





Integrating Substance Use Screening in Perinatal Care
Utilizing Patient and Staff Voices to Promote Screening Practices among Perinatal Patients with Substance Use Disorders
Essence Hairston, LCSW, LCAS, CCS¹*, Ahmad A Kittaneh, PhD¹, Elisabeth Johnson, PhD, FNP-BC, CARN-AP, LCAS¹, Andrea K. Knittel, MD, PhD³, Ashley Sutton, MD⁴, Alison Sweeney, MD⁴, Hendrée E. Jones, LP, PhD¹,²*
- Horizons Division and Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, Chapel Hill, NC 27510, [email protected]
- Departments of Psychiatry and Behavioral Sciences and Obstetrics and Gynecology, School of Medicine, Johns Hopkins University, Baltimore, MD 21224
- Division of General Obstetrics and Gynecology, Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC 27514
- Department of Pediatrics, University of North Carolina at Chapel Hill School of Medicine, UNC Healthcare, Chapel Hill, NC 27599
*Denotes first author status
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Hairston, E., et al., 2025. Utilizing Patients’ and Staff Voices to Increase Screening Practices among Perinatal Patients with Substance Use Histories. Medical Research Archives, [online] 13(7).
https://doi.org/10.18103/mra.v13i7.6642
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6642
ISSN 2375-1924
ABSTRACT
Objectives: National and international guidance recommends verbal screening to identify perinatal patients with substance use problems. However, perinatal patients report negative medical experiences and a rational fear of disclosing substance use due to negative consequences for disclosure. To improve screening experiences and accuracy, this study focused on the input of patients and staff with substance use disorders.
Methods: Participants were perinatal patients with substance use histories in a gender-specific treatment program (n = 6) or staff (peer support specialists, paraprofessionals, or Qualified Providers) working with perinatal patients (n = 14) in a gender-specific substance use disorder treatment program. Qualitative information was gathered in three ways: 1) focus groups with perinatal patients, 2) focus groups with paraprofessionals and QPs, and 3) three individual interviews were conducted. A descriptive phenomenological approach was used for analysis.
Results: The three themes that emerged from the perinatal patients with substance use histories group were provider fear of Child Protective Services (CPS), provider competency, and provider compassion. Three themes also emerged from the staff: methods to improve the assessment, concerns related to CPS, and challenges when working with healthcare professionals. Both groups recommended that (1) the screener’s introduction needs to provide information about CPS reporting, (2) patients receive a list of treatment resources, and (3) healthcare providers are trained in compassionate screening.
Discussion: Participants recommended that pregnant patients with substance use histories are more likely to share their substance use history if there is a sense of safety through compassionate care. Before screening, healthcare providers should be committed to seeking training to treat perinatal substance use, adopt stigma-free language, support autonomy to disclose substance use history due to previous encounters, and be transparent about the use of the information and outcome, and have treatment resources readily available to reduce the harms of mandatory reporting to CPS.
Keywords: Pregnancy, opioids, screening, substance use
Introduction
Perinatal alcohol and other substance use are common and addressing such use can lead to improved maternal and child outcomes. Alcohol continues to be the most commonly used substance among reproductive-aged women and perinatal women, with alcohol directly correlated to adverse outcomes (i.e., fetal alcohol spectrum disorder, FASD), despite opioid and opioid-poly illicit use being the leading cause of behavioral health overdose deaths and hospitalizations during the perinatal period.¹˒² Between 2017–2020, alcohol and substance use increased by over 80% among pregnant women.¹˒³ On average, 10–14% of pregnant women report using alcohol during pregnancy, and binge drinking at least once in the past 20 days.²˒³ In terms of opioid and opioid-poly use, about 7% of pregnant women reported using opioids,⁴ and about 5–8.3% of pregnant women reported using an illicit substance in the past 30 days.⁴˒⁵ About 630,000 infants are born with FASD,⁶ and substance use exposure during utero increased by 380% during 2002–2012 when neonatal abstinence syndrome (NAS) is documented.⁴˒⁷
Despite the adverse outcomes of alcohol and illicit opioids and other substances during pregnancy, and the prevalence of FASD and NAS among infants, screening and care planning that improve maternal-infant outcomes continue to be under-utilized and understudied.¹˒⁸˒⁹ A universal screening practice in healthcare settings can prevent, mitigate, and improve the quality of life for the perinatal patient and infant. However, to refer, treat, and provide care recommendations, the maternal-infant dyad must be adequately screened and detected for associated risks.⁹
Undetected, alcohol and illicit substances are also intertwined with co-occurring perinatal conditions.¹˒¹⁰ Research has indicated that reproductive-aged women and perinatal women with alcohol and illicit opioid and substance use histories are more likely to have experienced childhood and adulthood traumatic experiences predisposing them to developing a co-occurring condition (such as Post-Traumatic Stress Disorder, PTSD)¹⁰ or reinforcing the use of alcohol or illicit substances; as a result, furthering the complexities when caring for the population.¹˒¹⁰ Despite the benefits of reducing perinatal alcohol and substance use, such implementation to screen and identify alcohol or substance use has not been a standardized practice.⁸
To understand the complexities of implementation barriers, there is a need to understand the system-level (healthcare) and intrapersonal (and experiences of perinatal women with substance use histories) barriers that harmfully impact care engagement.¹˒² Healthcare settings can serve as a system-level to screen, refer, and employ interventions to mitigate adverse birth outcomes and other SUD-associated co-occurring conditions.¹˒²˒¹¹ While pregnancy is a protective factor,¹⁰˒¹² and an opportunity to increase care engagement among women with substance use histories, many healthcare institutions have yet to implement a universal screening tool for the identification of alcohol and substance use in pregnancy.¹˒⁸ Literature shows that implementation barriers can be associated with limited timing and staffing, unfamiliarity with tailored screening tools for the perinatal population, and training on how to care for perinatal substance use.²˒¹² Most women who enter prenatal care or a hospital setting will not be screened or assessed for alcohol or illicit opioid or substance use.¹¹˒¹³˒¹⁴ Among obstetricians, 79% frequently screen for substance use during pregnancy, yet only 11% use a validated instrument.¹⁴˒¹⁵ While national and international guidelines recommend the use of verbal screening tools, many providers use urine drug tests (often quick tests and not confirmed) to inform their clinical practice and reporting requirements. Such interventions utilizing urine drug testing to inform clinical referrals and recommendations can lead to ethically and legally harmful outcomes.¹˒¹⁶
While providers have their limitations in screening and detecting for alcohol or illicit opioid and other substance use,²˒¹² perinatal patients with substance use histories share that the potential outcomes of care engagement can be traumatizing.¹⁶˒¹⁷ Many perinatal patients identify federal and state mandatory reporting
and infant separation as a form of trauma.¹⁶˒¹⁷ While many providers screen for alcohol and illicit opioid use and other substances, not all providers or programs operate and treat perinatal substance use consistently.¹ Research has shown that a trusting alliance, compassionate care models, and collaboration among providers and perinatal women with substance use histories are associated with higher care retention.¹ Yet, for over 45 years, studies and court proceedings¹⁶˒¹⁷˒¹⁸˒¹⁹˒²⁰˒²¹ continue to reveal a disconnect between providers and perinatal patients with substance use histories.²˒¹⁰ Perinatal women with substance use histories continue to experience greater discrimination and bias in policies and healthcare settings compared to other populations and conditions.¹˒²² Specifically, studies that have examined race, socioeconomic statuses, and perinatal substance use outcomes at the time of delivery indicate that women of color,¹⁷˒²⁰˒²¹ uninsured,²³ and lower socioeconomic status²⁴˒²⁵ are more likely to be required to submit a urine sample for drug testing, referred to child welfare services, or experience criminalization when screened for substance use.¹⁷ When these overarching factors (stigma, fear, hospital trauma) exist, the individuals are more likely to internalize their shame and guilt, and may return to use and refuse to trust providers.¹⁰˒¹⁷
Early identification followed by a therapeutic response of brief intervention and referral to maternal-infant and co-occurring treatment is recommended by the U.S. Preventive Services Task Force and is effective in reducing substance use in pregnancy.¹˒¹³ While numerous validated screeners are acceptable for identifying problem substance use,¹⁰˒¹³ the 5Ps Screen for Alcohol/Substance Use tool has been widely accepted and used due to its indirect line of questions and specificity for the perinatal period.¹¹˒²⁶ The 5Ps Screen for Alcohol/Substance Use tool contains questions that query substance use by the pregnant woman’s parents, peers, partner, in her past, and/or current pregnancy.¹¹˒²⁶ Like any screener, how it is introduced may influence patients’ responses to the questions. While universal screenings are primarily used to detect perinatal substance use, screenings create a clinical pathway to address other SUD-related conditions among maternal-infant and treat co-occurring perinatal conditions.¹˒²˒¹⁸˒²⁷ As a result, creating an opportunity to optimize behavioral (overdose and mental health conditions) and physical health (postnatal and postpartum) outcomes throughout the perinatal trajectory.¹˒²˒⁸˒¹⁰ While previous qualitative studies have included patients’ and obstetricians’ reports,¹˒²⁸˒²⁹ there is minimal research that has investigated factors related to how healthcare providers introduce the screener and influence the ways pregnant and birthing patients with substance use problems may experience the screening questions.¹˒⁸ The purpose of the qualitative study was to improve the substance use screening experiences and accuracy by revising a screening prompt based on the input of patients and staff with substance use disorders.
Methods
All study procedures were approved by the University of North Carolina at Chapel Hill Institutional Review Board (IRB# 22-2915). Individuals consented to participate in the study.
Participants
All participants were recruited using two forms of purposeful sampling: critical case and homogeneous sampling. Purposeful sampling is an intentional approach to uplift the voices of populations who are not always given opportunities to be heard and gather information from those who are informed about the specific topic of focus. Critical case sampling was used to identify perinatal patients with substance use histories. Participants were selected from those residing in a perinatal substance use disorder residential treatment program and engaging in a specific group therapy in North Carolina (n=6). Participants provided informed consent for the evaluation team to ask questions about the 5Ps screening prompt in a group setting as a form of quality improvement and service provision. Homogeneous sampling was used to recruit peer support specialists, who were working in a healthcare system or perinatal SUD residential treatment
program, and paraprofessionals and qualified professionals (QPs) working in a perinatal and maternal outpatient or residential programming in North Carolina (n=14) based on their connection to the perinatal SUD community. Six participants were in the perinatal patients with substance use histories focus group, eleven staff, and three individual interviews were conducted with two peer support specialists and one QP. All individuals who were approached for participation agreed, and no potential participants were ineligible or refused. EH led the focus groups and interviews. To reduce participant influence and bias, none of the participants in the study were receiving clinical services, clinical staff training, or supervision from EH.
Treatment Setting and Time
The two focus groups and individual interviews were collected over a week via a HIPAA-compliant telehealth platform in December 2022. The facilitator of the treatment group educated the perinatal participants with substance use histories about quality improvement and assurance efforts to evaluate service provision. The facilitator informed the perinatal participants with substance use histories that the research and evaluation team aimed to gain a deeper understanding of patients’ experiences when seeking care in a healthcare setting. The group provided consent to share their experiences. Treatment groups are closed sessions among perinatal women and families actively enrolled in an enhanced outpatient program and residential program. The HIPAA-compliant Zoom platform was utilized due to the coronavirus pandemic and safety measures related to evaluation and quality improvement tasks. Similarly, the research and evaluation team identified peer support specialists and qualified professionals who have worked in a high-risk prenatal SUD care clinic, a perinatal SUD outpatient program, or a residential program for SUD in North Carolina. The peer support specialists and qualified professionals in the focus group met via the HIPAA-compliant Zoom platform. The three individual interviews took place in person, adhering to social distancing requirements in a conference space at the outpatient program. The outpatient treatment setting is uniquely designed for pregnant and parenting women and their children and families, offering childcare and parenting support when needed.
Procedures
EH gathered information from patients in a perinatal and maternal program (n=6) in a one-hour focus group via a HIPAA-compliant telehealth platform. Each participant read a draft prompt that was developed by a Working Group at our institution as part of the “comprehensively lessening Opioid Use Disorder impact” prenatal pilot initiative of the Perinatal Quality Collaborative of North Carolina:
“I have several questions for you to complete about substance use. We ask all our pregnant patients these questions because we care about all aspects of your health. The more you can tell us about your health, the better we will be able to care for you and your pregnancy. The provider will talk with you about your answers shortly. If you answer yes to the questions included in this screener, we will provide additional resources and support. If you have more questions regarding how this information will be used, talk with your healthcare provider.”
In addition to the main prompt, perinatal participants with substance use histories were asked three follow-up questions:
-
Would you feel comfortable answering the following questions in a healthcare setting as a pregnant or birthing person with a history of substance use during pregnancy or postpartum?
-
If not, what would increase the chances for a pregnant or birthing person with substance use disorder to feel comfortable answering these questions?
-
Would you add or remove language from the original prompt?
Information from the peer support specialists, paraprofessionals, and qualified providers was
gathered in a one-hour focus group via a HIPAA-compliant telehealth platform. Similarly, read the prompt and were asked the two follow-up questions below:
-
If not, what would increase the chances for a pregnant or birthing person with substance use disorder to feel comfortable answering these questions?
-
Would you add or remove language from the original prompt?
DATA ANALYSIS
Thematic analysis was conducted using information from the follow-up questions to adjust the original prompt. Coding was done by hand, and the research team generated initial codes upon re-reading the text. Coding was done broadly to allow for as many potential themes as possible. Codes were then sorted into potential themes, and connections between themes were discussed and finalized with the co-authors. After two focus groups and three individual interviews, the same themes emerged:
-
Fear of child protective services,
-
Provider competency,
-
Provider compassion,
-
Methods to improve the assessment/prompt,
-
Concerns related to CPS,
-
Challenges working with healthcare settings.
Albeit a small sample size, the determination of saturation was met, given that no new themes emerged. Participants were provided with a written copy of the qualitative data collected during the two focus groups to ensure accuracy of the language used to initiate a revision prompt. Similarly, the three individual sessions were also provided with data collected from their interviews to ensure the language captured reflected the participants’ words. Once the perinatal patients with substance use histories, peer support specialists, paraprofessionals, and QPs confirmed accuracy, the evaluation team compiled information from the two focus groups and three individual sessions to create a revised suggested 5Ps prompt based on the themes identified and reflecting the language provided by participants. To ensure accuracy and inclusion of all voices, a member-checking process was conducted to ensure the accuracy and approval from all participants of the newly revised prompt. The member checking process was conducted by EH reaching out to all participants (N=20) to review and give final approval of the revised prompt.
Results
Six themes were identified from the participant groups. The three themes that emerged from the perinatal participants with substance use histories group were fear of CPS, provider competency, and provider compassion. The three themes from the peer support specialists, paraprofessionals, and QPs (staff) included methods to improve the assessment, concerns related to CPS, and challenges when working with healthcare professionals. Two themes overlapped and shaped the final outcomes found in the discussion section. The full results can be found in Table 1.
PARTICIPANT THEMES: PERINATAL WOMEN WITH SUBSTANCE USE PROBLEMS
Theme 1: Fear of Child Protective Services.
Participants in the group discussed fear of caregiver-infant separation, “fear of CPS getting involved.” It is well-documented that perinatal women are hesitant to seek care due to loss of custody or parental rights³⁰˒³¹. The perinatal participants with substance use histories group also indicated mistrust among CPS workers, and many participants agreed that “even if CPS says that reunification is the plan, that isn’t always the case.” While keeping custody is the primary goal when CPS is involved, not all women can regain custody of their infant or child if a CPS report has been made. Lastly, other subthemes related to CPS were the emotional trauma that results from the CPS report and involvement, sharing that “(CPS) disrupts the kid’s mental health and mom’s mental health.”
Table 1. Qualitative Themes as exemplified by quotes from participants.
| Patients | Patient themes | Patient Quotes |
|---|---|---|
| Patients | Fear of CPS | “Fear of CPS getting involved”, “even if CPS say that reunification is the plan, that isn’t always the case” and “they [CPS] disrupt the kid’s mental health and mom’s mental health” (Pregnant/birthing woman in treatment) |
| Provider competency | “Some places don’t even know about the treatment options during pregnancy.” (Pregnant/birthing woman in treatment) | |
| Provider Compassion | “It would take a certain type of person who really cares to do this screening and trained to do this work like a peer support specialist or substance use counselor” “someone that will not judge us” (Pregnant/birthing woman in treatment) | |
| “It is hard to be open and honest with a doctor” (Pregnant/birthing woman in treatment) | ||
| “I’ve had s**** doctors and providers, and I wouldn’t feel comfortable with it.” “I don’t know if people just don’t want to get the training or what, but providers will still look at you in disgust.” | ||
| Peer Support Specialists and Paraprofessionals | Concerns related to CPS | “Will staff be responsible to report to CPS if the mother has substance use?” (Peer support working in a healthcare setting) |
| “Will staff be responsible to report to CPS if someone refuses to do the screening?” (Peer support working in a perinatal and residential treatment setting) | ||
| “It should say something like we can’t ensure that CPS won’t be contacted later on and be honest about what could happen.” (Paraprofessional working in a perinatal substance abuse residential treatment program) | ||
| “I would like to know what are the policies around CPS” (Qualified Professional working in a perinatal and maternal substance abuse outpatient treatment program) | ||
| Methods to improve assessment/prompt | “Can a substance use provider do the assessment and connect the patient to treatment.” (Peer support working in a healthcare setting) | |
| “the client should be informed of how the information will be used beforehand – not after the completion of screening.” (Paraprofessional working in a maternal substance use disorder residential treatment program) | ||
| Challenges when working with healthcare providers | “It can be difficult to have someone share their experiences about SU.” (Peer support working in a perinatal and residential treatment setting) |
Theme 2: Provider Competency
The focus group discussion of perinatal participants with substance use histories focused on the importance of a trained professional or peer support specialist with experience in caring for substance use during the perinatal period. Studies show that many healthcare providers are not trained in screening, treating, or referring as it relates to caring for perinatal patients with substance use problems³⁰˒³¹. Other pregnant and birthing participants supported a statement made by one perinatal participant with substance use histories: “It would take a certain type of person who really cares to do this screening and trained to do this work like a peer support specialist or substance use counselor.” The lack of training in screening leads to undetected perinatal treatment needs and disproportionately impacts access to care among pregnant and birthing patients compared to non-pregnant or postpartum patients¹˒¹⁰˒³¹. The perinatal participants with substance use histories also discussed the importance of providers having community-based resources and assistance in care coordination readily available if an individual desired treatment during the screening. Although the screening and referral components are critical, there is a gap in the next steps of SBIRT implementation, brief interventions, and treatment.¹˒⁸˒¹³˒¹¹ Many healthcare providers are not equipped or knowledgeable about the resources to support perinatal participants with substance use histories¹⁹˒³⁰˒³¹. One perinatal participant acknowledged that providers are unaware of the community-based resources, “some places don’t even know about the treatment options during pregnancy.”
Theme 3: Provider Compassion
Caring for perinatal patients with substance use histories requires compassionate and evidence-based interventions and practices. Compassionate care encompasses non-stigmatizing words and behaviors, promote shared-decision making.¹ Perinatal participants with substance use histories emphasized that an ideal characteristic of the screener would be “someone who will not judge us.” The use of compassionate language empowers patients to feel seen and validated.¹˒¹⁰. When employed correctly, compassionate care ensures that any negative tones or stereotypes are removed when talking to or about the client (i.e., a person living with a substance use disorder, a person seeking assistance for their substance use disorder, or concern).¹˒⁸ On the other hand, non-compassionate language and practices induce bias and stigma that reinforce hesitancy among perinatal patients with substance use histories to seek care.¹˒²⁸˒³²˒³³ When individuals have mistrust of providers, their willingness to engage in screening processes decreases.¹˒²⁸ One participant expressed, “It is hard to be open and honest with a doctor,” and another shared, “I wouldn’t feel comfortable with it.” Other participants acknowledged that even when training exists, providers will continue to struggle with bias and acting out stigmatizing behaviors in practice. One participant mentioned, “I don’t know if people just don’t want to get the training or what, but providers will still look at you in disgust.”
PARTICIPANT THEMES: RECOVERY PEER SUPPORT SPECIALISTS AND QUALIFIED PROFESSIONALS
Theme 1: Methods to Improve the Assessment/Prompt
Upon reading the initial prompt, the peer support, paraprofessionals, and QPs discussed modifying the screening prompt to inform patients of how the information gathered from the 5Ps screening tool will be used. One comment shared and received support from the larger group added, “the client should be informed of how the information will be used beforehand—not after the completion of screening.” The comment elicited discussions around fear, confidentiality, and the importance of informed consent. The discussions among the peer support specialists, paraprofessionals, and QPs participant group birthed the idea of modifying the script to promote autonomy, transparency, and honor the client’s privacy before facilitating screening. The peer support, paraprofessionals, and QPs offered to revise the screening prompt and encouraged
the perinatal participants with substance use histories group to make any necessary changes or modifications.
Theme 2: Concerns Related to CPS
CPS was referenced throughout the study among peer support specialists in healthcare settings, paraprofessionals, and qualified professionals. Understanding the impact of CPS involvement on unmanaged substance use during pregnancy, the staff were interested in exploring autonomy and confidentiality related to CPS referral and involvement. Specifically, the staff asked questions about informed consent and mandating reporting laws regarding substance use during pregnancy.
Theme 3: Challenges when Working with Healthcare Professionals
The peer support, paraprofessionals, and QPs participants shared about the difficulties in cultivating relationships among healthcare professionals. Peer support specialists shared about their lived experiences entering healthcare facilities and feeling shame, guilt, and judged at the time of delivery. A peer support specialist working in a perinatal and maternal residential program, “It can be difficult to have someone share their experiences about SU” in a healthcare setting, acknowledging the fear and potential outcomes if someone discloses their substance use history. For decades, anti-drug and mandatory reporting policies related to substance use during pregnancy have enabled healthcare professionals to be implicit in the criminalization of substance use during pregnancy.¹⁹˒²² The fear of being penalized due to their unmanaged substance use adversely impacts perinatal patients with substance use histories, and their willingness to trust and seek care.⁸˒²³˒²¹
The shared themes among both groups recommend that (1) the screener’s introduction needs to provide information about CPS reporting, (2) patients should receive a list of gender-specific treatment resources, and (3) healthcare providers need to be trained in compassionate and non-stigmatizing screening practices.
REFINING THE 5Ps PROMPT
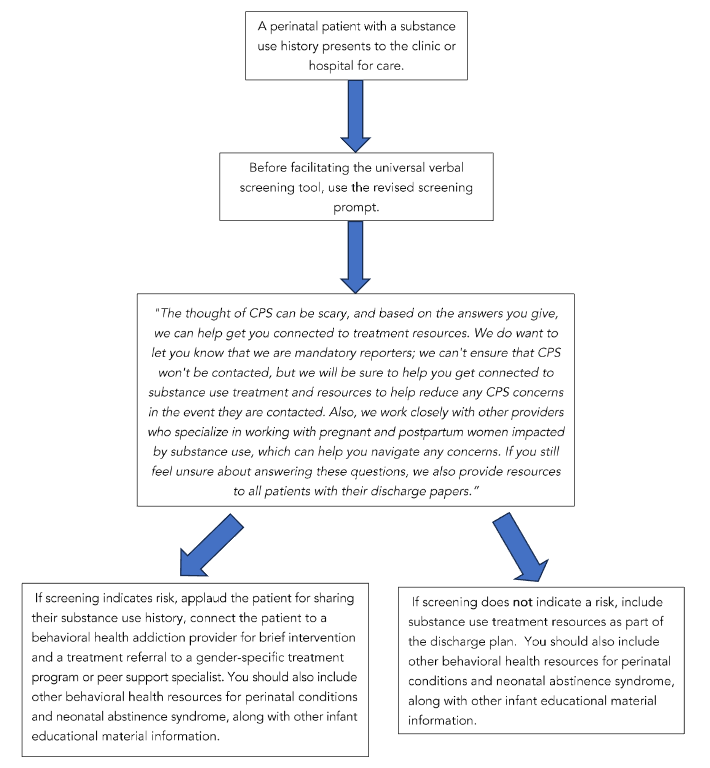
Participants from the peer support specialists, paraprofessionals, and QPs group expressed the importance of honoring autonomy, informing patients about the use of the screening, and how and what information will be shared with CPS due to mandatory reporting laws. The participants recommended a revised screening prompt. Participants supported the use of the prompt before facilitation of a perinatal/postnatal substance use screen (Figure 1):
“The thought of CPS can be scary, and based on the answers you give, we can help get you connected to treatment resources. We do want to let you know that we are mandatory reporters; we can’t ensure that CPS won’t be contacted, but we will be sure to help you get connected to substance use treatment and resources to help reduce any CPS concerns in the event they are contacted. Also, we work closely with other providers who specialize in working with pregnant and postpartum women impacted by substance use, which can help you navigate any concerns. If you still feel unsure about answering these questions, we also provide resources to all patients with their discharge papers.”
Discussion
Given the hesitancy among perinatal patients to disclose their substance use during pregnancy,²²˒³¹ there is a need to identify how healthcare systems can consider factors that impede care engagement.¹˒⁸ The themes that emerged from this study align with previous qualitative findings,¹²˒²⁴˒²⁹ adding to the qualitative literature that has documented patients’ fear and hesitancy to access care. While the overlapping themes include fear of child protective services among all participants, a critical aspect of the importance of language and the use of information shared when revising the screening prompt was deemed pivotal. Likewise, another essential finding from this study was that the shared decision among the two focus groups and individual interviews highlighted the importance of compassion and transparency in child welfare services referrals.
Therefore, there is a need to understand what clinical training, staff credentials, and treatment referrals are most available when perinatal women indicate a history of substance use at the time of healthcare or prenatal visits.
While this study builds upon previous literature on evolving peer support specialists and qualified professionals providing behavioral health addiction treatment, the study extends with an opportunity to increase care engagement by using a pre-screening prompt. Another strength of the study is that it is prospective, patient-centered, and highly participatory. However, it has limitations. One major limitation is the small sample size, which does temper the conclusions’ strengths. Albeit a small sample, the findings align with previous qualitative studies among perinatal patients¹²˒²⁹ that captured lived experiences. Based on shared commonalities among previous qualitative studies¹²˒²⁹, and the findings from the current study, the research team confirms that no new themes emerged; therefore, saturation was met. Secondly, another limitation is the coronavirus (COVID-19) affecting recruitment and sample selection. Due to the COVID-19, the ability to recruit more outpatient perinatal participants with substance use histories impacted the sample size. Although the treatment program is equipped to meet the needs of pregnant and parenting women and their children, the families enrolled in outpatient treatment may have had issues with internet or connecting issues, parenting minor children due to closed childcare centers.³⁴˒³⁵ Likewise, convenience sampling was also a limitation of the population, impacting recruitment. North Carolina has more than 26 programs for pregnant and parenting individuals, and the expansion of recruitment and sampling would have enhanced the studies. To fully understand reporting substance use during pregnancy, future research would expand on the qualitative findings through a more expansive recruitment approach among the 26 perinatal and pregnant gender-specific treatment programs, including perinatal women with substance use histories leaving jails and prisons to capture the lives of perinatal subpopulations.
Additionally, a future study could implement the screening prompt as an intervention that is tested and evaluated on the acceptability and feasibility among perinatal women with substance use histories in North Carolina. Therefore, a more robust mixed-methods study will be able to identify factors further to advance the implementation of an evidence-based screening tool in healthcare settings.
Conclusion
Albeit a small qualitative study of pregnant patients with substance use histories and substance use treatment program staff (N=20), the findings from this qualitative aligns with previous studies and publications, indicating fear of caregiver-infant separation, lack of addiction training, and provider compassion being contributing factors among perinatal patients to seek care and share about their SUD.¹˒⁸˒¹¹˒¹³˒¹⁴ While this study reinforces what we know about increasing barriers to care engagement, this study could be the first of its kind to help understand factors associated with screening barriers in a healthcare setting and future opportunities to evaluate and test the implementation of a screening prompt. Further, the study expands on why barriers and challenges exist and provides a solution on how to overcome those pitfalls. This study provides an opportunity for system and intrapersonal improvement. The most significant finding from this study is the need to conduct a field study among a larger perinatal patient population and to assess acceptability and feasibility within healthcare systems. Other significant highlights are addressing care and policy responses to reduce intrapersonal challenges among perinatal patients with substance use histories, such as internalized fear, stigma, and shame among perinatal patients with substance use histories. To improve patients’ trust at the time of care engagement, it is essential to adopt the following recommendations based on perinatal patients with substance use histories: 1) Inform patients of their rights and mandatory reporting laws 2) Acknowledge the fear of CPS involvement and mitigate those fears and inequities, 3) Provide gender- and family-specific referral treatment options for all perinatal patientsand their families, 4) Engage in training that enhances strategies to treat substance use during pregnancy and hired addiction providers trained to care for perinatal patients with substance use histories, 5) Increase compassion. Based on our findings, we also recommend that clinical entities evaluate planned screening implementation by obtaining feedback from perinatal patients with substance use histories before the implementation of universal screening. The revised screening prompt created from the participants is one of many steps that can be implemented and studied to increase care engagement, promote health equity for perinatal people with substance use histories, and identify factors that create challenges and barriers (Figure 1).
Acknowledgments:
We would like to thank members of the Perinatal Quality Collaborative of NC, the 5P’s working group on implementing universal SUD screenings to detect substance use or misuse, and the patients and staff for their time.