

Gender Differences in Autism: Initial Referral Insights
Gender Differences in Autism Presentation at Initial Clinical Referral: Diagnostic Measures, Empathy, and Adaptive Functioning
Cory Shulman, PhD¹, Zili Nir, PhD¹˒², Danielle Bitton, MA¹
- The Autism Center School of Social Work and Social Welfare The Hebrew University of Jerusalem.
- Faculty of Psychology The College of Law and Business Ramat Gan.
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Shulman, C., Nir, Z., Bitton D., Gender Differences in Autism Presentation at Initial Clinical Referral: Diagnostic Measures, Empathy, and Adaptive Functioning. [online] 14(1). https://doi.org/10.18103/mra.v14i1.7164
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v14i1.7164
ISSN 2375-1924
ABSTRACT
Background: Autism spectrum disorder is diagnosed more frequently in boys than girls, raising concerns that gender differences in symptom presentation and measurement may contribute to under-recognition in females. This study examined gender differences in autistic traits, diagnostic instrument scores, empathy, adaptive functioning, and co-occurring conditions among children evaluated at the time of initial referral for autism spectrum disorders.
Methods: Participants were 135 children (69 boys, 66 girls) matched on age and IQ. Parents completed the Social Responsiveness Scales-2, the Griffith Empathy Measure, and the Empathy Quotient questionnaires, and were interviewed using the Autism Diagnostic Interview-Revised and the Vineland Adaptive Behavior Scales-3rd edition. Children were assessed with the Autism Diagnostic Observation Schedule-2nd edition. Group differences, correlations, regressions, and moderation analyses tested gender-based variations in diagnostic profiles and associations among measures.
Results: Girls showed significantly higher parent-reported autistic traits on the Social Responsivity Scales-2 across all domains (p < .001), but no gender differences emerged on the Autism Diagnostic Observation Schedule-2 or the Autism Diagnostic Interview-Revised scores. Girls demonstrated higher cognitive empathy (p < .01), and empathy predicted adaptive functioning only for girls. Adaptive functioning was more strongly associated with autistic traits for girls than boys. Moderation analyses indicated that gender significantly altered the associations between Social Responsivity Scales-2, Autism Diagnostic Interview-Revised scores, empathy, and adaptive functioning. Girls with autism spectrum disorder were more likely to have a sibling diagnosed with autism, whereas boys were more likely to present with emotional or behavioral co-occurring conditions.
Conclusions: Findings suggest that autism spectrum disorder manifests differently across genders at initial referral and that standardized diagnostic instruments may insufficiently capture female-typical presentations. Identical diagnostic scores have different functional implications for boys and girls, underscoring the need for gender-informed diagnostic frameworks and more nuanced assessment practices.
Keywords: Autism spectrum disorder; gender differences; diagnostic measures and assessment; empathy; adaptive functioning.
INTRODUCTION
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by differences in social communication as well as restricted and repetitive patterns of behavior. Although ASD occurs across genders, males are diagnosed far more frequently than females, with prevalence estimates approaching a 3-4:1 ratio. This discrepancy has raised questions about whether ASD is truly more common in males or whether diagnostic practices, gendered expectations, and measurement limitations obscure recognition of ASD in girls. An increasing body of research suggests that multiple social, behavioral, and methodological factors contribute to lower observed rates of ASD diagnosis among females.
One contributing factor involves gendered expectations for social behavior, which shape how autistic traits are perceived by caregivers, educators, and clinicians. Girls typically demonstrate stronger social reciprocity and empathy, more sustained peer engagement, and greater emotional responsiveness than boys, and when girls exhibit social difficulties, these behaviors may be attributed to shyness, anxiety, or relational challenges rather than to a neurodevelopmental condition. In contrast, similar patterns in boys may be interpreted as more atypical relative to gendered norms, increasing the likelihood of referral for evaluation. As a result, misinterpreted, particularly when their social challenges are subtle or inconsistent across settings.
A related aspect of diagnostic disparities is clinician bias, including the persistent assumption that ASD is more common in boys. Historically, diagnostic criteria were derived from clinical samples composed largely of boys, shaping expectations about what autistic behavior should look like. Contemporary diagnostic training continues to emphasize male-typical characteristics, such as overt social aloofness or intense, circumscribed interests. These expectations may lead diagnosticians to under-recognize ASD in girls whose behaviors do not necessarily align with these patterns or who demonstrate relative social strengths that mask underlying difficulties. Consequently, girls may require greater functional impairment before ASD is considered diagnostically.
Measurement challenges further compound these issues. The major standardized diagnostic instruments—the Social Responsiveness Scale, Second Edition (SRS-2), the Autism Diagnostic Interview Revised (ADI-R), and the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2)—were developed and validated using samples composed predominantly of males. As a result, the content and scoring algorithms of these tools may reflect male-typical manifestations of ASD, raising the possibility of measurement bias in identifying ASD in girls. Differences in parent or caregiver expectations for gender-normative behavior may additionally influence how symptoms are reported on rating scales, particularly in domains related to social communication and interaction.
These limitations have particular relevance for constructs central to ASD diagnosis, such as empathy. Empathy, which involves emotional mental states, is a core aspect of social functioning and is commonly referenced in both diagnostic criteria and clinical impressions. Yet empathy itself is shaped by gendered socialization, with girls often expected to demonstrate more empathic behavior than boys. Introducing separate empathy measures therefore offers an important opportunity to evaluate whether empathy-related characteristics align with diagnostic scores similarly for boys and girls, or whether they reveal additional gender-linked differences not captured by standard ASD instruments. This feature of the present study adds another layer of nuance to understanding gender differences in diagnostic presentation in ASD.
METHODS
PARTICIPANTS
A matched sample of 69 boys and 66 girls (total of 135 children) with a suspicion of autism participated in this study. There were no significant differences by gender in age (boys: M = 89.09 months, SD = 30.18; girls: M = 88.15 months, SD = 35.00) or cognitive functioning as measured by standardized IQ tests according to age (boys: M = 87.99, SD = 17.74; girls: M = 87.97, SD = 19.19). Household composition was comparable across groups, with similar numbers of children per family, number of household members, and number of rooms in the residence. Most families reported a monthly income above the highest categorical threshold provided (>12,000 units), with no significant differences between groups. Mothers completed the majority of questionnaires (boys: 66.7%; girls: 65.2%), with a smaller proportion completed jointly by both parents and an even smaller minority completed by fathers only. Parental age did not differ significantly between groups (Mother age: boys: M = 43.01, girls: M = 43.06; Father age: boys: M = 45.84, girls: M = 45.43). Most parents were married (mothers: ~86%; fathers: ~89%), and the majority of mothers and fathers reported academic-level education. Family lifestyle (secular, traditional, religious, or ultra-orthodox) showed no gender-related differences.
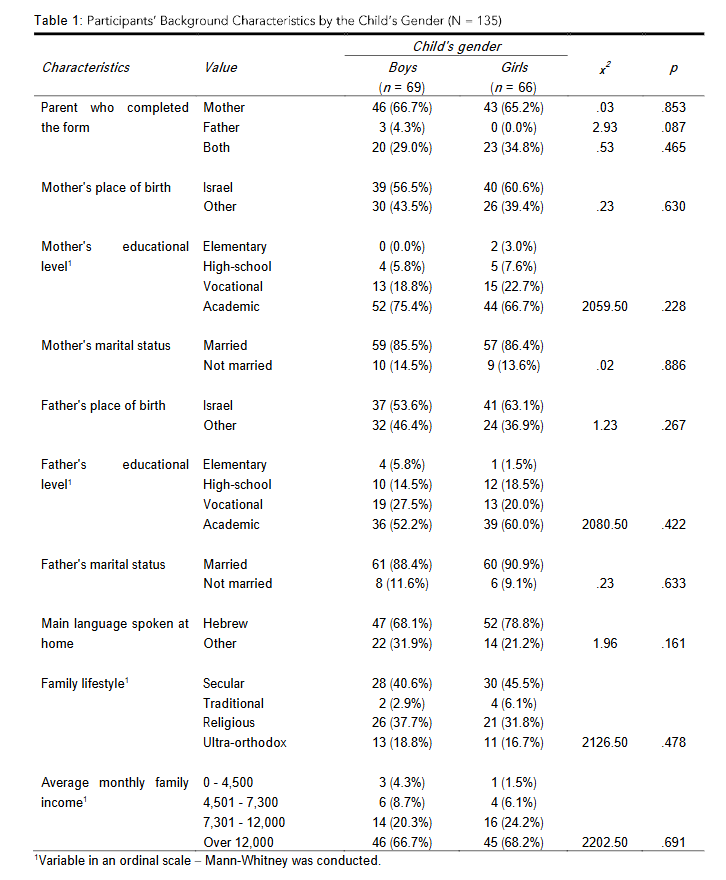
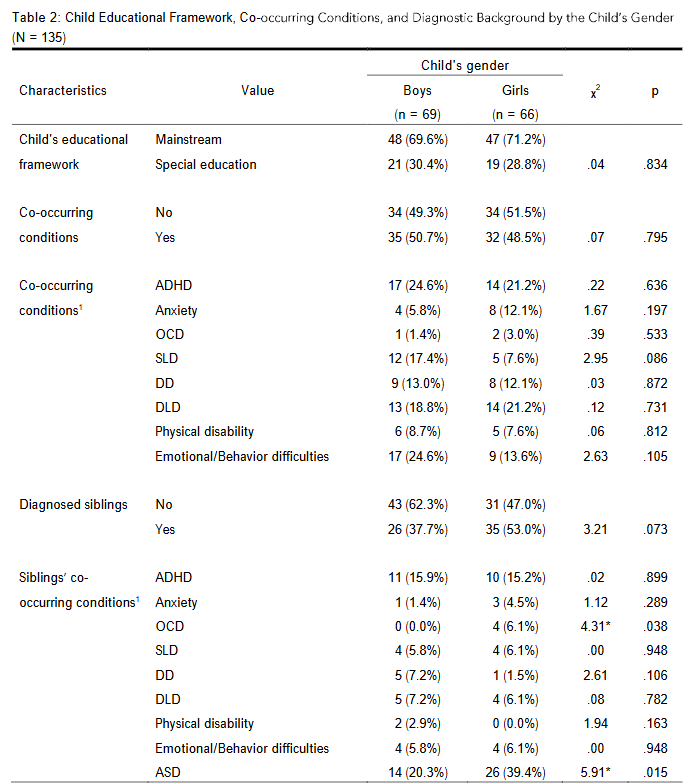
Educational placement was similarly distributed, with most children enrolled in mainstream education (boys: 69.6%; girls: 71.2%), and the remainder in special education settings (boys: 30.4%; girls: 28.8%). Co-occurring diagnoses were common in both groups, with 50.7% of boys and 48.5% of girls presenting at least one additional diagnosis. The prevalence of specific co-occurring conditions, including other neurodevelopmental disorders (e.g., ADHD, developmental language disorder, developmental delay) and psychiatric conditions (e.g., anxiety, OCD and emotional disorders) did not differ significantly by gender. Children could be assigned more than one co-occurring condition, resulting in totals exceeding the number of participants. The mean number of additional diagnoses per child was similar across genders (boys: M = 1.14, SD = 1.09; girls: M = 0.98, SD = 0.36). Approximately one third of the sample had siblings with diagnosed developmental or psychiatric conditions (boys: 20.3%; girls: 39.4%). The girls had significantly more siblings with an ASD diagnosis than the boys (X2 = 5.91; p = .015) as well as more siblings with an OCD diagnosis.
MEASURES
Three measures were used to characterize autism traits: (1) Social Responsiveness Scale-2 (SRS-2), (2) the Autism Diagnostic Interview-Revised (ADI-R); and (3) the Autism Diagnostic Observation Schedule-2 (ADOS-2).
The Social Responsiveness Scale 2nd Edition is a caregiver-completed questionnaire which yields three indices that were analyzed in the present study (total score, social communication/interaction (SCI) index, and restricted and repetitive behaviors (RRB) index). Higher raw scores indicate greater impairment. Raw scores were retained to avoid norm-referenced adjustments that might obscure variability within autistic samples. Missing item responses (<10% of items) were prorated following scoring guidelines. Protocols with >10% missing were excluded from analyses. Subscale scores were entered as continuous variables. No transformations were applied. The internal consistency of the total score, SCI index, and RRB index were high (α = .96, α = .95 and α = .86, respectively).
The Autism Diagnostic Interview Revised (ADI-R) is a semi-structured interview with primary caregivers. Sub-domain scores were obtained for social interaction domain, verbal and non-verbal communication domains, and restricted and repetitive behaviors (RRB) domain. Raw ADI-R scores were used rather than algorithm scores because the study aimed to examine dimensional variation in symptom expression rather than diagnostic classification. Algorithm scores are optimized for categorical diagnosis and may obscure meaningful variability, particularly in females with ASD, whose symptom profiles may not align with male-normed diagnostic thresholds. Use of raw scores allowed for greater sensitivity to individual and gender-specific differences and facilitated correlational and moderation analyses. The internal consistency of the social interaction domain, verbal and non-verbal communication domains, and restricted and repetitive behaviors (RRB) domain were good (α = .85, α = .78, α = .76 and α = .70, respectively).
The Autism Diagnostic Observation Schedule 2nd Edition (ADOS-2) is a standardized, semi-structured assessment tool used in establishing an autism diagnosis. A clinician interacts with the person being evaluated and, based on the person’s social communication, social interaction, and restricted/repetitive behaviors. Participants completed the appropriate module of the ADOS-2 based on their chronological age and expressive language level. All examiners met research reliability standards. Analyses drew on the Calibrated Severity Score (CSS), which adjusts symptom ratings for age and language level. CSS values (0-10) were used as continuous outcomes. The ADOS-2 Calibrated Severity Scores (CSS) have demonstrated good test-retest reliability across modules, with intraclass correlation coefficients in .87), which suggests that the CSS is a consistent metric of autism symptom severity, though internal consistency is not commonly reported due to the observational nature of the score.
Intellectual functioning in young children was assessed using age-appropriate, standardized instruments with strong psychometric properties. For preschoolers, the Mullen Scales of Early Learning (MSEL) was used, providing a measure of early cognitive ability as an Early Learning Composite score that serves as an estimate of general cognitive functioning and has demonstrated good internal consistency and test-retest reliability, with reported reliability coefficients typically in the good-to-excellent range. For children aged six years and older, intellectual ability is often measured using the Wechsler Intelligence Scales for Children-4th Edition (WISC-IV), which was used to obtain a Full-Scale IQ score. The WISC-IV has been extensively validated and shows strong reliability, with internal consistency coefficients for composite scores exceeding .90. Together, these instruments allow for developmentally sensitive and psychometrically robust assessment of cognitive functioning across early childhood and the school-age years.
Empathy was assessed using two measures, depending on the age of the participant. The empathy of children younger than 8 was assessed with the Griffith Empathy Measure (GEM), a 23-item parent-report questionnaire which assesses affective (20 items) and cognitive (3 items) empathy. Items are rated on a 9-point Likert scale scored so that higher scores indicate greater empathy. The Empathy Quotient (EQ) was used to measure empathy in children 8 years and older. It is a 60-item questionnaire comprising 40 empathy-relevant items and 20 fillers, with empathy items grouped into Cognitive Empathy (20 items), Affective Empathy (11 items), and Social Skills (9 items). EQ items are rated on a 4-point Likert scale. In order to compare results, Z-scores were calculated and used in analyses. Scores were treated as continuous variables with higher scores indicating greater empathic ability. The internal consistency among children younger than 8 of the total EQ, cognitive and affective components of empathy were good (α = .90, α = .70 and α = .89, respectively). The internal consistency among children younger than 10 of the total GEM, cognitive and affective components of empathy were good (α = .94, α = .92 and α = .83, respectively).
Adaptive functioning was evaluated using the Vineland Adaptive Behavior Scales 3rd Edition Comprehensive Interview Form. Analyses included standard scores for Communication, Daily Living Skills, and Socialization, and the Adaptive Behavior Composite (ABC). Standard scores (mean 100, SD 15), which were treated as continuous variables, were used for all analyses. The measure demonstrates excellent internal consistency (α = .86 – .99 across domains and composites) and moderate to high test-retest reliability (α = .94).
PROCEDURE
The study protocol received approval from the University Institutional Ethics Committee, and all procedures were conducted in accordance with institutional and international ethical standards for research involving human participants. Recruitment took place through well-baby clinics and educational facilities serving children within the target age range. Recruitment materials described the purpose of the study and invited interested families to contact the research team directly. Parents who expressed interest were provided with detailed information regarding study procedures. Following the receipt of informed consent, parents completed the set of standardized questionnaires assessing autistic traits and empathy. Subsequently, trained, research reliable clinicians conducted the ADI-R and the Vineland-3 interviews with a primary caregiver. A meeting was then scheduled for a comprehensive developmental assessment with the children, involving the Mullen Scales of Early Learning for younger children and the Wechsler Intelligence Scales for Children, which were administered by registered expert psychologists familiar with assessing autistic children. During the assessment, the child’s communication profile was examined using the ADOS-2. All assessments were administered individually in a quiet clinical setting. Data from parent-report measures, clinician interviews, and child assessments were integrated for analysis.
RESULTS
DATA ANALYSIS
All statistical analyses were conducted using SPSS Version 29. Preliminary analyses included inspection of descriptive statistics, skewness, kurtosis, and Shapiro Wilk tests to assess the distribution of study variables. Although most variables were approximately normally distributed (skewness and kurtosis between 1 and +1), the measures showed significant deviations from normality in the Shapiro-Wilk tests. As a result, nonparametric tests were used to examine gender differences and associations.
To address the first research aim, we examined boys and girls at the time of initial clinical referral for ASD using the SRS-2, ADI-R, ADOS-2, separate empathy measures and the children’s adaptive functioning using Mann Whitney U tests. Effect sizes for nonparametric tests were calculated using the formula 𝑟 = 𝑍/√𝑁. Spearman rank-order correlation coefficients, rather than Pearson correlations, were computed to address the second research aim regarding the associations between autism traits and empathy measures and the children’s adaptive functioning within each gender, given the non-normal distributions. Finally, to examine the third research question, whether children’s gender moderated the associations between each diagnostic instrument and adaptive functioning, as well as between empathy measures and adaptive functioning, moderation analyses were conducted using the PROCESS macro (Model 1) with bootstrapping (5,000 resamples) to generate bias-corrected 95% confidence intervals (CIs).
Only overall summary scores of the SRS (total), EQ (total z-score), and VABS were included in correlation analyses and moderation models. This decision was based on several considerations: (1) total scores provide conceptually broad, clinically interpretable measures of social impairment, empathy, and adaptive functioning; (2) the subscales within each instrument were highly intercorrelated (higher than r = .50); (3) this approach ensures that moderation findings reflect robust, generalizable patterns rather than idiosyncratic subscale effects; (4) it reduces the total number of statistical analyses conducted, thereby minimizing concerns related to multiple comparisons and type I error inflation. Covariates included IQ and which parent completed the questionnaires, which could potentially confound the findings. Bootstrapping was employed to address the non-normal distribution of the variables, providing robust estimation of interaction effects. Given the large number of statistical tests conducted in the study, controlling for type I error was a concern. While Bonferroni correction is a common method to adjust for multiple comparisons, it is often overly conservative and can increase the likelihood of Type II errors, particularly in studies with moderate sample sizes. To balance the risk of type I and type II errors, we set a more stringent alpha level of .01, rather than applying Bonferroni correction. This approach allows for a reasonable control of false positives while retaining sufficient power to detect meaningful effects. Therefore, results with significance alpha level of .05 should be considered marginally significant and interpreted with caution.
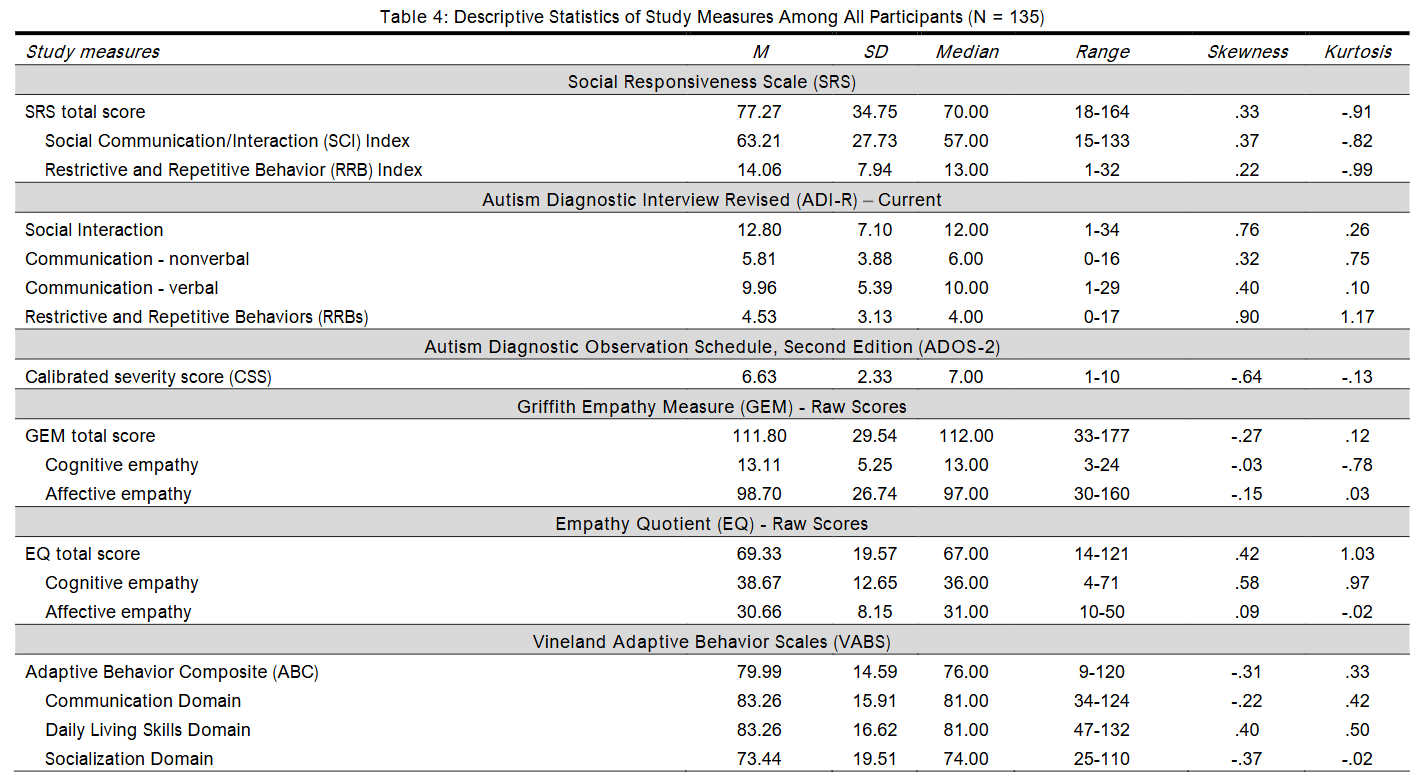
PRELIMINARY ANALYSES: DESCRIPTIVE STATISTICS AND NORMALITY
Descriptive statistics (mean, SD and median) as well as skewness and kurtosis values were calculated for all study measures. The skewness and kurtosis values indicate that most variables were reasonably close to normal, with values between -1 and +1, generally considered acceptable for a normal distribution. To be more robust, Shapiro Wilk tests were conducted to examine whether the study measures deviated significantly from normal distribution. The results indicated significant deviation from normality, supporting the use of nonparametric analyses in examining the study aims.
GENDER DIFFERENCES IN AUTISTIC TRAITS AND EMPATHY AT CLINICAL REFERRAL
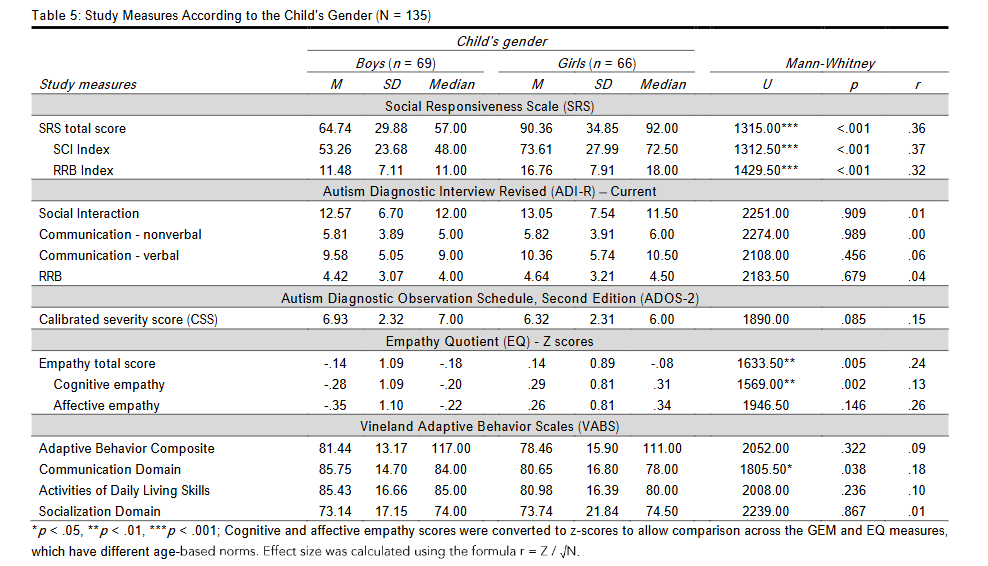
The Mann-Whitney test results indicated significantly higher scores on the SRS total score, SCI index, and RRB index among girls compared to boys with a suspicion of autism (all ps < .001), indicating greater impairment. In addition, the EQ total z-score and the cognitive component z-score were significantly higher among girls compared to boys (ps < .01). Finally, the gender difference in the communication standard score in VABS-3 was marginally significant (p = .038), with boys scored slightly higher than girls. The study measures according to gender appear in Table 5.
ASSOCIATIONS BETWEEN AUTISTIC TRAITS, EMPATHY, AND ADAPTIVE FUNCTIONING
The second research aim examined the associations between autistic traits, empathy, and adaptive functioning separately for boys and girls. Given the non-normal distribution of the study variables, as indicated by skewness, kurtosis, and Shapiro-Wilk tests, Spearman’s rank-order correlation coefficients were computed.
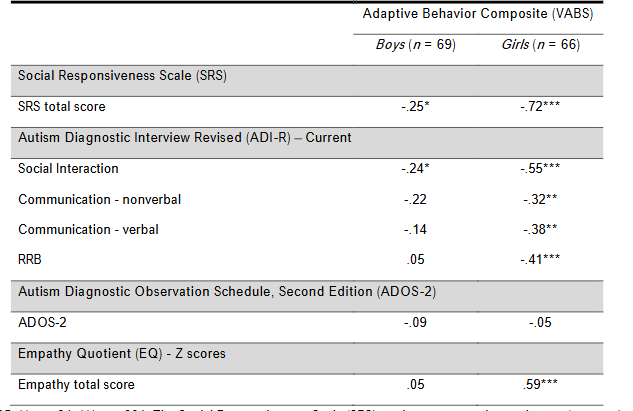
As presented in Table 6, higher levels of autistic traits were generally associated with lower adaptive functioning, with stronger and more consistent associations observed among girls than boys. Specifically, the SRS total score was negatively correlated with adaptive functioning in both boys and girls, but, while this association was strong and statistically significant among girls (r = .72, p < .001), it was only marginally significant among boys (r = .040). This pattern indicates that greater social impairment was associated with poorer adaptive behavior in both groups, with a substantially stronger association observed among girls. Similarly, ADI-R current scores showed negative associations with adaptive functioning, with different patterns across genders. Among boys, the association between social interaction scores and adaptive functioning was marginally significant (r = .049), whereas communication (verbal and nonverbal) and RRB scores were not significantly associated with adaptive behavior. In contrast, among girls, ADI-R social interaction (r < .001), nonverbal communication (r < .01), verbal communication (r < .01), and RRB scores (r < .001) were all significantly and negatively correlated with adaptive functioning, indicating that greater symptom severity across multiple ASD domains was associated with poorer adaptive behavior. ADOS-2 scores were not significantly associated with adaptive functioning in either boys (r = .464) or girls (r = .673), suggesting that in this sample, ADOS-2 total scores did not show a clear relationship with overall adaptive behavior. Regarding empathy, the EQ total z-score was not significantly associated with adaptive functioning among boys (r = .05, p = .675). However, among girls, empathy was positively correlated with adaptive functioning (r = .59, p < .001), indicating that higher levels of empathic abilities were associated with better adaptive behavior.
Overall, these findings suggest gender-specific patterns in the associations between autistic traits, empathy, and adaptive functioning, with girls showing stronger associations compared to boys.
GENDER AS A MODERATOR OF THE ASSOCIATIONS BETWEEN AUTISM-RELATED CHARACTERISTICS, EMPATHY, AND ADAPTIVE FUNCTIONING
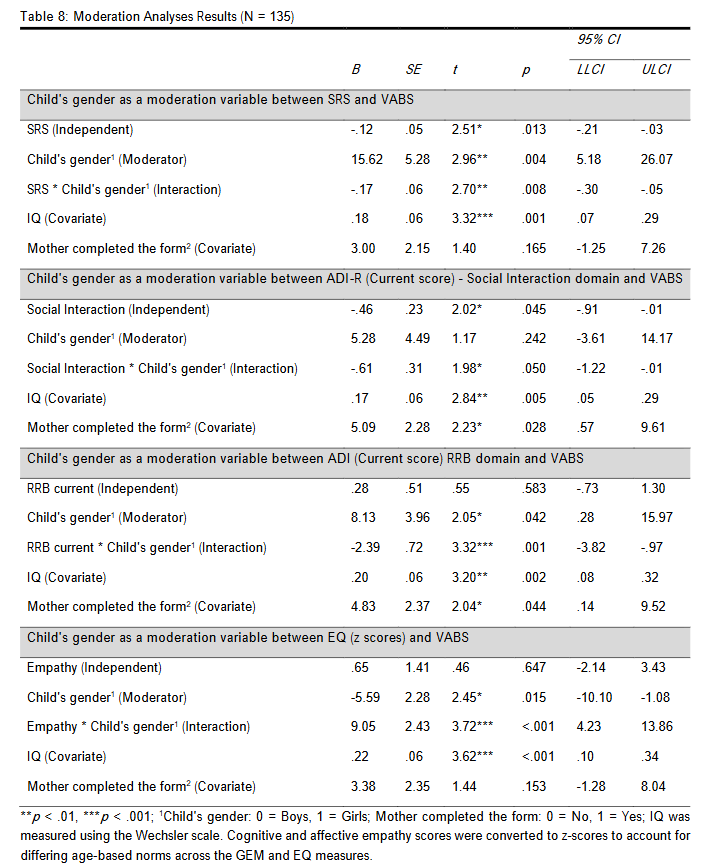
The third research aim examined whether child gender moderated the associations between autism-related characteristics (SRS, ADI-R, ADOS-2), empathy, and adaptive functioning. Moderation analyses were conducted using the PROCESS macro for SPSS (Model 1; Hayes, 2018). Given the non-normal distribution of the study variables, bias-corrected bootstrapping procedures with 5,000 resamples were employed to generate 95% CIs.
Prior to testing the moderation models, a multiple regression analysis was conducted to identify background variables that significantly explained adaptive functioning and therefore should be included as covariates. The Adaptive Behavior Composite score of the VABS served as the dependent variable. A stepwise regression approach was used to identify the most parsimonious set of explanatory variables while minimizing model overfitting.
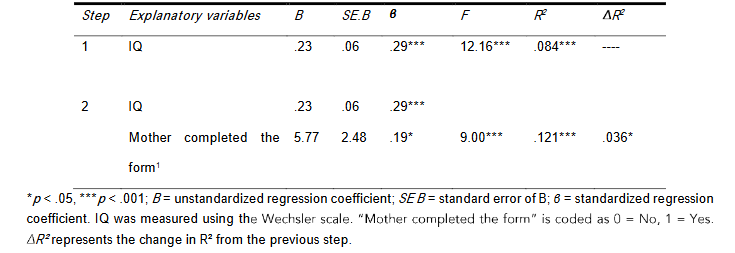
As presented in Table 7, IQ emerged as a significant explanatory variable in the first step, explaining 8.4% of the variance in adaptive functioning, F(1, 133) = 12.16, p < .001. In the second step, whether the mother completed the form entered the model and accounted for an additional 3.6% of the variance (R² = .036, p = .036), which can be considered a marginally significant contribution under the more conservative alpha level. Based on these findings, IQ and whether the mother completed the form were included as covariates in all moderation analyses.
The moderation results show that child gender significantly moderated the associations between several autism-related characteristics, empathy, and adaptive functioning. SRS total scores were marginally negatively associated with adaptive functioning, B = .12, SE = .05, p = .013, indicating that greater social impairment was associated with lower adaptive behavior. Child gender had a significant main effect, B = 15.62, SE = 5.28, p = .004. The interaction between SRS and child gender was significant, B = -.17, SE = .06, p = .008, 95% CI [-.30, -.05], indicating that the negative association between social responsiveness difficulties and adaptive functioning was stronger among girls than boys. For the ADI-R current social interaction domain, the main effect on adaptive functioning was marginally significant, B = -.46, SE = .23, p = .045. The main effect on child gender was not significant, B = 5.28, SE = 4.49, p = .242. The interaction with child gender was marginally significant, B = -.61, SE = .31, p = .050, suggesting a trend toward a moderating effect of gender on the association between social interaction difficulties and adaptive functioning. For the ADI-R current RRB domain, the main effect of RRB symptoms on adaptive functioning was not significant, B = .28, SE = .51, p = .583. The main effect on child gender was marginally significant, B = 8.13, SE = 3.96, p = .042. The effect of child gender as a moderator was marginally significant, B = 8.13, SE = 3.96, p = .042. The interaction between RRB symptoms and child gender was significant, B = -2.39, SE = .72, p = .001, 95% CI [-3.82, -.97], indicating a moderating effect of gender on the association between RRB and adaptive functioning. For empathy, the main effect on adaptive functioning was not significant, B = .65, SE = 1.41, p = .647. The main effect on child gender was marginally significant, B = -5.59, SE = 2.28, p = .015. However, the interaction between empathy and child gender was highly significant, B = 9.05, SE = 2.43, p < .001, 95% CI [4.23, 13.86], indicating that higher empathy was associated with better adaptive functioning among girls. Other measures, including ADI-R current verbal and nonverbal communication domains and ADOS-2 total scores, did not show significant or marginally significant moderation by child gender and are therefore not presented in detail.
DISCUSSION
The present study examined gender differences in autistic traits, diagnostic profiles, empathy, adaptive functioning, and co-occurring conditions among boys and girls referred for ASD evaluation at the time of initial clinical concern. By using two gender-balanced groups matched on age and IQ and incorporating multiple diagnostic instruments, including separate empathy measures, and adaptive functioning as an outcome measure, this study provides a uniquely detailed window into how ASD manifests in girls and boys at the earliest stage of the diagnostic process across childhood. The findings reveal distinctive gender-based patterns in parent-reported autistic traits, empathy, adaptive functioning, and contextual diagnostic factors, offering new insight into why ASD may be under-recognized or differentially identified across genders.
GENDER DIFFERENCES IN AUTISTIC TRAITS AT CLINICAL REFERRAL
The most robust gender difference emerged on the parent-report SRS-2, where girls demonstrated substantially higher levels of autistic traits across all scales (total scale, social communication/interaction and RRB indices). This stands in contrast to the widely held view that girls present with fewer or subtler social communication difficulties. Instead, our results indicate that by the time girls are referred for evaluation, their difficulties may be more pronounced or more disruptive than those of boys, suggesting a higher threshold for clinical concern in girls. This aligns with the hypothesis that girls may require more overt or impairing symptoms before adults recognize ASD-related difficulties.
Despite these parent-reported differences, no significant gender differences emerged in ADOS-2 calibrated severity scores or in ADI-R algorithm or current scores. This divergence between the SRS-2 and clinician- or interview-based assessments raises important questions about how ASD symptoms are recognized and interpreted across different contexts. One possibility is that parents observe difficulties in naturalistic settings that are less apparent in structured assessment environments, where demands are more predictable and adult-supported. Girls may show greater variability across contexts, struggling in unstructured peer interactions, for example, but appearing more regulated or socially engaged when interacting with a trained clinician in a one-on-one setting. Parents may therefore be capturing real but context-sensitive challenges that standardized tools, designed around more prototypical or male-typical ASD presentations, do not fully detect.
Alternatively, it is possible that clinicians are better able than parents to identify autistic features in girls, even when those features differ from male-typical patterns. Trained clinicians may recognize subtle social difficulties, gaze patterns, or interactional nuances during the ADOS-2 or ADI-R that parents do not necessarily label as autistic traits. Parents may interpret certain behaviors, such as emotional sensitivity, social withdrawal, or intense preoccupations, through gendered expectations rather than as potential ASD frameworks and expertise might allow them to identify ASD-consistent features that parents interpret differently.
These possibilities are not mutually exclusive. Instead, they highlight the complex interplay between context, expertise, and gendered expectations. Girls who experience significant social challenges in everyday life may transiently manage or mask these difficulties in clinical settings, reducing their visibility in standardized assessments. At the same time, parents may misinterpret or fail to recognize certain autistic behaviors as symptoms, particularly when they align with socially normative or gender-consistent patterns. The result is a multidirectional discrepancy: parents may see things clinicians do not, clinicians may see things parents do not, and standardized tools may insufficiently capture either perspective for girls. Overall, the inconsistency across measures underscores a critical diagnostic challenge: relying on standardized instruments that were normed primarily on male samples may result in an incomplete understanding of girls’ autistic experiences, particularly when those experiences are shaped by context, compensation, or gendered socialization. This further emphasizes the need for clinicians to integrate multiple perspectives, including parent report, clinical observation, developmental history, and functional assessment, to form a more comprehensive and gender-sensitive diagnostic picture.
EMPATHY AS A GENDER-DIFFERENTIATING CONSTRUCT IN AUTISM SPECTRUM DISORDER
A unique contribution of the present study was the inclusion of independent empathy measures, appropriate to the ages of the participants. Across instruments, girls scored significantly higher than boys on total empathy and cognitive empathy, with a marginal difference in affective empathy. These findings align with normative gender patterns, and therefore, have notable diagnostic implications. Clinicians may discount ASD in girls who exhibit relatively intact or heightened empathy, especially when empathy is misinterpreted as incompatible with ASD. Our data show that empathy should not be considered uniformly protective or clarifying; rather, empathy in girls may mask autistic traits in clinical interactions, contributing to underdiagnosis.
Critically, moderation analyses revealed that gender significantly altered the relationship between empathy and adaptive functioning. Not surprisingly, empathy strongly predicted better adaptive behavior among girls but not boys. This suggests that girls may use empathic abilities to compensate for social challenges in daily life, buffering functional impairment even when underlying autistic traits are present. This compensatory effect may delay recognition of ASD in girls and underscores the importance of evaluating empathy as a multidimensional construct.
ADAPTIVE FUNCTIONING AND DIFFERENTIAL ASSOCIATIONS WITH DIAGNOSTIC MEASURES
Although boys and girls showed similar mean levels of adaptive functioning across Vineland domains, the correlational patterns revealed marked gender differences. In girls, adaptive functioning demonstrated substantially stronger negative correlations with SRS-2 total scores and ADI-R current scores. In boys, these relationships were weaker or nonsignificant. This suggests that for girls, the presence of autistic traits is more directly and tightly linked to everyday functional impact.
Moderation models confirmed that gender significantly influenced how diagnostic scores predicted adaptive functioning, including for the SRS-2, ADI-R RRB domain, and ADI-R current scores. These findings reinforce the importance of evaluating gender as an active, shaping variable in ASD assessment rather than merely a demographic descriptor. The finding that identical diagnostic scores may have different implications for functional outcomes in boys and girls highlights a crucial, but often overlooked, dimension of ASD assessment: the clinical meaning of a given score is not uniform across genders. For girls, autistic traits, particularly those captured in parent-report or interview-based measures, were more strongly associated with adaptive functioning deficits than they were for boys. This suggests that when girls present with autistic features, these features may translate more directly into functional challenges in everyday life. Girls may experience greater social-emotional distress, heightened effort to navigate social situations, or accumulating functional impairment that becomes evident only when daily demands exceed their compensatory capacities. In boys, by contrast, the weaker associations between diagnostic scores and adaptive functioning imply that measured autistic traits may coexist with a broader range of adaptive outcomes. Boys may display overt autistic characteristics without equivalent declines in daily functioning, possibly because their behaviors align more closely with conventional autism profiles that clinicians and caregivers are attuned to recognize and support.
As a result, boys’ functional challenges may be buffered by earlier referral, more rapid recognition, or better alignment between their observable behaviors and existing diagnostic frameworks. For clinicians, this means that a score indicating different levels of day-to-day difficulty depending on whether the child is a girl or a boy. Standardized cutoffs and severity classifications, while essential for diagnostic consistency, may not fully capture the lived impact of autistic traits for girls. Overreliance on score thresholds without attention to gender-related patterns may therefore lead to underestimation of impairment in girls or overinterpretation of impairment in boys. These findings underscore the importance of broader functional profiles, particularly for girls. Clinicians should consider not only the numerical severity ratings but also how those behaviors interact with well-being, social environment, and available supports. Such an approach allows for a more nuanced interpretation of symptom severity and may help mitigate the gender-based disparities in ASD identification and service provision.
CO-OCCURRING CONDITIONS AND DIAGNOSTIC CONTEXT
Although boys and girls did not differ in IQ or age, additional analyses revealed meaningful gender-specific diagnostic contexts. Girls diagnosed with ASD were significantly more likely to have at least one sibling with ASD, whereas this pattern was less common among boys. This suggests that clinicians may be more willing to consider ASD in a girl when there is a known familial context. Girls without such cues may be less likely to be referred or diagnosed. This interpretation is consistent with concerns that clinicians require stronger external indicators before recognizing ASD in girls.
In contrast, boys diagnosed with ASD were more likely to present with co-occurring emotional or behavioral difficulties. These externalizing behaviors may increase clinical visibility and facilitate referral earlier in development, even when such behaviors are not specific to ASD. Together, these findings indicate that diagnostic pathways for ASD may be partially shaped by gender-based expectations and contextual cues. Clinicians may rely on family history to identify ASD in girls while relying on behavioral dysregulation to trigger evaluation in boys.
CLINICAL AND DIAGNOSTIC IMPLICATIONS
The present findings, taken together, point to several key implications for clinical practice, specifically that girls may require more severe or functionally impairing symptoms before ASD is recognized, especially in the absence of a family history of ASD. It is important to note that diagnostic tools developed with male-dominated samples may under-detect ASD in girls, particularly in structured settings where compensatory behavior is possible. Since differing empathy profiles emerged for girls and boys, empathy should not be used as a proxy for ruling out ASD in girls; instead, clinicians should evaluate how empathy interacts with social functioning and daily living skills. Adaptive functioning deficits appear more tightly coupled with autistic traits in girls, suggesting that functional assessments are especially crucial in the evaluation of girls. The study also highlighted that co-occurring externalizing problems may expedite ASD evaluation for boys, while their absence in girls may delay diagnostic consideration. Collectively, these findings support the need for gender-sensitive diagnostic frameworks and highlight the importance of integrating multiple sources of information when evaluating girls for ASD.
LIMITATIONS AND FUTURE DIRECTIONS
Several limitations warrant consideration when interpreting these results. The sample was drawn from a single clinical context, which may limit generalizability. Although empathy measures were harmonized using z-scores, differences in measurement structure across instruments may introduce interpretive complexity. Parent-report data, although essential, may be influenced by gendered expectations. Finally, the cross-sectional design precludes assessment of developmental trajectories, compensatory mechanisms, or changes in symptom expression over time. Future research should examine longitudinal patterns of autistic trait emergence in girls, the diagnostic impact of empathy and compensatory behaviors, and the distinctive presentation of co-occurring conditions according to gender. Studies should also explore clinician decision-making processes to better understand how contextual cues shape referral and diagnosis across genders.
CONCLUSIONS
The findings of this study underscore the complexity of how ASD presents in boys and girls at the time of clinical referral and demonstrate that diagnostic pathways are shaped not only by symptom severity but also by contextual, familial, and gendered factors. Girls referred for ASD showed markedly higher parent-reported autistic traits than boys, yet these differences were not reflected in clinician-administered measures such as the ADOS-2 or ADI-R. This discrepancy highlights important interpretive nuances: parents may observe challenges in naturalistic settings that are not elicited in structured assessment environments, while clinicians may identify subtler autistic features that parents do not recognize as atypical. These perspectives are not contradictory but complementary, emphasizing that both naturalistic parent observations and structured professional assessments are essential and each is incomplete on its own when evaluating girls for ASD.
Furthermore, the study demonstrates that identical diagnostic scores can carry different functional meanings for boys and girls. Autistic traits were more strongly associated with adaptive functioning in girls, indicating that daily living challenges may be more tightly linked to their underlying autistic characteristics. Clinicians relying solely on standardized cutoffs may therefore underestimate impairment in girls or interpret scores without considering gender-based variability in functional impact. These findings highlight the critical need for clinicians to contextualize diagnostic scores within a broader framework of social context and compensatory strategies. In addition, girls diagnosed with ASD were more likely to have siblings with ASD, suggesting that clinicians may require stronger external cues to consider ASD in girls. Boys, in contrast, were more likely to present with emotional or behavioral comorbidities, which may prompt earlier referral even when such difficulties are not specific to autism. These patterns indicate that the diagnostic process itself is shaped by gendered expectations about behavior and by the contextual cues clinicians and families use to interpret concerns. Taken together, these findings highlight the need for gender-sensitive diagnostic practices that integrate multiple sources of information, including parent report, clinician observation, empathy measures, and adaptive functioning profiles. They also point to the limitations of relying on diagnostic instruments developed predominantly with male samples, which may insufficiently detect or characterize ASD in girls. Girls showed higher parent-reported autistic traits, distinct empathy profiles, stronger associations between diagnostic scores and adaptive functioning, and unique patterns of co-occurring conditions and family history. Standard diagnostic tools failed to capture some of these differences, underscoring the need for more nuanced, gender-informed assessment practices. By integrating empathy measures, multiple diagnostic tools, and matched samples, this study contributes new insights into the underlying gender disparities in ASD diagnosis and highlights the importance of developing more equitable and comprehensive diagnostic approaches and clinician training.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
This study was supported by the Israel Science Foundation (ISF) (Grant number 1423/17).
Ethics Approval and Consent to Participate:
The study was approved by the Institutional Ethics Committee of The Hebrew University. Written informed consent was obtained from all parents or legal guardians of participating children.
Acknowledgments:
The authors thank the participating children and their families, as well as the clinicians and research staff who contributed to recruitment, assessment, and data collection.
REFERENCES:
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
- Lai MC, Lombardo MV, Auyeung B, Chakrabarti B, Baron-Cohen S. Sex/gender differences and autism: setting the scene for future research. J Am Acad Child Adolesc Psychiatry. 2015;54(1):11-24.
- Loomes R, Hull L, Mandy WPL. What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. 2017;56(6):466-474.
- Mandy W, Chilvers R, Chowdhury U, et al. Sex differences in autism spectrum disorder: evidence from a large sample of children and adolescents. J Autism Dev Disord. 2012;42(7):1304-1313.
- Duvekot J, van der Ende J, Verhulst FC, Greaves-Lord K. Factors influencing the probability of a diagnosis of autism spectrum disorder in girls versus boys. Autism. 2017;21(6):646-658.
- Lockwood Estrin G, Milner V, Spain D, Happé F, Colvert E. Barriers to autism spectrum disorder diagnosis for young women and girls: a systematic review. Rev J Autism Dev Disord. 2021;8(4):454-470.
- Hull L, Mandy W, Lai MC, et al. The female autism phenotype and camouflaging: a narrative review. Rev J Autism Dev Disord. 2020;7(4):306-317.
- Hull L, Petrides KV, Allison C, et al. Gender differences in self-reported camouflaging in autistic and non-autistic adults. Autism. 2020;24(2):352-363.
- Dworzynski K, Ronald A, Bolton P, Happé F. How different are girls and boys above and below the diagnostic threshold for autism spectrum disorders? J Am Acad Child Adolesc Psychiatry. 2012;51(8):788-797.
- Shulman C, Rice CE, Morrier MJ, Esler A. The role of diagnostic instruments in dual and differential diagnosis in autism spectrum disorder across the lifespan. Psychiatr Clin North Am. 2020;43(4):605-628.
- Rochat MJ. Sex and gender differences in the development of empathy. J Neurosci Res. 2023;101(5):718-729.
- Driver B, Chester V. The presentation, recognition and diagnosis of autism in women and girls. Adv Autism. 2021;7(3):194-207.
- Young H, Oreve MJ, Speranza MJ. Clinical characteristics and problems diagnosing autism spectrum disorder in girls. Arch Pediatr. 2018;25(6):399-403.
- Kaat AJ, Ghods SS, Farmer C, et al. Sex differences in clinical recognition and diagnosis of autism spectrum disorder: Evidence from a multisite cohort. J Child Psychol Psychiatry. 2020;61(2):135-144.
- Constantino JN, Gruber CP. Social Responsiveness Scale Second Edition (SRS-2) Manual. Torrance, CA: Western Psychological Services; 2012.
- Lord C, Rutter M, Le Couteur A. Autism Diagnostic Interview Revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord. 1994;24(5):659-685.
- Lord C, Rutter M, DiLavore PC, Risi S, Gotham K, Bishop S. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual. Torrance, CA: Western Psychological Services; 2012.
- Janvier D, Choi YB, Klein C, Lord C, Kim SH. Brief report: examining test-retest reliability of the Autism Diagnostic Observation Schedule (ADOS-2) calibrated severity scores (CSS). J Autism Dev Disord. 2022;52(3):1388-1394.
- Mullen EM. Mullen Scales of Early Learning: AGS Edition. Circle Pines, MN: American Guidance Service; 1995.
- Wechsler D. Wechsler Intelligence Scale for Children Fourth Edition (WISC-IV) Technical and Interpretive Manual. San Antonio, TX: Psychological Corporation; 2003.
- Dadds MR, Hunter K, Hawes DJ, et al. A measure of cognitive and affective empathy in children using parent ratings. J Child Psychol Psychiatry. 2008;49(2):111-118.
- Baron-Cohen S, Wheelwright S. The Empathy Quotient: an investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. J Autism Dev Disord. 2004;34(2):163-175.
- Lawrence EJ, Shaw P, Baker D, Baron-Cohen S, David AS. Measuring empathy: reliability and validity of the Empathy Quotient. Psychol Med. 2004;34(5):911-920.
- Sparrow SS, Cicchetti DV, Saulnier CA. Vineland Adaptive Behavior Scales, Third Edition (Vineland-3). San Antonio, TX: Pearson; 2016.
- Farmer C, Adedipe D, Bal VH, Chlebowski C, Thurm A. Concordance of the Vineland Adaptive Behavior Scales, second and third editions. J Intellect Disabil Res. 2020;64(1):18-26.
- George D, Mallery P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference. 16th ed. New York, NY: Routledge; 2019.
- Field A. Discovering Statistics Using IBM SPSS Statistics. 5th ed. London, UK: Sage; 2018.
- Tabachnick BG, Fidell LS. Using Multivariate Statistics. 7th ed. Boston, MA: Pearson; 2019.
- Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-based Approach. 2nd ed. New York, NY: Guilford Press; 2018.
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879-891.
- Armstrong RA. When to use the Bonferroni correction. Ophthalmic Physiol Opt. 2014;34(5):502-508.
- Napolitano A, Schiavi S, La Rosa P, et al. Sex differences in autism spectrum disorder: diagnostic, neurobiological, and behavioral features. Front Psychiatry. 2022;13:889636.
- Milner V, Colvert E, Mandy W, Happé F. A comparison of self-report and discrepancy measures of camouflaging: exploring sex differences in diagnosed autistic versus high autistic trait young adults. Autism Res. 2023;16(3):580-590.
- Quantity and quality of empathic responding by autistic and non-autistic adolescent girls and boys. Autism. 2021;25(1):199-209.
- Song Y, Nie T, Shi W, Zhao X, Yang Y. Empathy impairment in individuals with autism spectrum conditions from a multidimensional perspective: a meta-analysis. Front Psychol. 2019;10:1902.
- Harmsen IE. Empathy in autism spectrum disorder. J Autism Dev Disord. 2019;49(10):3939-3955.
- Mandic-Maravic V, Pejovic-Milovancevic M, Mitkovic-Voncina M, et al. Sex differences in autism spectrum disorders: does sex moderate the pathway from clinical symptoms to adaptive behavior? Sci Rep. 2015;5:10418.