

Epidural vs. PCA for Scoliosis Surgery: A Comparative Study
A Retrospective, Multicentre Comparison of Continuous Epidural Analgesia and Patient-Controlled Analgesia Following Posterior Spinal Instrumented Fusion for Adolescent Idiopathic Scoliosis
Maisha M Jamali 1,2; J. Paige Little 1; Kris Lundine 5; Gregory E Moloney 3; Donna M Peachey 5; Maree T Izatt 1,2; Adam F Parr 2; Robert D Labrom 1,2; Dimitrios Vagenas 4; Geoffrey N Askin 1,2
- Biomechanics and Spine Research Group, Queensland University of Technology at the Centre for Children’s Health Research,
Brisbane, Australia - Orthopaedics Department, Queensland Children’s Hospital, Brisbane, Australia
- Anaesthetics Department, Queensland Children’s Hospital, Brisbane, Australia
- Research Methods Group, Faculty of Health, Queensland University of Technology
- The Royal Children’s Hospital, Melbourne, Australia
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Jamali, MM., Little, JP., et al., 2025. A Retrospective, Multicentre Comparison of Continuous Epidural Analgesia and Patient-Controlled Analgesia Following Posterior Spinal Instrumented Fusion for Adolescent Idiopathic Scoliosis. Medical Research Archives, [online] 13(10).
https://doi.org/10.18103/mra.v13i10.7044
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.7044
ISSN: 2375-1924
Abstract
Introduction: The Queensland Children’s Hospital (QCH) in Brisbane, Australia offers continuous epidural analgesia as standard postoperative care for adolescent idiopathic scoliosis following posterior spinal instrumented fusion. Intravenous patient-controlled analgesia, is a well-established alternative for managing postoperative pain. Both modalities are associated with side effects. Epidurals are linked to transient neurological changes, while patient controlled analgesia is associated with opioid induced complications. To compare continuous epidural analgesia to patient controlled analgesia, data from Queensland Children’s Hospital and the Royal Children’s Hospital (RCH) (where patient controlled analgesia is standard for postoperative analgesia), was analyzed. The primary objective was to assess safety and side-effects of both methods by assessing objective postoperative outcomes.
Methods: A retrospective chart review was conducted at Queensland Children’s Hospital from 06/01/2020 to 19/12/2022 and at Royal Children’s Hospital from 07/01/2020 to 13/12/2022. The study included 203 patients, with 120 patients from Royal Children’s Hospital and 83 from Queensland Children’s Hospital. Mean ages were 14.64 +/- 1.54 and 14.92 +/- 1.71 respectively (P=0.28). Mean cobb scores were 70.55 +/- 17.83 and 66.70 +/- 10.59 respectively (P=0.06). Data analysis involved student’s t-test and Chi-squared analysis using SPSS software.
Results: Patient demographics were comparable, however Queensland Children’s Hospital patients had more levels fused (P<0.01). Queensland Children’s Hospital patients experienced lower rates of sedation and discharge without a bowel motion (P<0.01). Temporary neurological complications were exclusive to QCH patients (26 cases), however all cases resolved without further complications. Rates of respiratory depression, postoperative nausea and vomiting, readmissions and deep surgical infections were similar (P>0.05). At RCH, 51.67% of patients mobilized with physiotherapy assistance of POD1, compared to 54.22% at QCH. Mean discharge time for Royal Children’s Hospital and Queensland Children’s Hospital was 3.45+/-1.15 and 5.36+/-1.69 days respectively (P<0.01). Both centres had 6 unplanned readmissions (P=0.49).
Conclusion: Both continuous epidural and patient-controlled analgesia are safe and effective following posterior spinal fusion for adolescent idiopathic scoliosis, though they differ in complication profiles. Epidurals are linked to transient neurological effects, while PCA is associated with opioid-related sedation and respiratory depression. Differences in recovery outcomes, particularly diet resumption and discharge, may reflect the impact of accelerated discharge pathways on optimizing patient recovery.
Keywords
Continuous Epidural Analgesia, Patient-Controlled Analgesia, Adolescent Idiopathic Scoliosis, Postoperative Pain Management, Spinal Fusion
Introduction
Scoliosis is a three-dimensional anatomic alteration of the spine, characterised by a curvature measured in the coronal plane of at least 10 degrees, as defined by the Cobb method, see image 1. 1. The most prevalent form is adolescent idiopathic scoliosis (AIS), with a population prevalence of 2-4% of children aged 10-18 years 2,3. Surgical intervention is indicated for curves with concern of progression and causing physiological distress, such as loss of pulmonary function 4. Posterior spinal instrumented fusion (PSIF), has been the standard surgical approach, encompassing extensive midline dissection through subcutaneous fat, fascia and ligaments to affix alloy rods which impart corrective and distracting forces 5. As such, post-operative pain is a challenging aspect of scoliosis corrective surgery and, if poorly controlled, can lead to increased morbidity, delayed recovery, prolonged duration of opioid use and higher health care costs 6.
Intravenous patient-controlled analgesia (PCA) is a widely studied and accepted method for managing post-operative pain for many procedures including PSIF in children with adolescent idiopathic scoliosis 7. Despite its widespread use, commonly observed complications include nausea, vomiting, pruritus, respiratory depression, sedation, confusion, urinary retention and inadequate analgesia 8,9. Epidural analgesia is an alternate method for management of post-operative pain. This requires the placement of an epidural catheter prior to closure of the surgical wound with infusion of a combination of local anaesthetic and an opioid agent post-operatively. Epidural analgesia has concerns related to epidural haematomas, epidural abscess, transient neurological changes and dural puncture headaches10. Occasionally, epidurals may create a temporary change in neurological examination requiring cessation. As such this method is cautiously utilised, particularly for patients who have undergone spinal correction surgery 7. In a separate review, the authors of the present study conducted a thorough evaluation of the safety profile of epidural analgesia, which will be referred to within this paper 11.
Both methods of post-operative analgesic control have been utilised in the AIS field, however the use of PCA predominates, with limited literature on the use of continuous epidural analgesia (CEA) in the AIS patient cohort.
In carrying out a retrospective patient chart review, this study aimed to determine if the use of continuous epidural analgesia and patient controlled analgesia was comparable following posterior spinal fusion for adolescent idiopathic scoliosis. Specifically, post-operative outcomes related to the analgesic modality and conducted a safety profile review to ensure the comparability and acceptability of both pain relief methods for the AIS population.
Methods
Since its inauguration in 2015, the Queensland Children’s Hospital (QCH) Brisbane, Australia has utilised CEA as the standard analgesic modality for PSIF surgical correction of AIS. In comparison, the Royal Children’s Hospital (RCH) in Melbourne, Australia provides PCA as part of standard care. A multicentre retrospective chart review was therefore designed, with the QCH cohort compared against a matched PCA cohort from the Royal Children’s Hospital.
Ethics in accordance with the National Health and Medical Research Council’s “National Statement on Ethical Conduct in Human Research (2007), NHMRC and Universities Australia Australian Code for the Responsible Conduct of Research (2007) and the “CPMP/ICH Note for Guidance on Good Clinical Practice” was granted for this project. The study was approved by the appropriate Institutional Review Board (IRB), the Children’s Health Queensland Hospital and Health Service Human Research Ethics Committee, reference LNR/21/QCHQ/75249, and as such the requirements for written informed consent was waived by the IRB. A retrospective chart review was performed for AIS patients who underwent PSIF and received CEA from 06/01/2020 to 19/12/2022, and PCA from 07/01/2020 – 13/12/2022. Patients with alternative causes of scoliosis (neuromuscular, congenital, post traumatic) or previous spinal surgery were excluded. Ages ranged from 10 to 18 at both centres, with body height ranging from 135-175cm and 140-185cm and body weight ranging from 30-110kg and 35-105kg at CEA and PCA centres respectively. Additional demographic data, including the distribution of females, pre-operative cobb angle and surgical levels fused were collected from the electronic medical records.
Data extraction included patient demographics (age, sex, height, weight), curve characteristics (major Cobb angle), operative details (levels fused), and postoperative course. Outcome measures included efficacy endpoints (days to first defecation, resumption of solid diet, and length of stay) and safety endpoints (sedation, respiratory depression, bowel motion, postoperative nausea and vomiting, readmission, surgical infection, and temporary neurological change). All data were independently verified by two investigators.
Statistical analysis was performed with IBM SPSS v28. Continuous variables were analysed using bootstrapped Student’s t-tests, while categorical outcomes were compared with Chi-squared tests. A significance level of p<0.05 was adopted.
Continuous epidural analgesia protocol
Epidural catheters placement prior to surgical closure was typically conducted with an 18 gauge (French) size and was inserted by the surgeon under direct visualisation, or through the standard loss of resistance to air technique through the ligament flavum, using a Touhy needle, see image 2 12. The catheters were placed five centimetres within the epidural space at a chosen thoracic and/or lumbar level, to ensure adequate spread and coverage of local anaesthetic. Catheters were tunnelled to an exit point lateral to the midline incision utilised for the PSIF surgery. Upon completion of instrumentation and final neuromonitoring evoked stimulations, an epidural bolus of local anaesthetic containing 1 microgram/kg Fentanyl +/- 50 microgram/kg of morphine was administered. After awakening, an infusion of local anaesthetic (typically levobupivacaine 0.125%) was commenced at a total of 0.2 mls/kg/hr with a maximum rate of 0.3mls/kg/hr. No further opioid analgesia was provided through the catheter. Epidural infusion rates were typically commenced at a ratio of 1/3rd to the superior and 2/3rd to the inferior epidural and remained in-situ for 64-72 hours. Patients were placed on regular oral paracetamol and ibuprofen as required. In instances where analgesia was deemed insufficient, rescue oral opioids were offered. Oral analgesics were frequently timed to be given pre-physiotherapy. On the third post-operative morning, epidurals infusions were ceased at 0600 with a subsequent enteral opioid plan. If analgesic failure did not occur, catheters were removed later that day. While this centre does not follow a formalised discharge pathway, certain prerequisites were required for patient discharge as per Table 1.
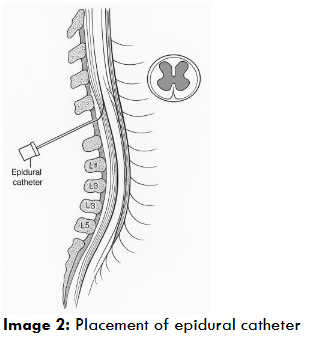
Table 1: Discharge criteria for CEA and PCA patients
| Discharge requirements | CEA (QCH) | PCA (RCH) |
|---|---|---|
| Oral intake | Tolerating a solid diet | Passing urine |
| Gastrointestinal | Passed one formed bowel motion | Passing urine |
| Passing flatus | ||
| Pain | Adequate pain control on oral analgesic (or pain relieving) medication | |
| Mobility | Deemed safe from physiotherapy and occupational therapy to have returned to reasonable activities of daily life (toileting, transfers, independent mobility) |
Patient controlled analgesia protocol
A PCA with a ketamine infusion commencing at 0.2mg/kg/hr was commenced post-operative day (POD) zero. Additional enteral Targin at a dose of 10mg/5mg PO BD for <60kg (15mg/7.5mg for ≥60kg) was commenced on the same afternoon if it were a morning case, and commenced the next morning if it was an afternoon case. Supplemental IV/oral Paracetamol, NSAIDs, Diazepam (PRN), tramadol (PRN) and clonidine (PRN) were also provided. Requirements for discharge were dictated as per Table 1. These patients were assigned an accelerated discharge pathway as per hospital protocol (see table series; 1). The pathway encouraged resumption of a solid diet, independent mobilisation and removal of the indwelling catheter on POD1. Patients were routinely discharged at 72-96 hours post-operatively if discharge goals had been met (See table 1).
Table series 1: Accelerated Discharge Pathway for Adolescent idiopathic scoliosis patients following posterior spinal fusion
| Day | Task |
|---|---|
| Day 0 | Reviewing the class, signs of clear discharge |
| Day 1 | Continue monitoring |
| Day 2 | Regular diet as tolerated |
| Day 3 | Discharge planning |
Post-operative outcome measures
Post-operative outcome measures were chosen to assess both efficacy and safety of the analgesic methods. To evaluate efficacy, we measured time-to-event parameters including the number of days until the first bowel motion, resumption of a solid diet, and discharge from hospital.
Safety outcomes selected for review included sedation, respiratory depression, bowel motion, post-operative nausea and vomiting (PONV), readmission and deep infection. Elevated sedation scores were recorded based on any elevation noted in nursing charts entries or in accordance with the Children’s Early Warning Tool (CEWT). Respiratory depression was marked by either (1) reduced respiratory rate (e.g., to less than 10 breaths/min) or (2) reduced oxygen saturation (e.g., arterial oxygen saturation less than 90%) 13. Occurrence of post-operative nausea and vomiting was recorded if any nausea or vomiting, beyond POD 0, required pharmacological intervention. Discharge without bowel motion was also recorded. It is important to highlight the protocol governing the administration of PCA analgesia does not mandate a bowel movement occurring before discharge, however at QCH, this was recommended prior to discharge. Readmissions related to the initial PSIF admission were recorded. Instances of deep surgical infections necessitating surgical washout were included for both CEA and PCA cohorts considering the associated risk in the profile of epidural catheters 14.
Assessment of any temporary neurological changes was an important component in assessing the safety profile of CEA. Neurological examinations for these patients were conducted in accordance with the international standards for neurological classification of spinal cord injuries scale as established by the American spinal injury association (ASIA) 15. A post operative neurological assessment was initially performed in the post-anaesthesia care unit (PACU) once the patient regained consciousness. Subsequent daily assessments were conducted by the treating clinicians, following ASIA examination guidelines, with documentation of motor and sensory scores. Immediate attention was given to any differences from the pre-operative baseline. This protocol has been further elaborated in a paper currently under in press11. All patients in this study had complete sensory perception and motor strength on discharge.
Data collected was analysed with IBM SPSS software. To obtain a robust result, a bootstrapped Students T test was utilised to compare demographics and all continuous outcomes; days to first bowel motion, days to return to full diet and days till discharge from hospital. Chi squared analysis was utilised for safety related measures. Further analysis of mobilisation utilised a bootstrapped Students T test and Chi squared analysis to obtain significance data.
Results
The study identified a cohort of 120 patients who received PCA analgesia and 83 patients who received CEA analgesia. Patient demographics, detailed in Table 2, showed comparable results. Comparison of the mean pre-operative major cobb angles neared statistical significance (p=0.06), with the CEA having a mean cobb angle of 70.55 degrees and the PCA cohort having a mean major cobb angle of 66.70 degrees. Statistical significance was observed in the variance of the number of levels fused (P<0.01).
Table 2: Patient demographics for PCA and CEA cohorts (mean (SD))
| PCA (n=120) | CEA (n=83) | P Value comparing PCA and CEA | |
|---|---|---|---|
| Age (years) | 14.92 (1.71) | 14.64 (1.54) | 0.28 |
| Females | 92 | 71 | 0.12 |
| Height (cm) | 163.31 (11.47) | 159.57 (8.30) | 0.11 |
| Weight (kg) | 56.48 (12.86) | 56.68 (14.08) | 0.91 |
| Major Cobb angle (degrees) | 66.70 (10.59) | 70.55 (17.83) | 0.06 |
| Levels fused | 10.02 (1.74) | 10.7 (1.65) | <0.01 |
The study further examined time-to-event efficacy parameters, encompassing days to first defecation, days to return to a solid diet and days to hospital discharge, with associated P values presented in Table 5. All measured parameters had statistically significant disparities between the two cohorts (P<0.01). The significance of this outcome should be considered in the context of implementation of an accelerated discharge pathway for PCA patients, compared to CEA patients who did not.
Table 3: Mobilisation on POD1
| POD1 mobilisation | PCA (n=120) | CEA (n=83) | P Value comparing PCA and CEA |
|---|---|---|---|
| Number of patients, (% of cohort) | 112 (94.17%) | 49 (59.04%) | <0.05 |
Table 4: Occurrence of patient safety related complications for PCA and CEA cohorts (Chi squared)
| Safety outcomes | PCA (n=120) | CEA (n=83) | P Value comparing PCA and CEA |
|---|---|---|---|
| Elevated sedation | 90 | 1 | <0.01 |
| Respiratory depression | 9 | 5 | 0.68 |
| Discharge without bowel motion* | 91 | 7 | <0.01 |
| Post operative nausea and vomiting | 88 | 56 | 0.37 |
| Readmissions | 6 | 6 | 0.49 |
| Deep surgical infection requiring washout | 2 | 1 | 0.79 |
| Temporary neurological change | 0 | 26 | <0.01 |
Discussion
There is a paucity of literature comparing CEA and PCA as modalities of pain management following posterior fusion in adolescent scoliosis patients. In attempt to assess the comparability and acceptability of both pain relief methods, an objective evaluation of metrics related to the effectiveness and safety of both modalities was conducted. Patient demographics between cohorts were similar, however statistical significance emerged in the number of vertebral levels fused for the CEA cohort when compared to PCA (P = <0.01). Additionally, comparison of mean major cobb angles yielded a result nearing a significant difference (P=0.06). Though operative hours were not collected for the purposes of this study, these results warrant consideration for larger curves to potentially generate more challenging and lengthy surgical procedures. This could potentially impact a patient’s post operative recovery and the levels of pain experienced.
There were statistically significant differences observed in the time required to achieve post-operative efficacy outcomes (first defecation, return to diet, hospital discharge) between the two cohorts as per Table 5. Though the PCA protocol aims for the initiation of a solid diet on POD1 if tolerated, the statistically significant result (P<0.01) reflects the discretisation of time, indicating resumption of oral diet on POD2 for both cohorts. The prompt resumption of a full diet post-operatively is associated with benefits for wound healing and recovery, and an expedited recovery of gastrointestinal function. Whilst malnutrition is recognised to impede would healing and post-operative rehabilitation, the disparity in results between cohorts did not manifest in any patients presenting with chronic wound related concerns 16,17.
While postoperative nausea and vomiting could potentially limit the resumption of diet, pharmacological intervention was administered for all identified cases of PONV, possibly mitigating its impact on diet tolerance. The effectiveness of an accelerated discharge pathway for PCA patients is clearly demonstrated when examining days to discharge, revealing statistically significant differences between both cohorts. On average, patients who underwent PCA were discharged by day 3, compared to day 5 for CEA patients. Achieving earlier discharge is a shared goal for practitioners and healthcare facilities, particularly in light of escalating demands and pressures on hospitals and bed capacity. However, it is essential to acknowledge this accomplishment within the context of potential risks associated with readmission. Both cohorts had 6 readmissions, with no statistical significance between cohorts, suggesting that an accelerated discharge pathway does not increase the risk of readmissions. Other factors such as patient comorbidities, post-discharge care, and follow-up protocols may also influence readmission rates.
Table 5: Number of post-operative days required to achieve efficacy outcomes between cohorts (T tests), (mean (SD))
| Efficacy outcomes (days) | PCA | CEA | P Value comparing PCA and CEA |
|---|---|---|---|
| First defecation | 3.52 (1.38) | 4.47 (1.31) | <0.01 |
| Return to diet | 1.20 (0.46) | 1.68 (1.27) | <0.01 |
| Discharge from hospital* | 3.45 (1.15) | 5.36 (1.69) | <0.01 |
*The accelerated discharge pathway for PCA recommends discharge on POD3 (refer to appendix 1).
Similarly, enhanced recovery protocol for PCA patients encourages discharge on POD3, with no obligatory bowel motion required. As such, only 29 patients had a documented first day of defecation. Importantly, none of the 91 patients for PCA or 7 for CEA returned for reasons of constipation. When considering the early time to return to diet, in conjunction with recommended time to mobilization for this cohort, two factors acknowledged to expedite return to gastrointestinal (GI) function, including bowel function, it can be appreciated why this is not a discharge requirement. For patients who received CEA analgesia, there was preference for bowel motion prior to discharge, resulting in a statistically significant difference between cohorts. In some instances, the decision to discharge prior to a bowel motion was based on a comprehensive evaluation of the patient’s overall recovery status. As such, seven patients were discharged without a bowel motion in the CEA cohort. No patients across both cohorts were documented to have returned with concerns of post-operative ileus. Preference for a bowel motion prior to discharge is a consideration in the observed differences to discharge day from hospital.
Mean time to discharge was statistically significantly different between the cohorts, with a mean result of 5.36 (1.69) days for CEA patients compared to 3.45 (1.15) days for PCA patients. This result is appreciated to be influenced by not only preferences for bowel motions before discharge, but also the requirement of epidural catheters to remain in-situ until the morning of POD3. A review of the complication profile experienced between these cohorts, as per table 4, highlights the inherent risk profiles associated with each analgesic modality. In a separate review by the authors of the current study, a comprehensive assessment of the safety profile of epidural analgesia was conducted 11. Amongst the 83 patients who received an epidural, 26 patients experienced a temporary neurological change. Of this cohort, three patients experienced sensory changes, ten experienced a reduction in motor strength and thirteen patients experienced both motor and sensory changes. All cases of temporary neurological change resolved on the same day of detection, following temporary cessation or reduction in the rate of epidural infusion. Only one patient went on to receive MRI imaging which was normal and neurological changes had improved.
Given the innate differences between these analgesia methods, no PCA patients experienced temporary neurological changes, resulting in an expected statistically significant result (P<0.01). In contrast however, the opioid administration in the PCA method is associated with heightened sedation by inhibiting ascending nociceptive circuits, which also modulate arousal 13,18–20. Accordingly, it was expected that the PCA cohort exhibited a statistically higher incidence of sedation (Table 4, P <0.01). All instances of sedation related events were mild, and did not require medical intervention or escalation in the form a medical emergency team call. These incidents were resolved for all patients during their inpatient stay. Whilst constipation is a recognised GI effect of opioids, the lack of requirement for a bowel motion prior to discharge for the PCA patients complicates the accurate assessment of true constipation in this study. The occurrence of post operative nausea and vomiting was more prevalent in the PCA cohort compared to the CEA cohort, although not statistically significant. This was consistent with established opioid related side effects 18,19.
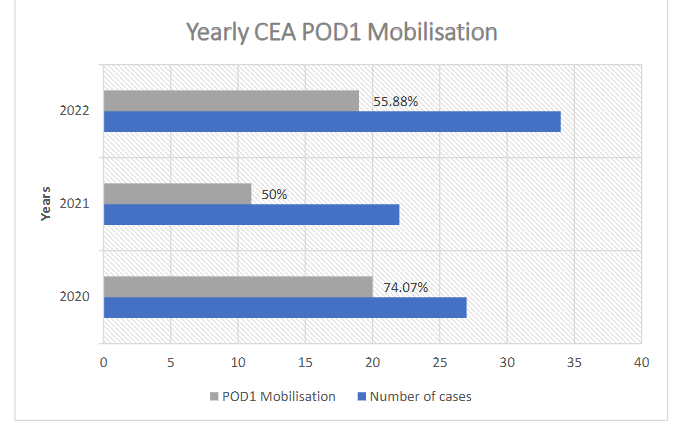
Statistical comparison of mobilisation between the PCA and CEA cohorts proved to be a challenge due to differing interpretations of mobility and mobilisation at each institution. As such, analysis was limited to any mobilisation that took place on postoperative day 1. Mobilisation is a crucial post-operative goal with established significance in preventing complications such as pressure sores, infections, constipation, pulmonary complications, venous stasis and deep venous thrombosis 21. It is also a valuable indicator of overall patient recovery and general health, and as such has become integral to many enhanced recovery programs that outline detailed mobilisation goals 22. Table 3 highlights a statistically significant disparity in mobilisation (P<0.05) between cohorts. A review of yearly mobilisation rates for CEA patients as per Figure 1 identified a fall of at least 18.19% from 2020 onwards. A retrospective audit exploring the adherence to clinical pathways for paediatric patients undergoing spinal fusion surgery at the same centre in 2023 identified reasons for delayed or prevented physiotherapy sessions, including patient distress, pain, unavailability, refusal or unavailability from family, nausea and vomiting, low blood pressure, staff shortages and the use of students and inexperienced staff 23. These finding highlight the importance and role of enhanced recovery pathways, which may help to manage patient and family expectations and improve adherence to post-operative goals for both staff and patients. Despite the disparity in mobilisation rates on POD1, no patients developed venous stasis resulting in deep venous thrombosis, there were no occurrences of pressure sores and all patients discharged with independent mobilisation. To uphold objectivity, statistical analysis of pain between the cohorts was omitted, given the potential for subjective variability in the reporting and recording of pain. This variability stemmed from the use of different pain scoring systems for data collection across the centres. One patient who received CEA required an operative washout for a surgical site infection, whereas two PCA patients underwent operative washouts for the same. A statistical analysis using Chi-squared yielded this a non-significant result (P=0.79). Comparison of respiratory depression did not show any statistically significant differences between the cohorts. Thus, despite a lower percentage of mobilisation for CEA patients on POD1, these patients did not experience any additional complications related to delayed mobilisation as acknowledged by the literature 24.
Conclusion
This study aimed to evaluate differences in efficacy and safety of continuous epidural analgesia compared to patient controlled analgesia following posterior instrumented fusion for adolescent idiopathic scoliosis. Data between cohorts from two separate hospital were compared, revealing that while both approaches are safe, they exhibit inherently varying complication profiles. Epidural analgesia is linked to temporary neurological changes and PCA analgesia has associations with opioid induced sedation and respiratory depression. Notable statistically significant differences were observed, particularly regarding efficacy outcomes, such as return to diet and discharge from hospital. Though this result may be influenced by the implementation of an accelerated discharge pathway, this underscores the importance of such pathways in optimizing patient care and recovery.
References
- J. Cobb, “Outline for the Study of Scoliosis,” Instructional Course Lectures, Vol. 5, 1948, pp. 261-275. – References – Scientific Research Publishing. Accessed April 15, 2024. https://www.scirp.org/reference/ReferencesPapers?ReferenceID=573326
- Kikanloo SR, Tarpada SP, Cho W. Etiology of Adolescent Idiopathic Scoliosis: A Literature Review. Asian Spine J. 2019;13(3):519. doi:10.31616/ASJ.2018.0096
- Dunn J, Henrikson NB, Morrison CC, Nguyen M, Blasi PR, Lin JS. Introduction. Published online 2018. Accessed October 31, 2023. https://www.ncbi.nlm.nih.gov/books/NBK493369/
- Maruyama T, Takeshita K. Surgical treatment of scoliosis: a review of techniques currently applied. Scoliosis. 2008;3(1). doi:10.1186/1748-7161-3-6
- Maruyama T, Takeshita K. Surgical treatment of scoliosis: a review of techniques currently applied. Scoliosis. 2008;3(1):6. doi:10.1186/1748-7161-3-6
- Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287. doi:10.2147/JPR.S144066
- Seki H, Ideno S, Ishihara T, Watanabe K, Matsumoto M, Morisaki H. Postoperative pain management in patients undergoing posterior spinal fusion for adolescent idiopathic scoliosis: A narrative review. Scoliosis Spinal Disord. 2018;13(1). doi:10.1186/s13013-018-0165-z
- Amaranath L, Andrish JT, Gurd AR, Weiker GG, Yoon H. Efficacy of intermittent epidural morphine following posterior spinal fusion in children and adolescents. Clin Orthop Relat Res. 1989;249:223-226. doi:10.1097/00003086-198912000-00024
- Motamed C. Clinical Update on Patient-Controlled Analgesia for Acute Postoperative Pain. Pharmacy 2022, Vol 10, Page 22. 2022;10(1):22. doi:10.3390/PHARMACY10010022
- Oliver J, Zeballos JL. Epidural Anesthesia. Essential Clinical Anesthesia Review: Keywords, Questions and Answers for the Boards. Published online March 9, 2022:190-191. doi:10.1017/CBO9781139584005.059
- Jamali MM, Moloney GE, Izatt MT, et al. A Retrospective Review of Continuous Epidural Analgesia Following Posterior Spinal Instrumented Fusion for Adolescent Idiopathic Scoliosis.; 2023.
- Prabhu PJ, Prabhu PJ. Epidural: Loss of Resistance. Epidural Administration – New Perspectives and Uses. Published online February 7, 2023. doi:10.5772/INTECHOPEN.109947
- Practice Guidelines for the Prevention, Detection, and Management of Respiratory Depression Associated with Neuraxial Opioid AdministrationAn Updated Report by the American Society of Anesthesiologists Task Force on Neuraxial Opioids and the American Society of Regional Anesthesia and Pain Medicine*. Anesthesiology. 2016;124(3):535-552. doi:10.1097/ALN.0000000000000975
- Christensen M, Jepsen OB. Epidural catheter infections. Journal of Hospital Infection. 2001;47(1):3-8. doi:10.1053/JHIN.2000.0872
- NT. INTERNATIONAL STANDARDS FOR NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY Movement.
- Fujii T, Morita H, Sutoh T, et al. Benefit of Oral Feeding as Early as One Day After Elective Surgery for Colorectal Cancer: Oral Feeding on First Versus Second Postoperative Day. Int Surg. 2014;99(3):211. doi:10.9738/INTSURG-D-13-00146.1
- Abela G. The potential benefits and harms of early feeding post-surgery: a literature review. Int Wound J. 2017;14(5):870-873. doi:10.1111/IWJ.12750
- Smith HS, Smith JM, Seidner P. Opioid-induced nausea and vomiting. Ann Palliat Med. 2012;1(2):12129-12129. doi:10.3978/J.ISSN.2224-5820.2012.07.08
- Opioid Toxicity and Withdrawal – Special Subjects – MSD Manual Professional Edition. Accessed December 11, 2023. https://www.msdmanuals.com/en-au/professional/special-subjects/illicit-drugs-and-intoxicants/opioid-toxicity-and-withdrawal
- Montandon G, Horner RL. Electrocortical changes associating sedation and respiratory depression by the opioid analgesic fentanyl. Scientific Reports 2019 9:1. 2019;9(1):1-11. doi:10.1038/s41598-019-50613-2
- Why is Ambulation Important to Recovery? – OakBend Medical Center. Accessed December 12, 2023. https://oakbendmedcenter.org/why-is-ambulation-important-to-recovery/#
- Jakobsen DH, Høgdall C, Seibæk L. Postoperative mobilization as an indicator for the quality of surgical nursing care. British Journal of Nursing. 2021;30(4):S4-S15. doi:10.12968/BJON.2021.30.4.S4/ASSET/IMAGES/LARGE/BJON.2021.30.4.S4_T04.JPEG
- Hudson A, Galluzzo L, Bundy R, Bruce R, Ullman A. Exploration of adherence to a clinical pathway for paediatric patients undergoing spinal fusion surgery: A retrospective audit.
- Pederson JL, Padwal RS, Warkentin LM, Holroyd-Leduc JM, Wagg A, Khadaroo RG. The impact of delayed mobilization on post-discharge outcomes after emergency abdominal surgery: A prospective cohort study in older patients. PLoS One. 2020;15(11). doi:10.1371/JOURNAL.PONE.0241554