

Knowledge and Practices on Mpox in Zimbabwe
Knowledge, Perceptions, and Preventive Practices on Mpox in Zimbabwe: Insights from districts with suspected and confirmed cases
Denford M. Chuma¹, Amos Milanzi², Naomi N. Wekwete ², Tatenda Songore³, Nokuphiwa Moyo³, James Munamati², Juliet T. Milanzi⁴, Lovemore Makurirofa²
- United Nations Children Fund (UNICEF)
- Department of Demography Settlement and Development, Faculty of Social and Behavioural Sciences, University of Zimbabwe
- Youth Advocates Zimbabwe
- Department of Mathematics and Computational Sciences, Faculty of Science, University of Zimbabwe
OPEN ACCESS
PUBLISHED: 31 December 2025
CITATION: Chuma, D.M., et al., 2025. Knowledge, Perceptions, and Preventive Practices on Mpox in Zimbabwe: Insights from districts with suspected and confirmed cases. Medical Research Archives, [online] 13(12).
https://doi.org/10.18103/mra.v13i12.7014
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i12.7014
ISSN 2375-1924
ABSTRACT
Background: The global Mpox outbreak remains a major health concern. Confirmed cases and deaths were reported in Africa between 2022 and 2024, with the Democratic Republic of the Congo, Burundi, and Uganda accounting for most cases. In Zimbabwe, 45 suspected and 2 confirmed cases have been recorded to date. Although Zimbabwe has recorded only two confirmed cases, the threat remains significant due to regional transmission and frequent cross-border movement. Addressing the Mpox outbreak at its early stage is therefore critical to preventing a potential health crisis.
Methods: The study employed a cross-sectional design with mixed data collection methods in three selected districts of Harare and Midlands Provinces, chosen due to their experience with Mpox cases. Quantitative data were collected through the questionnaire administered to 451 community members, and qualitative data were collected through 12 focus group discussions with community members and 10 key informant interviews with health officials, programme officers, youth officers, and a religious leader. Quantitative data were analysed using SPSS version. Content and thematic analyses were used to analyse qualitative information from the focus group discussions and key informant interviews.
Results: The study found that 70.1% of respondents had heard of Mpox, with higher awareness among those aged 40-49, married or cohabiting, rural residents, and university-educated individuals. Most of the respondents correctly identified close contact with infected persons (68.5%) and touching contaminated surfaces (53.7%) as key modes of transmission, and avoiding skin-to-skin contact (73.2 percent) as the main prevention measure. Other prevention practices mentioned included handwashing (64.5% and vaccination (63.2%). Misconceptions were common, including beliefs about transmission via blood, contaminated food or water, airborne spread, mosquito bites, and various myths (e.g., Mpox as untreatable, foreign-introduced, or affecting only people with HIV). Attitudes towards Mpox were generally negative; 47.7% reported open discussions about the disease in their communities. Vaccination hesitancy was notable (38.8 percent), driven by fear of side effects, misinformation, and mistrust in the health system. Almost half of the respondents (47.5%) had taken preventive measures, primarily hand hygiene. Most respondents recognised the importance of avoiding close contact with symptomatic individuals (94.4%), handwashing (64.5%), and not sharing personal items (86.9%). Seeking prompt care after exposure or symptom onset was reported by 78.5%.
Conclusion: The study found that while a significant proportion of people had heard about Mpox, community knowledge about its transmission was limited, with misconceptions about its transmission. There was considerable vaccine hesitancy. There is need to strengthen community-based health education by leveraging radio, social media, and mobile messaging platforms to promote correct practices and dispel misinformation about Mpox.
Keywords
Mpox, Zimbabwe, public health, vaccination, community awareness
Introduction
The global Mpox (formerly known as monkeypox) outbreak remains a significant health concern, with cases reported across multiple continents. In 1958, researchers in Denmark discovered the first incidence of the Mpox virus (MPXV) in a group of monkeys. Following that, in 1970, the MPXV, an orthopox Deoxyribonucleic Acid (DNA) virus that is zoonotic, was first discovered in humans in the Democratic Republic of the Congo. Subsequently, the disease became endemic throughout the West and Central Africa. Since then, in 2003, the first case of an Mpox infection was recorded in non-endemic nations, caused by an imported rodent from Ghana. Mpox cases were then recorded in the United Kingdom, Israel, and Singapore between 2018 and 2019. In May 2022, a significant number of Mpox cases were reported from nations with no known history of transmission, leading the World Health Organization (WHO) to declare the outbreak a public health emergency of international concern (PHEIC) on 23 July 2022.
Since 1 January 2022, Mpox cases have been reported to the WHO from 23 Member States across Africa. As of 3 November 2024, a total of 13,552 laboratory-confirmed cases, including 76 deaths, have been reported to WHO. The three countries with the majority of the cases in 2024 were the Democratic Republic of Congo (n = 8,662), Burundi (n = 1,726), and Uganda (n = 359).
A significant number of suspected Mpox cases that are clinically compatible with Mpox remain untested due to limited diagnostic capacity in most African countries and thus never get confirmed. The Mpox outbreak that occurred in 2022 was sporadic and had varying characteristics in comparison to its prior presentations, such as a prolonged incubation period (up to 21 days), occurrence of infections outside an endemic region, a high prevalence in males, sexual transmission, anogenital lesions, and the involvement of younger patients. In Zimbabwe, Mpox has not reached comparable levels in other countries, and as of December 2024, 45 suspected cases have been reported, with two confirmed cases, both with a history of recent travel to countries experiencing outbreaks, highlighting the ability of the virus to transcend borders in our interconnected world. Vigilance remains important due to the risk of cross-border spread and existing healthcare challenges.
Currently, the unexpected outbreak of Mpox has raised concerns for global health systems. While the world was still coping with the aftermath of the COVID-19 pandemic, it was hit with another wave of an infectious disease, spreading and threatening to become a pandemic. The emergence of a new infectious disease adds complexity to the global health crisis, requiring additional resources and attention.
Humans can contract Mpox by direct contact with infected animals, humans, and contaminated surfaces and materials (such as contaminated bedding, linens, towels, lesion dressings, or needles) and raw meat. Furthermore, it is possible that squirrels, prairie dogs, and rodents contributed to the spread of MPXV to humans. The recent discovery of MPXV transmission from humans to dogs underscores the importance of researching the dynamics of Mpox dissemination in depth.
Mpox is a self-limiting disease with a case fatality rate between 1% and 10%. Symptoms include fever, headache, back pain, myalgia, fatigue, lymphadenopathy, and a variety of skin lesions (including papules, pustules, and ulcers) on the face and body. The progression of this skin eruption includes the appearance of macules, papules, pustules, vesicles, and finally scabs. Lymphadenopathy appears to be one of the primary features that distinguish Mpox from smallpox.
The World Health Organization (WHO) declared that one of the largest challenges created by the pandemic is the lack of knowledge about Mpox in certain countries, particularly those impacted by the illness. A study conducted in Indonesia revealed that general practitioners, like other nations, particularly lower and middle-income countries, had minimal understanding of the Mpox virus. The major reason cited for the low levels of knowledge was that these countries have never seen an actual epidemic of this illness. However, higher levels of knowledge of Mpox were reported in Jordan among healthcare students, where 70.1% of the respondents had good knowledge and even higher levels in Nigeria among academics, tertiary students, and healthcare workers (99.1%). The most cited sources of information included social media (31.1%), newspapers and TV (29.0%), while the least cited was the radio (11.7%).
A study in Nigeria shows that most of the respondents reported that Mpox is transmitted through broken skin-skin contact (81.8%) and contact with infected bodily fluid (80.4%), consumption of inadequately cooked flesh of infected animals (58.3 percent), respiratory droplets (55.8%), contaminated clothing or linen (50.3%). The most cited ways to prevent Mpox infection were avoiding contact with animals suspected of having the disease or those that had died from it (89.3%), frequent handwashing with soap and water (80.4%), and thoroughly cooking all foods of animal origin.
There are numerous complications associated with Mpox, such as keratitis, paraphimosis, encephalitis, pneumonitis, myocarditis, conjunctivitis, and secondary bacterial infections. Children, pregnant women, and immunosuppressed individuals, particularly HIV-positive people, are at elevated risk for severe outcomes. Thus, vaccine acceptance among People Living with HIV (PLWH) is crucial for managing and mitigating the spread of infectious diseases, including Mpox. Currently, there is no MPXV-specific vaccine or drug available for use. Nevertheless, antiviral medications such as Cidofovir, Tecovirimat (TPOXX), Brincidofovir, and Vaccinia Immune Globulin Intravenous (VIGIV) have proven to be effective.
The Mpox infection cannot be cured with antibiotics; however, they may be used to manage and prevent secondary bacterial infections. The smallpox vaccine offers cross-protection against MPXV. While vaccines are crucial for eradicating infectious diseases like Mpox, recent reports have indicated that, in general, people are hesitant to be vaccinated in response to the current Mpox outbreak. Several reasons were cited for vaccine hesitancy, including fear of negative side effects, misinformation, and mistrust of medical staff or the healthcare system. Although vaccination remains one of the most effective public health interventions for preventing infectious diseases, the COVID-19 pandemic has seen a significant rise in vaccine hesitancy, often triggered by emerging information, new policies, or newly reported vaccine risks. Individuals who had not previously received other vaccines were at a higher risk of refusing to vaccinate against Mpox for themselves and for their children. However, high vaccination readiness can help mitigate this risk. Therefore, interventional education campaigns targeting populations at risk of vaccine hesitancy to combat misinformation and avoid low vaccination rates are needed urgently. When a new infectious disease is discovered, assessing knowledge and attitudes becomes essential. This fits with previous findings showing that misinformation about the dangers of an emerging infectious pathogen can increase anxiety, worry, and even the possibility of conspiratorial thinking. In addition, bridging knowledge gaps might be considered a crucial component for preventing an Mpox epidemic.
Understanding the current levels of knowledge and attitudes is critical to the development and implementation of an effective infection control strategy. To date, there is a dearth of literature on knowledge and attitudes towards Mpox in Zimbabwe. Thus, this study contends that, given the rapid spread of Mpox infection and its potential to escalate into an epidemic, further research is necessary. Zimbabwe’s health priorities, shaped by policies such as the National Health Strategy (2021-2025), focus on improving access to essential health care, including responses to infectious disease outbreaks. Zimbabwe confirmed its first two Mpox cases in October 2024: an 11-year-old boy in Harare and a 24-year-old male in Mberengwa. Both individuals had recently travelled outside the country; the boy to South Africa and the man to Tanzania. Although Zimbabwe has had only these two tracked cases, the threat remains real, especially given regional transmission and cross-border movement. Addressing the Mpox outbreak in its infancy aligns with these priorities by strengthening surveillance and integrating response efforts into the broader health framework for managing infectious diseases. Risk Communication and Community Engagement (RCCE) is crucial in responding to the Mpox outbreak, especially in districts potentially exposed through travel or trade corridors. The WHO developed the Surveillance, case investigation and contact tracing for Mpox guideline. The overall goal of continued Mpox surveillance, case investigation, and contact tracing is to detect new outbreaks and stop transmission to contain the global outbreak, protect people at risk in endemic and new settings, and make progress towards elimination of human-to-human transmission. Effective RCCE strategies help communities understand the symptoms, transmission, and prevention methods, thereby reducing stigma and encouraging individuals to seek care. Integrating RCCE with traditional public health measures, such as vaccination and contact tracing, can enhance the response effectiveness by building trust and ensuring that the public actively participates in prevention efforts. This study aimed to gather information on knowledge, perceptions, and practices related to Mpox across the selected districts in Zimbabwe.
Methods
The study used a cross-sectional design and mixed methods for data collection. Data were systematically collected through structured questionnaires that measured various dimensions of Mpox knowledge, perceptions, and prevention practices. This approach facilitated a comprehensive understanding of the Mpox landscape among the target population. The targeted population included children from 8 years old to older people up to 82 years. The provinces were chosen because they were affected by the Mpox outbreak. The study was conducted in two provinces, Harare and Midlands, covering three project districts, namely Harare, Mberengwa and Kwekwe districts. A stratified random sampling technique was implemented to ensure adequate representation from diverse geographic contexts, specifically in Harare, Mberengwa and Kwekwe. The survey was used to collect data from randomly selected individual community members, with 451 questionnaires administered. The survey sample size was calculated using a 5% margin of error, 95% confidence level, 50% response distribution and a population of 2,375,000 community members in the three districts (Zimbabwe National Statistics Agency, 2022). Twelve focus group discussions (FGDs) were conducted with purposively selected community members, including children, young women, young men, older women and older men, until saturation was reached. Ten purposively selected key informant interviews (KIIs) were conducted with one District Medical Officer, one District Nursing Officer, one District Environmental Health Officer, one community nurse, one Nutritionist, one Jointed Hands Welfare Organization (JHWO) Programs Officer, two Youth Officers, and one religious leader.
Data analysis was performed using SPSS version 25.0. Quantitative survey data was collected through electronic devices running CSEntry 7.6.0. During fieldwork, data was electronically transmitted to team leaders at the end of each day for review. Team leaders provided summary feedback on any emerging issues, ensuring data quality before it was securely stored in an online CSEntry database. Data cleaning was performed using frequency analysis to identify and correct inconsistencies. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were computed. Additionally, first-order analyses, such as chi-square tests (p-values), were conducted to assess statistical significance. Content and thematic analyses were used to analyse qualitative information obtained from FGDs and KIIs.
ETHICAL CONSIDERATIONS
The study adhered to Institutional Research Ethics and the Declaration of Helsinki. This research was assessed and approved by the Department of Demography Settlement and Development Ethics Review Committee, in accordance with the ethical principles of respect for persons, beneficence, and justice. No subjects were interviewed without their informed verbal consent/assent. Participants aged 18 years and above signed a consent form, while guardians of participants aged 8-17 years signed the parental consent form. The children aged 8-17 years also provided verbal consent. Interviewers received thorough training in human subjects protection, with particular emphasis on safeguarding privacy and confidentiality. No personally identifying information was collected. Respondents were informed that they were allowed to skip questions or to stop the interview altogether if they wished to do so. Respondents were provided with the contact details of the Ministry of Health and Child Care (MoHCC), which served as an independent resource to address any questions, concerns, or problems related to their participation in the study. In the case of a medical emergency during the study, respondents were referred to the nearest public health facility.
Results
DEMOGRAPHIC CHARACTERISTICS OF THE PARTICIPANTS
The participants ranged in age from 8 to 82 years old, with adolescents under 19 years constituting the largest proportion (37.3%). The participants had an average age of 29 years, with a minimum of 8 years, a median of 25 years, and a maximum of 82 years. (Not shown in Table 1). The majority of the participants were females (66.1%). Most participants identified themselves as Christians (83.8%), while Islam (0.4%) and African Tradition (1.8%) were the least reported. The majority of respondents were never married (51.7%), followed by those who were married or cohabiting (36.4%). Most participants reported having some secondary education (35.5%), 24.6% had completed secondary school, and 12% were attending college. More than half of the participants (61.4%) reported residing in urban areas, while 38.6% lived in rural areas. Harare had the highest percentage of participants (41.5%), followed by Mberengwa (34.8%) and Kwekwe (23.7%) (Table 1).
| Demographic Characteristic | Percent | Number | |
|---|---|---|---|
| Sex | Male | 33.9 | 153 |
| Female | 66.1 | 298 | |
| Age | 8-19 | 37.3 | 168 |
| 20-29 | 21.3 | 96 | |
| 30-39 | 16.0 | 72 | |
| 40-49 | 12.9 | 58 | |
| 50-59 | 8.2 | 37 | |
| Over 60 | 4.4 | 20 | |
| Marital Status | Married/Cohabiting | 36.4 | 164 |
| Never Married | 51.7 | 233 | |
| Widowed | 5.5 | 25 | |
| Divorced | 4.2 | 19 | |
| Separated | 2.2 | 10 | |
| Religion | Islam | 0.4 | 2 |
| African Tradition | 1.8 | 12 | |
| Apostolic Sect | 11.1 | 50 | |
| Christianity | 83.8 | 378 | |
| None | 2.7 | 12 | |
| No response | 0.2 | 1 | |
| Level of education | No education | 1.8 | 8 |
| Some Primary | 10.2 | 46 | |
| Completed Primary | 4.7 | 21 | |
| Some Secondary | 35.5 | 160 | |
| Completed Secondary | 24.6 | 111 | |
| College | 12.0 | 54 | |
| University | 9.5 | 43 | |
| Don’t know | 0.4 | 2 | |
| Other | 1.3 | 6 | |
| Residence | Rural | 38.6 | 174 |
| Urban | 61.4 | 277 | |
| District | Harare | 41.5 | 187 |
| Mberengwa | 34.8 | 157 | |
| Kwekwe | 23.7 | 107 | |
| Total | 100 | 451 |
KNOWLEDGE ABOUT Mpox
Table 2 shows participants awareness of Mpox by demographic characteristics. Overall, less than three-quarters (70.1%) of the participants had heard about Mpox. Participants aged 40 to 49 years were more likely to have heard about Mpox (86.2%) compared to other age groups (p=0.004). A higher proportion of participants who were married or cohabiting (82.3%) reported having heard about Mpox compared to other marital statuses (p=0.001). Participants from rural areas were more likely to have heard about Mpox (90.8%) compared to those from urban areas (57%) (p<0.0001). Participants who had attained university level were more likely to have heard about Mpox (83.7%) compared to other levels of educational attainment (p=0.02). A significantly higher proportion of participants from Mberengwa District (96.8%) reported having heard about Mpox compared to other districts (p=0.001).
| Ever heard about Mpox | Demographic Characteristic | Yes(%) | N | P-value |
|---|---|---|---|---|
| Sex | Male | 69.9 | 153 | 0.97 |
| Female | 70.1 | 298 | ||
| Age | 8-19 | 61.3 | 168 | 0.004* |
| 20-29 | 66.7 | 96 | ||
| 30-39 | 75.0 | 72 | ||
| 40-49 | 86.2 | 58 | ||
| 50-59 | 81.1 | 37 | ||
| Over 60 | 75.0 | 20 | ||
| Marital Status | Married/Cohabiting | 82.3 | 164 | 0.001** |
| Never Married | 63.5 | 233 | ||
| Widowed | 60.0 | 25 | ||
| Divorced | 68.4 | 19 | ||
| Separated | 50.0 | 10 | ||
| Religion | Islam | 100 | 2 | 0.02* |
| Christianity | 72.0 | 378 | ||
| Apostolic Sect | 58.0 | 50 | ||
| African Traditional | 25.0 | 8 | ||
| None | 83.3 | 12 | ||
| No response | 100 | 1 | ||
| Level of education | No education | 100 | 8 | 0.02* |
| Some Primary | 63.0 | 46 | ||
| Completed Primary | 76.2 | 21 | ||
| Some Secondary | 61.9 | 160 | ||
| Completed Secondary | 70.3 | 111 | ||
| College | 77.8 | 54 | ||
| University | 83.7 | 43 | ||
| 100 | 2 | |||
| Other | 100 | 6 | ||
| Residence | Rural | 90.8 | 174 | 0.0001*** |
| Urban | 57.0 | 277 | ||
| District | Harare | 51.3 | 186 | 0.0001*** |
| Mberengwa | 96.8 | 157 | ||
| Kwekwe | 63.6 | 107 | ||
| Overall | 70.1 | 316 |
The findings on participants awareness of Mpox concur with findings from qualitative FGDs and KIIs. When asked about whether they had ever heard about Mpox, one participant in an FGD in Harare, with confirmation from others, had this to say: We have heard about Mpox, formerly known as monkeypox, which is a viral disease that has garnered increased attention in recent years. While it was traditionally endemic to certain regions of Central and West Africa, there have been significant outbreaks and reports in various parts of the world, including North African countries.
However, it is noteworthy that some of the respondents had never heard of Mpox. One participant in an FGD in Harare, with confirmation from others, had this to say: We have never heard of Mpox in Zimbabwe before; this is a new disease that we are just now learning about. The sudden emergence of Mpox has caught many in our community by surprise, as we were previously unaware of its existence or potential impact.
District health executive members also acknowledged being aware of Mpox, as remarked by the Mberengwa District Nursing Officer during a key informant interview: Yes, I have heard that Mpox is a disease that is spread through close contact with infected people and sharing clothes or linen with them. Generally, the community had limited knowledge about how Mpox spreads. Most of the participants mentioned close contact with an individual who has Mpox (68.5%) and touching contaminated surfaces (53.7%) as the primary mode of transmission. Participants also exhibited misconceptions and knowledge gaps regarding other potential transmission routes, including blood contamination (36.4%), unsafe food practices such as consuming contaminated food (27.1%), and exposure to contaminated water (21.3%) (Table 3).
| Mode of Spread of Mpox | Percent | Number |
|---|---|---|
| Through contaminated water | 21.3 | 96 |
| Through close contact with someone who has mpox | 68.5 | 309 |
| Through blood contamination | 36.4 | 164 |
| Through mosquito bites | 18.2 | 82 |
| Contact with faeces | 28.2 | 127 |
| Eating contaminated food | 27.1 | 122 |
| Touching contaminated surfaces | 53.7 | 242 |
| Eating from the same plate | 43.0 | 194 |
| Dirty hands | 32.6 | 147 |
| Air/breeze | 37.3 | 168 |
| I don’t know | 26.2 | 118 |
| No answer | 17.1 | 77 |
The quantitative findings concur with the qualitative findings. When asked how Mpox spreads, one participant in an FGD in Harare, with confirmation from others, remarked: Mpox is primarily spread through direct contact with individuals who are infected with the Mpox virus. The most significant mode of transmission is through direct skin contact with the lesions or rashes of an infected person. These lesions can be found on various parts of the body, including the face, hands, and other exposed areas. Touching these lesions can introduce the virus into the body, especially if there are any cuts or abrasions on the skin.
District health executive members also acknowledged that they had heard about Mpox, as remarked by the Mberengwa District Nursing Officer in a key informant interview, who shared these remarks: Mpox is primarily spread through direct contact with individuals who are infected with the Mpox virus. Understanding the specific ways in which this contact occurs is crucial for effective prevention and control measures. One of the most common ways Mpox is transmitted is through direct skin contact with an infected person. This can happen when touching the lesions or rashes that develop on the skin of an infected individual. The virus can enter the body through broken skin, mucous membranes, or even intact skin in some cases. The virus can also be present in the bodily fluids of an infected person, such as saliva, blood, or pus from skin lesions. Activities that involve contact with these fluids, such as caring for an infected person or engaging in sexual activity, can facilitate transmission through contact with the infected person.
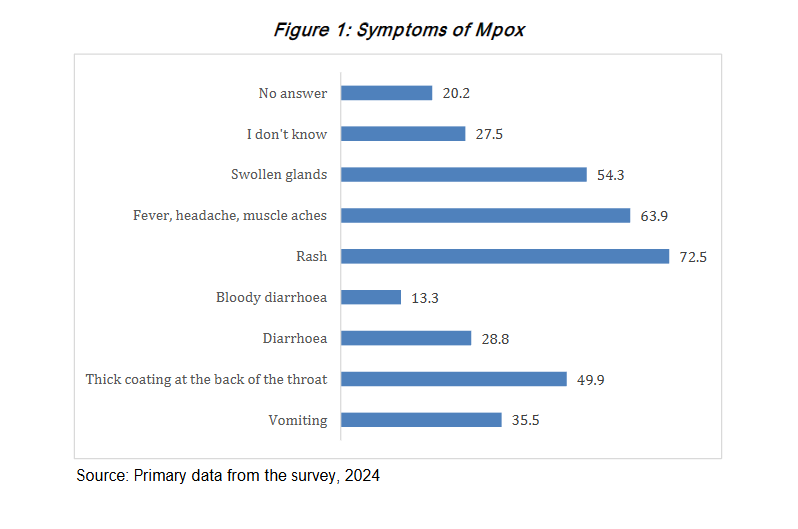
Figure 1 shows that the majority of participants (72.5%) identified rash as the major symptom associated with Mpox, followed by fever, head and muscle aches (63.9%), swollen glands (54.3%), and thick coating at the back of the throat (49.9%). However, 27.5% of the participants were unaware of the symptoms.
While it is imperative to note that the discussants demonstrated that they were not familiar with the majority of the symptoms, when asked about symptoms of Mpox, one participant in an FGD in Mberengwa, with support from others, remarked: Mpox is characterized by a distinctive rash that can include blisters, which may resemble the rash seen in chickenpox. This was further explained by the District Environmental Health Officer for Mberengwa in a key informant interview, who shared these remarks: The Mpox rash typically begins with flat, red spots known as macules. As the infection progresses, these spots can evolve into raised bumps (papules). Following the papule stage, these bumps may fill with fluid, forming blisters (vesicles). These blisters are often painful or itchy and can vary in size. After blistering, the lesions can develop into pustules, which are similar to those seen in chickenpox. Pustules are characterized by a raised, inflamed appearance filled with pus. Eventually, the pustules crust over and form scabs as they heal. This progression from macules to papules to blisters and pustules can take several days. This was further explained by the District Nursing Officer for Mberengwa in a key informant interview, who shared these remarks: Before the rash appears, individuals with Mpox may experience flu-like symptoms, including fever, headache, muscle aches, and swollen lymph nodes. This is similar to the prodromal phase of chickenpox, where individuals may feel unwell before the rash develops. The overall duration of Mpox can be longer than that of chickenpox. While chickenpox typically resolves within a week or two, Mpox can take several weeks for the rash to heal completely.
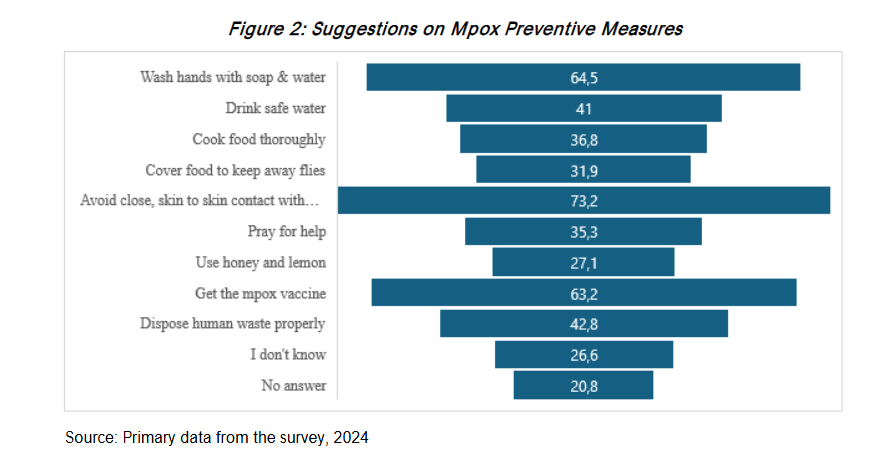
Figure 2 illustrates suggested measures for preventing Mpox. The majority of participants (73.2%) reported that avoiding close, skin-to-skin contact with individuals exhibiting Mpox-like symptoms was the primary method of prevention, followed by handwashing with soap and water (64.5%) and receiving the Mpox vaccination (63.2%). The least mentioned measures were disposing of human waste properly (42.8%) and cooking food thoroughly (36.8%). However, 26.6% of participants reported being unaware of how to prevent Mpox, and some held misconceptions, including the use of lemon and honey (27.1%) and praying for help (3.3%). When asked about how Mpox can be prevented, one participant in an FGD in Kwekwe, with support from others, remarked: Preventing the spread of Mpox relies heavily on minimizing close physical interactions with those who are infected or showing symptoms. Mpox is transmitted primarily through direct contact with an infected person. This includes touching the skin lesions, rashes, or any bodily fluids from the infected individual, which can harbour the virus. Close physical contact increases the risk of transmission, highlighting the importance of maintaining distance. This was further explained by the District Nursing Officer for Mberengwa in a key informant interview, who shared these remarks: People exhibiting symptoms of Mpox, such as fever, swollen lymph nodes, and the characteristic rash, are particularly contagious. The rash often develops into lesions that can leak fluid, further increasing the risk of spreading the virus through direct contact.
The majority of the participants suggested avoiding close, skin-to-skin contact with a person infected with Mpox as the major preventive measure (73.2%). Other major preventive measures cited were washing hands with soap and water (64.5%) and getting the Mpox vaccine (63.2%). See Figure 2.
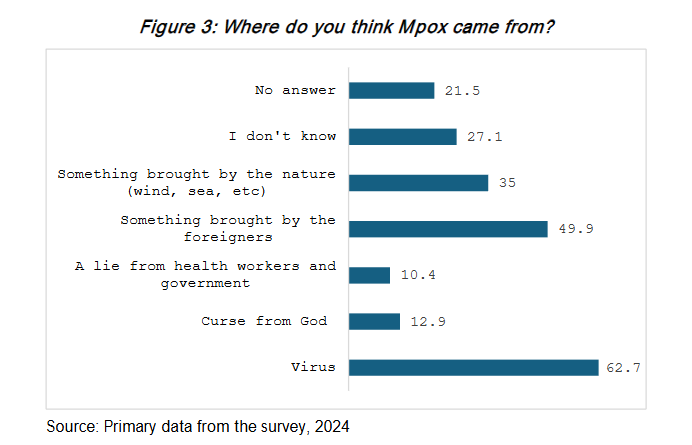
Figure 3 shows that the majority of participants perceived that Mpox came from a virus (62.7%). However, half of the participants believed that it was something brought by foreigners (49.9%), something brought by nature (wind, sea, etc.) (35%), and a curse from God (12.9%).
When asked about the origin of Mpox, one participant in an FGD in Kwekwe, with support from others, remarked: This is a virus brought by people coming from outside the country, particularly from North Africa. The emergence and spread of certain viruses, such as Mpox, can often be linked to international travel and migration patterns. Other respondents were not aware of the origin of Mpox. When asked the question Where do you think Mpox came from?, one participant in an FGD in Mberengwa, with support from others, remarked: We really don’t know where these diseases are coming from, maybe it’s a curse from the ancestors, or it’s a gimmick from the former colonialists.
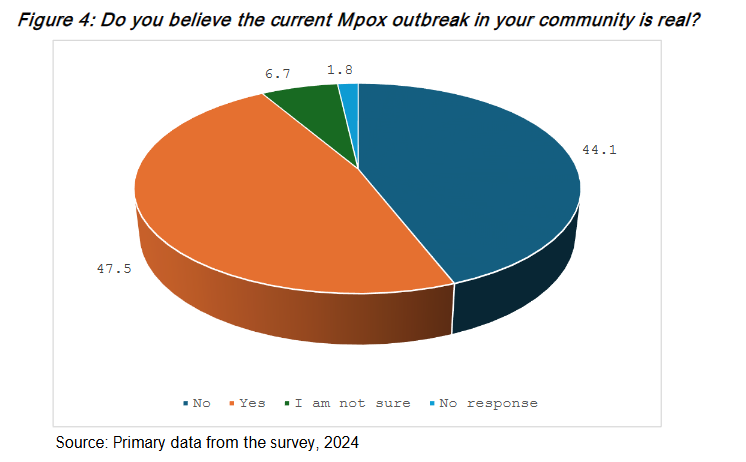
Figure 4 shows that 47.5% of participants believed the current Mpox outbreak was real, 44% did not believe in its existence, and approximately 6.7% were uncertain about their stance.
When asked if the respondents believed the current Mpox outbreak in the community was real, one participant in an FGD in Harare, with support from others, remarked: The Mpox outbreak is real, and we need to prepare ourselves to deal with it before it goes out of control like COVID-19. The emergence of Mpox as a public health concern cannot be underestimated. As we have learned from the COVID-19 pandemic, timely and effective preparation is crucial to controlling the spread of infectious diseases.
However, some sectors of the community were doubtful about the reality of Mpox, as one participant in an FGD in Kwekwe remarked, with support from others: We don’t know what to believe anymore, some of the diseases are not real, particularly the Mpox. It’s a business for companies which produce vaccines.
| If you do believe the Mpox outbreak is real, who or what do you think caused the Mpox outbreak | Percent | Number |
|---|---|---|
| Foreigners and travellers | 19.3 | 57 |
| Cross boarders | 15.3 | 45 |
| Monkeys | 10.8 | 32 |
| Migration from affected areas | 10.5 | 31 |
| Lack of awareness and knowledge | 2.7 | 8 |
| Virus | 3.4 | 10 |
| Poor hygiene and isolation | 3.4 | 10 |
| Overpopulation | 0.7 | 2 |
| I don’t know | 22.2 | 38 |
A follow-up question was asked of respondents who indicated that Mpox was real, regarding their views on the causes of the disease. One participant in an FGD in Harare, with support from others, remarked: Foreigners and individuals who travel abroad are significant vectors for introducing the Mpox virus into our communities. As international travel increases, so does the risk of infectious diseases being imported from regions where Mpox is endemic. Travellers returning from affected areas may unknowingly carry the virus, contributing to local outbreaks.
However, some respondents did not know the cause of the Mpox outbreak, as one participant in an FGD in Mberengwa remarked, with support from others: We believe that the disease is real and poses a genuine threat to our community, yet we remain uncertain about the specific factors that triggered the outbreak. There is a collective concern regarding the origins of the disease, whether it stems from environmental changes, increased human-animal interaction, or other underlying issues.
| If you do not believe the Mpox outbreak is real, why do you think people (organisations, media, government) are talking about it? | Reasons for talking about Mpox | Percent | Number |
|---|---|---|---|
| To create fear | 34.6 | 54 | |
| Fake news | 19.9 | 31 | |
| To make money (Mpox business) | 14.7 | 23 | |
| To oppress a certain group/community | 14.7 | 23 | |
| For political purposes/gains | 13.5 | 21 | |
| I don’t know | 37.2 | 58 | |
| No response | 21.2 | 33 |
Nearly half of the participants (46.8%) were highly concerned about the risk of Mpox infection, while 18.2% were moderately concerned, and 12.2% reported no concern at all.
When asked about how concerned they were about becoming infected and sick from Mpox, one participant in an FGD in Mberengwa, with support from others, remarked: We lack the capacity to effectively manage some of these health conditions, which poses a significant challenge for our community. When individuals are affected by diseases like Mpox, the limited resources and infrastructure can lead to devastating consequences. Without adequate healthcare facilities, trained personnel, and access to treatment, many patients may not receive the care they need in a timely manner. This can result in severe health deterioration, increased transmission rates, and higher mortality rates.
Under half of the participants (47.7%) reported that people in their community spoke openly about Mpox and did not feel any shame, 34.4% of participants reported not speaking openly about the disease, and 15.7% were unsure of the reason. When asked whether people easily talked about Mpox or feel any shame associated with, one participant in an FGD in Kwekwe, with support from others, remarked: Yes, we speak openly about Mpox without feeling any shame, recognising the importance of transparency in addressing health issues. Open dialogue allows us to share experiences, knowledge, and concerns, fostering a supportive environment. However, it is imperative to note that some members of the community were very secretive about their lives. One participant in an FGD in Harare, with support from others, remarked: We don’t share our private lives with the community, even in discussions about Mpox, due to a variety of reasons rooted in cultural norms.

Figure 5 shows the reasons why people spoke openly about Mpox in their communities. The majority of the respondents (36.7%) mentioned awareness and education about the disease, and 10.7% mentioned preventing further spread of the disease. Participants also reported fear of the disease (18.1%) and fear of death (12.6%).
When asked why people did not easily talk about Mpox in their community, one participant in an FGD in Mberengwa, with support from others, remarked: Community conversations also provide an opportunity to highlight the importance of seeking medical attention if symptoms arise or if individuals believe they have been exposed to the virus. When we discuss Mpox openly, we empower others to take proactive steps in protecting their health and the health of their families.
Table 6 shows that sex workers (57.2 percent), LGBTQ+ groups (53.2%) and children (52.8%) were perceived to be most likely to transmit Mpox. People living with immunodeficiencies (65.9%) were perceived to be the most at risk if they got infected by Mpox, followed by children (65.2%), sex workers (64.3%) and pregnant women (57.6%).
| Who do you think is most likely to transmit Mpox? | Who is most at risk if they get infected? | Percent | Number |
|---|---|---|---|
| People living with immunodeficiencies | 65.9 | 297 | |
| Children | 65.2 | 294 | |
| Pregnant women | 57.6 | 260 | |
| Sex Workers | 64.3 | 290 | |
| LGBTQ+ groups | 59 | 266 | |
| I am not sure | 25.3 | 114 | |
| No answer | 18 | 81 |
When asked about who they thought was most likely to transmit Mpox and who would be at greatest risk if infected, one participant in a Harare FGD, supported by others, remarked: While we do not have sufficient information to fully address the dynamics of Mpox transmission, there is a growing concern that sex workers may be at a higher risk of transmitting the virus. This stems from the nature of their work, which often involves close physical contact with multiple partners, increasing the likelihood of exposure to infectious diseases. Furthermore, vulnerable populations such as children and individuals living with immunodeficiencies are particularly at risk if they contract Mpox. Their developing or weakened immune systems make it more challenging for them to fight off infections, leading to potentially severe health complications.
Regarding main rumours or beliefs, concerns, and questions in their community about Mpox, participants reported that Mpox was often perceived as a deadly disease, with some believing that it could not be treated. Other participants believed Mpox was the same as COVID-19 and could be treated using traditional herbs and methods, such as steaming. Some participants also reported misconceptions, such as believing Mpox only affected people with HIV, was caused by poor hygiene, or was a foreign disease introduced by foreigners and cross-border traders. Participants reported that Mpox could also be caused by consuming wild animals such as monkeys and baboons, and noted that it commonly affects young children.
Prevention Practices of Mpox
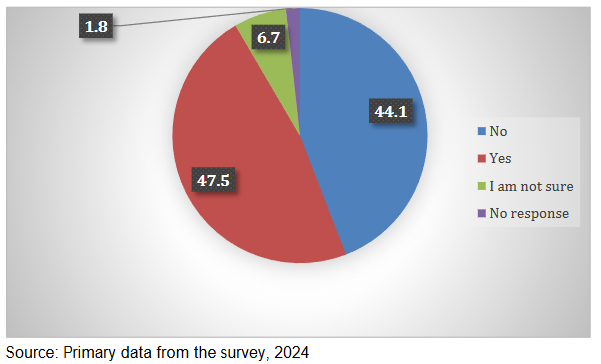
Figure 6 shows whether individuals had taken any preventive measures to protect themselves from Mpox. Almost half (47.5%) of the participants had taken preventive measures.
When asked if the respondents had taken any preventive measures to protect themselves from Mpox, one participant in an FGD in Harare, with support from others, remarked: We are making every effort to implement preventive measures to protect ourselves from Mpox, with hand hygiene being the most practised measure. Hand hygiene plays a crucial role in preventing the transmission of infectious diseases, including Mpox. Regularly washing our hands with soap and water or using alcohol-based hand sanitizers helps eliminate germs and viruses that may be present on our hands. This simple yet effective practice is particularly crucial after touching potentially contaminated surfaces or having contact with infected individuals.
However, it is also important to note that other respondents were not engaging in any protective practices. When asked if the respondents had taken any preventive measures to protect themselves from Mpox, one participant in an FGD in Kwekwe, with support from others, remarked: We are currently not taking any preventive measures to protect ourselves because we do not fully understand some of these diseases. This lack of understanding can lead to confusion and uncertainty about how the virus spreads and what steps are necessary to reduce our risk of infection.
| Mpox Preventive Measures Taken | Percent | Number |
|---|---|---|
| Washing your hands with soap and water more regularly | 91.1 | 195 |
| Avoiding skin-to-skin/close contact with people with mpox-like symptoms | 94.4 | 202 |
| Not sharing personal or other objects touched by people with mpox-like symptoms | 86.9 | 186 |
| Getting the mpox vaccine | 38.8 | 83 |
| Isolating myself or family members with mpox-like symptoms | 75.7 | 162 |
| Checking on myself and my family members (especially children) to ensure they are not experiencing any symptoms. | 79.0 | 169 |
| Ensuring that my children are informed on how to protect themselves from mpox | 72.0 | 154 |
| Ensuring that my children know they should not have physical contact with other children if these have mpox like symptoms. | 72.9 | 156 |
| Seek/go to the health centre after suspicious symptoms and/or contact with people with mpox symptoms | 78.5 | 168 |
| I don’t know | 17.3 | 37 |
| No response | 18.2 | 39 |
When asked about the preventive measures taken to protect from Mpox, one participant in an FGD in Mberengwa, with support from others, remarked: Regular handwashing is one of the most effective preventive measures against infectious diseases, including Mpox. By washing your hands frequently with soap and water, you can significantly reduce the risk of transmitting viruses and bacteria. This practice is important after using the bathroom, before eating, after coughing or sneezing, and after contact with shared surfaces. Using an alcohol-based hand sanitizer can be an effective alternative.
This was supported by the District Nursing Officer for Mberengwa in a key informant interview, who shared these remarks: Avoiding close physical contact with individuals who exhibit symptoms similar to Mpox is crucial for preventing the spread of the virus. This includes recognizing symptoms such as fever, swollen lymph nodes, and a distinctive rash that progresses to lesions. Being aware of these signs can help you make informed decisions about interactions. Keeping a safe distance from those who are symptomatic minimizes the risk of transmission through direct contact or respiratory droplets. Limiting physical interaction, such as avoiding hugs, handshakes, or any other form of close interaction, is essential until the individual has been evaluated and cleared by a healthcare provider.
However, most respondents were very reluctant to get the Mpox vaccination. One participant in an FGD in Kwekwe, with support from others, remarked: The risk of contracting Mpox is low, especially with the few cases reported in our area and country at large. This does not necessitate vaccination, and public concerns about surrounding COVID-19 vaccines, there is no need to rush into vaccination.
Discussion
This section sequentially discusses the knowledge, perceptions, and prevention practices on Mpox.
KNOWLEDGE OF Mpox
Assessing knowledge levels about Mpox was an important objective and a critical variable of this study. The study revealed that 70.1% of the respondents had heard about Mpox. This is comparable with the 70% good knowledge found among Jordanian healthcare students, but lower than the 99.1% observed in a study involving academics, tertiary students, and healthcare workers in Nigeria. The notably higher knowledge levels in the Nigerian study may be attributed to the participants higher educational attainment compared to those in other settings. However, the 70.1% knowledge is higher than 48 percent among the general population in Saudi Arabia and a minimal understanding of the Mpox in Indonesia. In this current study, participants aged 40-49, married or cohabiting, rural residents, and those with a university education were more likely to be aware of Mpox. Interestingly, participants from rural areas were more likely to have heard about Mpox (90.8%) than those from urban areas (57%). This may be because one of the reported cases was from Mberengwa, a rural area, prompting health workers to intensify awareness efforts in those communities to prevent further infections. Participants who had attained university-level education were more likely to have heard about Mpox (83.7%) compared to other levels of educational attainment. This implies that communities with lower levels of education will be at risk of contracting Mpox, delayed recognition of symptoms, and poor adoption of preventive behaviours. This can be addressed by continuous awareness and advocacy about the disease through various media platforms such as social media, radio, community health workers and other appropriate channels within the communities.
Participants correctly identified close contact with infected individuals (68.5%) and touching contaminated surfaces (53.7%) as the main transmission routes. The majority of the participants (73.2%) reported that avoiding close, skin-to-skin contact with people with Mpox-like symptoms was the major way to prevent illness with Mpox. Qualitative interviews emphasized direct skin contact with lesions as a key mode of Mpox transmission, with healthcare workers providing detailed biomedical explanations. Skin-to-skin contact was also mostly cited as the major mode of transmission in other similar studies. Other prevention measures included handwashing with soap and water and receiving the Mpox vaccination. Knowledge of Mpox transmission is crucial, as individuals with accurate information are more likely to adopt recommended preventive measures. Adequate knowledge also facilitates early recognition of signs and symptoms, enabling timely medical attention and ultimately reducing both the severity of illness and the potential spread of the disease.
However, the study revealed that misconceptions were common among the participants regarding transmission via blood (36.4 percent), contaminated food (27.1%), and contaminated water (21.3%). Airborne transmission and mosquito bites were also mentioned. Some participants believed that Mpox is a deadly or untreatable disease, while others thought it is similar to COVID-19 and can be treated with traditional herbs or steam therapy. Some believed that it is a foreign disease, introduced by foreigners or cross-border traders, and others thought it only affects people living with HIV or is caused by poor hygiene. In addition, more than a fifth of the respondents (26.6%) reported being unaware of how to prevent Mpox, and some held misconceptions. Misconceptions may lead individuals to underestimate their risk of Mpox infection or rely on ineffective prevention methods, increasing vulnerability to infection. In addition, people who hold incorrect beliefs may not recognise symptoms early or may resort to inappropriate remedies, leading to delayed diagnosis and treatment. Communities with limited understanding may inadvertently spread misinformation, complicating outbreak control and surveillance, and undermining public health communication efforts. The presence of misconceptions highlights gaps in current health education strategies, hence the need for more tailored, culturally appropriate, and accessible awareness campaigns.
PERCEPTIONS OF Mpox
The study aimed to assess the perception of Mpox within the selected districts affected by Mpox in Zimbabwe. The findings revealed that 47.5 percent believed the current Mpox outbreak was real, 44 percent of the participants did not believe in its existence, and approximately 6.7 percent were uncertain about their stance. Of the participants who did not believe Mpox was real, 34.6 percent believed reports and awareness programmes about Mpox were intended to instil fear, while 19.9 percent considered it to be fake news. However, a remark from one of the key informants highlighted that the Mpox outbreak is real and that everyone should be prepared to respond appropriately to avoid a repeat of the COVID-19 experience. The emergence of Mpox as a public health concern should not be underestimated; therefore, timely and effective preparedness measures are essential to ensure the disease is controlled should it re-emerge.
The findings revealed negative attitudes towards Mpox. The study revealed that slightly under half of the participants (47.7 percent) reported that people in their community spoke openly about Mpox, 34.4 percent reported that they did not speak openly about the disease, and 15 percent were unsure why. This aligns with a previous study in Nigeria, which reported negative perceptions of Mpox. The negative perception about Mpox found among the respondents, who are in the community and are in the best position to flatten the epidemiological curve of the disease, is a global public health risk. This is because the necessary steps and basic precautionary measures needed to limit the transmission of the diseases may be discarded, leading to increased national spread.
The participants believed that the causes of the Mpox outbreak were foreigners and travellers (19.3%), crossing borders (15.3%), close contact with an infected person (11.5%), monkeys (10.8%), and migration from affected areas (10.5%). They believed that foreigners and individuals who travel abroad were significant drivers of spreading the Mpox virus into their communities. Their belief is understandable, as the two Mpox cases reported in Zimbabwe had a history of recent travel outside the country. Travellers returning from affected areas may unknowingly carry the virus, contributing to local outbreaks.
Mpox PREVENTION PRACTICES
The study aimed to assess Mpox practices within the selected districts affected by Mpox in Zimbabwe. The findings show that almost half (47.5 percent) of the participants had taken preventive measures against Mpox, while 44.1 percent had not. The fact that 48 percent of the respondents had taken preventive measures to protect themselves from Mpox is a positive indicator of awareness and proactive behaviour within the community. The FGDs revealed that participants who took preventive action primarily practised hand hygiene. This is consistent with previous studies. However, this also suggests that a significant proportion (52 percent) of individuals may not be engaging in protective practices. In the FGDs, some participants reported no action, citing lack of knowledge and uncertainty about Mpox. This gap highlights the need for ongoing education and outreach efforts to ensure that more people understand the importance of preventive measures.
Increasing awareness and accessibility of resources can help enhance community protection against Mpox. A significant proportion of individuals recognise the importance of avoiding skin-to-skin or close contact with people with Mpox-like symptoms (94.4 percent) and washing hands with soap and water more regularly as a primary defence against Mpox. Participants also emphasised the importance of not sharing personal items or other objects touched by individuals with Mpox-like symptoms (86.9 percent), and seeking care at a health facility after developing suspicious symptoms and or having contact with someone showing Mpox symptoms (78.5 percent). The majority of participants (73.2 percent) reported that avoiding close, skin-to-skin contact with individuals exhibiting Mpox-like symptoms was the primary method of prevention, followed by handwashing with soap and water (64.5 percent) and receiving the Mpox vaccine (63.2 percent). The least frequently mentioned preventive measures were proper disposal of human waste (42.8 percent) and thorough cooking of food (36.8 percent). However, 26.6 percent of participants reported being unaware of how to prevent Mpox, and some held misconceptions, including using lemon and honey (27.1 percent) or relying on prayer for protection (3.3 percent).
There has been reluctance to take the Mpox vaccine (38.8 percent). This is consistent with studies conducted in other regions where many people are hesitant to be vaccinated in response to the current Mpox outbreak. While vaccines are crucial for eradicating infectious diseases like Mpox, there has been reluctance to take the Mpox vaccination (38.8 percent). Therefore, interventional education campaigns targeting populations at risk of vaccine hesitancy to combat misinformation and prevent low vaccination rates are needed urgently. When a new infectious disease is discovered, it can be helpful to examine knowledge and attitudes. This fits with previous findings showing that misinformation about the dangers of an emerging infectious pathogen can increase anxiety, worry, and even the possibility of conspiratorial thinking. In addition, bridging knowledge gaps might be considered a crucial component for preventing an Mpox epidemic. This is consistent with findings from studies conducted in other regions where many people were hesitant to be vaccinated in response to the current Mpox outbreak. Several reasons were cited for vaccination hesitancy, including fear of negative side effects, misinformation, and mistrust of medical staff or the healthcare system.
Conclusions
The study showed that while a significant proportion of participants had heard of Mpox, many held misconceptions and demonstrated gaps in understanding regarding its transmission. Misbeliefs included transmission through blood contamination, unsafe food practices, and exposure to contaminated water. These misconceptions are consistent with myths and misconceptions documented in recent literature. Most participants identified avoiding close, skin-to-skin contact with individuals showing Mpox-like symptoms as the main preventive measure, followed by handwashing with soap and water, and receiving the Mpox vaccine.
The study found that while people generally spoke openly about Mpox, some community members still questioned the existence of the Mpox outbreak. Notably, there was significant reluctance to accept vaccination as a preventive measure, highlighting a critical gap in risk perception and health-seeking behaviour. The study assessed Mpox prevention practices in selected districts of Zimbabwe affected by the outbreak. Findings show that many individuals recognised key preventive measures, including avoiding skin-to-skin or close contact with individuals showing Mpox-like symptoms and practising regular handwashing with soap and water. Participants also highlighted the importance of not sharing personal items with symptomatic individuals and seeking prompt medical care if they develop suspicious symptoms or have contact with a suspected case. However, the study also revealed that some community members lacked knowledge on how to prevent Mpox, indicating the need for strengthened health education and targeted risk communication efforts.
Recommendations
The study showed that the community had limited knowledge regarding the transmission of Mpox. There is a need to implement targeted, comprehensive health education programs and campaigns within communities, focusing on Mpox prevention to address widespread misconceptions about its transmission. These programs should be age-appropriate, interactive, and delivered in a culturally sensitive manner. The mixed attitudes expressed by participants regarding the existence of the Mpox outbreak highlight the importance of community engagement. Encouraging active participation in community-level initiatives, such as awareness campaigns and clean-up drives, can further strengthen their sense of responsibility for preventing Mpox. Additionally, involving local leaders, community health workers, and other community members in educational activities can help create a supportive environment that reinforces positive attitudes and practices. Furthermore, interventional education campaigns targeting populations at risk of vaccine hesitancy are urgently needed to combat misinformation and prevent low vaccination rates. Improving access to clean water by establishing or upgrading water supply systems is essential. Sanitation facilities should be enhanced with soap, and proper waste management must be ensured. It is also crucial to educate communities about the importance of not sharing personal items (e.g., clothing,
References
1. Parker S, Buller RM. A review of experimental and natural infections of animals with monkeypox virus between 1958 and 2012. (2013). Future Virol, 8(2):129–57. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3635111/
2. Thornhill JP, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison LB, et al. (2022). Monkeypox Virus Infection in Humans across 16 Countries, N Engl J Med., 387(8):679–91.
3. Ahmed S.K., Abdulqadir S.O., Omar RM, Hussein S., Qurbani K., Mohamed M.G. et al. (2023). Knowledge, Attitudes, and Willingness of Healthcare Workers in Iraq’s Kurdistan Region to Vaccinate against Human Monkeypox: A Nationwide Cross-Sectional Study. Vaccines, 11(12):1734.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10747727/
4. Vaughan A., Aarons E., Astbury J., Balasegaram S., Beadsworth M., Beck 3,14, Meera Chand C.R., O’Connor C., Dunning J., Ghebrehewet S., Harper N., Howlett-Shipley R., Ihekweazu C., Jacobs M., Kaindama L., Katwa P., Khoo S., Lamb L., Mawdsley S., Morgan D., Palmer R., Phin N., Russell K., Said B., Simpson A., Vivancos R., Wade M., Walsh A., Wilburn J. (2018). Two cases of monkeypox imported to the United Kingdom, September 2018. Euro Surveillance, 23(38). 1800509. doi: 10.2807/1560-7917.ES.2018.2 3.38.1800509. https://pubmed.ncbi.nlm.nih.gov/30255836/
5. Nuzzo J.B., Borio L.L. and Gostin L.O. (2022). The WHO Declaration of Monkeypox as a Global Public Health Emergency. JAMA, 328(7). https://pubmed.ncbi.nlm.nih.gov/35895041/
6. WHO. (2024). Global Mpox Trends [Internet]. [cited 2025 Sept 8]. Available from:
https://worldhealthorg.shinyapps.io/mpx_global/
7. Kumar A, Gautam A, Dutt D. (2016). Biotechnological Transformation of Lignocellulosic Biomass into Industrial Products: An Overview. ABB, 07(03):149–68.
http://www.scirp.org/journal/doi.aspx?DOI=10.4236/abb.2016.73014
8. Heskin J, Belfield A, Milne C, Brown N, Walters Y, Scott C, et al. Transmission of monkeypox virus through sexual contact: A novel route of infection. J Infect. 2022 Sept;85(3):334–63.
9. UNICEF. Mpox Factsheet for UNICEF-Zimbabwe, | UNICEF Zimbabwe. (2024).
https://www.unicef.org/zimbabwe/reports/mpox-factsheet-unicef-zimbabwe
10. Ghazy RM, Yazbek S, Gebreal A, Hussein M, Addai SA, Mensah E, et al. Monkeypox Vaccine Acceptance among Ghanaians: A Call for Action. (2023) Vaccines, 11(2):240.
https://doaj.org/article/4423dfe396ae437ea0020cc5553651ec
11. de Sousa D., Frade J., Patrocínio J., Borges-Costa J., Filipe P.. Monkeypox infection and bacterial cellulitis: A complication to look for. International Journal of Infectious Diseases, 2022, Volume 123: 180-182. https://pubmed.ncbi.nlm.nih.gov/36055636/
12. Du M., Deng J., Yan W., Liu M., Liang W., Niu B., Liu J.. Mpox vaccination hesitancy, previous immunisation coverage, and vaccination readiness in the African region: A multinational survey. (2025) EClinicalMedicine, 80,103047.
13. Sallam M., Al-Mahzoum K., Al-Tammemi A.B., Alkurtas M., Mirzaei F., Kareem N., Al-Naimat H., Jardaneh L., Al-Majali L., AlHadidi A., Al-Salahat K., Al-Ajlouni E., AlHadidi N.M., Bakri F.G., Harapan H., Mahafzah A. (2022) Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare, 10(9):1722. doi: 10.3390/healthcare10 091722. PMID: 36141334; PMCID: PMC9498667.
14. Awoyomi O.J., Njoga E.O., Jaja I.F., Oyeleye F.A., Awoyomi P.O., Ibrahim M.A., Saulawa M.A., Galadima H.B., Rowaiye A.B., Olasoju T.I., Idrisa J.A., Olalere F.D.H., Olasoju M.I., Adisa O.H., Adetunji V.E., Idemudia O.O., Ezenduka E.V., Oguttu J.W. (2023). Mpox in Nigeria: Perceptions and knowledge of the disease among critical stakeholders-Global public health consequences. PLoS ONE, 18(3):e02 83571. https://doi.org/10.1371/journal.pone.0283571
15. Hashmi M.U., Abid A., Tahir H. Muhammad Athar Khawaja M.A. (2024). Mpox now a global emergency: A reality versus myths. MedPharmRes, 8(2):147-151. eISSN: 2615-9139
DOI: https://doi.org/10.32895/UMP.MPR.8.2.16
16. Swed S., Bohsas H., Patwary M.M., Alibrahim H., Rakab A., Nashwan A.J., Hafez W., Hassan N.A.I. , Shoib S., Elsayed M., Sawaf B., Albuni M.K., Battikh E., Mohamed G.M.K., AlBozom A., Shaddad E., Fathey S., Htay M.N., Sah S., Cherrez-Ojeda I., Mohanty A., Padhi B.K., Rodriguez-Morales A.J., Gandhi A.P., Sah R. (2023). Knowledge of Mpox and its determinants among the healthcare personnel in Arabic regions: A multi-country cross-sectional study. New Microbes and New Infections, 54 101146. https://doi.org/10.1016/j.nmni.2023.101146
17. Tafawa C.R., Brar M., Sah S., Mehta R., Bushi G., Balaraman A.K., Pandey S., and Verma A. (2024). Mpox emerges in Zimbabwe: A turning point in global health vigilance. New Microbes and New Infections, 62, 101542, ISSN 2052-2975, https://doi.org/10.1016/j.nmni.2024.101542.
18. Sah R., Srivastava S., Mehta R., et al. (2024). Global Mpox Outbreak: Are we prepared for emerging strains? New Microbes and New Infections, 62, 101466, https://doi.org/10.1016/j.nmni.2024.101466
Most read articles by the same author(s)
- Denford M. Chuma, Amos Milanzi, Naomi N. Wekwete, Tatenda Songore, Nokuphiwa Moyo, Tafadzwa Mutiro, James Munamati, Juliet T. Milanzi, Lovemore Makurirofa, Effectiveness of the Youth-Led COVID-19 Technologically Innovative Interventions in Zimbabwe , Medical Research Archives: Vol 13 No 5 (2025): Vol.13, Issue 5, May 2025