





Subungual Melanoma: Diagnosis and Case Insights
Subungual Melanoma of the Toenail Presenting as Dystrophic Discoloration: A Case Report
Neil M. Paige, MD, MSHS¹² and Aksone Nouvong, DPM¹³
- VA Greater Los Angeles Healthcare System
- Department of Medicine, David Geffen School of Medicine at UCLA
- Department of Surgery, David Geffen School of Medicine at UCLA
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: Paige, N. M. and Nouvong, A., 2025. Subungual Melanoma of the Toenail Presenting as Dystrophic Discoloration: A Case Report. Medical Research Archives, [online] 13(5).https://doi.org/10.18103/mra.v13i5.6540
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6540
ISSN 2375-1924
ABSTRACT
Subungual melanoma (SUM) is a rare form of cutaneous melanoma that often presents with advanced disease due to delay in diagnosis or misdiagnosis. Here we share a case of subungual melanoma that presented to us; 48-year-old man with SUM of the third toenail that was initially believed to be onychomycosis. As a result, it is concluded that structured algorithmic approach is paramount to investigating pigmented lesions of the nail in order facilitate earlier diagnosis of SUM, to limit the possibility of life-threatening complications.
Introduction
Black-brown pigmentation of the nail or nail bed raises the suspicion of something sinister, like subungual melanoma. But in reality, melanoma of the nail apparatus is quite rare and other causes of darkening of the nail are much more common. However, making a timely and accurate diagnosis is of paramount importance as delays in diagnosing a subungual melanoma may result in limb loss, metastases, and even death.
Subungual melanoma is usually a variant of acral lentiginous melanoma that occurs on the palms, soles, fingernails or toenails. Subungual melanoma is unlike cutaneous malignant melanoma, as it does not appear to be related to sun exposure. Subungual melanoma accounts for 3 percent of all melanomas in white individuals compared to 30 percent in persons with greater (non-white) pigmentation.¹
The delay in the ultimate diagnosis of the SUM in the case below illustrates the difficulty in making an accurate and timely diagnosis due to concealment of the nail bed by nail itself; nail lacquer; or co-existing pathologies like onychomycosis. A systematic approach considering both historical and physical examination features of each component of nail apparatus will help guide the clinician to improve the accuracy of the diagnosis.
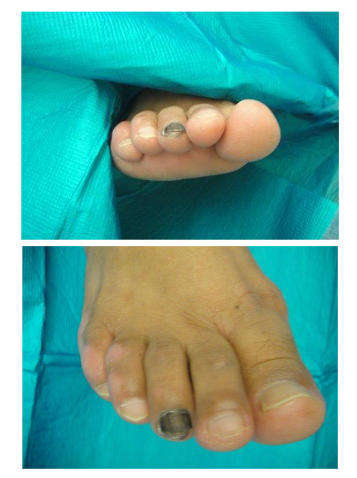
Case
48-year-old Latino male who initially presented with dystrophic discoloration of his third nail for 3–4 years. Related that the nail had progressively become more dystrophic over time. He denied pain, erythema or history of acute trauma. He did state that he often wears tight shoes and is fairly active. He was diagnosed with onychomycosis and was treated with multiple courses of the topical antifungal agents without improvement. As he was mainly asymptomatic, he did not seek further medical care though his nail continued to change. He continued to cut and file his nails down on a regular basis. He subsequently developed worsening discoloration of his nail, which gradually appeared more blackish in color, extending to the eponychium. He again did not seek further medical attention, as he was told that it was a subungual hematoma secondary to his activities and tight shoes. He presented to the clinic months later and due to a positive Hutchinson’s sign, the clinician referred him for wide excision biopsy of the nail, which revealed an acral lentiginous melanoma. Ultimately, he had a terminal Syme’s toe amputation. He underwent a sentinel lymph node biopsy, and the pathology report results were negative for metastasis.
Anatomy of the Nail Apparatus
The nail unit is comprised of the nail plate, the nail bed which lies under the nail and the matrix. The nail plate is a modified form of stratum corneum, providing a laminated keratinized structure overlying the nail bed and matrix.² The nail grows proximally at the germinal matrix. At the base of the nail there is the lunula which is the crescent shaped pale color seen. The nail is surrounded by epidermis to create both proximal and lateral nail folds. At the base of the nail the skin is referred to as the eponychium. Melanocytes are present within the nail matrix both distal and
proximally and are the cells that are ultimately responsible for melanonychia or melanocyte activation of the nail. A feature often seen is longitudinal melanonychia (LM) is a clinical description defined as a black-brown pigmented band that extends from the proximal nail fold to the free edge of the nail plate.³ This can occur in both malignant and non-malignant conditions.
Diagnostic approach to melanonychia
Given the multitude of etiologies when considering melanonychia, recent literature recommends a structured stepwise approach.⁵ Black-brown coloring of the nail apparatus always raises the concern for subungual melanoma. But in truth, this diagnosis is relatively uncommon. In one series of 100 patients, only one in 25 patients with nail discoloration needed additional careful evaluation, whereas the remaining cases were deemed to be likely from a benign condition.⁴
A detailed history and physical examination is important in determining the etiology of a pigmented lesion of the nail apparatus. Piraccini and colleagues make the following recommendations when evaluating patients with nail discoloration: All nails should be evaluated including both toenails and fingernails. The evaluation should be carried out in a well-lit area.⁴
Piraccini and colleagues developed a diagnostic algorithm as follows.⁴ The first step is to determine if melanonychia is present or if the discoloration is due to other reasons. Subungual hematoma is by far the most common cause of black-brown nail pigmentation. A history of trauma is likely, but hematomas can also occur from repetitive microtraumas. Subungual blood can persist for a long period of time. Other causes of exogenous pigmentation include pigmented nail lacquers and staining of fingernails of heavy smokers (especially in the thumb, index, and middle fingers). Scraping with a curette will reveal a normal nail underneath. Fungal infections or chronic Pseudomonal infections of the nail can also appear black-brown in color. Another not uncommon benign cause is pyogenic granuloma.
If melanonychia is confirmed, the number of nails involved also may suggest a benign etiology. Subungual melanoma is exceptionally uncommon to occur in multiple nails at the same time. Common causes of benign LM include aging nails in certain races, especially in African-American, Asians, and Latino populations (persons who also have a higher risk of SUM). Melanocytic activation might occur during many circumstances, such as physiologically in darkly pigmented skin individuals; hormonally stimulated during pregnancy; or in response to inflammatory or infectious stimuli of the nail unit (including but not limited to nail psoriasis, and nail lichen planus), chemotherapeutic agents, adverse effects of drugs, repetitive frictional trauma, systemic disorders (Laugier-Hunziker syndrome, Peutz-Jeghers syndrome).⁵⁶⁷
Subungual melanoma incidence and diagnostic features
Subungual melanomas are a subtype of cutaneous melanomas that typically arise from the nail matrix and spreads to other areas of the nail unit. The disease is relatively rare with reported incidence rates of 0.7–3.5% of all melanoma cases.⁴ There is equal distribution between men and women. It is most commonly diagnosed in the sixth decade of life for women and seventh for men.⁸ Though it can be found on any digit, the great toe (hallux) and thumb are most affected, accounting for 75–90% of cases.⁹ In the African population, SUM accounts for 75% of melanomas, 25% in the Chinese population and 10% in the Japanese population.⁸
Subungual melanoma is often diagnosed at advanced disease stages due to varied clinical presentation, misdiagnoses, late presentation, insufficient biopsy material, co-existing pathologies that mask signs of melanoma, and concealment with nail lacquer. Common misdiagnoses include subungual hematoma, onychomycosis, pyogenic granuloma, and ingrown toenails. Nail plate dystrophy is also a common finding in patients with SUM, making the diagnosis more difficult.
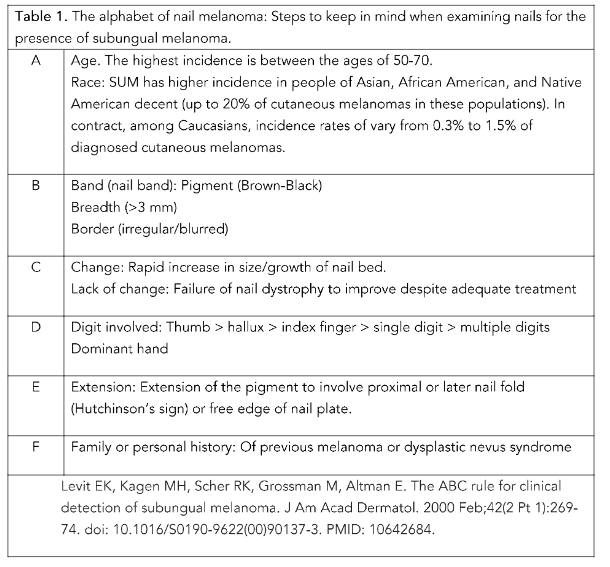
Levit and colleagues developed a nail specific “ABCDEF” rule for SUM which expands the ABCD rule which is used for evaluating cutaneous melanoma to provide a construct to improve the rate and timeliness of diagnosis.⁵ ¹⁰
Not all melanomas present with the typical physical exam findings such as the dark pigmentation of the nail bed or adjacent cuticle. Black et al. describe a case of osteoinvasive amelanotic melanoma of the nail bed that was difficult to diagnose due to lack of pigmentation on physical examination.¹¹ ¹² Indeed, Levit notes the incidence of amelanotic melanoma is more common in SUM when compared to cutaneous melanomas.¹³ One characteristic feature that can preclude to diagnosing SUM is the Hutchinson’s sign. Subungual melanoma originates in the nail matrix and often first appears with longitudinal melanonychia. The typical mode of spread is from the nail matrix directly to the adjacent nail plate and across the nail bed and to the hyponychium and nail folds.¹³ However, Hutchinson’s sign which when present is helpful to suggest the diagnosis of SUM, will likely not be present in patients with amelanotic SUM.
Treatment and Prognosis
After confirmation with a biopsy, the standard treatment for SUM is surgical resection and/or digital amputation. Functional outcome should be considered when planning treatment. A recent meta-analysis noted a 5-year cumulative survival rate of 77.0%.¹⁴ Sentinel lymph node biopsy in patients with cutaneous melanoma often provides important
prognostic information. But in patients with SUM, Leberherr and colleagues conclude there is limited studies to suggest a definitive conclusion as to when SLNB is required. They suggest further scientific studies can address this knowledge deficiency.¹⁴
Conclusion
Overall, a suspicious black-brown lesion of the nail apparatus should be thoroughly evaluated using a stepwise and thoughtful approach. Although rare, SUM is a “do not miss” diagnosis that should always be present on the differential diagnosis. A SUM should be considered in patients that are being treated for a suspected benign lesion which does not improve with standard therapy.
Financial Supports and Conflict of Interest:
None.
References to off-label and/or investigational usage(s) of pharmaceuticals or instruments in their presentation:
None.
Acknowledgement of Commercial Support:
No commercial support was received in the production of this activity.
References
1. Güneş P, Göktay F, Haneke E. A case of adult-onset longitudinal melanonychia due to nail matrix compound nevus. J Cutan Pathol. 2020 Dec;47(12):1159-1163. doi: 10.1111/cup.13800. Epub 2020 Sep 10. PMID: 32640104.
2. de Berker D. Nail anatomy. Clin Dermatol. 2013 Sep-Oct;31(5):509-15. doi: 10.1016/j.clinder matol.2013.06.006. PMID: 24079579.
3. Nevares-Pomales OW, Sarriera-Lazaro CJ, Barrera-Llaurador J, Santiago-Vazquez M, Lugo-Fagundo N, Sanchez JE, Sanchez JL. Pigmented Lesions of the Nail Unit. Am J Dermatopathol. 2018 Nov;40(11):793-804. doi: 10.1097/DAD.00000000 00001106. PMID: 30339563.
4. Piraccini BM, Dika E, Fanti PA. Tips for diagnosis and treatment of nail pigmentation with practical algorithm. Dermatol Clin. 2015 Apr;33(2): 185-95. doi: 10.1016/j.det.2014.12.002. Epub 2015 Feb 7. PMID: 25828711.
5. Levit EK, Kagen MH, Scher RK, Grossman M, Altman E. The ABC rule for clinical detection of subungual melanoma. J Am Acad Dermatol. 2000 Feb;42(2 Pt 1):269-74. doi: 10.1016/S0190-9622 (00)90137-3. PMID: 10642684.
6. Ma DL, Vano-Galvan S. Hyperpigmentation in Laugier-Hunziker syndrome. CMAJ. 2011 Sep 6;183(12):1402. doi: 10.1503/cmaj.110211. Epub 2011 Aug 8. PMID: 21825050; PMCID: PMC3168631.
7. Mole RJ, MacKenzie DN. Subungual Melanoma. 2023 Apr 14. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 29494087.
8. Decker A, Connolly KL, Lee EH, Busam KJ, Nehal KS. Frequency of Subungual Melanoma in Longitudinal Melanonychia: A Single-Center Experience. Dermatol Surg. 2017 Jun;43(6):798-804. doi: 10.1097/DSS.0000000000001112. PMID: 28296790.
9. Ingkaninanda P, Visessiri Y, Rutnin S. Clinicopathological Features and Prognostic Factors of Malignant Melanoma: A Retrospective Analysis of Thai Patients in Ramathibodi Hospital. J Med Assoc Thai. 2015 Aug;98(8):820-7. PMID: 26437541.
10. Littleton TW, Murray PM, Baratz ME. Subungual Melanoma. Orthop Clin North Am. 2019 Jul;50(3):357-366. doi: 10.1016/j.ocl.2019.03.003. PMID: 31084838.
11. Black AT, Lahouti AH, Genco IS, Yagudayev M, Markinson BC, Spielfogel WD. A Rare Case of Osteoinvasive Amelanotic Melanoma of the Nail Unit. Skin Appendage Disord. 2021 Feb;7(2):139-143. doi: 10.1159/000512331. Epub 2020 Dec 23. PMID: 33796562; PMCID: PMC7991606.
12. Kokikian N, Baltayan A, Nouvong A. A rare case of circumferential osteoinvasive subungual melanoma: A case report. SAGE Open Med Case Rep. 2024 May 30;12:2050313X241257698. doi: 10.1177/2050313X241257698. PMID: 38828380; PMCID: PMC11143801.
13. Koushk Jalali B, Kreuter A. Subungual melanoma. CMAJ. 2018 Aug 27;190(34):E1018. doi: 10.1503/cmaj.180513. PMID: 30150244; PMCID: PMC6110648.
14. Lieberherr S, Cazzaniga S, Haneke E, Hunger RE, Seyed Jafari SM. Melanoma of the nail apparatus: a systematic review and meta-analysis of current challenges and prognosis. J Eur Acad Dermatol Venereol. 2020 May;34(5):967-976. doi: 10.1111/jdv.16121. Epub 2020 Jan 6. PMID: 3178 8861.