

Recurrent Shock Episodes: Identifying Common Causes
12 years of recurrent distributive shock episodes – Where to look when a search for common causes comes up short?
Robert Anderson APRN1, DNP, CNP
- Department of Pulmonary/Critical Care; Mayo Clinic (Rochester, Minnesota; USA)
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION: Anderson, R., 2025. 12 years of recurrent distributive shock episodes – Where to look when a search for common causes comes up short? Medical Research Archives, [online] 13(6).
https://doi.org/10.18103/mra.v13i7.6572
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6572
ISSN 2375-1924
Abstract
Shock is a state of circulatory failure with common etiologies to include sepsis, cardiac dysfunction, hemorrhage, and vascular flow obstruction. Accurate and timely identification of the etiology of shock is essential to prevent multi-organ dysfunction and death. This is a case of a 69-year-old female who presented with 12 years of recurrent shock episodes thought to be due to recurrent sepsis of unknown source. Despite an exhaustive review of infectious sources and other common shock etiologies, a durable explanation for shock was not found. A review of chronic medications demonstrated concurrent chronic use of lisinopril and verapamil; with discontinuation of lisinopril her episodes of recurrent shock ceased. Concurrent use of ACE-I and CCB can suppress native sympathetic cardiovascular responses to insignificant hemodynamic insults. Therefore, going back to the basics with a review of exogenous variables (i.e. medications) is an essential first step in identifying the cause of recurrent episodes of shock when no other common unifying etiology can be identified.
Keywords: distributive shock, recurrent episodes, diagnosis, management strategies
Introduction
Shock is defined as a state of circulatory failure in which cellular hypoxia is the outcome of inadequate oxygen delivery to meet cellular metabolic requirements. Timely optimization of hemodynamic parameters to deliver oxygen to the tissue is essential to prevent clinical deterioration and death. Identification of shock-etiology and shock-type helps to guide diagnostic and management strategies to allow for optimization of hemodynamic parameters to deliver oxygen to the tissues. Yet, even despite this, refractory shock can lead to irreversible tissue damage and subsequent multi-organ dysfunction and death.
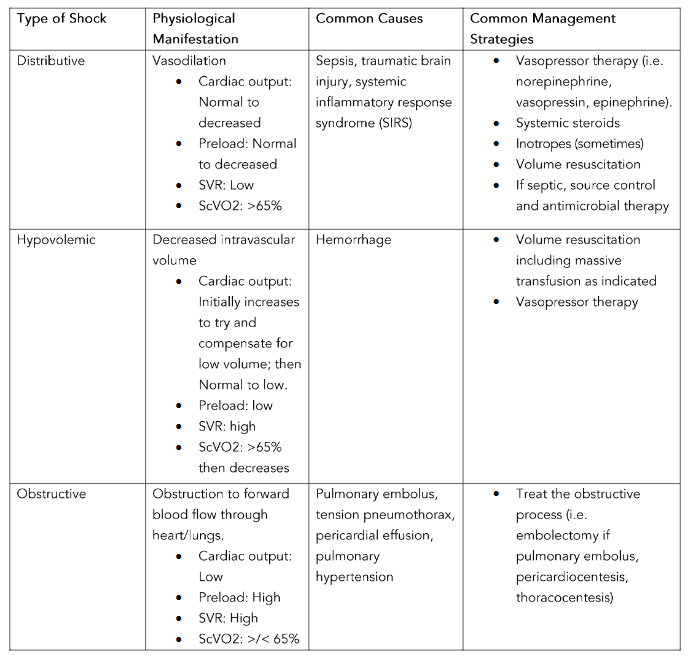
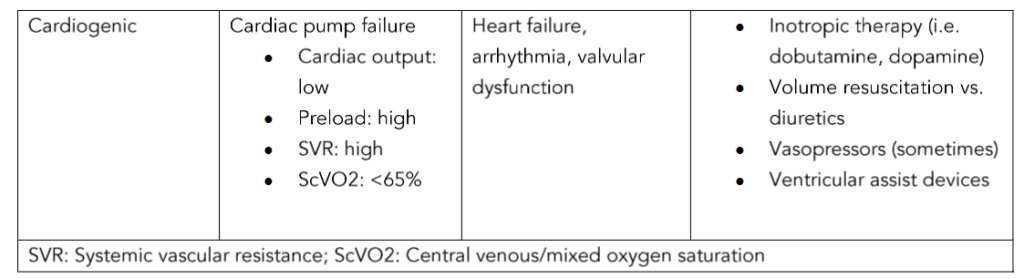
Accurate classification of shock-type is important in guiding appropriate diagnostic and management strategies. The four main classifications of shock include distributive (i.e. commonly due to sepsis), hypovolemic (i.e. volume loss such as hemorrhage), obstructive (i.e. pulmonary embolus), and cardiogenic (i.e. primary myocardium failure, valvular dysfunction, or arrhythmia). The most common shock presentation is that of distributive shock. Therefore, distributive shock carries the broadest etiology differential including infectious/sepsis, systemic inflammatory response syndrome (SIRS), neurogenic (i.e. traumatic brain injury), and undifferentiated vasoplegia.
References
Fountain J. H., Kaur J., and Lappin S. L. (2024). Physiology, renin angiotensin system, StatPearls. Retrieved from
https://www.ncbi.nlm.nih.gov/books/NBK470410/
Gaieski, D., Mikkelsen, M. (2025). Definition, classification, etiology, and pathophysiology of shock in adults. UpToDate. Retrieved from
https://www.uptodate.com/contents/definition-classification-etiology-and-pathophysiology-of-shock-inadults?search=shock&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
Herman L. L., Padala S. A., Ahmed I., and Bashir K. (2024). Angiotensin-converting enzyme inhibitors (ACEI), StatPearls. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK431051/
Huang J., Buckley N. A., Isoardi K. Z., Chiew A. L., Isbister G. K., Cairns R., Brown J. A., and Chan B. S. (2021). Angiotensin axis antagonists increase the incidence of haemodynamic instability in dihydropyridine calcium channel blocker poisoning, Clinical Toxicology, 59, 464–471.
Keller, J., Kendric, K., LeSaint, K. (2024). A case report of angiotensin II use in the treatment of refractory shock due to amlodipine and lisinopril toxicity. Case Reports in Critical Care. Retrieved from https://onlinelibrary.wiley.com/doi/epdf/10.1155/crcc/7543758
Wall, T. (2024). Side effects of antihypertensive drugs, chapter 17. Side effects of drugs annual. Elsevier.
Wira, C.R., Kearns, T., Fleming-Nouri, A., et al. (2024). Considering Adverse Effects of Common Antihypertensive Medications in the ED. Current Hypertension Reports, 26, 355–368.