





Bradasch Technique for Mandibular Position in TMD Patients
Clinical Use of the Bradasch Technique for Mandibular Position Transfer in Asymptomatic Temporomandibular Disorder Patients
Matias KYM ¹; Beckers P ²; Kubiak RJF ³; Hümmelgen LH ⁴; Ravazzi GMNC ⁵; Gonçalves FM ⁶, Stechman-Neto J ⁷.**
- Postgraduate Program in Dentistry, Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0000-6511-4293
- Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0005-1648-6206
- Postgraduate Program in Dentistry, Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0003-3826-2850
- Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0008-5306-6448
- Postgraduate Program in Human Communication Health, Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0002-6574-9878
- Postgraduate Program in Human Communication Health and Postgraduate Program in Dentistry, Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0002-7972-2844
Postgraduate Program in Human Communication Health and Postgraduate Program in Dentistry, Tuiuti University of Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0002-0259-2420📧 [email protected]
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Matias, KYM., Beckers, P., et al., 2025. Clinical Use of the Bradsach Technique for Mandibular Position Transfer in Asymptomatic Temporomandibular Disorder Patients. Medical Research Archives, [online] 13(7).
https://doi.org/10.18103/mra.v13i7.6791
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6791
ISSN 2375-1924
Abstract
Background: Precise occlusal diagnoses and rehabilitation following temporomandibular disorder management demand reliable replication of mandibular positioning. The Bradasch technique provides a standardized method for transferring a therapeutically stabilized mandibular position to a semi-adjustable articulator.
Objective: To describe the clinical protocol and methodological basis of the Bradasch technique for transferring mandibular position following neuromuscular stabilization using an occlusal splint.
Methods: A patient with temporomandibular disorder underwent stabilization with a flat, smooth occlusal splint incorporating anterior and canine guidance. After 60 days of symptom remission, facial arch registration transferred the mandibular position to a semi-adjustable articulator. It calibrated incisal pin adjustment, enabling occlusal analysis in a therapeutic position.
Results: The technique identified occlusal interferences and discrepancies between maximum intercuspation and orthopedic mandibular comfort position. This guided accurate diagnostic and rehabilitative planning.
Conclusion: This case report illustrates the potential of the Bradasch technique to enable precise transfer of a therapeutically stabilized mandibular position using a semi-adjustable articulator. Although the outcome was favorable in this individual case, broader clinical studies are necessary to validate the generalizability and diagnostic utility of the technique.
Keywords: Occlusal splint, articulator, mandibular position, prosthodontic rehabilitation.
Introduction
Temporomandibular disorder (TMD) is an umbrella term for pain and dysfunction involving the masticator muscles and the temporomandibular joints (TMJs). They are the most common orofacial pain conditions. Its prominent features include regional pain in the face and preauricular area, limitations in jaw movement, and noise from the TMJs during jaw movements 1. The global prevalence of TMD is estimated to be approximately 31% in adults and older people 2, with a higher incidence in women, particularly between the second and fourth decades of life 3.
Although the etiological role of dental occlusion in TMD has been debated, recent literature suggests that occlusion alone does not cause TMD; it can be a perpetuating or predisposing factor 3. Therefore, occlusal assessment remains essential during diagnosis and treatment planning. Studies have shown that occlusal discrepancies may contribute to increased muscular activity and proprioceptive confusion, which can perpetuate orofacial pain 4.
Occlusal appliance therapy is one of the most commonly used treatments for TMD pain, with stabilization appliances being the type most often recommended. The treatment is reversible and atraumatic and may induce relaxation of the jaw muscles, unload the TMJs, and protect the teeth from wear due to bruxism 1. The primary goal of contemporary TMD management is to restore functional balance within the stomatognathic system, alleviate pain, and reestablish joint and muscular coordination. When correctly adjusted and monitored, they significantly contribute to lowering TMJ overload and normalizing muscle function 5,6.
Once clinical stabilization is achieved, clinicians must rehabilitate the patient based on a therapeutically stable mandibular position. This process demands precision in transferring the neuromuscularly deprogrammed mandibular posture to the planning articulator. In this context, semi-adjustable articulators (SAAs) are essential for replicating mandibular movements and occlusal contacts 7-9.
Transferring this position to a semi-adjustable articulator (SAA) allows detailed analysis of occlusal relationships, identification of premature contacts, and informed prosthodontic or orthodontic planning 9,10. The Bradasch technique, developed for this purpose, enables accurate registration and replication of the mandibular position attained during successful TMD therapy. It offers a systematic approach for clinicians to finalize cases with improved predictability.
This article presents the Bradasch technique, contextualizing its clinical application and value in transferring the therapeutic mandibular position to an SAA following TMD stabilization.
Clinical Management
A female patient, 30 years old, with diagnoses myogenous TMD and associated occlusal instability, underwent a treatment protocol development at the CDATM, University of Tuiuti of Paraná. Neuromuscular stabilization was achieved using a flat occlusal splint (hard acrylic, anterior and canine guidance). After 60 days of symptom remission and clinically verified occlusal stability, the following transfer steps were performed:
Impressions and Model Preparation:
Maxillary and mandibular impressions were taken using alginate (Figure 1A). The casts were poured (Figure 1 B), prepared with stabilization grooves, and kept hydrated until use (Figure 1C).
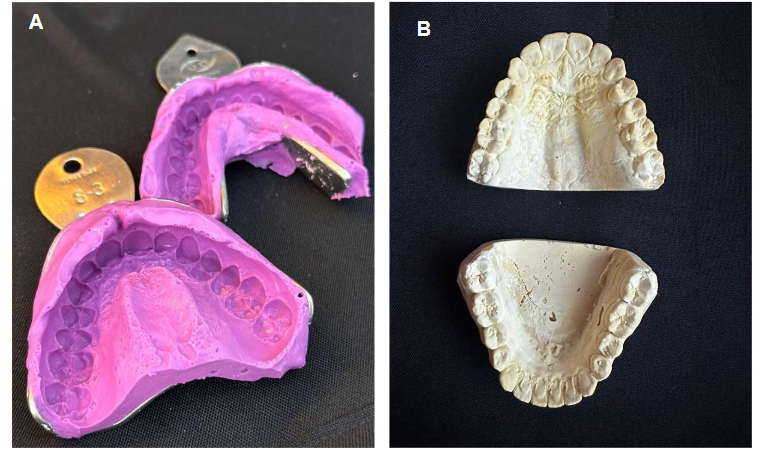
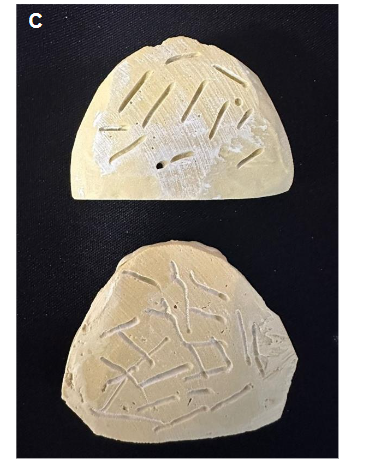
Impression Note: A. impression using alginate. B. Models. C. additional retentions
Facebow Transfer and Mounting:
The maxillary cast was transferred to the BioArt™ 4000s articulator using the facebow, following the manufacturer’s instructions.
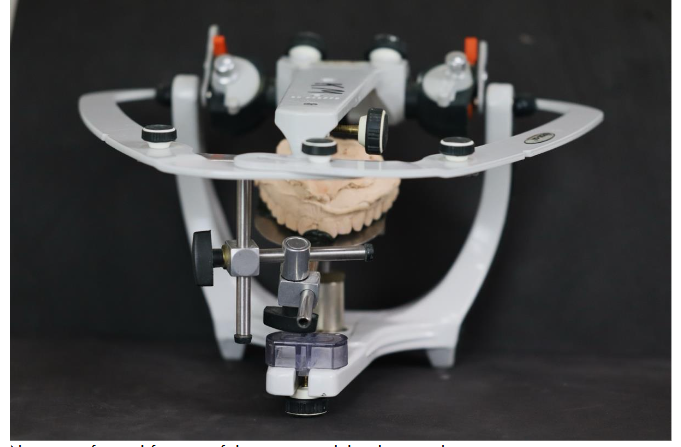
Record on the Splint:
The intermaxillary record was obtained with the splint in place, using low-fusing modeling compound at contact points. The patient was instructed to occlude in the orthopedic stability position (Figure 3).

Measurement of Interincisal Distance:
Vertical distances were measured with and without the occlusal splint using a caliper, based on consistent reference points on the maxilla and mandible (Figure 4A, 4B).

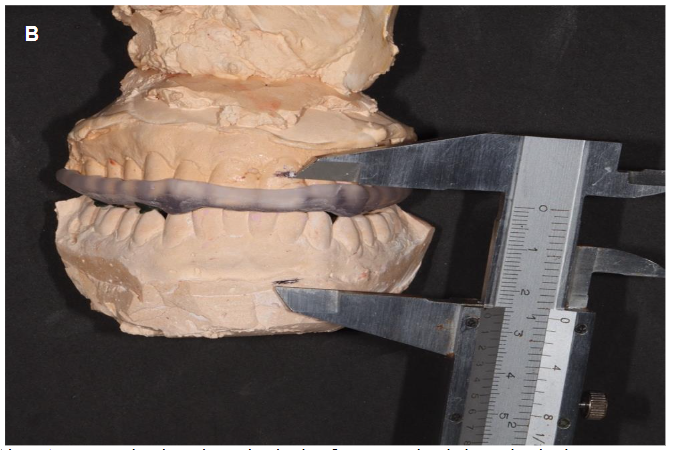
Note: A. measured without the occlusal splint. B. measured with the occlusal splint
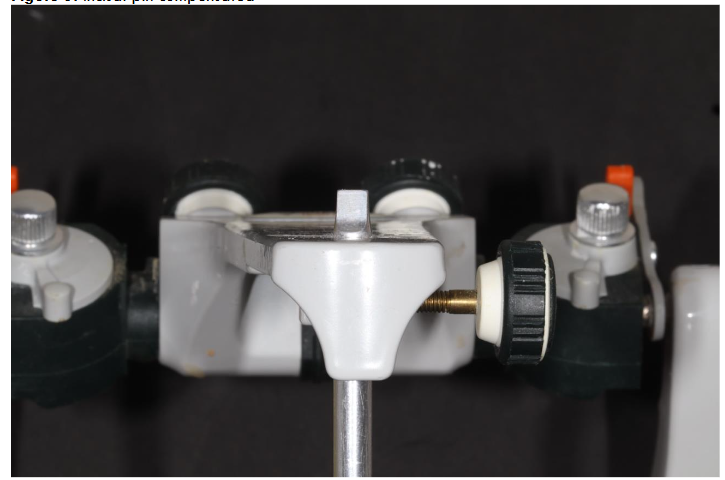
Incisal Pin Adjustment:
According to clinical protocols, the difference between vertical measurements was multiplied by 1.5 to compensate for the splint thickness and transferred to the incisal pin [3,x = (A − B) ∗ 1,5 (figure 5) “x” represents the distance to be compensated on the incisal pin; “A” is the vertical dimension without the splint; “B” is the vertical dimension with the splint.
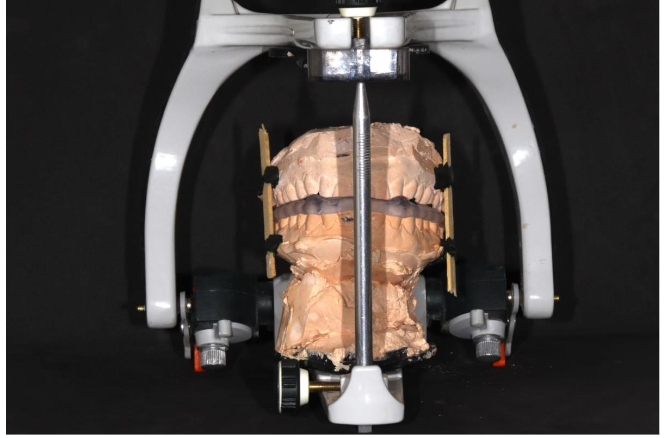
Mounting of the Mandibular Cast:
After mounting the maxillary cast with the splint in place, the mandibular cast was adapted using the intermaxillary record (in modeling compound), and the incisal pin height was adjusted (Figure 6).
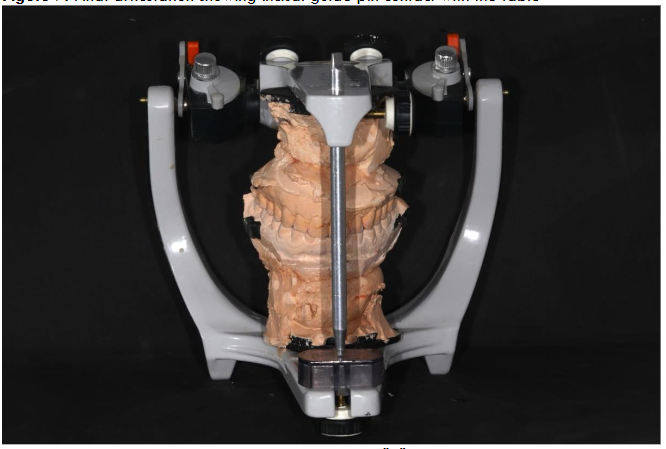
Occlusal Contact Analysis:
Final articulation was performed with the splint removed and the incisal pin returned to zero. Primary occlusal contacts were marked, and adjustments were made to verify and maintain the position of orthopedic stability (Figure 7).
Discussion
This case report demonstrates the clinical applicability of the Bradasch technique as a tool for transferring a therapeutically stable mandibular position to a semi-adjustable articulator. This method offers a reliable means of simulating occlusal dynamics, allowing clinicians to perform detailed occlusal adjustments and ensure long-term rehabilitation stability. Nevertheless, given the nature of this single-case design, results must be interpreted with caution. Further research involving controlled clinical trials is needed to validate the reproducibility and efficacy of the Bradasch technique across broader patient populations. Future integration with digital articulator systems and intraoral scanners may expand the scope and accessibility of this technique11.
Multiple authors emphasize the importance of neuromuscular deprogramming in temporomandibular disorder patients, aiming to break the habitual proprioceptive pattern sustained by the periodontal ligaments and neuromuscular reflexes12-14. Valle RT, Grossmann E(2019) emphasize that habitual intercuspation is often a conditioned response, rather than a reflection of orthopedic stability15. Deprogramming enables clinicians to achieve a mandibular position that reflects muscular relaxation and joint comfort, rather than habitual function. Various techniques exist for this purpose, including bilateral manipulation, occlusal JIGs, neuromuscular deprogramming appliance (NDA), TENS devices, and occlusal splints12,13.
In this context, occlusal devices are particularly significant. Not only do they provide symptomatic relief, but they also enable gradual neuromuscular adaptation and allow for the identification of a reproducible condylar position, if the patients need rehabilitation treatment. Silva (2008) and Okeson (2021) argue that occlusal devices act as a temporary neuromuscular guide, altering the vertical and horizontal mandibular dimensions and fostering a new balance between muscles, joints, and teeth14.
A pivotal clinical dilemma is whether the final rehabilitative occlusion should be guided by the maximum intercuspation, habitual, or stabilized position reached through the occlusal device. Studies suggest that post-treatment mandibular posture differs significantly from occlusal devices, particularly after successful temporomandibular disorder management 16.
This supports the concept that the orthopedic comfort position, determined through occlusal splint therapy, should be the basis for prosthetic planning. Rehabilitation work is necessary for the patient, and it must be for rehabilitation, not for treating TMD17. However, this position must be accurately transferred to a physical model to be advantageous diagnostically. This is where the Bradasch technique demonstrates clinical value.
The Bradasch technique provides a standardized protocol to transfer the stabilized mandibular position to a semi-adjustable articulator (SAA), ensuring the fidelity of occlusal records and enhancing diagnostic reliability. Using a formula-based adjustment for incisal pin compensation, derived from interincisal measurements with and without the occlusal distance (OD), ensures that the altered vertical dimension introduced by the OD is respected during mounting.
This reproducibility is essential because the traditional MIH position often hides occlusal interferences, posterior discrepancies, or deviations in the closure trajectory that only become evident when analyzing the casts in the SAA under a therapeutic mandibular position 8 reinforces that mounting on an SAA provides a three-dimensional understanding of occlusal contacts free from neuromuscular adaptation or proprioceptive bias.
Predictability and Limitations
The Bradasch technique also addresses a frequent challenge. The method mitigates errors and enhances communication with rehabilitative teams in clinical practice, such as the lack of predictability in mounting procedures, by providing clear steps, from occlusal stabilization to model mounting and incisal pin calibration.
Nonetheless, some limitations persist. The technique requires technical proficiency and a clinician’s familiarity with articulator handling. The process may be complicated in digital workflows due to the need for physical impressions and cast generation. Additionally, time is a factor: stabilization using ODs often takes weeks to months, which may challenge patient adherence.
Despite these limitations, the technique is a valuable, evidence-based approach for clinicians seeking precision in post-TMD rehabilitation. It aligns with the modern principles of minimally invasive dentistry, where the clinician must respect the adaptive capacity of the patient’s stomatognathic system while ensuring that occlusal relationships are functionally and anatomically sound.
Future Integration with Digital Dentistry
An emerging area of interest is the integration of techniques like Bradasch into digital workflows. While traditional methods rely on physical impressions and articulator mounting, advances in digital articulators and intraoral scanning have opened up possibilities for the virtual transfer of therapeutic mandibular position8,18. However, more studies are needed to validate these digital methods’ accuracy and clinical equivalence, especially in complex rehabilitative cases following successful TMD treatment.
Summary of Contributions
- Reinforces the importance of post-treatment mandibular stabilization in successful TMD cases when patients need rehabilitation treatment
- Validates the use of occlusal splints for neuromuscular deprogramming.
- Provides a reproducible method (Bradasch) for transferring therapeutic positions to SAAs.
- Enhances diagnostic accuracy for subsequent prosthetic planning.
- Offers a bridge between analog and digital prosthodontic workflows.
Conclusion
This case report demonstrates the clinical feasibility of using the Bradasch technique to transfer a therapeutically stabilized mandibular position to a semi-adjustable articulator. While the results are promising, further studies with larger samples must confirm their reproducibility and clinical impact in broader prosthodontic rehabilitation settings.
Conflicts of Interest Statement:
The author declares no conflict of interest.
Funding Statement:
No funding was received for this study.
References
- List T, Jensen RH. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia. Jun 2017;37(7):692-704. doi:10.1177/0333102416686302
- Valesan LF, Da-Cas CD, Réus JC, et al. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig. Feb 2021;25(2):441-453. doi:10.1007/s00784-020-03710-w
- Manfredini D, Lombardo L, Siciliani G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: end of an era? J Oral Rehabil. Nov 2017;44(11):908-923. doi:10.1111/joor.12531
- Kalladka M, Young A, Thomas D, Heir GM, Quek SYP, Khan J. The relation of temporomandibular disorders and dental occlusion: a narrative review. Quintessence Int. Apr 5 2022;53(5):450-459. doi:10.3290/j.qi.b2793201
- Garrigos-Pedron M, Elizagaray-Garcia I, Dominguez-Gordillo AA, Del-Castillo-Pardo-de-Vera JL, Gil-Martinez A. Temporomandibular disorders: improving outcomes using a multidisciplinary approach. J Multidiscip Healthc. 2019;12:733-747. doi:10.2147/JMDH.S178507
- De Leeuw R, Klasser GD. Orofacial pain: guidelines for assessment, diagnosis, and management. Fifth ed. American Academy of Orofacial Pain. Quintessence Publishing Co, Inc.; 2018.
- Clark JR, Hutchinson I, Sandy JR. Functional Occlusion: II. The Role of Articulators in Orthodontics. Journal of Orthodontics. 2001;28(2):173-177. doi:10.1093/ortho.28.2.173
- Buduru S, Finta E, Almasan O, et al. Clinical occlusion analysis versus semi-adjustable articulator and virtual articulator occlusion analysis. Med Pharm Rep. Jul 2020;93(3):292-296. doi:10.15386/mpr-1595
- Jeong MY, Kim MJ, Lim YJ, Kwon HB. Evaluation of eccentric tooth contact on a semi-adjustable articulator by using an occlusal analysis system. The Journal of prosthetic dentistry. Jan 2024;131(1):34-41. doi:10.1016/j.prosdent.2021.11.026
- Ribeiro OA, M.I.Brito. Validação de protocolos de montagem de um articulador semi-ajustável arcon e respectivo arco facial. 2015.
- Lin YC, Scialabba R, Lee JD, Sun J, Lee SJ. Assessment of Occlusal Vertical Dimension Change in Mechanical and Virtual Articulation: A Pilot Study. Dent J (Basel). Nov 8 2022;10(11)doi:10.3390/dj10110212
- Andrighetto AR, de Fantini SM. Effects of neuromuscular deprogramming on the head position. Cranio. Jul 2015;33(3):183-8. doi:10.1179/2151090314y.0000000016
- Tamburini SAF, Escoboza CS, Montes de Oca Zavala A, Flores ALM, Santibañez García JA, Guízar Mendoza JM. Comparison of three options for neuromuscular deprogramming treatment. J Clin Orthod. Jan 2022;56(1):101-110.
- Okeson JP. Management of Temporomandibular Disorders and Occlusion. 8th ed. Mobsy; 2021.
- Valle RT Grossmann E. Disfunções Temporomandibulares: Novas Perspectivas. Editora Tota; 2019.
- Kattadiyil MT, Alzaid AA, Campbell SD. The Relationship Between Centric Occlusion and The Maximal Intercuspal Position and Their Use as Treatment Positions for Complete Mouth Rehabilitation: Best Evidence Consensus Statement. J Prosthodont. Apr 2021;30(S1):26-33. doi:10.1111/jopr.13316
- Greene CS, Obrez A. Treating temporomandibular disorders with permanent mandibular repositioning: is it medically necessary? Oral Surg Oral Med Oral Pathol Oral Radiol. May 2015;119(5):489-98. doi:10.1016/j.oooo.2015.01.020
- Revilla-León M, Zeitler JM, Kois JC. An overview of the different digital facebow methods for transferring the maxillary cast into the virtual articulator. J Esthet Restor Dent. Dec 2024;36(12):1675-1686. doi:10.1111/jerd.13264