





Precision Diagnostics in Trigeminal Neuralgia: Insights
“`html
Bridging Imaging and Molecular Biomarkers in Trigeminal Neuralgia: Toward Precision Diagnostics and Prognostication in Neuropathic Pain
Authors: M. Abikhalil, M. S. Bhav Jain, B.S.1, R. Shing, X. M. D., P. D. Christopher Jackson, M.D., Judy Huang, M.D., C. T. Chen Battegowda, M.D., P. Michael Lim, M.D.
Department of Neurosurgery, Stanford University School of Medicine, Stanford, California, USA. Department of Neurosurgery, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
OPEN ACCESS
Published 31 May 2025
CITATION
Abikhalil, H., et al., 2025. Bridging Imaging and Molecular Biomarkers in Trigeminal Neuralgia: Toward Precision Diagnostics and Prognostication in Neuropathic Pain. Precision Diagnostics in Trigeminal Neuralgia.
Introduction
Trigeminal neuralgia (TN) is a disabling, excruciating craniofacial pain syndrome that is episodic, electric shock-like pain paroxysms occurring in the distribution of one or more divisions of the trigeminal nerve (CN V). The pain is abrupt in onset and often precipitated by innocuous stimuli such as light touch, speaking, chewing, or even wind exposure. Such characteristic triggering features are found in as many as 79% of cases, are an important diagnostic feature, and are most often located in the perioral and nasal regions, corresponding to the preferential involvement of the V2 (maxillary) and V3 (mandibular) divisions.
Subsequent episodes of pain may occur in the absence of identifiable triggers, leading to increased morbidity and impaired quality of life. Insufficiently validated screening tools and many inappropriate online patient resources further hinder appropriate referrals for targeted diagnostic algorithms and patient resources. Early and accurate diagnosis is crucial since cases with both surgical and non-surgical indications vary dramatically according to the TN phenotype. Given that traditional clinical and radiological parameters are limited in terms of sensitivity and specificity, there is a developing interest in combining molecular biomarker research with advanced image acquisition techniques for improved diagnosis, prognostication, and treatment stratification of TN.
New advances in neuroimaging using deep learning machine learning techniques, together with proteomic and transcriptomic profiling, have emerged as promising avenues for enhancing the precision of TN diagnosis and treatment.
Table 1. Deep Learning Applications in Neuropathic Pain Imaging.
| Neuropathic Pain Condition | Imaging Modality | DL Model | Clinical Value | Limitations |
|---|---|---|---|---|
| Trigeminal Neuralgia | High-res T2-weighted MRI, DTI | U-Net, CNNs | Automated segmentation of classical vs idiopathic TN | Small sample sizes, generalizability across centers, and interpretability concerns |
| Sciatica | Lumbar MRI | CNN-based classifiers | Prediction of nerve root involvement | Lack of standardization; misclassification risk |
| Diabetic Neuropathy | Functional MRI | Diffusion Tensor Imaging; DTI | Integration of clinical features and imaging biomarkers | Limited clinical applicability |
These observations support a model in which distinct molecular cascades underlie divergent neuropathic pain mechanisms through shared downstream effectors such as neuronal sensitization and glial activation. Therapeutic targets aligned with these mechanisms have been increasingly identified through molecular profiling and differential gene expression studies. As an inhibitor of Wnt signaling and microglia–astrocyte crosstalk, SFRP1 may contribute to sustained neuropathic pain in TN and might serve as a new therapeutic target. FKBP5, previously associated with glucocorticoid resistance and stress-induced signaling, has emerged as a potential biomarker in psychiatric and neurodegenerative disorders.
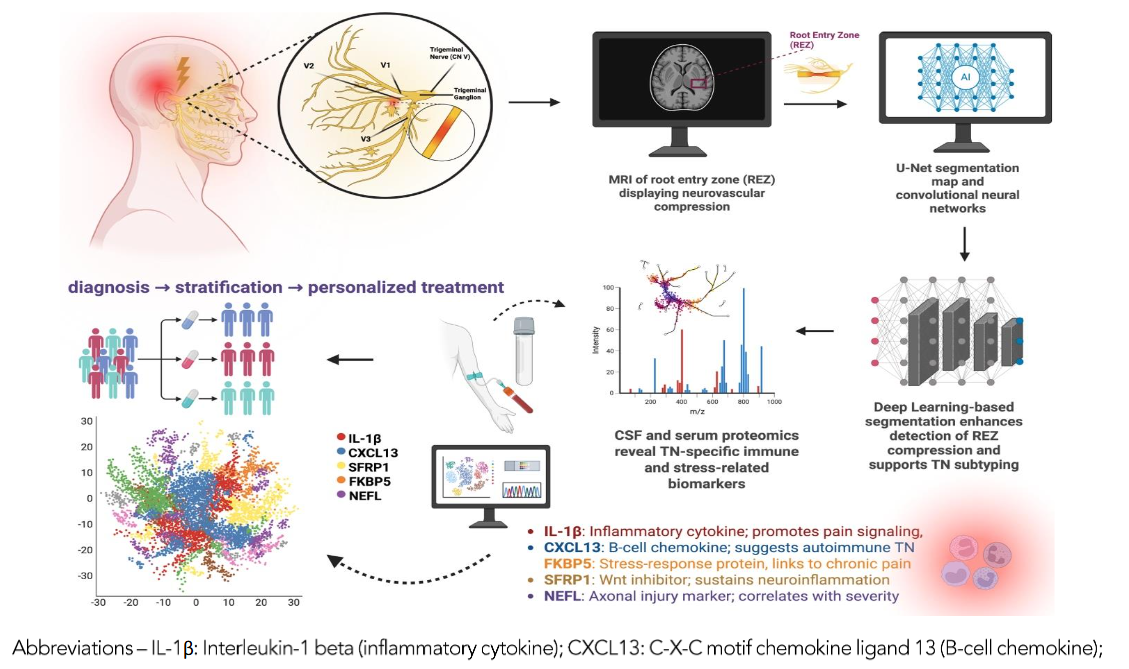
Integrating Imaging and Molecular Biomarkers: Toward Precision Neuropathic Pain Care
The whole picture of neuropathic pain demands an integrated approach that considers imaging, proteomics, and molecular dimensions. High-resolution imaging techniques, such as diffusion tensor imaging (DTI), magnetic resonance neurography (MRN), and high-resolution 3D MR, enable the characterization of trigeminal nerve compression, demyelination, and central white matter changes. Concurrently, proteomic and transcriptomic studies have identified molecular signatures in the neurovascular interface of TN patients following microvascular decompression (MVD), such as exposure to spinal cord injury markers.
Key Molecular Biomarkers in Trigeminal Neuralgia
| Biomarker | Function | Clinical Relevance |
|---|---|---|
| FKBP5 | Regulates glucocorticoid receptor sensitivity | Potential biomarker for stress response |
| SFRP1 | Inhibitor of Wnt signaling | May contribute to chronic pain mechanisms |
| PRDX1 | Antioxidant defense | Associated with neuropathic pain severity |
| GFAP | Astrocyte activation marker | Indicator of neuroinflammation |
Findings in TN may be generalizable to other neuropathic pain conditions, such as diabetic peripheral neuropathy and complex regional pain syndrome (CRPS), that share molecular signatures, such as axonal degeneration, neuroinflammation, and aberrant glial signaling. Radiomic features from high-resolution MR neurography or spinal imaging may unmask conserved structural patterns (such as dorsal root ganglia hypertrophy, white matter tract reorganization) among them. Moreover, proteomic markers identified in TN, such as S100B, PRDX1, and GFAP, may be universal biomarkers of neuropathic pain severity and therapeutic response.
Hence, the application of integrative mapping techniques will facilitate the identification of unified biomarker panels for pain conditions.
Future Directions in Neuropathic Pain Research
Future research in neuropathic pain will require next-generation, large-scale trials that integrate imaging, proteomics, single-cell transcriptomics, and clinical outcomes across patient populations. Improved single-cell proteomics and spatial transcriptomics will enable cell-type-specific mapping of neuropathic pain drivers in pain-affected nerves, DRG, and spinal cord segments. Concurrently, radiogenomic models that link genotype, molecular phenotype, and imaging biomarkers are poised to enhance subtype-specific diagnosis and guiding treatment.
References
- Cruciani, G., Giulia D. Stefano, and Andrea Trini. “Trigeminal neuralgia: new classification and diagnostic grading for practice and research.” Neurology 83.8 (2014): 754-762.
- Cruciani, Giorgio, et al. “Trigeminal neuralgia: diagnostic re-evaluation of patients referred for neurosurgery.” The Clinical Journal of Pain 18.1 (2002): 14-21.
- Benfato, Lars, et al. “Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia.” The Lancet Neurology 19.9 (2020): 784-796.
- DeSouza, D.D., Hodaie, M., Davis, K.D. “Abnormal trigeminal nerve microstructure and brain white matter in idiopathic trigeminal neuralgia.” Pain 2014; 155(1):37-44.
- Ellar, J.R., Raslan, A.M., Burcheli K.J. “Trigeminal neuralgia: definition and classification.” Neurosurg Focus. 2005;18(5):e3.
- Steinberg, Haldor. “Is this really trigeminal neuralgia? Diagnostic re-evaluation of patients referred for neurosurgery.” Scandinavian Journal of Pain 21.1 (2014): 788-793.
- Kolakowski, Łukasz, et al. “Interdisciplinary strategies for diagnostic and therapeutic management of trigeminal neuralgia.” Medical Image Analysis 75 (2021): 102-111.
Keywords
Trigeminal Neuralgia, Neuropathic Pain, Imaging, Molecular Biomarkers, Precision Medicine, Deep Learning
“`