






Optimal Surgical Scars: Aligning Incisions with Skin Folds
“`html
Surgical Skin Incisions Result in Optimal Scars When Made Parallel to Main Folding Lines
Gottfried Lemperle, MD, PhD
Retired plastic surgeon, Division of Plastic Surgery, University of California, San Diego, CA. 200 West Arbor Drive, San Diego, CA 92103-8890
Present home: Wolfsgangstr. 64, D-60322 Frankfurt/Main, Germany
Tel. +49-69-1302-4217
[email protected]
OPEN ACCESS
PUBLISHED 31 July 2025
CITATION Lemperle, G., et al., 2025. Surgical Skin Incisions Result in Optimal Scars When Made Parallel to Main Folding Lines. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6662
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6662
ISSN 2375-1924
ABSTRACT
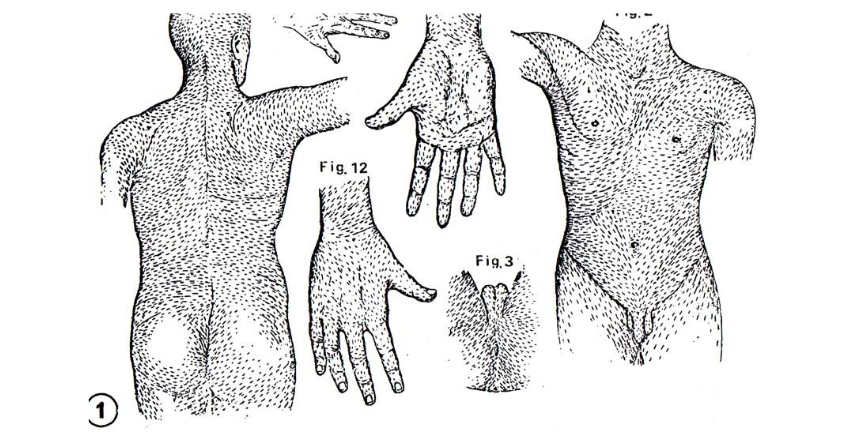
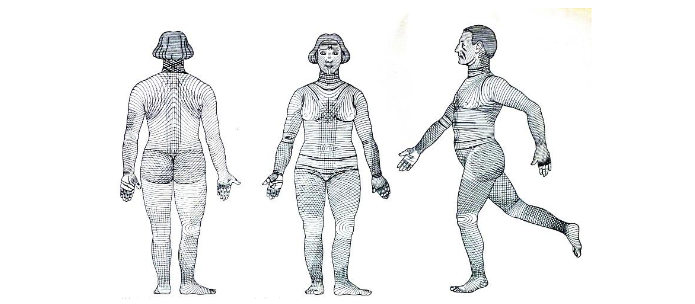
Women and young adults often judge the success of an operation based on the condition of the remaining scar. Optimal scars are the hallmark of plastic surgeons, while all other surgical specialties blame scar formation on the patient. If you look at the direction of the collagen fibers in histological images of the dermis, you will see that they adapt parallel to the later skin folds on head, torso and limbs and form wrinkles with age. However, since it is not possible to examine the skin of all areas histologically, we have made use of a little-known fact: the striae distensae of all humans, both women and men, run in the same directions, perpendicular to the main folding lines or tension lines of the skin. On the basis of visible stretchmarks (striae distensae) in the skin, which always appear in the same direction in men and women against skin tension, we demonstrated these Main Folding Lines on other parts of the body of children and young adults which are well-established on face and abdomen. In a former publication, the direction of striae distensae on photographs of 213 individuals were transferred to a human template. This striae-composite was compared with 276 images of incisions in our clinical data base of our scars, scar revisions, and scars from the Internet. They were put in opposition to well-known Langer´s lines along with descriptions of folding and lines but were running perpendicularly to the direction of the underlying muscles. Langer´s lines are still the recommendation and matrix for surgical incisions in most surgical text books, even if they were never meant as those by their first describer, an anatomist in 1861. In order to achieve minimal scarring, we should look at the direction of collagen fibers within the dermal matrix and surgeons should attempt to place incisions parallel to skin tension lines, i.e. in skin folds or skin creases. Main Folding Lines (MFL) should be used in elective incisions in children, adolescents, and young women as guide for the prevention of later visible hypertrophic or hypotrophic wide scars.
Keywords: Skin incisions, striae distensae, main folding lines, surgical incisions.
INTRODUCTION
Women and young adults often judge the success of an operation based on the condition of the remaining scar. Plastic surgeons are therefore frequently confronted with corrections of conspicuous scars. However, they know as little about the direction of the main folding lines as other surgical specialists do about the optimal direction for their incisions. This article therefore aims to show the direction in which the first skin incision can be made in order to leave scars that are as invisible as possible in young patients. Minimal invasive and endoscopic surgeries have revolutionized thoracic, abdominal, and orthopedic surgery, and have become today´s gold standard, resulting in much smaller scars. However, children and adolescents are still prone to develop hypertrophic scars, which could be prevented by surgical incisions in the direction of the main folding lines of the skin. The list of ineffective treatments for scars is long, including heparin-, panthenol-, and silicone creams, needling rollers, and laser therapy. The only effective treatments are early pressure dressings and corticosteroid injections in hypertrophic scars, or surgical excisions of broad indented hypotrophic scars. It often takes decades for better methods to find their way into standard textbooks. Surgical and orthopedic textbooks do not mention natural folding lines for optimal surgical incisions. The purpose of this publication is to facilitate the determination of optimal incision lines perpendicular to the direction of striae distensae. This correlation has been demonstrated in an earlier publication of 2014.
HISTORY OF SURGICAL INCISION LINES
During the past century, thirty-eight various guidelines have been developed regarding elective incisions. Most surgical textbooks include Langer’s of 1861,
or a slight modification, such as the incision proposed by Kocher in
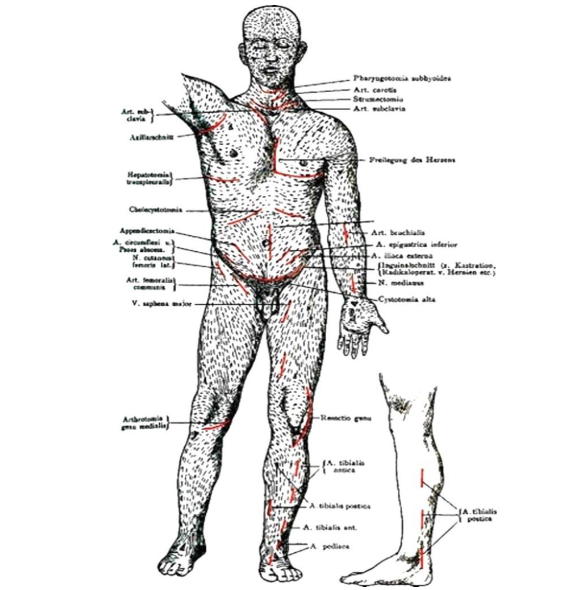
. They run perpendicular to muscle action of 1951 despite the fact that these incisions run oblique or even perpendicular to skin folds on forehead, cheeks, breasts, and abdomen. They run vertically across the ante-cubital region, the wrist, thigh, and distal regions of the extremities, although concordant on neck, shoulders, back and buttocks. The concept of using natural striae distensae for optimal incision lines is new and proves the natural folds which appear only later in age.

.
HISTOLOGY OF TENSION LINES
The presence of tension lines and normal wrinkle lines in the skin depends on the interrelation between elastic fibers and collagen fibers, as well as on the anchorage of collagen bundles one upon another.

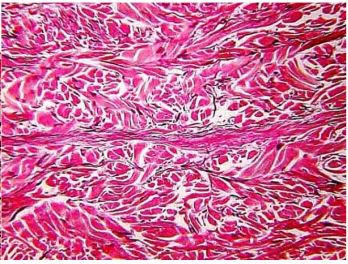
The fibroblasts in striae possess a contractile phenotype more akin to myofibroblasts and the elastic fiber network proximal to the epidermal-dermal junction appears to be more prone to destruction in active striae. The collagen lattice can be ruptured under the influence of steroids and especially estrogens. The newly synthesized collagen becomes reorganized by tension and is aligned in the direction of the presumed stress. The same happens in wound healing and therefore striae are considered dermal scars.
STRIAE DISTENSAE
In 1927, dermatologist Felix Pinkus was the first to question lines as a guide for skin incisions and he described the folding as the ideal direction for elective incisions. However, these drawings are too confusing to serve as instructions for the surgeon on where to make the incisions. He also described and illustrated the location of striae, but did not relate them to skin incisions. Unfortunately, the publication in a German dermatological textbook did not reach the surgical community.
Striae distensae are characterized by linear, smooth bands of atrophic skin that are reddish at first and ultimately turn pale. In young adolescents, they can appear during growth spurts on hips, inner thighs, and female breasts, as well as on shoulders, lower back, and outer thighs of boys without measurable changes in their hormone levels. Eighty percent of adolescents in Korea show striae: in girls more pronounced on buttocks, thighs and calves, and in boys on buttocks, knees and lower back. During pregnancy, striae distensae appear in the abdominal skin often during the first months of pregnancy and before tension is caused by the growing fetus and uterus. Obesity, oral contraceptives, and breast augmentation can also cause striae in a small percentage of women. The widest and deep red striae are seen in Cushing patients and in those under chronic systemic or local cortisone therapy.
MATERIALS AND METHODS
In a former publication, a total of 213 photos were examined of patients with striae as adolescents, during and after pregnancy, diagnosed with focal and after disease or steroid use and abuse. Sources included our own image files (78 pictures) as well as an extensive Internet Google search on ‘stretch marks’ and ‘striae’ (135 pictures). All relevant striae were copied onto blank human templates and 3 overall direction charts were created.
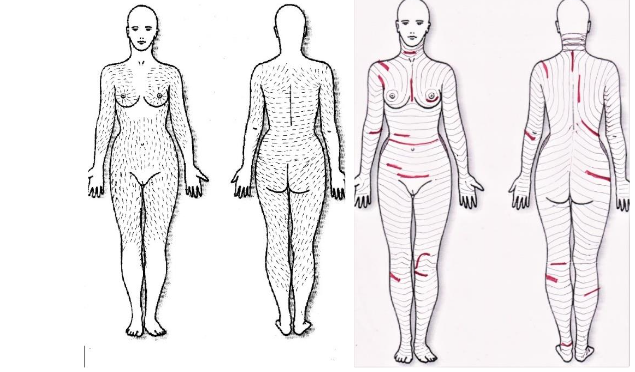
Regardless of their etiology, all striae demonstrated a similar clinical appearance and same direction in both male and female skin. Furthermore, the direction of the lamellae in patients with linear elastosis was the same as the main folding lines across the entire body. In addition, 276 images of unknown surgical incisions and scars were retrieved from the Internet, their direction and width were compared to the main folding lines and the following compound was designed. Together with an orthopedic colleague, we see the resulting red incision lines as an opportunity to open the skin in patients who want the scar to be as invisible as possible.
RESULTS: THE OPTIMAL DIRECTION OF SURGICAL INCISIONS
FACE AND NECK
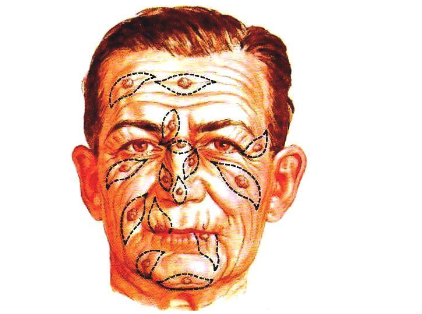
Disturbing scars from surgical mistakes must be kept at an absolute minimum in the face, where existing folds and wrinkles determine the logical direction of an incision or a fusiform skin excision.
Incision lines on the neck should run horizontally and preferably inside existing horizontal neck folds as high as possible. The collar for goiter surgery dates back to the late 19th century, when women were wearing high-necked dresses or heavy jewelry.

Vertical tracheotomy incisions against the folding lines of the neck are often followed by ugly contracted scars.
Incisions for tracheotomies, thyroidectomies, or for access to cervical discs should always be done higher up in the lower horizontal neck fold and clear of the jugulum in order to avoid hypertrophic scarring. The same problem of hypertrophic scarring can occur on the necks of young people, where incisions should always be made horizontally.
SHOULDER AND ARM
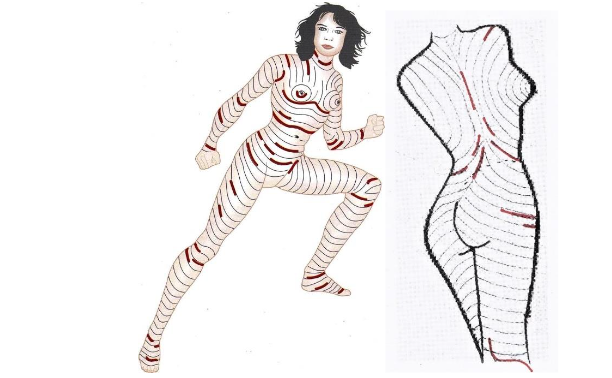
Striae observed in body builders and in patients with linear focal elastosis or Cushing syndrome all point in one direction: horizontal over pectoral and deltoid muscles. Viewed from the front, the main folding lines therefore appear vertical between neck and shoulders, but in reality, if viewed from the side, they are virtually horizontal. Wide and hypertrophic scars often develop over the shoulder, over the AC-joint and after open reposition of a clavicle fracture.

Therefore, in young patients anterior incisions across the joint and deltoid muscle should be avoided in favor of posterior vertical incisions between axilla and upper arm head. On the arms, striae develop straight vertically, but somewhat obliquely from the anterior axilla to the inner elbow.

The tension lines on the upper arm and forearm are not perpendicular to the muscle pull or circumferential, but somewhat oblique and proceed over the joints into the horizontal skin folds. Longitudinal and vertical incisions to expose a bone fracture on the upper arm must be avoided in favor of oblique and semi-circumferential incisions, which will heal inconspicuously.
DISCUSSION
In many areas of the body surface, the described folding run closely to the Langer lines, with which they are often confused. Langer lines were created by static forces in the skin of cadavers. The normal wrinkle lines are produced by dynamic forces acting on the skin of a living person. If we exclude Langer lines as historic and not primarily intended as recommendation for the direction of skin incisions, we are left with three well known publications on skin incisions and optimal scarring: Pinkus described main folding lines produced by skin in 1927. Kraissl recommended incisions perpendicular to the lines running perpendicular to lines, especially as they cross joints and facial folds. In normal folding lines, the predominant orientation of collagen fibers is parallel to the folds and wrinkles. Collagen bands in scars also form parallel to the wound edges, regardless of scar location. Striae distensae develop perpendicular to the direction of the strongest tension on the skin, and nature reveals that the tension lines or main folding lines are perpendicular to the striae. Tension cannot be seen through the skin and folds appear only later in age. Surgeons, who have difficulty to identify striae or later skin folds in young patients, may use the graphics in this publication as guidance. Here is an example on the neck of a young female patient with pterygium colli of two z-plasties, where incisions along the hypothetical tension lines healed normally, but those contrary to the tension lines (or better: main folding lines) healed differently with hypertrophy.

CONCLUSION
Non-observance of skin tension lines can cause widening or hypertrophy of scars. A linear incision develops a wider gape if it occurs parallel to striae rather than transversely to them. Skin tension seems a hard to imagine and therefore confusing expression, while Folding are easier to see, imagine and understand. The simplest rule for making optimal incisions in the most favorable direction is to follow natural wrinkle lines. If these cannot be seen, the skin or moving the joints on the extremities will show them. Incisions come together naturally and improper ones tend to.
CONFLICT OF INTEREST STATEMENT:
The author has no conflicts of interest to declare.
FUNDING STATEMENT:
None.
ACKNOWLEDGEMENTS:
None.
DISCLOSURE:
The corresponding author has nothing to declare.
AUTHORS CONTRIBUTION:
This manuscript was a clinical extension of a prior article of 2014 relating the direction of surgical incisions to the direction of striae distensae.
REFERENCES:
- Lemperle G, Tenenhaus M, Dieter Knapp D, Lemperle SM. The direction of optimal skin incisions derived from striae distensae. Plast Reconstr Surg. 2014;134:1424-1434.
- Kocher T. Textbook of Operative Surgery (3rd English ed.). London: Adam and Charles Black 1911:p.30.
- Borges AF, Alexander JE. Relaxed skin tension lines, z-plasties on scars, and fusiform excision of lesions. Brit J Plast Surg. 1962;15:242-253.
- Langer K. On the anatomy and physiology of the skin, I. The cleavability of the cutis [Translation from German in 1861]. Br J Plast Surg. 1978;31:3-8.
- Carmichael SW. The tangled web of Langer’s lines. Clin Anat. 2014;27:162-168.
- Wilhelmi BJ, Blackwell SJ, Phillips LG. Langer’s lines: to use or not to use. Plast Reconstr Surg. 1999;104:208-214.
- Kraissl CJ, Conway H. Excision of small tumours of the skin of the face with special reference to the wrinkle lines. Surgery. 1949;4:592-600.
- Kraissl CJ. The selection of appropriate lines for elective surgical incisions. Plast Reconstr Surg. 1951;8:1-28.
- Pinkus F. Die Faltung der Haut, in Pinkus F: Die normale Anatomie der Haut. Handbuch der Haut und Geschlechtskrankheiten Vol 1, Berlin: Springer 1927:4-76.
- Borges AF. Elective Incisions and Scar Revision. Boston: Little, Brown 1973:5-10.
- Borges AF. Relaxed skin tension lines (RSTL) versus other skin lines. Plast Reconstr Surg. 1984;73:144-150.
- Piérard GE, Lapière CM. Microanatomy of the dermis in relation to relaxed skin tension lines and Langer’s lines. Am J Dermatopathol. 1987;9:219-224.
- Viennet C, Bride J, Armbruster V, Aubin F, Gabiot AC, Gharbi T, Humbert P. Contractile forces generated by striae distensae fibroblasts embedded in collagen lattices. Arch Dermatol Res. 2005;297:10-17.
- Arem AJ, Kischer CW. Analysis of striae. Plast Reconstr Surg. 1980;65:22-29.
- Courtiss EH, Longacre JJ, deStefano GA, Brizio L, Holmstrand K. The Placement of elective skin incisions. Plast Reconstr Surg. 1963;31:31-44.
- Alshaiji JM, Handler MZ, Schwartzfarb E, Izakovic J, Schachner LA. Unilateral striae distensae affecting the right axilla in a 16-year-old boy: brief report. Pediatr Dermatol. 2014;31:617-618.
- Cho S, Park ES, Lee DH, Li K, Chung JH. Clinical features and risk factors for striae distensae in Korean adolescents. J Eur Acad Dermatol Venereol. 2006;20:1108-1113.
- Basile FP, Volpe A, Basile AR. Striae distensae after breast augmentation. Aesth Plast Surg. 2012;36:894-900.
- Rotsztejn H, Juchniewicz B, Nadolski M, Wendorff J, Kamer B. The unusually large striae distensae all over the body. Adv Med Sci. 2010;55:343-345.
- Jeong JS, Lee JY, Kim MK, and Yoon TY Linear focal elastosis following striae distensae: Further evidence of keloidal repair process in the pathogenesis of linear focal elastosis. Ann Dermatol. 2011;23(Suppl 2):S141-S143.
- Lemperle G, Holmes RH, Cohen SR, Lemperle SM: A classification of facial wrinkles. Plast Reconstr Surg. 2001;108:1735-1750.
- Lim SY, Kwack WG, Kim Y. Comparison of outcomes between vertical and transverse skin incisions in percutaneous tracheostomy for critically ill patients: a retrospective cohort study. Crit Care. 2018;22:Article # 246.
- Russell CJ, Bush JA, Russell GW, Thorlby A, McGrouther DA, Lees VC. Dynamic skin tension in the forearm: effects of pronation and supination. J Hand Surg Am. 2009;34:423-431.
- Bedard P, Keon WJ, Brais MP, Goldstein W. Submammary skin incision as a cosmetic approach to median sternotomy. Ann Thoracic Surg. 1986;41:339-341.
- Shrotria S. The peri-areolar incision – gateway to the breast! Eur J Surg Oncol. 2001;27:601-603.
- Halm JA, Lip H, Schmitz PI, Jekeel J. Incisional hernia after upper abdominal surgery: a randomised controlled trial of midline versus transverse incision. Hernia 2009;13:275-280.
- Bickenbach KA, Karanicolas PJ, Ammori JB, et al. Up and down or side to side? A systematic review and meta-analysis examining the impact of incision on outcomes after abdominal surgery. Am J Surg. 2013;206:400-409.
- Heller L, Chike-Obi C, Xue AS. Abdominal wall reconstruction with mesh and components separation. Semin Plast Surg. 2012;26:29-35.
- Leunig M, Hutmacher JE, Ricciardi BF, Impellizzeri FM, Rüdiger HA, Naal FD. Skin crease ‘bikini’ incision for the direct anterior approach in total hip arthroplasty: a two- to four-year comparative study in 964 patients. Bone Joint J. 2018;100-B(7):853-861.
- Andermahr J, Jubel A, Elsner A, Schulz-Algie PR, Schiffer G, Koebke J. Die Hautspaltlinien und die Schnittführung bei Fußoperationen. Orthopäde 2007;36:265-272.
“`