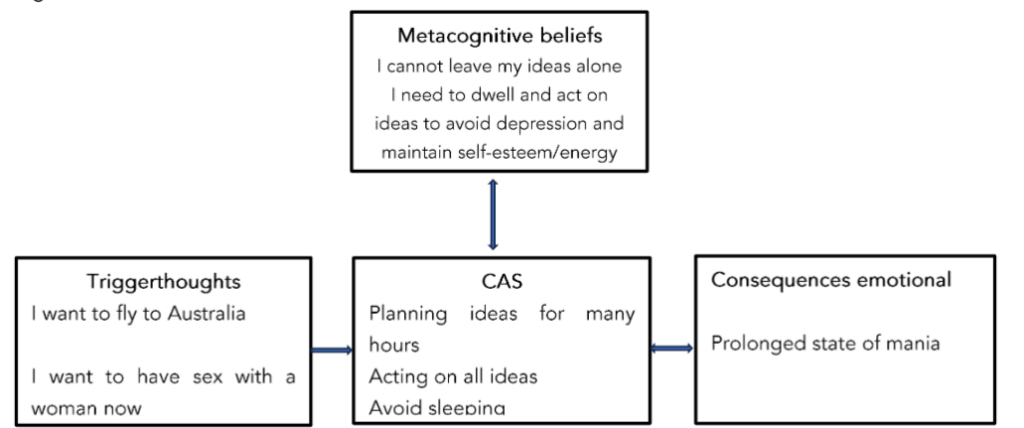
Figure 1+2 the reformulated A-M-C model. Adapted from Wells (2000). Copyright 2000 by John Wiley and Sons Limited. Adapted by permission.
After filling out the case formulation both for a depressive and a manic period Daniel was socialised to the model using guided discovery questions like: “Looking at this model do you think that the trigger thoughts or the many hours ruminating/ dwelling and planning (CAS) is the cause of prolonged states of depression and mania?” “If you believed that rumination and the other CAS strategies are not uncontrollable what would happen to your emotions?”. The goal of these questions is to socialise Daniel to understand how the CAS is driving prolonged states of depression and mania similarly, he is guided to discover that the CAS is driven by low meta-awareness and negative and positive metacognitive beliefs about the uncontrollability and usefulness of the CAS.
Introducing attention training (ATT / SPACE) and Detached Mindfulness (DM)
The next stage in therapy is introducing attention training and the opposite of the CAS called detached mindfulness.
The Attention Training Technique (ATT) was developed as part of MCT to help moderate CAS activation by increasing top-down attentional control and flexibility. ATT consists of auditory attentional exercises that require individuals to engage in executive control skills including selective attention, divided attention, and attention switching (for a comprehensive overview of ATT, see Wells, 2007)⁷.
From the first session and throughout treatment, ATT is implemented to enhance metacognitive awareness and show the patient that they can be flexible with their attention independently of events inside or outside of their mind.
DM is the state of awareness of internal events, without responding to them with sustained evaluation, attempts to control or suppress them, or respond to them behaviourally⁷. DM is introduced using two metaphors: 1) the fish hook metaphor and 2) the telephone metaphor. The fish hook metaphor: Trigger thoughts are like fish hooks in your mind and the best strategy is to leave the thoughts alone. Telephone metaphor: Trigger thoughts are like the telephone ringing. If you patiently leave it alone it eventually will stop ringing. Daniel chooses the fish hook metaphor as his preferred illustration of handling trigger thoughts (CAS) and leaving them alone (DM). Afterwards, DM is demonstrated using the tiger task. In this exercise Daniel is asked to visualise a tiger in his mind and after this to let go of trying to control the image and instead practice strategies of DM, attention shift and postponing any rumination or acting on manic thoughts.
Luckily, when it comes to depression most research suggests that this state is more a result of rumination than lack of Serotonin⁸.
After 10 sessions Daniel scores low on his uncontrollability and positive beliefs. He is able to leave alone both depressive and manic trigger thoughts and thereby keep himself in a balanced place with naturally fluctuating moods without prolonged states of mania and depression.
Please find full details of all techniques above for depression in Metacognitive therapy for anxiety and depression⁷.
Discussion
The results of previous studies in metacognitions and MCT for bipolar disorder suggest that MCT could potentially be an effective treatment for this difficult to treat patient group.
The main target in MCT is to improve self-regulatory executive functioning and reduce self-defeating processes. This intervention is different from other approaches used in the treatment of bipolar disorder. To work more systematically and directly on the attentional processes and executive functions, but also reducing the level of perseverative thinking, such as depressive and manic rumination, is unique to the MCT approach. Furthermore, targeting the cognitive attentional syndrome (CAS) and restructuring dysfunctional metacognitive beliefs is at the core of MCT in order to achieve more adaptive self-regulation and cognitive flexibility.
The results of previous single case trials suggest that MCT was associated with good clinical response from pre to post-treatment for metacognitive beliefs and symptoms. The gains seem to be maintained at 1-year follow-ups. This relatively brief intervention seems to be feasible for outpatient treatment and appears to compare favorably with comprehensive treatments of longer duration.
The MCT protocol described in this article illustrated with a prototype case example how this treatment is well tolerated by patients with bipolar disorder and associated with significant improvements.
We demonstrate the effect on a male patient from our clinic suffering from bipolar disorder.
In our clinic, our experience is that most bipolar patients will benefit from MCT. However, larger controlled and randomized RCTs are now needed to further investigate and demonstrate effects of MCT for bipolar disorder.
Conclusion
This case report on a 35-year old male suffering from bipolar disorder describes a new treatment for bipolar disorder: Metacognitive therapy. Further randomized and controlled trials are needed to investigate the promising effect of metacognitive therapy for this population.
Testimonial from a patient diagnosed with bipolar disorder I:
A British 37-year-old female diagnosed with bipolar disorder I participated in CEKTOS’ six-week online transdiagnostic metacognitive group therapy treatment in March 2024. Throughout the program, she worked on identifying the metacognitive beliefs that fueled both her depressive and manic episodes. Through techniques such as attention training (ATT) and detached mindfulness (DM), she learned how to disengage from ruminative thinking and avoid acting on impulsive thoughts during manic states. By the end of the six weeks, she experienced greater stability in her mood, reporting fewer extreme highs and lows. She also felt more in control of her thoughts, with reduced distress and improved emotional balance. The group therapy environment provided her with a sense of shared experience, enhancing her confidence in managing her condition. The following statement is extracted from a written interview in August 2024:
“Firstly, the therapy as a whole was profoundly helpful, particularly the insomnia component – this may be something else to market to as my sleep now is literally that of a different person. Before I was sleeping fitfully, waking multiple times, and the lack of sleep was both causing and exacerbating mania symptoms. When depressed (contributed to by antipsychotics), I was sleeping 14 hours a day, but not generally feeling too guilty about it or feeling any particular time pressure in my greatly reduced waking hours. I was taking sleeping pills combined with clonazepam (and sometimes promethazine also) approximately 6 times a month, usually after waiting two hours after going to bed (since approximately summer 2020). Post the MCT session specifically targeting it, the first initial week I took sleeping pills several times, but have not had any zopiclone or clonazepam since March (onset of the MCT group therapy). My sleep is much calmer, more solid. I still wake in the night but much less, and I am not sleeping heavily past 9am (helped by being on a lower antipsychotic dose also). I am extremely grateful for this change, and I cannot see how I would have achieved this by any other means.
I have had a much clearer head and haven’t needed to consciously apply techniques because days have been going smoothly. When I have experienced mania symptoms, they cleared up surprisingly quickly. When a friend passed away last month, I felt tangible feelings of grief rather than a miasma of grief for every bereavement I’ve experienced. Apophenia – ascribing meaning to meaningless events – this has greatly reduced, and I believe I have more awareness of it when it does occur. I have been able to notice that I am experiencing emotions in real time rather than thinking two weeks later, oh, perhaps I was angry then. I have had occasion to use the word ‘euthymic’ frequently in my mood diary. My weight is stable, whereas it usually tracks an up and down course following my mood. Positive stimulating events are just as triggering as negative ones for me, and [the MCT therapist] noted this when she said ‘You need to hold back from experiencing positive emotions.’ I have not been writing/ruminating in my personal journal because there’s nothing to ruminate about.
The MCT therapist was unflappable and nonjudgemental, which has not always been my experience in clinical and therapeutic settings.” – Female, Age 37, UK
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
None.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013. doi:10.11 76/appi.books.9780890425596.
2. Özdel K, Kart A, Türkçapar MH. Cognitive behavioural therapy in treatment of bipolar disorder. Arch Neuropsychiatry. 2021.
3. Bebbington P, Ramana R. The epidemiology of bipolar affective disorder. Soc Psychiatry Psychiatr Epidemiol. 1995;30(6):279-292. doi:10.1007/BF00805795.
4. Newman CF, Leahy RL, Beck AT, Reilly-Harrington NA, Gyulai L. Bipolar disorder: A cognitive therapy approach. American Psychological Association; 2002. doi:10.1037/10442-001.
5. Szentagotai A, David D. The efficacy of cognitive-behavioral therapy in bipolar disorder: A quantitative meta-analysis. J Clin Psychiatry. 2010;71(1):66-72. doi:10.4088/JCP.08r04559yel.
6. Chiang KJ, Tsai JC, Liu D, Lin CH, Chiu HL, Chou KR. Efficacy of cognitive-behavioral therapy in patients with bipolar disorder: A meta-analysis of randomized controlled trials. PLoS One. 2017;12(5) . doi:10.1371/journal.pone.0176849.
7. Wells A. Metacognitive Therapy for Anxiety and Depression. Guilford Press; 2009.
8. Wells A, Matthews G. Attention and emotion: A clinical perspective. L Erlbaum; 1995.
9. Wells A, Matthews G. Modelling cognition in emotional disorder: The S-REF model. Behav Res Ther. 1996;34(11-12):881-888. doi:10.1016/S0005-7967(96)00050-2.
10. Normann N, Van Emmerik AAP, Morina N. The efficacy of metacognitive therapy for anxiety and depression: A meta-analytic review. Depress Anxiety. 2014;31(5):402-411. doi:10.1002/da.22273.
11. Normann N, Morina N. The efficacy of metacognitive therapy: A systematic review and meta-analysis. Front Psychol. 2018;9:2211. doi:10. 3389/fpsyg.2018.02211.
12. Rochat L, Manolov R, Billieux J. Efficacy of metacognitive therapy in improving mental health: A meta-analysis of single-case studies. J Clin Psychol. 2018;74(6):896-915. doi:10.1002/jclp.22567.
13. Østefjells T, Melle I, Aminoff SR, et al. An exploration of metacognitive beliefs and thought control strategies in bipolar disorder. Compr Psychiatry. 2017;73:84-92. doi:10.1016/j.comppsy ch.2016.11.008.
14. Palmer-Cooper EC, Woods C, Richardson T. The relationship between dysfunctional attitudes, maladaptive perfectionism, metacognition and symptoms of mania and depression in bipolar disorder: The role of self-compassion as a mediating factor. J Affect Disord. 2023;341:265-274. doi:10.1016/j.jad.2023.08.117.
15. Reinholdt-Dunne ML, Seeberg I, Blicher A, et al. Residual Anxiety in Patients with Bipolar Disorder in Full or Partial Remission: Metacognitive Beliefs and Neurocognitive Function. Cognit Ther Res. 2021;45(1):179-189. doi:10.1007/s10608-020-10148-7.
16. Callesen P. Live More Think Less. Icon Books; 2020.
17. Callesen P, Pedersen ML, Andersen CK, Wells A. Metacognitive therapy for bipolar II disorder: A single case series study. Neurol Psychiatry Brain Res. 2020;38:107-113. doi:10.1016/j.npbr.2020.08.004.
18. Wells A. Detached mindfulness in cognitive therapy: A metacognitive analysis and ten techniques. J Ration Emot Cogn Behav Ther. 2005;23(4). doi:10.1007/s10942-005-0018-6.