






Maxillomandibular Advancement for Severe Sleep Apnea
Maxillomandibular advancement Surgery in Morbidly Severe Obstructive Sleep Apnea: A 2-year follow-up
Asmaa El Mabrak1, Lamia Bouchghel1, Majid Amine2, Sofiane Ghorbal3, Farid El Quars1
- Professors, Department of Dento-Facial Orthopedics, Hassan II University, Casablanca, Morocco
- Resident, Department of Dento-Facial Orthopedics, Hassan II University, Casablanca, Morocco
- Private practitioner
*ORCID: https://orcid.org/0000-0002-2954-5237
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: El Mabrak, A., Bouchghel, L., et al., 2025. Maxillomandibular advancement Surgery in Morbidly Severe Obstructive Sleep Apnea: A 2-year follow-up. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6663
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6663
ISSN 2375-1924
ABSTRACT
Obstructive sleep apnea syndrome is a common disorder characterized by recurrent episodes of upper airway obstruction during sleep. Its prevalence is estimated at 2% to 4% among middle-aged adults (30 to 60 years), while approximately 1% of children are also affected. OSAS is now recognized as an independent risk factor for cardiovascular diseases, highlighting the importance of early diagnosis and appropriate treatment. Polysomnography remains the gold standard for diagnosing obstructive sleep apnea syndrome. Therapeutically, nasal continuous positive airway pressure is considered the first-line treatment for both snoring and obstructive sleep apnea. Oral appliances may be used in mild to moderate cases. However, in severe forms of the condition, especially when associated with craniofacial abnormalities, maxillomandibular advancement is often the only effective option capable of providing long-term improvement. This case report presents the management of a 27-year-old male patient with obstructive sleep apnea syndrome, associated with a significant mandibular retrognathia. The treatment plan involved maxillomandibular advancement, with the objective of increasing the oropharyngeal airway volume. The surgical outcome was favorable, offering a definitive resolution of the patient’s obstructive sleep apnea syndrome.
Keywords:
- Class II malocclusion
- obstructive sleep apnea
- OSA
- Maxillomandibular advancement oral surgery
INTRODUCTION
Obstructive sleep apnea (OSA) is a frequent respiratory disorder characterized by repeated episodes of partial or complete obstruction of the upper airway during sleep, resulting in intermittent hypoxia and frequent micro-arousals. These disturbances degrade sleep quality and are linked to a range of systemic complications, including hypertension, cardiovascular diseases, metabolic syndrome, stroke, and a heightened risk of premature mortality.
Beyond its physiological impact, OSA significantly affects patients’ quality of life, contributing to excessive daytime sleepiness, cognitive dysfunction, and memory problems. The current gold standard for OSA management is continuous positive airway pressure (CPAP) therapy, which maintains airway patency throughout sleep. However, adherence remains a major limitation, often due to discomfort and inconvenience associated with long-term device use.
In recent years, surgical alternatives have gained attention, with maxillomandibular advancement (MMA) emerging as a particularly effective option. This orthognathic procedure advances both the maxilla and mandible, thereby enlarging the posterior airway space at multiple levels—nasopharyngeal, oropharyngeal, and hypopharyngeal.
MMA has shown clinical outcomes comparable to those of CPAP, with reported success rates ranging from 75% to 100% in the short term. It enhances upper airway morphology—improving volume, surface area, and resistance to collapse—and frequently leads to significant symptom relief, including reduced daytime sleepiness and, in some cases, discontinuation of CPAP use.
This case report describes the successful treatment of a patient with severe retrognathia and obstructive sleep apnea syndrome (OSAS). The treatment consisted of mandibular and maxillary advancement surgery, a procedure intended to enlarge the oropharyngeal airway and permanently eliminate the obstructions causing OSAS.
CASE REPORT:
EXTRA- AND INTRA-ORAL EXAMINATION
The patient M.E., a 29-year-old male, presented to the Dentofacial Orthopedics Department of the Casablanca University Hospital with a functional complaint of recurrent obstructive sleep apnea, negatively impacting his quality of life. He also reported a gummy smile and a marked mandibular retrognathia. The patient had previously undergone orthodontic treatment, but experienced a relapse.
Clinical evaluation revealed an oval, elongated, and symmetrical face with a convex facial profile. Lip closure at rest was incomplete and required hyperactivity of the mentalis muscle. The patient had a short upper lip and an obtuse nasolabial angle. Vertically, the lower third of the face was predominant compared to the middle and upper thirds.

The patient demonstrated moderate oral hygiene. The upper and lower dental midlines were centered and coincident with the facial midline. The molar and canine relationships were classified as Angle Class II, with no dental crowding in either arch. The maxillary arch was broad, with an interincisal diastema and protruded upper incisors. The mandibular arch was U-shaped, with vestibular inclination of the lower incisors. A restoration was noted on tooth 44, along with a diastema between teeth 33 and 32.

• Panoramic radiograph: The panoramic radiograph revealed a complete dentition with no signs of alveolar bone loss. The mandibular condyles showed normal morphology, with no clinical or radiographic signs of temporomandibular joint dysfunction. A restoration and a root canal treatment were observed on tooth 44.
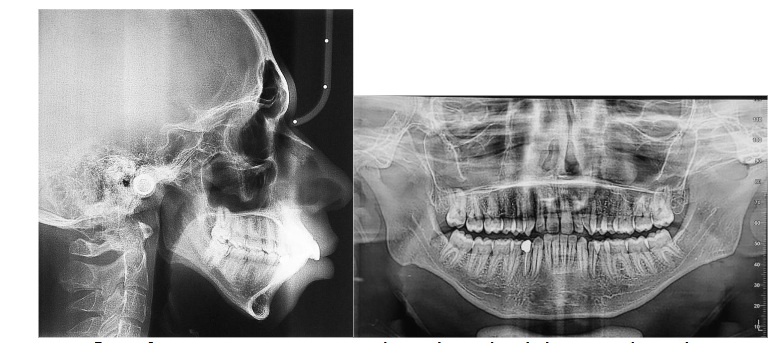
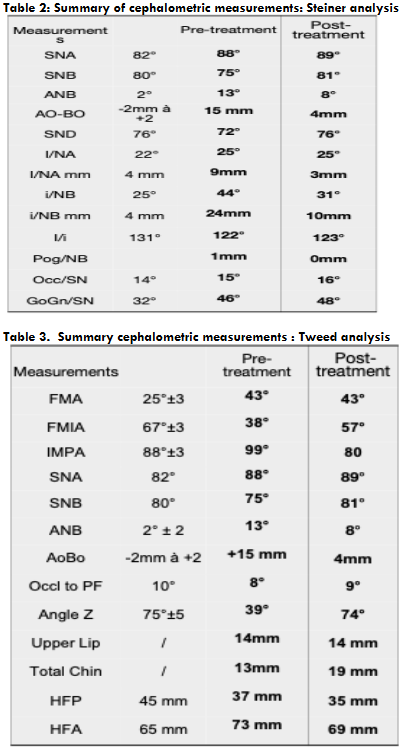
• Lateral cephalometric radiograph: Cephalometric analysis showed features of posterior mandibular rotation, with GoGn/SN = 46° and FMA = 43°. Steiner and Tweed cephalometric measurements confirmed a skeletal Class II pattern, with pro-alveolar upper incisors and retro-alveolar lower incisors.
Treatment plan:
The treatment plan began with the extraction of teeth 34 and 44, as well as all four third molars, as part of the orthodontic preparation phase.
A multidisciplinary consultation was conducted, involving both the orthodontics and maxillofacial surgery teams, to establish a comprehensive treatment approach for the patient’s severe mandibular retrognathism and obstructive sleep apnea (OSA).
A surgical treatment plan was established and accepted by the patient. The primary objective was to perform a maxillomandibular advancement (MMA) to correct the pronounced mandibular retrognathism, increase the upper airway volume, and thereby treat the OSA. The surgical procedure consisted of a bimaxillary osteotomy, including a Le Fort I impaction, maxillomandibular advancement, and a complementary genioplasty.
The orthodontic phase of the treatment included dental alignment and leveling, correction of dental rotations, retraction of the lower incisors, and final coordination of both arches. Simulation models were used to optimize the relationship between the upper and lower dental arches. After the orthodontic preparation, a significant improvement in anteroposterior projection was observed.

Treatment results:
Our therapeutic objectives were successfully achieved. The patient’s facial profile showed significant improvement, with a harmonious labial ratio and a satisfactory smile line.

From a functional perspective, the patient experienced complete resolution of obstructive sleep apnea, with clinical examination confirming normalization of sleep quality. A Class I canine relationship was established, with midline symmetry of the central incisors, and an ideal overbite and overjet were achieved.

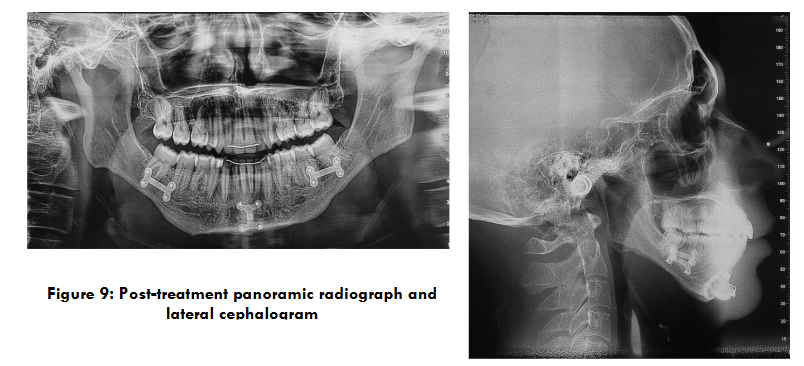
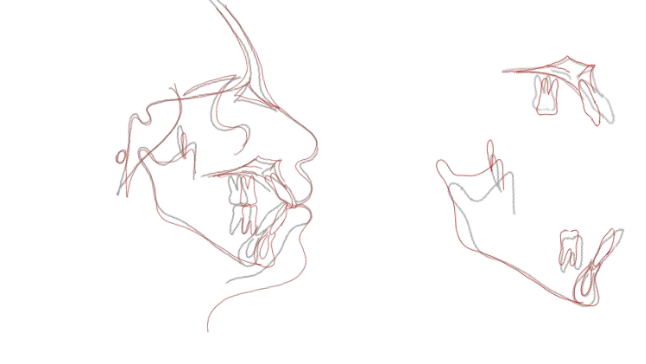
Post-treatment panoramic radiography demonstrated good parallelism of the dental roots, with no signs of root resorption (Fig. 9). Profile cephalometric analysis (Fig. 9), final cephalometric measurements (Tables I and II), and general and regional superimpositions (Fig. 10) all confirmed the restoration of normal dental and skeletal relationships.
DISCUSSION
This case report describes the successful treatment of a patient with severe retrognathia and obstructive sleep apnea syndrome (OSAS). The treatment consisted of mandibular and maxillary advancement surgery, a procedure intended to enlarge the oropharyngeal airway and permanently eliminate the obstructions causing OSAS.
Maxillomandibular advancement (MMA) is an invasive yet potentially effective surgical option in the treatment of obstructive sleep apnea (OSA) for patients who have difficulty tolerating continuous positive airway pressure and whose OSA has been refractory to other surgical modalities.
Maxillomandibular advancement achieves enlargement of the nasopharyngeal, retropalatal, and hypopharyngeal airway by physically expanding the facial skeletal framework via Le Fort I maxillary and sagittal split mandibular osteotomies. Advancements of the maxilla and mandible increase tension on the pharyngeal soft tissue, thereby enlarging the medial-lateral and anteroposterior dimensions of the upper airway.
In a meta-analysis, Soroush Zaghi et al. concluded that maxillomandibular advancement (MMA) is a highly effective surgical treatment for obstructive sleep apnea (OSA), showing consistent and significant improvements in both objective sleep parameters and patient-reported outcomes. In one study of 518 patients, 98.8% experienced improvements in respiratory metrics. The mean apnea-hypopnea index (AHI) decreased from 57.2 to 9.5 events/hour, and the respiratory disturbance index (RDI) from 65.8 to 21.4 events/hour — corresponding to reductions of 80.1% and 64.6%, respectively. Improvements were also observed in oxygen saturation (SpO₂ nadir) and daytime sleepiness (Epworth Sleepiness Scale), further supporting the efficacy of MMA as a comprehensive surgical solution for OSA.
A retrospective study by Goodday et al., involving patients with a mean preoperative AHI of 117.9, demonstrated a significant reduction in AHI to a postoperative mean of 16.1 (p < 0.001) following maxillomandibular advancement (MMA) surgery. These findings suggest that MMA can serve as a highly effective single-stage surgical intervention for extremely severe OSA, potentially eliminating the need for continuous positive airway pressure (CPAP) therapy and improving patient-reported outcomes.
Comparable outcomes were observed in a case study by Doff et al., in which a patient’s AHI was reduced from 139 to 6 following maxillomandibular advancement (MMA). They described the successful use of a combined surgical approach MMA, modified genioplasty, and cervicomental liposuction in a morbidly obese woman with severe OSA (AHI = 139) who was intolerant to CPAP. After surgery, her AHI dropped to 6, and her oxygen saturation improved significantly. They advocate this multimodal surgical strategy as a promising option for obese patients with CPAP intolerance, citing notable enlargement of the upper airway at the retropalatal and retroglossal levels.
While CPAP remains the gold standard for OSA treatment, its long-term compliance is often poor due to discomfort and intolerance. As noted by Butterfield et al., this has prompted many patients to seek alternative options, including surgical interventions such as MMA. MMA involves advancing the maxilla and mandible through concomitant osteotomies with the goal of enlarging the posterior airway space across multiple anatomical levels (nasopharynx, oropharynx, and hypopharynx), as described by Boyd.
According to Butterfield et al., this surgical advancement enhances airway patency and reduces pharyngeal collapsibility by repositioning the bony attachment sites of the pharyngeal musculature. Holty and Guilleminault performed a prior meta-analysis of 22 studies reporting AHI outcomes describing 627 adults undergoing MMA to treat OSA. They report a significant reduction in the mean AHI (63.9 vs 9.5 events/h; P < .001) at a mean follow-up of 5.3 months after MMA. The percentages of participants with a reduction greater than 50% and an AHI of fewer than 20, 15, 10, and 5 events/h after MMA were 86.0%, 77.6%, 63.4%, and 43.2%, respectively.
The outcomes of MMA surgery demonstrate improvements in sleep quality that are comparable to those experienced by patients using continuous positive airway pressure (CPAP) therapy. MMA brings about favorable changes in airway morphology, effectively reversing the long, narrow, and circular airway shape typically observed in individuals with obstructive sleep apnea (OSA). By advancing the bony insertion sites of the upper airway muscles, MMA results in a widening of the airway and a reduction in pharyngeal collapsibility, thereby improving airflow during sleep.
One study quantitatively assessed both linear and volumetric changes in the pharyngeal airway following MMA for the treatment of OSA. The findings underscore MMA’s success as a surgical intervention, demonstrating significant morphological improvements that include a shorter and broader airway, which correlate with marked reductions in the apnea-hypopnea index (AHI).
The effectiveness of MMA in managing severe OSA is further supported by another study, which reported a mean AHI reduction of 101.8 events per hour in patients with a preoperative AHI exceeding 100. Remarkably, six patients achieved a postoperative AHI of less than five, indicating a surgical cure.
It is also important to recognize that the success of MMA surgery can be significantly enhanced when combined with adjunctive procedures such as geniotomy or uvulopalatopharyngoplasty (UPPP). One study reported a near 100% success rate when MMA was performed after or concurrently with UPPP, highlighting the potential benefit of a comprehensive surgical approach.
Multiple studies have demonstrated that MMA surgery leads to significant improvements in subjective outcomes for patients with obstructive sleep apnea (OSA), particularly those with severe to morbid forms of the condition. In a comprehensive study by Goodday and Bourque, which included 116 patients, MMA surgery resulted in a 96% reduction in CPAP use, an 83% decrease in snoring, and a 94% reduction in witnessed apneas (p < .001). Notably, 89% of patients considered the surgery worthwhile, and 95% stated they would recommend it to other patients suffering from OSA.
For patients with extremely severe OSA (AHI > 100), Goodday et al. observed a significant reduction in excessive daytime sleepiness, as measured by the Epworth Sleepiness Scale (ESS), with the mean score improving from 12.9 to 5.0 (p = 0.004). In this subgroup, seven out of nine patients reported no remaining daytime sleepiness, and only one continued using CPAP postoperatively, further supporting MMA as a viable and effective treatment for the most severe cases.
Scott B Boyd et al. concluded that MMA is an effective long-term treatment for most patients with moderate to severe OSA, as evidenced by significant reductions in AHI, diastolic BP and subjective sleepiness, with concomitant significant improvements in quality of life. The results of this small cohort study suggest that MMA should be considered as the alternative treatment of choice for patients with severe OSA who cannot fully adhere to CPAP therapy.
In his systematic review, R. John explains that MMA (Mandibular Advancement) expands the skeletal framework to which the pharyngeal structures and tongue are attached. This leads to a reduction in airway collapsibility during negative-pressure inspiration and an increase in upper airway space. Joseph E concluded in his study that MMA for OSA led to statistically and clinically significant long-term horizontal skeletal angular advancements of the maxilla and mandible, with increases of 6% and 4.9%, respectively, unaffected by gender, age, or BMI. The results demonstrated substantial expansion of the maxillomandibular complex, with the maxilla advancing by 6% and the mandible by 4.9%, both of which were maintained for over 10 years. These findings confirm that horizontal expansion of the facial skeleton through MMA can be sustained in the long term, regardless of factors such as age, gender, or BMI.
Regarding the relationship between quality of life and maxillomandibular advancement (MMA) surgery for the treatment of obstructive sleep apnea (OSA), Kok Weng Lye et al. highlighted that although MMA remains the most effective surgical intervention for OSA, no comprehensive quality-of-life studies had been conducted. The disease-specific quality-of-life instrument (FOSQ) demonstrated a subjective improvement in functional outcomes among patients who underwent MMA. Quality-of-life measures should be incorporated into the evaluation of all surgical treatments, as they provide an essential dimension in assessing both patient outcomes and the effectiveness of procedures.
Others authors have argued that surgical intervention for patients with sleep apnea is reserved only for those who cannot or will not accept continuous positive airway pressure therapy; as such, the goal of surgery is not to cure a condition that is obviously incurable but rather to offer a treatment that will help abate symptoms and minimize ongoing multisystem damage.
CONCLUSION:
Maxillomandibular advancement (MMA) surgery is a well-established and increasingly utilized surgical treatment for patients with severe to extremely severe obstructive sleep apnea (OSA), particularly those who are intolerant to continuous positive airway pressure (CPAP) therapy. MMA involves the forward repositioning of the maxilla and mandible to enlarge the upper airway and reduce its collapsibility during sleep.
Studies have shown that MMA significantly reduces the apnea-hypopnea index (AHI), improves oxygen saturation, enhances airway morphology, and leads to high patient satisfaction. In some cases, it achieves results comparable to CPAP, with the added benefit of potentially eliminating the need for ongoing device use. These improvements are observed even in patients with extremely severe OSA (AHI > 100), where reductions in AHI and daytime sleepiness are particularly notable.
Despite these positive outcomes, evidence regarding the long-term efficacy and safety of MMA—especially in extremely severe OSA—remains limited. Further research is necessary to better define the long-term outcomes and to identify which patients are most likely to benefit from this surgical intervention.
REFERENCES:
- Boyd SB, Walters AS, Song Y, Wang L. Comparative effectiveness of maxillomandibular advancement and uvulopalatopharyngoplasty for the treatment of moderate to severe obstructive sleep apnea. J Oral Maxillofac Surg. 2013.
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002.
- Peppard PE, Young T, Barnet JH, et al. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177:1006.
- Boyaci H, Gacar K, Baris SA, et al. Positive airway pressure device compliance of the patients with obstructive sleep apnea syndrome. Adv Clin Exp Med. 2013;22:809.
- Hsieh YJ, Liao YF. Effects of maxillomandibular advancement on the upper airway and surrounding structures in patients with obstructive sleep apnoea: a systematic review. Br J Oral Maxillofac Surg. 2013;51:834.
- Vezina J, Blumen M, Buchet I, et al. Sleep-disordered breathing: choosing the right cephalometric analysis. J Oral Maxillofac Surg. 2012;70:1442.
- Li KK. Surgical management of obstructive sleep apnea. Clin Chest Med. 2003;24(2):365-370.
- Gokce SM, Gorgulu S, Gokce HS, Bengi AO, Karacayli U, Ors F. Evaluation of pharyngeal airway space changes after bimaxillary orthognathic surgery with a 3-dimensional simulation and modeling program. Am J Orthod Dentofacial Orthop. 2014;146(4):477-492.
- Okesenberg A, Arons E, Nasser K, et al. Severe obstructive sleep apnea: sleepy versus nonsleepy patients. Laryngoscope. 2010;120:643.
- Goodday RH, Bourque SE, Edwards PB. Objective and subjective outcomes following maxillomandibular advancement surgery for treatment of patients with extremely severe obstructive sleep apnea (AHI >100). J Oral Maxillofac Surg. 2015 Jul 20.
- Doff MHJ, Jansma J, Schepers RH, Hoekema A. Maxillomandibular advancement surgery as alternative to continuous positive airway pressure in morbidly severe obstructive sleep apnea: a case report. Cranio. 2013.
- Butterfield KJ, Marks PLG, McLean L, Newton J. Linear and volumetric airway changes after maxillomandibular advancement for obstructive sleep apnea. J Oral Maxillofac Surg. 2015;73:1133-1142.
- Holty JE, Guilleminault C. Maxillomandibular advancement for the treatment of obstructive sleep apnea: a systematic review and meta-analysis. Sleep Med Rev. 2010;14(5):287-297.
- Boyd SB, Walters AS, Song Y, Wang L. Comparative effectiveness of maxillomandibular advancement and uvulopalatopharyngoplasty for the treatment of moderate to severe obstructive sleep apnea. J Oral Maxillofac Surg. 2013.
- De Souza Carvalho AC, Magro Filho O, Garcia IR Jr, et al. Cephalometric and three-dimensional assessment of superior posterior airway space after maxillomandibular advancement. Int J Oral Maxillofac Surg. 2012;41:1102.
- Goodday RH, Bourque S. Subjective outcomes of maxillomandibular advancement surgery for treatment of obstructive sleep apnea syndrome. J Oral Maxillofac Surg. 2012;70:417.
- Boyd SB, Walters AS, Waite P, Harding SM, Song Y. Long-term effectiveness and safety of maxillomandibular advancement for treatment of obstructive sleep apnea. J Clin Sleep Med. 2015 Jul.
- John CR, Gandhi S, Sakharia AR, James TT. Maxillomandibular advancement is a successful treatment for obstructive sleep apnoea: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2018.
- Cillo JE Jr, Dattilo DJ. Maxillomandibular advancement for obstructive sleep apnea produces long-term horizontal advancement of the maxilla and mandible. J Oral Maxillofac Surg. 2019.
- Lye KW, Waite PD, Meara D, Wang D. Quality of life evaluation of maxillomandibular advancement surgery for treatment of obstructive sleep apnea. J Oral Maxillofac Surg. 2008 May.
- Friedman M, Wilson M. Re-redefining success in airway surgery for obstructive sleep apnea [comment]. Sleep. 2009;32(1):17.