






Obesity in African American Populations: Challenges & Solutions
Obesity among African American People in the United States: Epidemiological Patterns, Social Determinants, and Clinical Implications
Holly Lofton¹, Jamy D. Ard², Rameck R. Hunt³,⁴, Michael G. Knight⁵
- NYU Grossman School of Medicine, New York, New York, USA
- Wake Forest School of Medicine, Winston-Salem, North Carolina, USA
- Penn Medicine Princeton Health, Plainsboro Township, New Jersey, USA
- Rutgers RWJ Medical School, New Brunswick, New Jersey, USA
- The George Washington University School of Medicine and Health Sciences, Washington, DC, USA
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION: Lofton, H., et al., 2025. Obesity among African American People in the United States: Epidemiological Patterns, Social Determinants, and Clinical Implications. Medical Research Archives, [online] 13(6).
https://doi.org/10.18103/mra.v13i6.6674
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i6.6674
ISSN 2375-1924
ABSTRACT
Obesity represents a significant public health challenge affecting African American people in the United States, with disproportionate impacts across racial and ethnic groups. This comprehensive review examines the unique epidemiological patterns, social determinants, and management approaches for obesity among African American populations, with particular attention to the clinical implications.
Keywords
- Obesity
- African American
- Health disparities
- Social determinants
- Clinical implications
Introduction
Obesity has reached epidemic proportions in the United States, affecting approximately 42.4% of the adult population as of 2017–2018, a dramatic increase from 13.4–15.0% in the 1960s–1970s¹¹. However, this burden is not distributed equally across demographic groups. African American populations, particularly women, experience significantly higher rates of obesity compared to other racial and ethnic groups, regardless of socioeconomic status¹³. This disparity represents a critical challenge for public health practitioners and healthcare providers seeking to address the obesity epidemic through evidence-based, culturally appropriate interventions.
The etiology of obesity is complex and multifactorial, involving genetic predisposition, physiological mechanisms, behavioral patterns, environmental influences, and social determinants¹². Body mass index (BMI, kg/m²) remains the most widely used metric to categorize weight status, with obesity defined as a BMI ≥30 kg/m²¹¹. Although BMI provides a straightforward assessment tool, it has notable limitations, including inability to differentiate between fat mass and fat-free mass or account for variations in body composition across racial and ethnic groups¹¹.
The “obesity paradox” further complicates our understanding of obesity’s health implications, particularly for African American populations. This phenomenon describes the observation that individuals with higher BMI, particularly those categorized as overweight or having Class 1 obesity (BMI 30.0–34.9 kg/m²), may demonstrate better survival outcomes for certain medical conditions compared to normal-weight counterparts¹¹. Understanding these complex relationships is essential for developing targeted, effective interventions for obesity management in African American communities.
This review aims to synthesize current evidence regarding the epidemiology of obesity among African American people, examine the socioeconomic and structural determinants contributing to observed disparities, analyze challenges in obesity management specific to this population, and provide evidence-based recommendations for healthcare practitioners to implement culturally appropriate interventions.
Methodology
This narrative review was conducted through a comprehensive literature search of the Medline database on November 16, 2020. Search terms encompassed race-related terminology (African American OR Black* OR racial OR ethnic), obesity-related terms (obese OR obesity OR overweight), and topics of interest (prevalence OR etiology OR barriers* OR disparit* OR comorbidit* OR risk*)². Results were limited to English-language publications from 2010 to 2020.
Article selection proceeded through a systematic review of titles and abstracts for relevance. Additional references were identified through bibliographic review of retrieved articles, targeted searches, and author recommendations². The final collection of articles underwent critical evaluation for quality, relevance, and comprehensiveness of findings related to obesity in African American populations.
This methodological approach allowed for a thorough examination of both empirical studies and theoretical frameworks addressing obesity disparities, management challenges, and intervention strategies for African American communities, providing a foundation for evidence-based clinical recommendations.
Discussion and Analysis
EPIDEMIOLOGY OF OBESITY IN AFRICAN AMERICAN POPULATIONS
National Health and Nutrition Examination Survey (NHANES) data from 2017–2018 revealed that 49.6% of African American adults met criteria for obesity, compared to 42.2% among non-Hispanic White adults¹². This disparity demonstrates marked sex differences, with African American women experiencing substantially higher obesity rates (56.9%)
compared to African American men (41.1%)². Notably, African American men demonstrated slightly lower obesity prevalence than non-Hispanic White men (41.1% vs. 44.7%), suggesting complex sex-specific factors in obesity development and progression².
These patterns cannot be explained by socioeconomic status alone. While obesity prevalence typically decreases with higher education or income across demographic groups, African American women maintain higher BMI than White women at every level of educational attainment, with the greatest disparity observed among those with post-secondary education². Additionally, unlike other demographic groups, obesity prevalence among African American women does not differ significantly across income categories². Among African American men, the relationship between socioeconomic status and obesity follows a different pattern, with higher prevalence in higher-income groups compared to lower-income counterparts².
Longitudinal analysis indicates that disproportionate obesity rates among African American women represent a long-standing phenomenon rather than a recent development. A cohort study examining BMI changes between 1959 and 2006 among U.S. adults born between 1882 and 1986 found that BMI increases were already apparent among early 20th century birth cohorts, with the most rapid increase occurring among African American women².
HISTORICAL CONTEXT AND STRUCTURAL RACISM
Disparities in obesity prevalence and outcomes must be contextualized within historical patterns of structural racism in the United States. Structural racism refers to “the totality of ways in which societies foster racial discrimination, via mutually reinforcing inequitable systems” across housing, education, employment, healthcare, criminal justice, and other domains². These systems create and perpetuate unequal distribution of resources, opportunities, and burdens across racial groups.
Evidence directly links structural racism to obesity disparities. A county-level analysis of 324,572 U.S. adults found that measures of structural racism—including residential segregation, employment inequality, educational disparities, healthcare access, and criminal justice inequities—were associated with higher BMI among African American people². Similarly, a prospective study of 4,315 incident cases of obesity in African American women demonstrated positive associations between both everyday racism experiences and lifetime racism with increased obesity incidence². Longitudinal data further support connections between perceived discrimination and positive BMI trajectory among African American adults².
Residential segregation represents a significant pathway through which structural racism contributes to obesity disparities. Despite formal desegregation policies, residential segregation remains prevalent, concentrating African American populations in neighborhoods with limited access to quality education, healthcare resources, healthy food options, and safe recreational spaces, while increasing exposure to environmental pollutants and community violence². These neighborhood characteristics have been specifically associated with increased obesity risk among African American women².
HEALTHCARE ACCESS AND SYSTEMATIC BARRIERS
Healthcare access barriers significantly impact obesity management for African American people. Historical violations of medical ethics, including the infamous Tuskegee Study (1932–1972) and federally sanctioned healthcare segregation through the Hill-Burton Act (1946), have contributed to enduring mistrust of healthcare institutions in African American communities². This legacy manifests in decreased research participation and healthcare engagement, potentially limiting the effectiveness of obesity interventions².
Insurance coverage represents another structural barrier. Safety-net health systems disproportionately serve African American populations, yet few insurance plans provide comprehensive coverage for obesity management, including pharmacotherapy². Medicare specifically excludes obesity medication coverage,
while Medicaid drug coverage varies substantially by state². This often restricts African American patients to older, potentially more obesogenic medications for obesity-related complications rather than newer, more effective alternatives²³.
PATIENT-PROVIDER COMMUNICATION AND UNCONSCIOUS BIAS
Healthcare provider bias—both unconscious and conscious—affects quality of care for African American people with obesity. Research confirms that healthcare providers demonstrate implicit bias against both African American patients and patients with obesity, potentially affecting clinical decision-making and treatment recommendations².
Communication challenges between predominantly non-African American providers and African American patients contribute to suboptimal care. African American patients, particularly those with obesity, report lower likelihood of provider explanation adequacy and sufficient appointment time compared to White patients². African American patients with BMI ≥30.0 kg/m² are less likely to receive formal obesity diagnoses compared to White counterparts². Patients with racially/ethnically concordant providers demonstrate higher likelihood of receiving dietary guidance than those with discordant providers².
These communication barriers may result in missed opportunities for early obesity intervention and management. Evidence indicates that patients who receive explicit acknowledgment of their overweight status from providers demonstrate greater awareness of weight concerns, increased interest in weight management, and higher likelihood of recent weight loss attempts compared to those whose overweight status goes unacknowledged by providers².
PHYSICAL ACTIVITY, CARDIORESPIRATORY FITNESS, AND THE OBESITY PARADOX
Physical activity (PA) and cardiorespiratory fitness (CRF) represent critical factors in understanding obesity’s health implications, particularly regarding the “obesity paradox.” The obesity paradox describes the counterintuitive observation that individuals with overweight or mild obesity (Class 1: BMI 30.0–34.9 kg/m²) may experience survival advantages compared to normal-weight counterparts when managing certain chronic conditions, including cardiovascular disease, chronic kidney disease, chronic obstructive pulmonary disease, and specific cancers¹¹.
The “fat but fit” concept provides one explanatory framework for this phenomenon. Longitudinal data from the Aerobics Center Longitudinal Study (ACLS) demonstrated that individuals with obesity (defined by BMI, body fat percentage, or waist circumference) who maintained cardiorespiratory fitness levels above the age-specific and sex-specific 20th percentile showed mortality risks comparable to their normal-weight, physically fit counterparts¹¹. This evidence suggests that fitness may moderate obesity-associated mortality risk.
PA patterns vary substantially across racial/ethnic groups (Figure 1), influenced by cultural values, social norms, built environment characteristics, socioeconomic factors, and occupational patterns¹¹. Accessibility of safe recreational spaces, financial resources for structured exercise programs, and neighborhood walkability all affect PA opportunities in African American communities¹¹,². These disparities contribute to differences in CRF levels, which may impact cardiovascular health outcomes independent of weight status.
Racial/ethnic differences in the obesity paradox have been observed across multiple large cohorts (Table 1). Studies consistently demonstrate protective associations between higher BMI and mortality across racial/ethnic groups, though with varying relationship strength¹¹. Some research indicates particularly strong protective associations for African American participants with BMI ≥30 kg/m²¹¹. However, methodological considerations—including reverse causation, selection bias, competing death risks, and residual confounding—complicate interpretation of these findings¹¹.
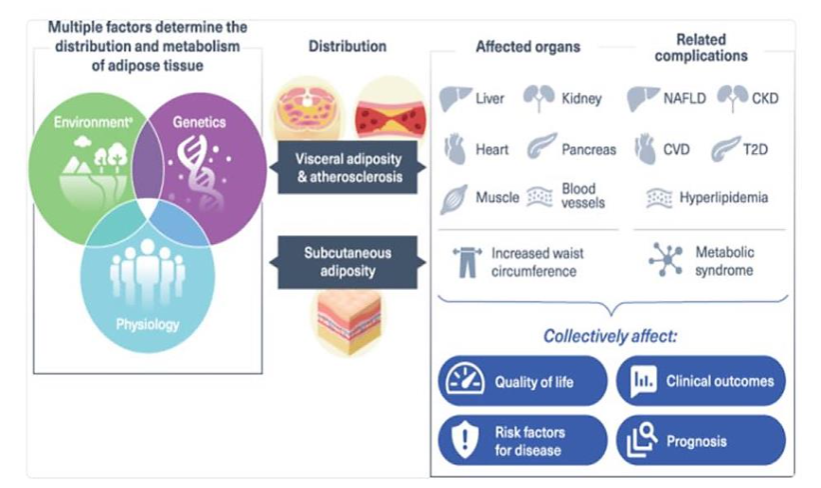
Table 1: Racial/Ethnic Variations in the Obesity Paradox Across Major Cohort Studies
| Author and year | Sample size | Race and/or ethnicity | Study outcomes |
|---|---|---|---|
| Wong et al., 1999 | 84,192 | Asian and Caucasian | In Asian participants, a U-shaped relationship between BMI and mortality risk was noted, with higher mortality observed at the lowest and highest BMI. |
| Glanton et al., 2003 | 151,027 | African American and Caucasian | BMI ≥30 kg/m² correlated to reduced mortality with a stronger association observed in African American participants. |
| Johansen et al., 2004 | 418,055 | African American, Asian and Pacific Islanders, Hispanic, and Caucasian | Higher BMI was associated with lower mortality rate in African American, Hispanic, and Caucasian, but not Asian participants. |
| Ricks et al., 2011 | 109,605 | African American, Caucasian, non-Hispanic, and Hispanic | Higher BMI was associated with survival advantage in African American, Hispanic, and Caucasian participants, with the highest observed in African American participants. |
| Hall et al., 2011 | 21,492 | Asian, Pacific Islander, Caucasian, and non-Hispanic | Higher BMI was associated with lower mortality in Asian, Pacific Islander, and Caucasian participants. |
| Park et al., 2013 | 40,818 | African American, Asian, and Caucasian | Lower mortality risk was observed across higher BMI levels regardless of race and/or ethnicity. |
| Author and year | Sample size | Race and/or ethnicity | Study outcomes |
|---|---|---|---|
| Wang et al., 2016 | 117,683 | African American, Caucasian, non-Hispanic, and Hispanic | Higher BMI was associated with lower mortality risk in African American and non-Hispanic Caucasian participants, while a U-shaped relationship was observed in Hispanic participants, such that lower and higher BMIs were not protective against mortality. |
| Doshi et al., 2016 | 123,624 | African American, Caucasian, non-Hispanic, and Hispanic | Inverse relationship between BMI and mortality in African American, Hispanic, and non-Hispanic Caucasian participants, with lowest risk for mortality observed in African American participants with a BMI ≥27.5 kg/m². |
BODY IMAGE PERCEPTIONS AND CULTURAL CONTEXT
Cultural perspectives on body image and weight significantly influence obesity management among African American populations. Research indicates that African American communities, particularly women, demonstrate greater acceptance of larger body sizes compared to White counterparts². This cultural context influences both self-perception of weight status and motivation for weight management.
Many African American women report misconceptions regarding normal weight, describing themselves as having healthy weight despite BMI classifications of overweight². Underestimation of weight category is common, potentially affecting perceived need for intervention². However, this cultural acceptance of larger body sizes may facilitate realistic treatment goal-setting, as African American patients may not hold unrealistic expectations of achieving “normal” BMI, which is rarely accomplished through non-surgical interventions².
When communicating with African American patients about obesity management, emphasizing health implications rather than aesthetic concerns may prove more effective. Research indicates that health represents the primary motivation for weight loss among African American people with obesity². However, many patients lack awareness of specific health implications associated with obesity and the degree of weight loss required (typically 5–10% sustained reduction) to achieve significant health improvements².
STRATEGIES FOR OBESITY MANAGEMENT IN AFRICAN AMERICAN POPULATIONS (FIGURE 3)
Effective obesity management for African American populations requires comprehensive approaches addressing both clinical and socio-structural factors. Healthcare practitioners should consider the following evidence-based strategies:
- Culturally Competent Communication:
Providers should acknowledge potential unconscious bias and improve communication techniques with African American patients. This includes providing adequate explanation of obesity diagnosis, health implications, and treatment options while allocating sufficient time for patient questions and concerns²³. - Health-Focused Motivation:
When discussing weight management with African American patients, emphasis should be placed on specific health benefits rather than aesthetic outcomes. Setting realistic treatment goals (typically 5–10% weight reduction) and clearly communicating associated health improvements can enhance motivation². - Addressing Social Determinants:
Healthcare practitioners should assess social determinants affecting patients’ weight management capabilities, including food security, neighborhood safety, transportation access, and financial resources. Connecting patients with community resources can address structural barriers to healthy behaviors²³.
4. Culturally Relevant Interventions:
Community-based and faith-based programs demonstrate particular effectiveness for African American populations. Such interventions leverage existing social structures and cultural strengths while providing peer support for behavior change².
5. Pharmacotherapy Considerations:
When prescribing medications for obesity or related conditions, practitioners should consider both efficacy across racial/ethnic groups and insurance coverage constraints. Advocating for equitable medication access represents an important component of comprehensive care²³.
6. Physical Activity Promotion:
Recommendations for physical activity should account for environmental constraints and cultural preferences. Supporting activities that can be performed safely within existing community contexts may enhance adherence¹².
7. Addressing Weight Stigma:
Healthcare settings should implement strategies to reduce weight stigma, which disproportionately affects African American patients with obesity and may contribute to healthcare avoidance¹³.
8. Provider Diversity and Training:
Increasing racial/ethnic diversity among healthcare providers and enhancing cultural competency training may improve care quality for African American patients with obesity².
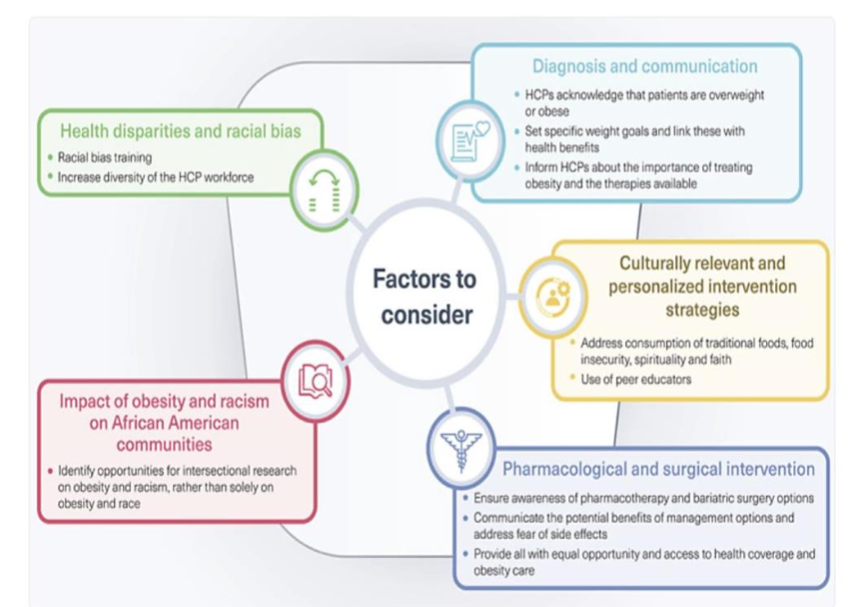
Figure 3
FIGURE 2: ECONOMIC DETERMINANTS OF OBESITY RISK
Economic instability can lead to limited financial resources and food insecurity, while disadvantaged neighborhoods create additional barriers (limited transportation, access to supermarkets, opportunities for physical activity, and exposure to violence). Limited education is associated with lower health literacy, fewer resources, and unhealthy behaviors. Inadequate access to health care, including primary care and nutritional counseling, exacerbates the risk of obesity⁴.
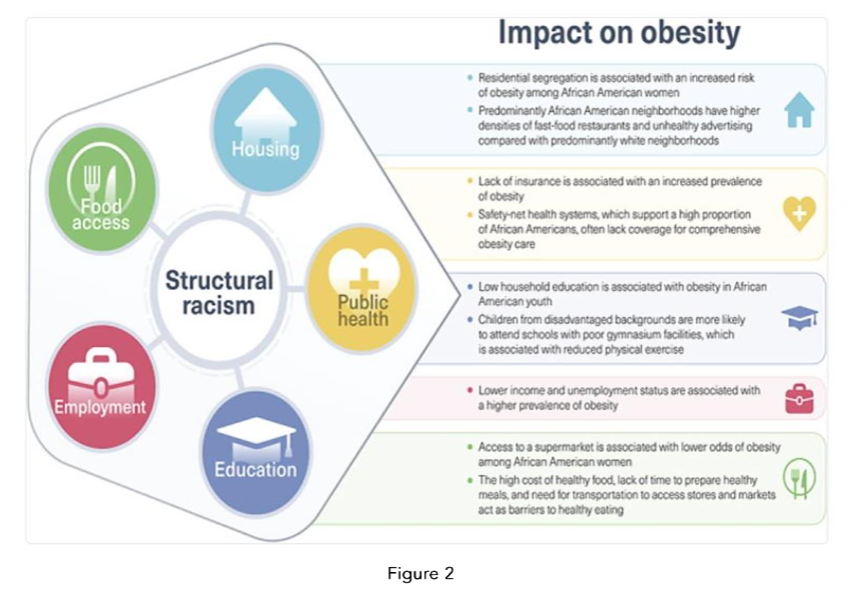
Figure 2
Conclusion
Obesity represents a complex public health challenge that disproportionately affects African American populations, particularly women, through intersecting social, economic, environmental, and healthcare factors. Structural racism creates and maintains systemic disadvantages affecting multiple determinants of obesity risk, including neighborhood characteristics, healthcare access, economic stability, and psychosocial stress. These factors operate collectively to produce observed disparities that cannot be attributed solely to individual behaviors or biological variations.
Effective obesity management for African American patients requires healthcare practitioners to adopt culturally sensitive, comprehensive approaches addressing both clinical needs and social determinants of health. Communication strategies emphasizing health outcomes rather than appearance, realistic goal-setting, and recognition of cultural perspectives regarding body size can enhance patient engagement. Structural interventions addressing community resources, healthcare access, and provider bias must complement individual-level approaches to achieve substantive improvements in obesity outcomes.Future research should explore the complex interplay between structural racism, physiological mechanisms, and obesity development in African American populations. Additionally, implementation science approaches are needed to identify optimal strategies for translating existing evidence into effective interventions within diverse healthcare and community settings. By addressing both proximal clinical factors and distal structural determinants, healthcare practitioners can contribute to more equitable obesity management for African American patients.
References:
Social, cultural and ethnic determinants of obesity. 2025.
https://art.torvergata.it/retrieve/d01a667c-338b-459c-95aa-bc43f83c31c1/NMCD%202025.pdf
Physical Activity, Cardiorespiratory Fitness, and the Obesity Paradox: Considerations for Race and/or Ethnicity. PMC11366992. 2024.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11366992/
A 9-year, bidirectional prospective analysis of depressive symptoms and adiposity: The African American Health Study. 2015.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10107750/
Maternal 24-h movement patterns across pregnancy and postpartum. PMC11068928. 2024.
https://pubmed.ncbi.nlm.nih.gov/36695059/