






Improving Maternal and Newborn Care: Zambia’s QoC Standards
Implementation of the WHO Quality-of-Care Standards for maternal and newborn care in selected Zambian Health Facilities – Lessons learnt from the Journey towards Centers of Excellence
Choolwe Jacobs¹*, Rosemary R Mwanza-Banda², Gertrude Sibuchi Kampekete³, Dennis Ngosa¹, Apurva Chaturvedi⁴, Fatima Gohar⁵, Sebeana Mayimbo², Sharon Kapoma², Mwiche Musukuma¹, Mildred Tolosi¹, Tedson Simwanza¹, Alinda Mae Lauer³, Caren Chizuni¹, Angel Mwiche², Josephine Nkhowani¹, Sarita Verma³
- University of Zambia, School of Public Health, Lusaka, Zambia
- Ministry of Health, Lusaka, Zambia
- UNICEF, Lusaka, Zambia
- UNICEF, Regional Office South Asia (ROSA) Region
- UNICEF, Eastern and Southern Africa Regional Office (ESARO)
OPEN ACCESS
PUBLISHED: 31 January 2026
CITATION: Jacobs, C., Mwanza-Banda, R.R., et al., 2026. Implementation of the WHO Quality-of-Care Standards for maternal and newborn care in selected Zambian Health Facilities – Lessons learnt from the Journey towards Centers of Excellence. Medical Research Archives, [online] 14(1).
https://doi.org/10.18103/mra.v14i1.XXXX
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v14i1.XXXX
ISSN 2375-1924
Abstract
Background: Maternal and newborn mortality remain a challenge in Zambia, particularly during the antepartum, intrapartum, and neonatal periods. To address these gaps and improve outcomes, the Ministry of Health (MoH) implemented standardized Maternal and Newborn Health (MNH) and Small and Sick Newborns (SSN) quality of care (QoC) standards to improve health outcomes and generate evidence to inform national scale-up. We set out to document the best practices and lessons learned from this collaborative initiative.
Methods: In 2024, the adapted MNH and SSN World Health Organization QoC standards were rolled out in the eight selected health facilities using a phased approach. Twenty-one related QoC indicators were integrated into the Health Management Information System (HMIS) via the District Health Information System Version 2 (DHIS2), supported by digital tools. Standard Operating Procedures and assessment tools were developed through stakeholder consultations. Capacity-building workshops and targeted mentorship supported implementation. Baseline, midline and end line assessments were conducted using health facility assessments and a qualitative case design to identify best practices and challenges.
Results: Key achievements included integrating MoH-approved indicators into HMIS, adopting digital checklists, strengthening mentorship, and improving quality-of-care standards. From baseline to endline, maternal and newborn care scores increased for Standard 2 (use of health information data) by 14% (Percentage change: 34.3%) and 13.5 percentage points (a 32.7% change), respectively. Similarly, under the small and sick newborn (SSN) guidelines, Standard 2 improved by 24.5% (percentage change: 49%), while Standard 3 improved by 21.1% (percentage change: 36.1%). Implementation was constrained by factors such as limited skilled personnel, deficiencies in respectful care, infrastructure gaps, and supply shortages. Nonetheless, several best practices were identified, including engagement of leadership and stakeholders, promotion of peer mentorship, and embedding QoC within existing health system structures.
Conclusions: The initiative demonstrates that integrating standardized QoC practices within existing health systems can significantly improve maternal and newborn outcomes. Sustaining and scaling these gains will require addressing resource gaps and strengthening data use for decision-making.
Keywords
Quality of care, maternal, newborn health, Centers of Excellence, Zambia.
Introduction
As countries strive to reduce the burden of maternal and newborn mortality, there is growing recognition that improving access to services alone is not enough. Although efforts to increase coverage, such as skilled birth attendance and facility-based deliveries, have expanded significantly, these interventions have proven insufficient in reducing mortality rates unless accompanied by quality care. Quality of care (QoC), defined as care that is safe, effective, timely, efficient, equitable, and people-centered, is a critical pillar of Universal Health Coverage (UHC) (World Health Organization). Unfortunately, quality of care remains low in many low- and middle-income countries (LMICs), especially sub-Saharan Africa, including Zambia.
In Zambia, great strides have been made to improve maternal and newborn health. However, notable burdens and gaps in maternal and newborn survival do exist across the country. Current trends indicate that Zambia is among 63 countries that are far from achieving the 2030 Sustainable Development Goals (SDG) target of reducing the neonatal mortality rate to ≤12 per 1000 live births and will need to double the annual rate of decline in neonatal mortality to do so. Improving the quality of care (QoC) during labor, delivery, and the immediate postnatal period is one of the most impactful strategies for reducing maternal and newborn mortality and improving overall health outcomes. Strengthening QoC could potentially avert 50% of maternal deaths and 58% of newborn deaths.
In pursuit of Sustainable Development Goal (SDG) 3, which aims to ensure healthy lives and well-being for all, Zambia has taken deliberate steps to improve maternal and newborn care. This includes the adaptation of WHO’s comprehensive QoC standards aimed at improving the quality of care of small and/or sick newborns in health facilities and provides the framework, input, process, and outcome measures for such care. In 2022, Zambia adopted the WHO QoC standards for Maternal Newborn Health, Small, and Sick Newborn Care and the 2022 WHO Essential Newborn Care training materials. Additionally, strategies to scale up Essential Newborn Care were included in the Zambia National Health Strategic Plan 2022 – 2026, and targets to reduce neonatal mortalities to 12 per 1000 live births or less by 2026 were set.
To facilitate implementation of the QoC, the Ministry of Health, Zambia, launched the Journey to Centers of Excellence (CoE) initiative in collaboration with partners such as UNICEF and Swedish International Development Agency (SIDA). The initiative was implemented across eight hospitals in Lusaka, Eastern, Southern, Luapula, and Muchinga provinces over a period of seven months, aimed at embedding quality care into routine maternal and newborn services and institutionalizing best practices.
However, despite this implementation, the initiative’s performance and the lessons from it are not well known. It is against this backdrop that the Zambian Ministry of Health requested a detailed assessment of the quality of care (QoC) in Zambia towards the scale-up of QoC standards. The objective of this study was to document the best practices and lessons learned from the implementation of the Centers of Excellence approach in Zambia, offering insights for policymakers, program implementers, and stakeholders involved in maternal and newborn health improvement efforts.
Methods
STUDY DESIGN AND SETTING
We utilized a mixed-methods approach, including health facility assessments and a qualitative case study design, to assess the implementation of the QoC initiative in seven selected journeys to the centres of excellence health facilities where WHO QoC standards were implemented from January to July 2024. Facility assessments were conducted at three time points: at baseline between 26/12/2023 and 29/12/2023; midline between 04/03/2024 and 08/03/2024; and endline between 29/07/2024 and 01/08/2024. The data for the qualitative case design were collected between 29/07/2024 and 01/08/2024. The facilities included Mansa, Choma, St Francis, and Chinsali general hospitals; Chipata Central Hospital; and the University Teaching Hospital (UTH) Children’s, Women’s, and Newborn hospitals. Selection of the facilities was guided by high-burden regions with poor maternal and neonatal health outcomes, as well as by consideration of SIDA priority provinces. The seven facilities provide basic and emergency care for both adults and children, as well as maternity care services. The seven facilities were referred to as the Journey to Centers of Excellence, serving as benchmarks for scaling up the implementation of QoC standards. Centres of excellence are essentially places where excellence on a particular medical front is delivered in a unique, focused manner to patients. It is used to coordinate care, reduce inefficiencies, and to improve the quality of health care services delivered. The goal of the journey to CoE facilities is to demonstrate the impact of implementing the standards and tracking the EPMM & ENAP (Every Woman, Every Newborn, Everywhere, #HealthyFutures) indicators.
THE JOURNEY TO THE CENTERS OF EXCELLENCE IMPLEMENTATION PROGRAM
We used a phased approach to implement the QoC standards. The Logical Model was utilized to describe the implementation of the intervention (QoC initiative). The Logical model is a theory of Change that provides an explicit, visual statement of the activities that would bring about change and the results we expect to see in this programme.
The phased implementation strategy involved holding consultative meetings with UNICEF, MoH, UNZA, and program managers as follows; Adaptation of MoH-approved ENAP indicators: Through a participatory, consultative process with UNICEF, MoH, and program managers, we developed and adapted 21 indicators to track progress across all 7 CoEs. This helped identify and prioritize areas for improvement.
Development of MoH-approved checklists and Standard Operating Procedures (SOPs): To guide and monitor the implementation of QoC standards for Essential Newborn Care (ENC) and the Small and Sick newborn (SSN), we adapted the WHO 2022 simplified checklists. In addition, SOPs were developed to guide the use of the checklists. Both checklists and SOPs incorporated gender mainstreaming, disability, and Water, Sanitation and Hygiene (WASH) considerations within clinical practice and care. Consultative/validation meetings were held with national, provincial, district, facility focal point persons, as well as maternal and neonatal health care providers and specialists, including pediatricians and gynecologists, to agree on the checklist and related SOPs. Additional consultative/validation meetings were held with MoH program officers, including M&E, public health, and focal point personnel, to agree on EPMM and ENAP indicators for monitoring.
Translation of adapted indicators and developed checklists: Adapted indicators and checklists were translated into facility-level digital scorecards and performance dashboards to monitor progress, identify, and prioritize areas for improvement. Specialists from the MoH’s Monitoring and Evaluation (M&E) and Information Technology (ICT) departments, as well as those from UNICEF, were engaged to design, build, test, and deploy the digital scorecard. The digital scorecards and associated dashboards were built on the open-source District Health Information System 2 (DHIS2) platform. Consultative and validation meetings were held with program managers, mentors, and ICT and M&E officers to translate the adapted checklist into a meaningful scorecard and associated dashboards that could be accessed on tablets or laptops. System design requirements also considered future integration with existing MNCH scorecards used at the national level. System SOPs for the digital scorecard and associated dashboards were also developed.
Capacity-building for health care providers on implementing QoC standards: Orientations and capacity-building sessions for program officers and health care providers in the CoEs were successfully held. These sessions were held with program officers, M&E focal points, and health information officers from all 7 CoEs. All capacity-building activities were completed before the rollout of QoC standards across all CoE sites.
Strengthening Quality Improvement (QI) teams at the provincial, district, and health facility levels and in maternal and newborn units: On-site service quality assessments (SQAs) and mentorship support were conducted using an adapted checklist to identify good practices and gaps across the 7 CoEs. Facility focal point persons and QI teams were the target to ensure success and sustainability. In total, two quality assessments and an intermediate mentorship visit were conducted in each facility during the project timeline. The Journey to CoEs coordinating team consisted of: Ministry of Health program officers (MNCH specialists, M&E officers specialised in HMIS, QI officers, and IT officers specialized in DHIS2); University of Zambia researchers; and UNICEF MNH specialists. These worked in close collaboration with facility focal point persons (MNH healthcare workers and facility M&E officers) from the 7 CoEs.
ASSESSMENTS
Quantitative approach
Health facility assessments were achieved by conducting facility visits to all CoEs and performing structured observations of available services in service specific areas of the facility using a QoC checklist. During the assessments, we also conducted interviews with the unit in-charges, i.e., maternal and newborn units.
Data collection and tools
The standards for improving the quality of care for maternal and newborn including small and sick newborns provides comprehensive guidance to health care providers in improving the quality of care for mothers and newborns. Assessment of implementation of standards by Health care workers was done through observations, review of records and checklist. A Standard Operation Procedure (SoP) was also used to guide reviewers in assessing provision of quality care for the mother and newborn including the small and sick newborns in health facilities. The SoP provided systematic guidance on how to conduct both self-assessment and onsite-supervision assessment at the health facilities to ensure that mothers and the newborn receive quality health care services using checklists.
Assessment Checklists
Two sets of checklists were developed according to the maternal and newborn, and small and sick newborn quality of care standards. The two (2) sets of checklists quality statements and components for assessing adherence to QoC standards, each covering inputs, processes and outputs for each quality statement. Each checklist was made up of domains according to standards and associated with quality statements. Under each statement were questions, each mapped to a specific standard or a set of them, with responses coded on a categorical scale of 0, 1 or 2. Where 0 represented absence of adherence, 1 full adherence and 2 for not applicable. All quantitative data using checklists was collected with electronic tablets, laptops, and using tracker platform in DHIS2.
Observations
Observations were conducted within the service delivery area. This approach complemented the checklists and interviews with staff.
Records/desk review
Data collectors obtained information on the quality of care for admitted and recently discharged patients by checking records. Other records such as meeting minutes and guidelines were reviewed. Trained national level and peer mentors collected data at three time points using digital gadgets (Tablets and laptops) unto the DHIS2.
Data Management and analysis
Data quality assessment were done by M&E officers at national and facility levels. In addition, weekly data quality meetings were done to resolve any inconsistences. Quantitative data that was captured using a checklist for maternal and newborn as well as small and sick newborn was extracted from the DHIS2. The percentage score for each standard was calculated at baseline, midline and endline evaluation time points. The maternal and newborn section and small and sick newborn had a total of 8 standards each. Each of the 16 standards had a number of quality statements and each quality statement had several components/items that were scored. Each component/item was scored as Yes=1 or No=0.
Quality statement percent scores for each quality statement were calculated by taking the total number of components/items achieved, divided by total component in that particular quality statement, multiplied by 100. Percent scores for each standard were then calculated by adding quality statement percent scores and dividing by the total number of quality statements under that particular standard, multiplied by 100.
Quality statement score = Total components achieved x 100 / Total components in the quality statement
Quality standard score = Total of all the quality statement percentage scores in the standard / Number of quality statements in the standard
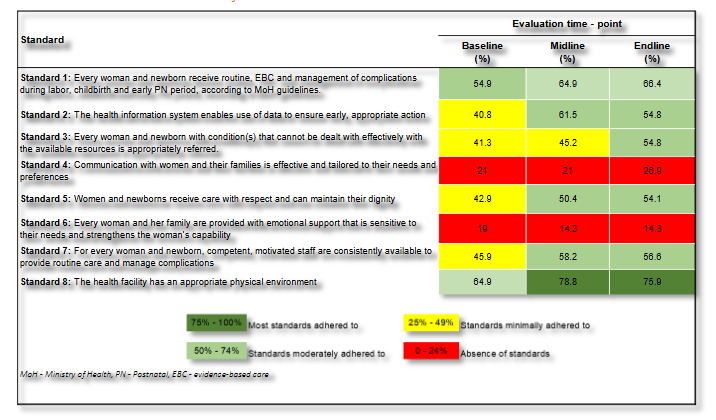
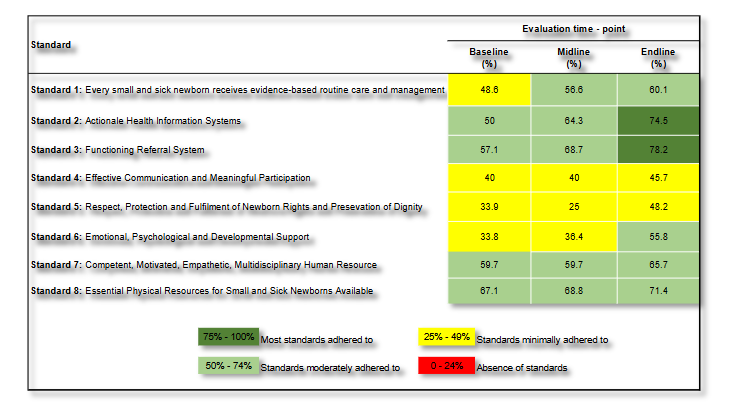
A percent score of 0 – 24% meant absence of standards, 25% – 49% meant Standards minimally adhered to, 50% – 74% meant Standards partially adhered to and 75% – 100% meant most standards adhered to. Performance for each QOC section (MNH or SSN) was presented in a scorecard across the evaluation time point. All data were analyzed using Stata 18 SE (StataCorp, College Station, TX, USA).
QUALITATIVE APPROACH
Qualitative case study design was used for Key Informant Interviews (KIIs) with unit in-charges. Any facility in-charge with less than one-year experience working in a specified facility were excluded. An interview guide was developed to help with KIIs. The guide had questions around challenges and lessons learnt in implementing the QoC standards. Digital recorders were used for interviews and data was transcribed verbatim for analysis. Trained research assistants conducted the interviews. We used thematic analysis to identify emerging themes guided by the Health Systems.
Ethical considerations
Permission to conduct implementation of WHO Quality-of-Care Standards in selected Zambian Health Facilities was sought from the Ministry of Health, Provincial health offices in all the provinces where the Health facilities came from, including Health facility management. Ethical approval was obtained from UNZABREC (Ref-No. 001-10-25), and final Authority to conduct research was obtained from the National Health Research Authority. Administrative approval was obtained from the Ministry of Health.
Results
DESCRIPTION OF KEY ACHIEVEMENTS
Through the journey to CoE QoC implementation program, the following were achieved; adaptation of MoH-approved ENAP indicators, development of MoH approved checklists and SoPs, translation of adapted-indicators and developed-checklists into facility-level digital scorecards and performance dashboards, and lastly, built capacity among health care providers to implement QoC standards. We developed and adapted a total of 21 indicators that were used to track progress in all the 7 CoEs. In addition, MoH approved checklists and SoPs were developed. The indicators as well as the checklists were translated into facility-level digital scorecards and performance dashboards, which were used for monitoring progress (identifying and prioritizing areas of improvement). These were built on an open-source platform on the Zambia HMIS – DHIS2. We also adapted the WHO quality of care standards.
PERFORMANCE OUTCOME OF QOC STANDARDS OF CARE
Maternal and newborn standards of care
Performance of maternal and newborn QOC standards generally improved over time between baseline and endline evaluations (February to July). Consistent improvements were seen in standard 2 (The Health Information System enables use of data to ensure early, appropriate action), standard 3 (Every woman and newborn with condition(s) that cannot be dealt with effectively with the available resources is appropriately referred) and standard 5 (Women and newborns receive care with respect and can maintain their dignity). From baseline to endline, the percentage score increased by 14 percent-points (percentage change 34.3%) 13.5 percent-points (percentage change 32.7%), and 11.2 percent-points (percentage change 26.1%) for standard 2, 3, and 5, respectively. Standard 6 (Every woman and her family are provided with emotional support that is sensitive to their needs and strengthens the woman’s capability), came out as the worst performing standard.
Small and Sick Newborn standards of care
Similarly, performance of the small and sick newborn standards of care also improved overtime. Consistent improvements were seen in standard 2 (The health information system enables collection, analysis and use of data to ensure early appropriate action to improve the care of every small and sick newborn) and 3 (Every small and sick newborn with a condition or conditions that cannot be managed effectively with available resources receives appropriate, timely referral through integrated newborn service pathways with continuity of care, including during transport). From baseline to endline, Standard 2 (50%, 74.5%), and Standard 3 (57.1%, 78.2) increased by 24.5% (percentage change 49%) and 21.1% (percentage change 36.1%) respectively. The lowest improvement was observed in standard 8 (The health facility has an appropriate physical environment, with adequate water, sanitation, waste management, energy supply, medicines, medical supplies and equipment for routine care and management of complications in small and sick newborns) (4.3 percentage point increase) and standard 4 (Communication with small and sick newborns and their families is effective, with meaningful participation, and responds to their needs and preferences, and parental involvement is encouraged and supported throughout the care pathway) (5.7 percentage point increase).
LESSONS LEARNT FROM QUALITATIVE FINDINGS DURING THE IMPLEMENTATION OF WHO QUALITY-OF-CARE STANDARDS
We used the health systems building blocks as predetermined themes for lessons learnt from qualitative findings during the implementation of WHO quality-of-care standards in the 7 CoEs. The sub-themes that emerged were subdivided into gaps identified and best practices documented during the implementation process.
| Theme (Health systems building blocks) | Sub-themes (Gaps identified) | Verbatim |
|---|---|---|
| Service delivery | Inconsistent delivery of essential newborn interventions | “We didn’t know that some prophylactic drugs like vitamin K were supposed to be administered routinely.” (Midwife KII1) |
| Deficiencies in respectful and responsive maternity newborn care | “It’s because of how the maternity ward is built; as you can see, there’s no provision to put an inquiry desk. Otherwise, the security guards respond to most queries, and charts help at times… For newborn privacy, I think it’s just an oversight.” (Midwife KII3) | |
| Inadequate Newborn Care and Infection Control Systems | “Challenges we have, amongst others, are that most patients admitted here are referred very late with infections already set. The NICU is also small … different cases sharing baby cots, we also need refresher training in infection prevention” (Midwife KII7) | |
| Health workforce/Human resource | General shortage of health personnel | “At most, we have over 90 neonates in our unit which has 3 ICUs for the critically ill and 2 other high care bays for stable sick neonates all managed by 5-6 nurses, it sometimes becomes very difficult to observe the babies effectively.” (Midwife KII4) |
| Inadequate orientation of multidisciplinary teams in QoC health facilities | “Time was limited for providers to understand the importance of implementing QoC in the facility.” (Midwife KII9) | |
| Information and Data | Lack of Standardized Indicator Frameworks | “We don’t have standardised registers to capture data….”(Midwife, Non KII8) |
| Compliance with Health Information and Review Protocols | ||
| Finance (Grants and funds etc.) | Inadequate Health Sector Financing as a Barrier to Quality and Equitable Care | “We have a high number of premature births requiring respiratory support but our CPAP machine has been out of use for over 3 months because we are waiting for biomedical engineers from MOH headquarters” (Nurse, KII3) |
| Insufficient Training Funds Undermining Data Quality and Specialized Care Capacity | “We have staff who are willing to learn, but without funding for specialized training, we depend on minimal partner led sessions, which are not enough to meet the needs in maternal and newborn care” (Midwife, KII2). | |
| Infrastructure, medical products and equipment | Shortage of medical and non-medical supplies | “Vit-k is there…our pharmacies, but there are times when we run out…” (Unit-Charge, KII5) |
| Inadequate Health Infrastructure as a Barrier to Quality and Equitable Care | “Our theatre is on the ground floor but when there is no power to use the elevator, we put mothers on the wheelchair and support them down the staircase if surgery is required.”(Midwife, KII4) | |
| Infrastructural limitations Weakening Referral Systems for Maternal and Newborn Health | “Our ambulance is okay, it’s just packed for now because of a broken spare part yet to be purchased but we do ask from other health facilities if theirs are not busy…”(Midwife, KII7) | |
| Inadequate spaces | “We sometimes allow the mothers to stay with their babies in our neonatal unit but not at all times as we also need space to work, our unit is not as big…” (Midwife, KII7) | |
| Leadership and governance | Lack of routine onsite mentorships by senior providers | ”we are aware about the routine peer mentorships, however we are carried away with routine duties, maybe we need to be reminded by our bosses to activate us..” (Nurse, KII4) |
GAPS TO IMPLEMENTATION OF QUALITY OF CARE
Service delivery
Inconsistent delivery of essential newborn interventions
The accounts from midwives in some hospitals revealed both systemic and informational gaps in newborn care practices. One midwife described how the demands of a busy ward sometimes lead to missed opportunities for administering prophylactic interventions before discharge. Stock-outs of essential commodities like Vitamin K and Tetracycline Eye Ointment (TEO) were reported to be common.
“Sometimes we get overwhelmed with work and forget to give the vaccines before discharges and also we have stock-outs of Vitamin-K and TEOs, and for the vaccines mostly get at their nearby facilities…” (Unit-Incharge KII 2)
In another Hospital, another midwife’s reflection highlighted a different but equally important issue: a lack of awareness that certain prophylactic drugs—such as Vitamin K are recommended for routine administration to all newborns. This indicates that beyond resource constraints, gaps in training and standard protocol awareness can hinder the consistent delivery of life-saving interventions.
“We didn’t know that some prophylactic drugs like vitamin K were supposed to be administered routinely.” (Midwife KII1)
Together, these experiences point to a combination of logistical, staffing, and knowledge-based barriers that prevent full implementation of newborn prophylaxis at the point of birth.
Deficiencies in respectful and responsive maternity and newborn care
Significant gaps were noted in the provision of respectful and responsive maternity and newborn care. These included limited privacy for newborns, poor communication with mothers and among healthcare professionals, and the absence of effective feedback mechanisms—such as service charters and dedicated information desks which reduced accountability and limited opportunities for client engagement. One midwife explained that some of these shortcomings stem from structural and procedural constraints:
“It’s because of how the maternity ward is built; as you can see, there’s no provision to put an inquiry desk. Otherwise, the security guards respond to most queries, and charts help at times… For newborn privacy, I think it’s just an oversight.” (Midwife KII3)
Inadequate Newborn Care and Infection Control Systems
Inadequate newborn care and weak infection control systems remained a critical challenge in health facilities. The absence of standardized neonatal protocols, insufficient thermal protection, overcrowded nurseries, and limited training of healthcare workers contribute to an environment where newborns were highly vulnerable to preventable complications and infections. Poor adherence to infection prevention guidelines further worsens the situation, significantly increasing neonatal morbidity and mortality. When the health care provider was asked about the infection prevention practices and control, one of the midwives had this to say:
“Challenges we have, amongst others, are that most patients admitted here are referred very late with infections already set. The NICU is also small … different cases sharing baby cots, we also need refresher training in infection prevention” (Midwife KII7)
Health workforce/Human resource
A pervasive shortage of health personnel emerged as a significant gap in delivering quality maternal, newborn, and child health (MNH) care. Units often lacked specialized staff trained in key areas such as communication with clients with disabilities needed to fully implement MNH and Safe Surgery Network (SSN) quality of care standards. Staffing shortages directly impacted patient care, contributing to medical errors, higher mortality rates, and increased infection risks. One pediatric nurse at Chipata Central described the strain on personnel:
“Sometimes two nurses are on duty against 20 neonates, which compromises care…” (Midwife KII8)
Similarly, a nurse from another hospital highlighted the overwhelming workload:
“At most, we have over 90 neonates in our unit which has 3 ICUs for the critically ill and 2 other high care bays for stable sick neonates all managed by 5-6 nurses, it sometimes becomes very difficult to observe the babies effectively.” (Midwife KII4)
Inadequate orientation of multidisciplinary teams in quality of care facilities
QoC team members come from diverse professional backgrounds and experience levels, requiring adequate orientation and mentorship in quality improvement (QI), MPDSR, monitoring and evaluation, and maternal and newborn care. However, limited orientation time at implementation sites hindered providers’ understanding and engagement. One pediatric nurse from Chipata Central noted:
“Time was limited for providers to understand the importance of implementing QoC in the facility.” (Midwife KII9)
Health financing
Inadequate Health Sector Financing as a Barrier to Quality and Equitable Care
It was observed that despite MoH being supported by partners in the MNH space like UNICEF in the implementation of the QoC standards for the journey to CoE’s in the four (04) provinces of Zambia, there were limitations in appropriate medical and non-medical equipment, medical and surgical supplies, essential medicines for MNH routine and curative care, WASH resources among others. This limitation was also noted on infrastructure such as private delivery rooms, space for mother and sick newborns together, delivery rooms in close proximity with obstetric theatres and neonatal units, accessibility by the differently abled and availability of mothers’ shelters.
In addition, there was also a lack of deliberate resources for maintaining some of the available equipment and infrastructure.
“We have a high number of premature births requiring respiratory support but our CPAP machine has been out of use for over 3 months because we are waiting for biomedical engineers from MoH headquarters” (Nurse, KII3)
“Our theatre is on the ground floor but when there is no power to use the elevator we put mothers on the wheelchair and support them down the staircase if surgery is required” (Midwife, KII6)
Insufficient Training Funds
These gaps are compounded by the absence of deliberate funding, at both central and facility level for specialized provider training in obstetrics, pediatrics, neonatology, emergency care, Emergency Obstetric and Newborn Care (EmONC), and essential and advanced newborn care, as required by quality-of-care standards. A midwife explained how the lack of resources limits professional development:
“We have staff who are willing to learn, but without funding for specialized training, we depend on minimal partner led sessions, which are not enough to meet the needs in maternal and newborn care” (Midwife, KII2).
Infrastructure/Medical products and equipment
Limited access to essential medical and non-medical equipment was observed at facilities, which negatively affected the implementation of QoC standards. The unavailability of appropriate doses of vitamin K interfered with timely prophylaxis for newborns, and inadequate resuscitative equipment further compromised emergency response readiness. Lack of stock control cards hindered prompt replenishment of medicine and surgical supplies. Non-medical equipment, such as linen and curtains, was in short supply, limiting privacy in the provision of Respectful Maternity Care.
“Vit-k is there…our pharmacies, but there are times when we run out…” (Unit-Incharge, KII5)
Inadequate Health Infrastructure as a Barrier to Quality and Equitable Care
Despite MoH and partner support, gaps in infrastructure continue to limit the delivery of quality maternal and newborn health services. Facilities face shortages of suitable delivery rooms, space for mothers and sick newborns, and proximity between delivery rooms, obstetric theatres, and neonatal units. Accessibility for people with disabilities and the availability of mothers’ shelters remain inadequate. Maintenance of existing infrastructure and equipment is also underfunded, leading to prolonged service disruptions.
A neonatal nurse from Choma General Hospital noted:
“We have a high number of premature births requiring respiratory support but our CPAP machine has been out of use for over 3 months because we are waiting for biomedical engineers from MOH headquarters.”(Nurse, KII5)
Similarly, a midwife from one Central Hospital explained:
“Our theatre is on the ground floor but when there is no power to use the elevator, we put mothers on the wheelchair and support them down the staircase if surgery is required.”(Midwife, KII4)
Infrastructural limitations Weakening Referral Systems for Maternal and Newborn Health
A critical challenge observed across Centers of Excellence (CoEs) was the weakening of referral systems for maternal and newborn health. Many facilities lacked dedicated funds for the procurement and maintenance of resident ambulances, resulting in limited availability of functional transport for emergency cases. These gaps contributed to delays in emergency referrals, placing undue pressure on lower-level health facilities that are often ill equipped to manage complex maternal and newborn health (MNH) cases.
A midwife from a General Hospital explained the situation:
“Our ambulance is okay, it’s just packed for now because of a broken spare part yet to be purchased but we do ask from other health facilities if theirs are not busy…”(Midwife, KII7)
This demonstration illustrates how resource constraints and equipment downtime disrupt timely referrals, highlighting the need for better funding and coordination to strengthen the MNH referral network.
Inadequate spaces
Facilities lacked adequate space to effectively implement family-centred care birthing choices such as having a companion in the delivery room and keeping the mother and sick newborn together. The absence of standard mothers’ shelters or waiting areas hindered caregiver support. Erratic water supply, especially during the night, undermined WASH efforts.
“We sometimes allow the mothers to stay with their babies in our neonatal unit but not at all times as we also need space to work, our unit is not as big…” (Midwife, KII7)
Leadership
Lack of routine onsite mentorships
Another gap that was observed was lack of onsite mentorship and limited opportunities for skills transfer performance improvement, and reinforcement of quality care standards. There was weak leadership engagement in day-to-day clinical practice and professional development. Another health care provider interviewed said;
”We are aware of the routine peer mentorships, however we are carried away with routine duties, maybe we need to be reminded by our bosses to activate us…” (Midwife, KII4)
Data and Information
Lack of Standardized Indicator Frameworks
A key challenge observed across Centers of Excellence (CoEs) was the absence of standardized indicator frameworks for the range of services offered in different Quality of Care (QoC) facilities. This inconsistency created significant barriers to data harmonization and performance monitoring, making it difficult to generate comparable information across sites. As a result, the effective use of scorecards and dashboards for tracking progress and guiding quality improvement was undermined. The gap underscored the need for a unified, context-appropriate set of indicators that can be consistently applied across service delivery points to strengthen data use, comparability, and accountability within the health system.
“We don’t have standardised registers to capture data….” (Midwife, KII8)
Non-compliance with Health Information and Review Protocols
An important gap identified was the non-compliance with established health information and review protocols, particularly in the area of maternal and newborn health. Despite the existence of national guidelines and policies mandating the review of newborn deaths, implementation remains weak at facility level. This lack of adherence to protocols undermines the health system’s ability to generate critical learning from preventable deaths and limits opportunities for data-informed decision-making. Without structured death reviews, facilities miss vital insights that could drive quality improvement and reduce avoidable mortality.
Best Practices
Early engagement of leadership and key stakeholders
Timely engagement and inclusion of health facility leadership, such as Medical Superintendents, focal point persons, Quality Improvement (QI) teams, Monitoring and Evaluation (M&E) officers, in-charges, and section heads, proved critical in driving efforts to improve the quality of care (QoC) in health services. Their active involvement fostered a sense of ownership and accountability at the facility level. Teams demonstrated openness to learning, proactively engaging with mentors and national facilitators to understand expectations and identify how they could meaningfully contribute to the initiative. This early collaboration created a strong foundation for sustained QoC improvements as mentioned by one of the participants;
“We value these initiatives and your call on us as facility leadership to be part of this program from the start, this way we shall be able to learn together and design high impact MNH interventions as a team for continuity” (Head clinical care Children hospital-UTH, KII3)
Peer Mentorship strengthened capacity in implementing QOC
We noted that mentorships, particularly peer mentorship, fostered shared learning and strengthened healthcare providers’ ability to implement QoC standards effectively. Furthermore, the mentorships contributed to the monitoring and evaluation of the implementation of Quality of Care (QoC) standards by facilitating discussions on progress related to maternal and newborn health indicators. Participants had this to say:
“These visits, along with peer-to-peer mentorship, have fostered shared learning, dissemination of best practices, and increased motivation among us staff in NICU and maternity wards” (Midwife, KII6)
Embedding QoC within existing structures
One notable best practice in the implementation of Quality of Care (QoC) standards was the strategic use of existing structures and resources. Facilities optimized available human resources, such as designated focal point persons, as well as existing supplies, equipment, and infrastructure—including essential medicines, functional private spaces, and basic privacy safeguards. Such practices contributed to improve QoC, particularly in promoting respectful and family-centred maternity care. For example, appropriate use of available curtains and clean linen ensured patient privacy and dignity during deliveries and examinations. A midwife from one of the settings described this approach:
“There was always clean linen to cover clients and ensure the curtains were drawn before delivery began or whenever doing examinations on mothers and newborns thereby supporting respectful and family centered maternity care.” (Midwife, KII4)
This example illustrates how making the most of existing resources, even in resource-constrained settings, can strengthen patient experience and uphold care standards.
Collaborative, data-driven alignment fostered ownership
To improve maternal and newborn health outcomes, facilities adopted a strategic focus on strengthening accountability mechanisms through the alignment of key indicators using a participatory, data-driven approach. This consultative process engaged stakeholders at multiple levels, fostering ownership of the data, enhancing accountability, and establishing a foundation for integrated health system performance tracking. A NICU nurse from one Hospital reflected on the change:
“Now that we have computers, tablets and proper registers, we have no excuse to give as to why we don’t have certain data.” (Nurse, KII5)
Provision of Electronic Data-Capturing Gadgets
The introduction of electronic gadgets such as laptops and tablets was identified as a best practice in improving data management within maternal and newborn health services. These devices reduced the time spent on data capturing, enhanced accuracy, and promoted timely reporting into the District Health Information System 2 (DHIS-2). A NICU nurse from one Central Hospital emphasized the change:
“Now that we have computers, tablets and proper registers, we have no excuse to give as to why we don’t have certain data.” (Unit In-charge, KII 9)
Discussion
We set out to document the best practices and lessons learned from the implementation of the CoEs approach in Zambia, offering insights for policy makers, program implementers, and stakeholders involved in MNH improvement efforts. We developed and implemented MoH approved indicators and checklist. Baseline to end line evaluations revealed improvements in the performance of QoC standards. Consistent improvements were seen in functional referral systems (Standard 3), communication (standard 4) and respect and dignity (standard 5) across maternal and newborn and small and sick newborn. Qualitative data reviewed inconsistent delivery of essential newborn interventions, deficiencies in respectful and responsive MNH as some sub-themes under service delivery theme. While under the Health work force, inadequate orientation of multidisciplinary teams in QoC health facilities and weak accountability in coordinating indicators and tracking digital performance for MNH emerged as sub-themes. The information theme had lack of standardized indicator frameworks across facilities, and limited training on effective communication as the sub-themes. While infrastructure, medical products and equipment theme had Shortage of medical and non-medical supplies Infrastructure limitations as sub-themes. Best practices included early engagement of leadership/stakeholders, peer mentorship strengthened capacity in implementing QOC, embedding QoC within existing structures, and collaborative data-driven alignment to foster ownership.
The development and implementation of MoH approved indicators and checklist was effective in ensuring uniformity and adherence to standard QoC guidelines and protocols for maternal and sick newborn across the CoEs facilities which is similar to another study. This was important for tracking implementation health outcomes and to guide policy formulation. Additionally, the digitization and visualization of the adapted checklist tool not only streamlined data collection but also empowered health facility staff to monitor their own progress along the journey to CoE enabling the use of their own data to identify priority areas for improvement, and visualize successes fostering a culture of accountability.
Consistent improvements were seen in functional referral systems, respect, dignity, and communication across maternal, newborn, small, and sick newborn even though communication percent score still remained unacceptably low. This was not a surprising finding as our qualitative results also revealed deficiencies in respectful and responsive care as one of the gaps. Communication just like dignity and respect is one of the elements under respectful maternity care. A previous study that looked at person-centered maternity care in Lusaka also reported communication and autonomy as the least performing domain. Improvements in communication, respect and dignity standards remain crucial, as various literature have highlighted the disrespectful treatment that women receive in health various across different regions. However, these cannot be achieved through implementation of QoC standards related to staff attitudes. Implementation of QOC standards requires a supportive environment for both healthcare providers and patients. This includes having enough medical and non-medical supplies, as well as proper infrastructure essential for providing safe, dignified, and family-centered care. In our assessment, infrastructure limitations shortage of medical and non-medical staff also came out as gaps that need to address for full actualization of high QoC levels.
Facilities lacked standardization of some indicators for capturing and synthesizing complex, QoC improvements for MNH as well as SSN health care. This adversely affected harmonization for data quality and monitoring performance measurement which is a critical component in facilitating QIS. This highlighted the need for a unified, context-appropriate set of indicators that could be applied consistently across various service delivery points to strengthen data use and improve the reliability of the data. The development and implementation of MoH approved indicators and checklist was effective in ensuring uniformity and adherence to standard guidelines and protocols for maternal and sick newborn across the CoEs facilities. Our implementation was similar to another process conducted in Malaysia, highlighting the importance of effective health outcomes tracking and policy formulation. Additionally, the digitization and visualization of the adapted checklist tool not only streamlined data collection but also empowered health facility staff to monitor their own progress along the journey to CoE enabling the use of their own data to identify priority areas for improvement, and visualize successes fostering a culture of accountability.
Shortage of health personnel also came out as a gap in the implementation of QoC standards. There was limited specialized human resource trained in relevant skills such as delivery of essential newborn interventions and communication with clients with disabilities available in the units to implement MNH and SSN QoC standards. Health staffing shortages and how they significantly impact patient care leading to medical errors, high mortality rate, and increased infection rates is not a new phenomenon WHO (2020). Therefore, this gap was not a surprising finding. Shortages of health workforce as well as the inequitable distribution of health workers result in heavy workloads for existing staff, which in-turn affects the quality of care given by an overwhelmed health workforce. Furthermore, the QoC team members were of different professional work experience and required extended orientation time in mentorship and implementation of QI, MPDSR, M&E, Maternal and Newborn Care.
Another gap that came out notable weak linkages between MPDSR enquiries and implementation of QoC in maternal and newborn health. The weak linkages might have contributed to MPDSR findings not being effectively translated into QoC improvements. While MPDSR is meant to guide action to prevent future deaths, it often becomes a routine reporting exercise because of poor integration with quality improvement efforts. There is need for accountability and clear follow-up on MPDSR recommendations looped to QoC standards.
One of the best practices observed during the implementation of QoC standards was the use of structured peer mentorship to build capacity and support continuous quality improvement in CoEs. Such practices have previously been documented to improvement in knowledge, self-confidence, and working capacity which highlights effectiveness in the delivery of quality care. This practice emerged as a powerful enabler of QoC implementation, fostering not only skills development but also a culture of accountability, collaboration, and continuous improvement within MNH services. The culture created a collaborative and supportive environment that promoted shared learning and experience-based knowledge exchange.
This was similar with what another study reported on mentorship under neonatal health workforce.
The implementation of QoC standards strategically leveraged existing facility-level structures and resources. This was another best practice as it took away the need for requiring significant new investments for resource-limited settings. We utilized available human resources (i.e. focal point persons), infrastructure, essential supplies, and space to enhance service delivery and uphold QoC standards. The designation of facility focal point persons proved effective in coordinating activities, facilitating communication, and ensuring accountability during implementation. This best practice underscores the importance of contextual adaptability in health system strengthening. The practice demonstrates that quality improvement does not always require external inputs; rather, it can begin with better organization and optimization of existing resources.
The study had several strengths and limitations worth noting. Among the strengths, the assessment was conducted at three time points baseline, midline, and endline, which meant that data were generated in real time as implementation progressed. This enabled continuous comparison of results and facilitated learning during the rollout. Another strength was the use of a mixed-methods approach, which allowed quantitative findings to be triangulated with qualitative data, thereby enriching the analysis.
However, the study also had limitations. We were unable to conduct detailed analyses of the indicators within the short timeframe. A more accurate assessment of changes in various indicators would require a longer observation period beyond six months. Additionally, no statistical tests were performed to determine the significance of observed changes in standards of care, as the evaluations were not powered to detect statistically significant differences.
Conclusions
The pilot implementation of QoC standards in the seven CoEs demonstrated improvements in QoC standards, consistent improvements were seen in functional referral systems, communication and respect and dignity under both maternal and newborn and small and sick newborn. This implementation of QoC standards in seven CoEs initiative further demonstrated that integrating standardized QoC practices within existing health systems could significantly improve maternal and newborn as well as small and sick newborn outcomes. Sustaining and scaling these gains will require addressing resource gaps that have been identified as well as learn from the best practices that have been documented.
Conflict of Interest Statement:
The authors declare that they have no competing interests.
Funding Statement:
This research was done with the assistance of UNICEF country in Zambia.
Acknowledgements:
The authors would like to thank the contributions of the Ministry of Health, UNICEF, University of Zambia, and healthcare workers at the participating facilities for their tireless efforts to provide care to mothers and their newborns. Specifically we would like to the thank the following for their contributions; Mercy Kanswanta, Albert Bubala and Gomenzga Musekete for their technical support. Lastly, we wish to thank the UNICEF, Lusaka, Zambia and UNICEF, Regional Office South Asia (ROSA) Region for supporting implementation of the Quality of Care program.
Authors Contribution
CJ, AC, RM, GS and CC was involved in conceptualising the design of the study. CJ, AC, RM, GS, FG, MT and CC were involved in the design of the study. SM, SK, ML, DN, MM, TS and RM were involved in data collection and data analysis. All authors drafted, read, revised, and approved the final manuscript.
Availability of data and materials
The dataset utilized and/or analysed in this study are accessible and can be obtained from the MoH in Zambia.
References:
- You D. Levels and trends in child mortality: report 2022: Unicef; 2023.
- Quach A, Madaj B, Fahy K, Konate AT, Souley I, Marcel LO, et al. Cross sectional survey of maternal and newborn quality of care in Niger: Selected findings, lessons learned and recommendations. PLOS Global Public Health. 2024;4(11):e0003268.
- Organization WH, Group WB. Delivering Quality Health Services: A Global Imperative: OECD Publishing; 2018.
- Khatri RB, Durham J, Karkee R, Assefa Y. High coverage but low quality of maternal and newborn health services in the coverage cascade: who is benefitted and left behind in accessing better quality health services in Nepal? Reproductive Health. 2022;19(1):163.
- Yanful B, Kirubarajan A, Bhatia D, Mishra S, Allin S, Di Ruggiero E. Quality of care in the context of universal health coverage: a scoping review. Health Res Policy Syst. 2023;21(1):21.
- Paulson KR, Kamath AM, Alam T, Bienhoff K, Abady GG, Abbas J, et al. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. The Lancet. 2021;398(10303):870-905.
- Sheffel A, King S, Day LT, Marchant T, Muzigaba M, Requejo J, et al. Advancing maternal and newborn health care measurement: Developing quality of care indices for postnatal and small and/or sick newborn care in low-and middle-income countries. medRxiv. 2024:2024.10. 03.24314852.
- Organization WH. Standards for improving quality of maternal and newborn care in health facilities. Standards for improving quality of maternal and newborn care in health facilities2016.
- Smith JD, Li DH, Rafferty MR. The implementation research logic model: a method for planning, executing, reporting, and synthesizing implementation projects. Implementation Science. 2020;15(1):84.
- Mahmud SH, Mohamed NE, Bakar AA. Implementing quality assurance in public health facilities: The Malaysian experience. Journal of US-China Public Administration. 2015;12(10):752-8.
- Freitas A, Costa T, Marques B, Gaspar J, Gomes J, Lopes F, et al., editors. A framework for the production and analysis of hospital quality indicators. International Conference on Information Technology in Bio-and Medical Informatics; 2011: Springer.
- Jiwani SS, Cisse K, Mutua MK, Jacobs C, Njeri A, Adero G, et al. Levels and determinants of person-centred maternity care among women living in urban informal settlements: evidence from client exit surveys in Nairobi, Lusaka and Ouagadougou. BMJ Global Health. 2025;10(3).
- Oluoch-Aridi J, Smith-Oka V, Milan E, Dowd R. Exploring mistreatment of women during childbirth in a peri-urban setting in Kenya: experiences and perceptions of women and healthcare providers. Reproductive health. 2018;15(1):209.
- Kruk ME, Kujawski S, Mbaruku G, Ramsey K, Moyo W, Freedman LP. Disrespectful and abusive treatment during facility delivery in Tanzania: a facility and community survey. Health policy and planning. 2018;33(1):e26-e33.
- Gebeyehu NA, Adella GA, Tegegne KD. Disrespect and abuse of women during childbirth at health facilities in Eastern Africa: systematic review and meta-analysis. Frontiers in Medicine. 2023;10:1117116.
- Motala S, Ngandu S, Mti S, Arends F, Winnaar L, Khalema E, et al. Millennium development goals: Country report 2015. 2015.
- Moxon SG, Ruysen H, Kerber KJ, Amouzou A, Fournier S, Grove J, et al. Count every newborn; a measurement improvement roadmap for coverage data. BMC pregnancy and childbirth. 2015;15(Suppl 2):S8.
- Awang S, Agins B, Mohd Ujang IR, Narayanan DN, Zulkifli NW, Hamidi N. Development of the National Policy for Quality in Healthcare for Malaysia. Health Research Policy and Systems. 2023;21(1):119.
- Gopee N. Mentoring and supervision in healthcare: Sage; 2015.
- Giesen J, Berings M, Bakker‐Jacobs A, Vermeulen H, Huisman‐De Waal G, Van Vught A. Facilitating an Evidence‐Based Quality Improvement Learning Culture in Nursing Teams Through Coaching and Identification of Key Influencing Factors: An Action Research Approach. Journal of advanced nursing. 2025;81(11):7802-19.
- Boga MI, Musitia P, Oluoch D, Sen D, Dayo H, Haaland A, et al. Implementing a Change Process to Support Respectful Communication in Newborn Units in Kenya: Experiences, Opportunities, and Challenges.
- LEONE S. analysis of quality improvement in maternal and neonatal health care, Sierra Leone.
- Gadeka DD, Akweongo P, Whyle E, Aryeetey GC, Aheto JM, Gilson L. Role of actor networks in primary health care implementation in low-and middle-income countries: a scoping review. Global health action. 2023;16(1):2206684.
- James BC, Chassin MR, Goldberg HI, King JG, Todd JS. Implementing practice guidelines through clinical quality improvement; Improving quality of care with practice guidelines; Should we be implementing untested guidelines?; The relevance of practical experience to American hospitals; Quest for quality or cost containment; Reply. Frontiers of health services management. 1993;10(1):3.
- Gates PE. Think globally, act locally: an approach to implementation of clinical practice guidelines. The Joint Commission journal on quality improvement. 1995;21(2):71-85.