

COVID-19 Vaccine Decision-Making in Pregnancy: Insights
Applying a Social Determinants of Health Framework to Understand COVID-19 Vaccine Decision-Making during Pregnancy and Postpartum: A Convergent Mixed Methods Study
Forgive Avorgbedor PhD, RN1*, Helene Vilme DrPH, MPH, MS2, Zainab Osakwe PhD, RN3, Ratchneewan Ross, PhD, RN, FTNSS, FAAN4, Mohammad Bany-Essa, RN, PhD student1, Amita Mittal MS1, Ayo Bankole, PhD, RN5
- University of North Carolina at Greensboro, School of Nursing
- Friedman School of Nutrition Science and Policy, Tufts University, Boston MA, 02111
- Adelphi University, USA
- The University of Louisville School of Nursing, USA
- Duke University School of Nursing
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: Avorgbedor, F., Vilme, H., et al., 2025. Applying a Social Determinants of Health Framework to Understand COVID-19 Vaccine Decision-Making during Pregnancy and Postpartum: A Convergent Mixed Methods Study. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6906
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6906
ISSN 2375-1924
ABSTRACT
Background: The COVID-19 pandemic disrupted healthcare access and trust, influencing vaccine decision-making among pregnant and postpartum individuals. While vaccine hesitancy research has focused primarily on individual-level attitudes, this study applies the Healthy People 2030 Social Determinants of Health framework to explore the broader system-level factors that shaped COVID-19 vaccine decision-making among pregnant and postpartum women.
Methods: and postpartum interviews) were recruited in the southeastern region of the United States. A convergent mixed method approach was used to analyze both the quantitative and qualitative data through five Social Determinants of Health domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context. Data integration occurred during interpretation using the Social Determinants of Health framework.
Results: We found that economic pressures, with many reporting employment-related vaccine mandates as a significant factor influencing their decision to vaccinate, educational disparities, healthcare interactions, neighborhood conditions, and social contexts all influenced vaccine-related behaviors during the pandemic. Qualitative data revealed that pregnant and postpartum women relied on trusted entities, such as their trusted healthcare providers, as one of the sources for vaccine information.
Conclusion: COVID-19 vaccine decision-making during pregnancy was influenced by a complex interplay of system-level factors. Interventions should integrate SDOH-informed screening in perinatal care, expand community-based communication strategies, and prioritize public health responses tailored to maternal health, especially during times of health crises.
Keywords
COVID-19, pregnancy, postpartum, vaccine hesitancy, social determinants of health, mixed methods, maternal health.
1. Introduction
The COVID-19 pandemic disrupted healthcare delivery worldwide, exacerbating existing structural barriers for pregnant and postpartum individuals. Amid rapidly shifting clinical guidelines, evolving public health mandates, and widespread misinformation, individuals were often forced to make critical health decisions in a climate of uncertainty. Pregnant and postpartum women, in particular, faced unique challenges accessing routine prenatal and obstetric care during the pandemic, and as a result often experienced poorer outcomes. As an example, an analysis of national surveillance data from 409,462 women with symptomatic COVID-19 in 2020 showed that pregnant women had an adjusted risk ratio of 3.0 for ICU admission, 2.9 for requiring mechanical ventilation, and 1.7 for death compared to non-pregnant women of similar age.
Despite these heightened risks, pregnant and postpartum individuals were not included in the initial development and clinical evaluation of COVID-19 vaccines, leading to a lack of evidence of vaccine efficacy which often introduced challenges to clinician decision-making, particularly in advising pregnant individuals who may have been eligible for the COVID-19 vaccine. At the same time, the pandemic exacerbated existing disparities in maternal care, contributing to poorer access and outcomes including higher rates of maternal mortality particularly among socially marginalized populations.
Previous studies explored factors that shaped COVID-19 vaccine decision-making among pregnant and postpartum women and factors such as culture, ethnicity, and religion were found to influence the decision about the vaccine. To further understand the role of structural factors in vaccine decision-making, this study was guided by the Social Determinants of Health (SDOH) framework, using data from pregnant and postpartum women to examine how structural and contextual factors influenced COVID-19 vaccine decision-making and healthcare navigation during pregnancy and the postpartum period. The SDOH framework identifies five key domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context that shape opportunities for health and well-being. Applying this framework helped to move beyond individual-level explanations of behavior to uncover how systemic barriers, material conditions, and social environments shaped perinatal experiences during a global health crisis.
2. Method
2.1 STUDY DESIGN AND FRAMEWORK
This study employed a convergent mixed methods approach, using a correlational research design for the quantitative arm and qualitative description for the qualitative arm to explore COVID-19 vaccine decision-making and information access among pregnant and postpartum women. The Social Determinants of Health (SDOH) framework from Healthy People 2030 was used to guide data analysis and interpretation. The five core SDOH domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context, were used to explore structural and contextual factors and behaviors. The SDOH framework defined the economic stability domain as the capacity to maintain financial resources to meet their basic needs and support health. The education access and quality domain was defined as the capacity to understand and make informed health decisions to support health. The healthcare access and quality domain was defined as access to high-quality healthcare to support health needs. The neighborhood and built environment domain was defined as a safe and accessible physical environment that supports health. The social and community context domain refers to the relationships, support systems, and community dynamics that influence health.
2.2 PARTICIPANT RECRUITMENT AND ELIGIBILITY
Participants were recruited between March and November 2022 through social media, community-based events, and health clinics in the southeastern United States. Eligible individuals self-identified as pregnant (≥24 weeks gestation) or postpartum (≤12 weeks), were at least 18 years old and could speak and read English. A total of 38 participants completed the online survey, and 28 participants agreed to participate in the qualitative interviews.
2.3 QUANTITATIVE DATA COLLECTION AND ANALYSIS
A total of 38 participants completed an online survey administered through Qualtrics between March and November 2022. We used validated measures aligned with the five domains of the Healthy People 2030 Social Determinants of Health (SDOH) framework. The participants reported demographic characteristics, such as COVID-19 vaccine status, age, race/ethnicity, education level, marital status, employment status, and insurance type. To assess Economic Stability, participants reported their employment status (employed or unemployed), and food insecurity using the validated 6-item short form of the U.S. Department of Agriculture Food Security Survey questionnaire; high scores indicate higher household food insecurity. Scores from this questionnaire were categorized as low food security and very low food security. Participants were also asked whether they were receiving any form of public assistance (yes/no). For Education Access and Quality, participants reported sources of information on the COVID-19 vaccine. Health Care Access and Quality was assessed by insurance type (Medicaid/TRICARE, private insurance, or uninsured) and their timing of prenatal care initiation, categorized as first, second, or third trimester. To evaluate the Neighborhood and Built Environment, we generated a Neighborhood-level Social Vulnerability Index (SVI) score; scores range from 0 (lowest vulnerability) to 1 (highest vulnerability) and provide a community-level indicator of social vulnerability. For Social and Community Context, participants completed the Everyday Discrimination Scale (EDS), a validated 9-item scale measuring the frequency of interpersonal discrimination, with scores ranging from 0 to 45. Participants also completed the Social Provisions Scale (SPS), a 24-item measure of perceived social support, with scores ranging from 24 to 96. To assess the perceived overall impact of the COVID-19 pandemic, participants were asked an open-ended question: “What is the impact of COVID-19 on your life?” Twenty-six (26) participants provided write-ups for this question. Responses to this item were analyzed using a content analysis approach. Two research team members independently reviewed all open-text responses and applied inductive coding to identify recurring categories of experience. Through iterative discussion and consensus, codes were grouped into higher-order thematic categories that reflected shared experiences related to social, occupational, emotional, and health domains. Exemplar quotes were selected to represent each theme, and approximate frequency counts were used to provide descriptive context.
2.4 QUANTITATIVE AND QUALITATIVE ANALYSIS
Descriptive statistics were calculated for all variables, with percentages reported for categorical variables and means, and standard deviations reported for continuous variables. All statistical analyses were performed using SAS v9.4 (SAS Institute, Cary, NC). Besides the open-ended question, we also conducted semi-structured interviews in a subset of survey respondents (n = 28). Semi-structured questions on COVID-19 vaccine decision-making included: “What do you think about pregnant women receiving the COVID-19 vaccine? What factors did you consider when making the decision, if any, did you have when contemplating getting vaccinated?” Interviews were conducted by two trained female researchers, audio-recorded, and professionally transcribed verbatim.
2.5 MIXED INTEGRATION
Integration was guided by the Healthy People 2030 Social Determinants of Health (SDOH) framework, allowing findings from both data sources to be organized and interpreted within five core domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context. Quantitative data provided a descriptive and comparative view of participant characteristics and structural exposures. In contrast, qualitative data offered rich context into lived experiences, decision-making, and meaning-making during the COVID-19 pandemic.
3. Ethics
The study was approved by the University of North Carolina at Greensboro Institutional Review Board. All participants provided informed consent before participating in the survey or interviews.
4. Results
We organized findings using the five domains of the Healthy People 2030 Social Determinants of Health (SDOH) framework.
4.1 SAMPLE CHARACTERISTICS
The sample included n = 38 pregnant and postpartum women in the quantitative arm (Mean age = 30.78 years, SD = 6.08) who were predominantly Black or African American (68.4%), followed by White (18.4%) and Multiracial/other (13.2%) individuals. Employment was disrupted during the pandemic, with 45% employed and 55% unemployed at the time of the survey.
4.2 ECONOMIC STABILITY
Quantitative data showed that 21% of participants experienced very low food security and 63% of participants were receiving public assistance, and many reported employment-related vaccine requirements as a driving factor in their decision to be vaccinated. Qualitative data highlighted how economic pressures, particularly the need to maintain or obtain employment, influenced vaccination behavior.
4.3 EDUCATION ACCESS AND QUALITY
Forty-two (42%) of participants had a high school education or less, and 29% had some college degree, 16% graduated from college and 10.5% relied on informal sources of information such as social media, family, and friends, reflecting both accessibility and trust issues in more formal educational or scientific resources.
4.4 HEALTH CARE ACCESS AND QUALITY
Most participants (79%) initiated prenatal care in the first trimester, and insurance coverage was 71.1% Medicaid. Qualitative data added important context, revealing that while some participants relied on healthcare providers as trusted sources of vaccine information, experiences with communication and guidance varied and may have influenced decision-making regarding vaccination during pregnancy.
4.5 NEIGHBORHOOD AND BUILT ENVIRONMENT
The mean Neighborhood SVI score was 0.64, indicating moderate-to-high social vulnerability across the sample. One participant referenced how living environments or housing situations shaped their perception of risk.
4.6 SOCIAL AND COMMUNITY CONTEXT
Participants reported a mean Everyday Discrimination Score (EDS) of 8.9, a mean Social Provisions Score (SPS) of 60.40, indicating a strong perceived social support. Qualitative data supported this finding, with participants highlighting the important role of family, friends, cultural values, and trust in public health institutions in shaping vaccine decision-making.
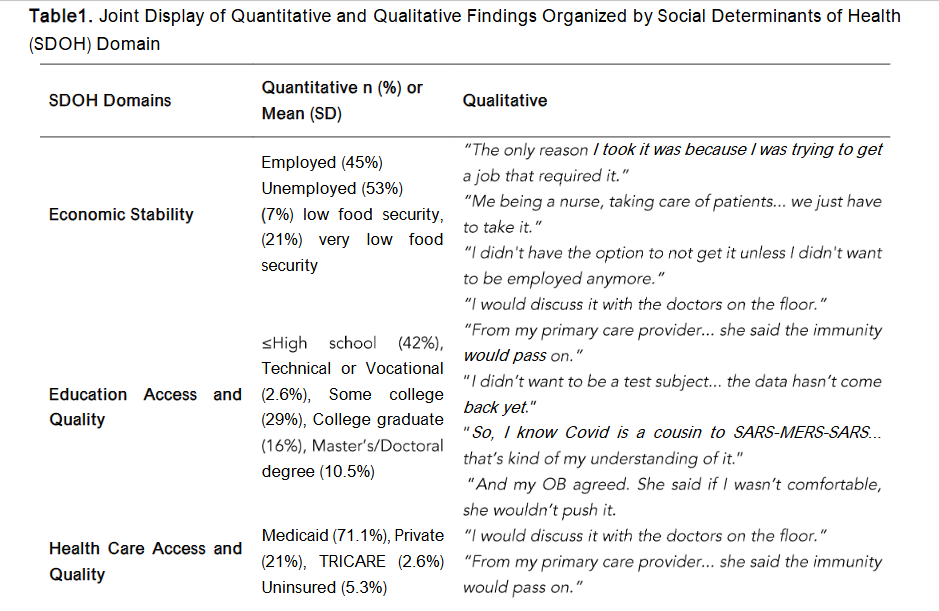
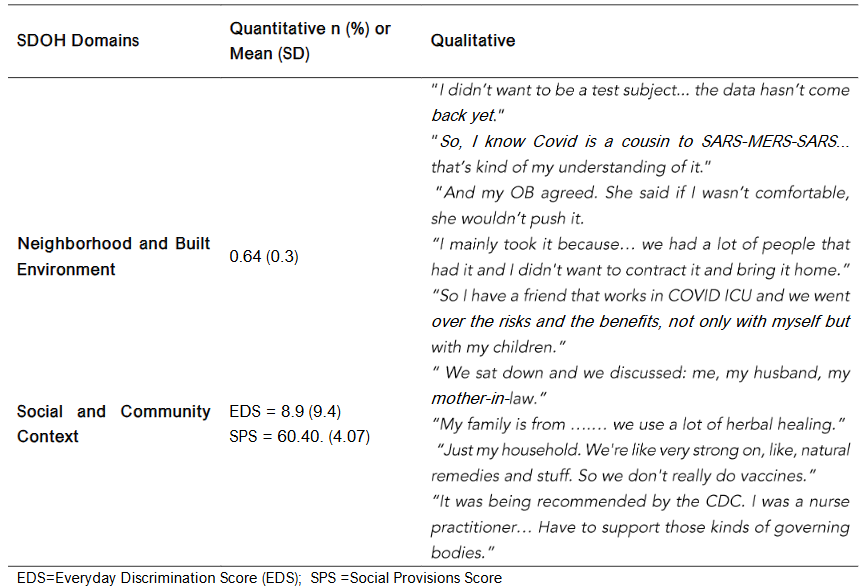
Table 1. Joint Display of Quantitative and Qualitative Findings Organized by Social Determinants of Health (SDOH) Domain
Overall Impact
Participants described a wide range of ways the COVID-19 pandemic affected their lives. Many participants reported life disruptions, including health scares, job loss, increased caregiving responsibilities, or loss of loved ones. Several shared that they or their children had contracted COVID-19 multiple times, and some described ongoing worry about infecting vulnerable family members or newborns. Others emphasized the mental health toll of isolation, fear, and disrupted routines. A smaller number reported positive impacts, including increased work hours or a renewed sense of purpose. Some participants indicated that COVID-19 had minimal or no impact.
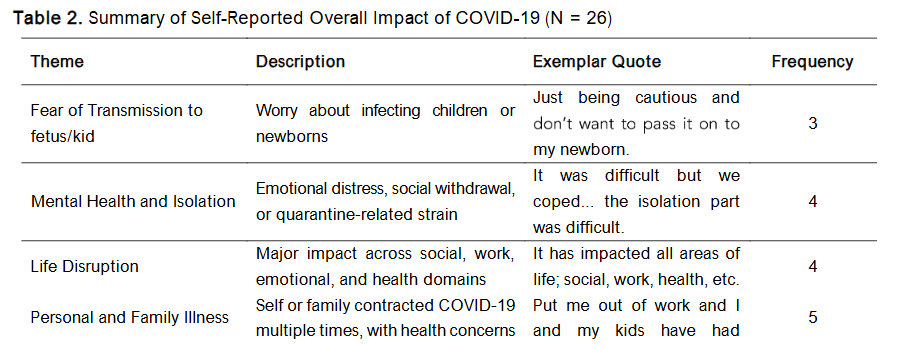
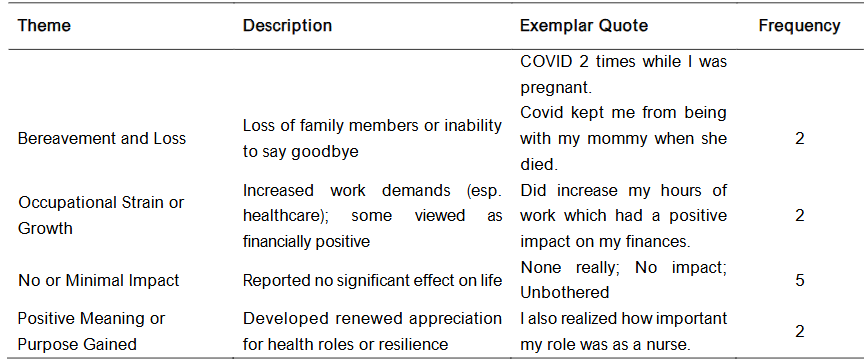
Table 2. Summary of Self-Reported Overall Impact of COVID-19 (N = 26)
5. Discussion
The SDOH framework guided this study to explore how pregnant and postpartum women navigated the decision-making process and access to information regarding the COVID-19 vaccine. Using a mixed-methods approach, we found that economic pressures, educational disparities, healthcare interactions, neighborhood conditions, and social contexts all influenced vaccine-related behaviors during the pandemic. In this sample, similar to other studies, we also found that pregnant and postpartum women relied on trusted entities, such as their trusted healthcare providers, as one of the sources for vaccine information.
Our data revealed reliance on social media, informal networks, and internet searches for vaccine information, highlighting challenges related to information access and health literacy within the domain of education access and quality. While some participants attempted to consult scientific sources, others expressed confusion and skepticism. This echoes the findings by Olorunsaiye et al., who documented gaps in vaccine literacy and the impact of mistrust and inconsistent information among Black pregnant and postpartum women. Women who lean on sources other than their healthcare providers for vaccine information may also be exposed to misinformation about the vaccine.
Healthcare access and quality emerged as a critical domain, with participants describing healthcare providers as key influences on vaccine decisions. Positive interactions encouraged uptake, particularly with OB/GYNs and primary care providers. However, there was inconsistent messaging and clarity about pregnancy-specific vaccine safety during the early stages of the COVID-19 vaccine, which also contributed to uncertainty. It was not until January 29, 2021, that the World Health Organization (WHO) revised its COVID-19 vaccine guidance to allow pregnant women at high risk of exposure or severe disease to be vaccinated, in consultation with their healthcare providers. In addition, pregnant and postpartum women were not included in the initial development and clinical evaluation of the COVID-19 vaccine, and the US Food and Drug Administration (FDA) and the Advisory Committee on Immunization Practices left open the option for pregnant and lactating women to receive the vaccine. Healthcare provider recommendation is indeed one of the most important factors influencing vaccine acceptance among pregnant women.
Regarding the neighborhood and built environment, participants referenced housing instability and community transmission risks. Our quantitative data showed a moderate mean SVI score, consistent with Kiefer et al., who found that higher community-level social vulnerability was associated with vaccine hesitancy and lower uptake. SVI highlights the importance of understanding community resources and providers in maternal health. These findings parallel recommendations from Ruyak and Kivlighan and Preis, Mahaffey, and Lobel, who called for more systematic integration of SDOH-informed psychosocial counseling into perinatal care.
Finally, social and community contexts shaped vaccine decisions. Many participants were motivated by the desire to protect family members, especially children and elderly relatives, which is consistent with the findings of Olorunsaiye et al. Some pregnant women in our study were motivated by the desire to protect their newborns. At the same time, conflicting messages from cultural, religious, or familial influences also discouraged some participants from vaccination. Importantly, our mixed-methods approach complements prior research by providing a systems-level perspective that emphasizes the role of structural determinants, rather than framing vaccine hesitancy solely as an individual behavioral process. The interplay of SDOH domains: economic, educational, structural, and social, shaped vaccine decisions and maternal trust in healthcare and information systems. This supports calls by Scroggins et al. and Jean-François et al. for integrating SDOH screening and interventions into routine perinatal care and public health planning.
6. Limitations
This study has limitations. The sample is small and, while diverse, was not nationally representative and was drawn primarily from the southeastern United States, which may limit generalizability. Further, all data were self-reported and thus subject to recall bias. Additionally, the cross-sectional design limits causal inference. While the convergent mixed methods design allowed for rich data triangulation, it may not have captured the full complexity of longitudinal shifts in attitudes and behaviors over time.
7. Implications for Practice and Policy
To promote COVID-19 vaccine uptake and advance maternal health equity, future efforts must address deeper drivers that go beyond individual decision-making processes. First, SDOH-informed screening and counseling should be embedded into routine prenatal care. As part of comprehensive maternal health services, healthcare providers should assess for economic instability, discrimination, social support, and neighborhood barriers. Second, trusted, community-based information channels must be expanded to counter misinformation and foster trust. These efforts should involve partnerships with community organizations, faith-based groups, and peer networks that are seen as credible sources of information among pregnant and postpartum individuals. Finally, healthcare systems must work to enhance responsiveness to the lived experiences of pregnant and postpartum women.
8. Conclusion
The COVID-19 pandemic exposed system-level barriers in maternal health. Using the SDOH framework, this study highlights how system-level factors shaped vaccine decision-making and information access for pregnant and postpartum women. By integrating qualitative and quantitative data, our findings underscore the urgent need for equity-driven, community-informed approaches to perinatal care and vaccine outreach both during public health crises and beyond.
9. Conflicts of Interest Statement
The authors declare no conflicts of interest related to the design, implementation, or reporting of this study.
10. Funding Statement
This work was supported by the Programs to Increase Diversity Among Individuals Engaged in Cardiovascular Health-Related Research (PRIDE-CVD) R25HL105446 (PI: M. Boutjdir) Small Research Project Fund.
11. Acknowledgements
None.
References
- Mithal LB, Otero S, Shanes ED, Goldstein JA, Miller ES. Cord blood antibodies following maternal coronavirus disease 2019 vaccination during pregnancy. American Journal of Obstetrics & Gynecology. 2021;225(2):192-194.
- Razzaghi H. COVID-19 vaccination coverage among pregnant women during pregnancy eight integrated health care organizations, United States, December 14, 2020 May 8, 2021. MMWR Morbidity and mortality weekly report. 2021;70.
- Adhikari EH, Moreno W, Zofkie AC, et al. Pregnancy outcomes among women with and without severe acute respiratory syndrome coronavirus 2 infection. JAMA network open. 2020;3(11):e2029256.
- Adhikari EH, Spong CY. COVID-19 vaccination in pregnant and lactating women. Jama. 2021;325(11):1039-1040.
- Emeruwa UN, Gyamfi-Bannerman C, Miller RS. Health care disparities in the COVID-19 pandemic in the United States: a focus on obstetrics. Clinical obstetrics and gynecology. 2022;65(1):123-133.
- Shephard HM. Inequities in COVID-19 Vaccination Coverage Among Pregnant Persons, by Disaggregated Race and Ethnicity Massachusetts, May 2021 October 2022. MMWR Morbidity and Mortality Weekly Report. 2023;72.
- Avorgbedor F, Gondwe KW, Aljarrah A, Bankole AO. COVID-19 vaccine decision-making among black pregnant and postpartum women. Journal of Racial and Ethnic Health Disparities. 2024;11(4):2073-2082.
- Bhattacharya O, Siddiquea BN, Shetty A, Afroz A, Billah B. COVID-19 vaccine hesitancy among pregnant women: a systematic review and meta-analysis. BMJ open. 2022;12(8):e061477.
- Creswell JW, Klassen AC, Plano Clark VL, Smith KC. Best practices for mixed methods research in the health sciences. Bethesda (Maryland): National Institutes of Health. 2011;2013:541-545.
- Office of Disease Prevention and Health Promotion. Social determinants of health. Healthy People 2030, U.S. Department of Health and Human Services. Retrieved June 18, 2025, from https://odphp.health.gov/healthypeople/priority-areas/social-determinants-health.
- Ruyak SL, Kivlighan KT. Perinatal behavioral health, the COVID-19 pandemic, and a social Determinants of Health framework. Journal of Obstetric, Gynecologic & Neonatal Nursing. 2021;50(5):525-538.
- United States Department of Agriculture, Economic Research Service. U.S. Household Food Security Survey. May 2024. Accessed April 7, 2025. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/survey-tools/.
- Flanagan BE, Gregory EW, Hallisey EJ, Heitgerd JL, Lewis B. A social vulnerability index for disaster management. Journal of homeland security and emergency management. 2011;8(1).
- Dr W. Racial differences in physical and mental health. J Health Psychol. 1997;2:335-351.
- Cutrona CE, Russell DW. Social provisions scale. Journal of Abnormal Psychology. 1987.
- Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qualitative health research. 2005;15(9):1277-1288.
- Obasanya M, Igenoza O, Gupta S, McElroy K, Brannon GE, Brown K. Racial and ethnic differences in maternal and child COVID-19 vaccination intent among pregnant and postpartum women in the USA (April June 2020): An application of health belief model. Journal of Racial and Ethnic Health Disparities. 2023;10(5):2540-2551.
- Alcendor DJ, Matthews-Juarez P, Smoot D, et al. The covid-19 vaccine and pregnant minority women in the us: Implications for improving vaccine confidence and uptake. Vaccines. 2022;10(12):2122.
- Olorunsaiye CZ, Degge HM, Osborne A, Gordon DN. COVID-19 Vaccine Literacy Among Black Pregnant and Postpartum Women in the USA. Journal of Racial and Ethnic Health Disparities. 2025:1-14.
- Zhao S, Hu S, Zhou X, et al. The prevalence, features, influencing factors, and solutions for COVID-19 vaccine misinformation: systematic review. JMIR public health and surveillance. 2023;9(1):e40201.
- Spong CY, Bianchi DW. Improving public health requires inclusion of underrepresented populations in research. Jama. 2018;319(4):337-338.
- Carson SL, Casillas A, Castellon-Lopez Y, et al. COVID-19 vaccine decision-making factors in racial and ethnic minority communities in Los Angeles, California. JAMA network open. 2021;4(9):e2127582-e2127582.
- Ellingson MK, Dudley MZ, Limaye RJ, Salmon DA. Vaccine decision-making in pregnant women: A systematic review of the literature. Expert review of vaccines. 2019;18(2):191-204.
- Myers KL. Predictors of maternal vaccination in the United States: An integrative review of the literature. Vaccine. 2016;34(34):3942-3949.
- Wilson RJ, Paterson P, Jarrett C, Larson HJ. Understanding factors influencing vaccination acceptance during pregnancy globally: a literature review. Vaccine. 2015;33(47):6420-6429.
- Kiefer MK, Mehl R, Rood KM, et al. Association between social vulnerability and COVID-19 vaccination hesitancy and vaccination in pregnant and postpartum individuals. Vaccine. 2022;40(44):6344-6351.
- Preis H, Mahaffey B, Lobel M. Factors related to COVID-19 vaccination intention and uptake among childbearing women. Health Psychology. 2023;42(8):567.
- Basile Ibrahim B, Kennedy HP, Combellick J. Experiences of quality perinatal care during the US COVID‐19 pandemic. Journal of midwifery & women’s health. 2021;66(5):579-588.
- Scroggins JK, Yang Q, Tully KP, Reuter-Rice K, Brandon D. Examination of Social Determinants of Health Characteristics Influencing Maternal Postpartum Symptom Experiences. Journal of Racial and Ethnic Health Disparities. 2025;12(1):625-639.
- Jean-Francois B, Bailey Lash T, Dagher RK, Green Parker MC, Han SB, Lewis Johnson T. The potential for health information technology tools to reduce racial disparities in maternal morbidity and mortality. Journal of Women’s Health. 2021;30(2):274-279.