





Cross-Border Malaria Prevention: Knowledge and Attitudes
KNOWLEDGE, ATTITUDES, AND PERCEPTIONS OF TRAVELLERS TOWARDS CROSS-BORDER MALARIA PREVENTION MEASURES IN KWAZULU-NATAL, SOUTH AFRICA
Ida Manyina Munsense¹ and Joyce M Tsoka-Gwegweni¹˒²
- Department of Public Health Medicine, School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
- Office of the Dean, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Munsense, IM. and Tsoka-Gwegweni, JM., 2025. KNOWLEDGE, ATTITUDES, AND PERCEPTIONS OF TRAVELLERS TOWARDS CROSS-BORDER MALARIA PREVENTION MEASURES IN KWAZULU-NATAL, SOUTH AFRICA. Medical Research Archives, [online] 13(4).
https://doi.org/10.18103/mra.v13i4.6347
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6347
ISSN 2375-1924
ABSTRACT
Background: Knowledge, attitudes, and perceptions of travellers could play a key role in preventing imported malaria in a country. It is believed that seeking pre-travel advice from health professionals could prevent diseases and improve travellers’ health. It is also reported that when travellers have sufficient knowledge of malaria, they will take the necessary precautions and adhere to preventive measures when traveling to endemic countries, and so are likely to minimize the chances of infections.
This study aimed to investigate the knowledge, attitudes, and perceptions of travellers towards cross-border malaria prevention measures in the KwaZulu-Natal province, South Africa.
Methods: A cross-sectional survey of 396 participants was conducted in 2019. The participants included all adults en route to Mozambique, Eswatini, and Zimbabwe recruited from a major taxi rank in KwaZulu-Natal province, South Africa. A structured questionnaire about knowledge, attitudes, and perceptions towards cross-border malaria prevention measures was administered.
Results: More than 90.9% of participants demonstrated a high level of knowledge about malaria transmission and prevention in general. This knowledge was mainly acquired through healthcare facilities. However, only 13.6% of participants adhered to the required preventive measures. Similarly, 72.8% of participants reported not being aware of any information about malaria preventive measures available at the borders.
Conclusion: The high level of knowledge about malaria transmission and prevention does not translate into positive attitudes and perceptions among cross-border travellers. Regular and active communication about the risk of malaria and the availability of cross-border malaria prevention measures is recommended. This approach will encourage travellers to use protection against malaria to prevent imported transmission.
1. Introduction
In 2022, the World Health Organization (WHO) estimated that there were 249 million cases of malaria worldwide. Of these, 233 million cases, or approximately 94%, occurred in the WHO African Region. An estimated 608,000 deaths were attributed to malaria globally. The African Region accounted for about 93.6% of all malaria cases and 95.4% of deaths worldwide, with 78.1% of the fatalities in this region being among children under 5 years old.¹ Although preventable, malaria is a major public health problem that exposes all categories of people at risk of being infected, including those who travel to high-risk areas without appropriate protection.² Cross-border movements from non-endemic malaria countries to endemic countries and high numbers of travellers, plus little use of malaria preventive measures, have contributed to the increased burden of imported malaria.³˒⁴
It is estimated that an average of 3.5 million travellers from different countries move across the South African (SA) borders during the summer season for various reasons. Consequently, these cross-border movements have an impact on communicable diseases, especially malaria.⁵ In SA, malaria is endemic in three provinces, namely KwaZulu-Natal (KZN), Mpumalanga, and Limpopo.⁶
South Africa is currently in a malaria elimination phase, intending to reach elimination by 2030.⁷ However, the biggest challenge to elimination efforts in SA has been imported malaria.⁸
Although KZN has reassuringly shown a significant decline in the number of cases compared to the other two endemic provinces, it has been found that the number of imported malaria cases is usually higher than local cases in KZN.⁹
It is reported that travellers’ knowledge, attitudes, and perceptions play a key role in preventing imported malaria in a country. It is believed that travellers who have sufficient knowledge of malaria will take the necessary precautions and adhere to preventive measures when traveling to endemic countries so that they are likely to avoid infections.¹⁰
Evidence has shown that a high level of knowledge about the causes, transmission, and prevention of malaria was detected among the community members in Shewa Robit Town in Ethiopia. However, a considerable proportion of the community members had misconceptions about the causes and transmission of malaria, suggesting the necessity of health education to raise the community’s awareness about the disease.¹¹ This study suggests that knowing about malaria and preventive measures is not enough and that one needs to make use of the information received to ensure well-being.
This was confirmed by previous studies conducted among travellers in Dubai, Hong Kong, Egypt, Boston, USA,¹² and the UK,¹⁵ which all suggest that there are educational needs for travellers heading to malaria-endemic countries in terms of the uptake of preventive measures and current efforts to improve health-seeking behavior. A critical survey of data collected during the period 1999–2000 among the member sites of the TropNet Europe Network shows that only 60.4% of European travellers compared to 77.2% of immigrant travellers used malaria chemoprophylaxis, and that only a minority of patients took drugs or drug-combinations appropriate for the drug resistance situation of the malaria parasite at the respective destinations.¹⁶
A cross-sectional survey carried out with employees of 20 randomly selected companies in the Jebel Ali Free Zone, north of Dubai, revealed low awareness of pre-travel health advice as reflected by the low uptake of specialist travel medical advice on travel vaccinations and malaria prophylaxis. This survey highlighted an important educational need for Dubai travellers.¹⁷ A study conducted at Johannesburg International Airport found that most travellers perceived that they had been exposed to high-risk areas during their travel without carrying antimalarial medication, whilst some were carrying inappropriate medications.¹⁸ This study also recommended the need to improve the knowledge, attitudes, and practices of travellers.
While KZN and SA as a whole experience high volumes of travellers from malaria-endemic countries, limited research has been done concerning the knowledge, attitudes, and perceptions of travellers towards cross-border malaria preventive measures. Therefore, the present study investigated the knowledge, attitudes, and perceptions of travellers crossing South African borders in the KZN province by land towards cross-border malaria preventive measures. The intention was to recommend evidence-based solutions that could inform policymakers in implementing strategies to prevent imported malaria.
2. Methods and Materials
2.1 Study Design and Study Area
A descriptive cross-sectional survey was conducted in May 2019 at a major taxi rank for international travellers situated at the YMCA in the city of Durban, in the KZN province of SA.
2.2 Study Population and Sample
The study population included all adults aged 18 years and above, both male and female, willing to sign written informed consent forms to participate in the study and travelling to either Mozambique, Eswatini, or Zimbabwe. All South African and non-South African travellers recruited at the taxi rank and heading to these neighboring countries crossing KZN ports of entry were included in the study.
All travellers crossing KZN ports of entry but not willing to provide written informed consent to participate in the study, and those who did not meet the above criteria, were excluded. The sample size was estimated to be 400 participants, proportionally allocated between the three countries, using simple random sampling.
2.3 Data Collection
The survey was conducted using questionnaires to establish travellers’ knowledge, attitudes, and perceptions concerning cross-border malaria preventive measures. A pilot study was conducted to test the data collection tool in March 2019. The test highlighted the necessity of a bilingual questionnaire due to the language barrier faced by Mozambican travellers.
In the actual study, the data collection tool was translated into Portuguese to accommodate these travellers, while an English version was provided for those heading to Eswatini and Zimbabwe. The questionnaire was divided into four sections:
-
Demographic characteristics of the participants
-
Knowledge about malaria and preventive measures
-
Attitudes of travellers towards malaria prevention measures
-
Perceptions of travellers towards cross-border malaria preventive measures
A Portuguese-speaking research assistant assisted with the data collection. Once the questionnaire was filled in, it was checked for completion and clarified when needed.
Ethical clearance for the study was obtained from the Biomedical Research Ethics Committee of the University of KZN (Reference No: BE382/18). Permission to access participants was sought from the taxi rank manager.
2.4 Data Analysis
Data was collected and entered into a Microsoft Excel Version 16 spreadsheet. The data was then processed and analyzed using R Statistical Computing Software, Version 3.6.3.
Descriptive analysis was used to detail the demographic characteristics of the participants, their knowledge about cross-border malaria prevention measures, and their attitudes and perceptions towards those measures. The data is presented using frequency distribution tables.
Chi-squared test was used to examine the association between variables. Categorical explanatory variables were cross-tabulated against dichotomous outcome measures of knowledge, attitudes, and perceptions. The statistical significance level was set at p < 0.05.
3. Results
3.1 Description of Study Participants
The demographic characteristics of the participants are shown in Table 1. In total, 396 participants were included, giving a response rate of 99%, with each country (Eswatini, Mozambique, and Zimbabwe) having a nearly equal proportion of travellers (130, 32.8%; 133, 33.6%; and 133, 33.6%, respectively).
The majority of the participants were female (212, 53.5%) in the age ranges of 18–35 years (248, 62.6%), followed by 36–50 years (123, 31.1%). Very few participants were South African citizens (36, 9.1%), and the rest were equally divided between citizens of the above three countries, with a slightly higher number being citizens of Zimbabwe (136, 34.3%).
A small proportion of the participants were citizens of other African countries or outside the African continent. Most participants (210, 53%) reported having achieved secondary and tertiary (146, 36.9%) levels of education.
Similarly, a high proportion of the participants (182, 46%) said that they were employed, and the main reason for travelling was a visit (266, 67.2%) to the countries for less than one month.
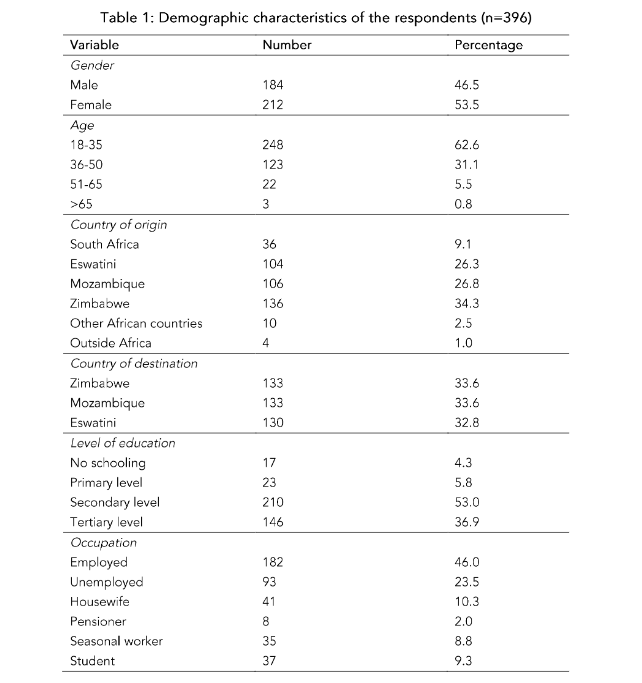
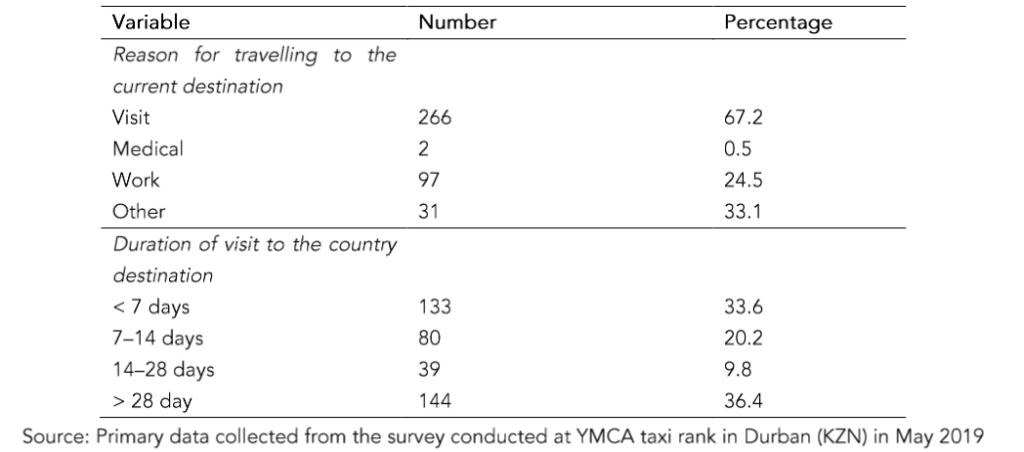
Table 1: Demographic characteristics of the respondents (n=396).
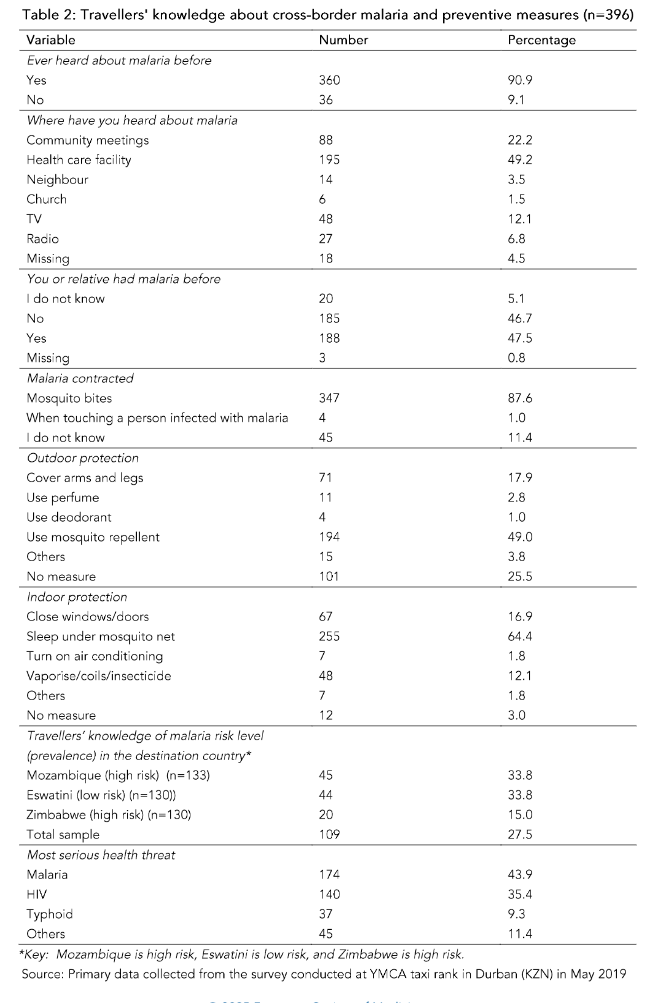
3.2 Knowledge of Travelers About Cross-Border Malaria Preventive Measures
Regarding the knowledge of travellers about cross-border malaria and its preventive measures, as presented in Table 2, a significant majority of participants (360, 90.9%) reported having heard about malaria before. The primary sources of information about malaria were health facilities, cited by 195 participants (49.2%), and community meetings, mentioned by 88 participants (22.2%). A small number of participants acquired information from alternative sources such as TV, radio, or church.
When asked about their personal or familial history of malaria, a considerable proportion of participants (188, 47.5%) confirmed that they or their relatives had previously contracted malaria. Furthermore, a significant majority of participants (347, 87.6%) correctly recognized that malaria is transmitted through mosquito bites.
In terms of protective measures, nearly half of the participants (194, 49.0%) correctly identified mosquito repellent as an outdoor protection method. Similarly, a substantial number of participants (255, 64.4%) correctly identified a mosquito net as an indoor protective measure.
When asked about the level of malaria risk in their destination country, only a small proportion of participants demonstrated knowledge about the risk level, particularly those traveling to Zimbabwe, with only 20 participants (15%) having awareness of the risk level. Regarding the perceived most serious health threat in their destination country, the majority of participants identified malaria as the primary concern (174, 43.9%), followed by HIV (140, 35.4%).
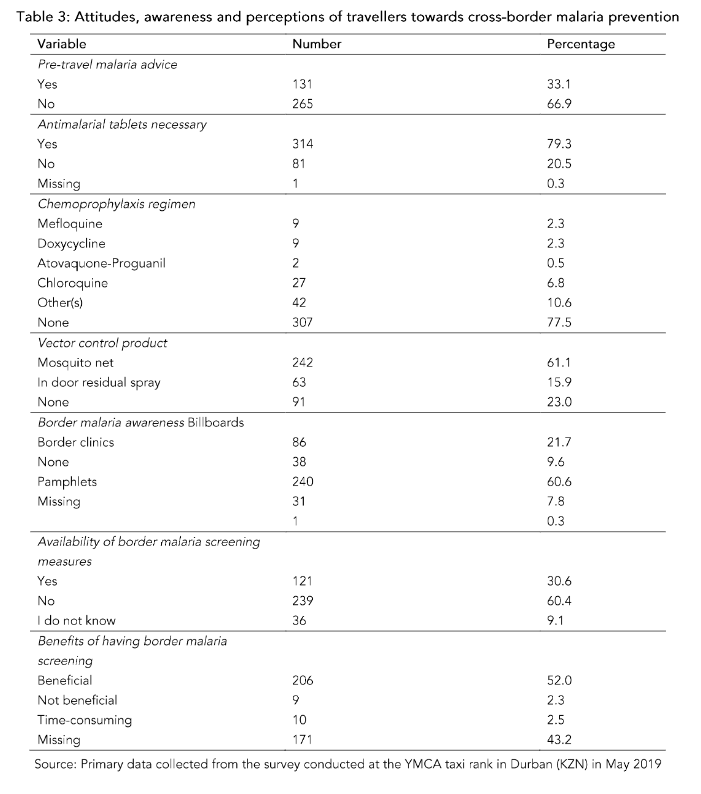
3.3 Attitudes, Awareness, and Perceptions of Travelers Toward Cross-Border Malaria Prevention
Regarding the attitudes of travellers towards malaria preventive measures, as depicted in Table 3, 265 (66.9%) reported not seeking pre-travel health advice. Interestingly, even though 314 participants (79.3%) acknowledged the necessity of taking antimalarial medication before traveling, the majority 307 (77.5%) stated that they did not have any antimalarial regimen.
In terms of the availability of vector control products at home, 242 participants (61.1%) reported having mosquito nets in their homes, while 255 (64.4%) indicated the use of indoor residual spray. However, 91 (23%) reported not possessing any of these vector control products at home.
Regarding malaria awareness at the border post, most participants 240 (60.6%) stated that there were no measures in place to create awareness about malaria at the border. Furthermore, a significant number of participants, 239 (60.4%), reported the absence of malaria screening at the border. However, it is noteworthy that 206 participants (52%) expressed their belief that implementing malaria screening at the border would be beneficial.
3.3 Attitudes, Awareness and Perceptions Towards Cross-Border Malaria Prevention
Table 3 illustrates the attitudes of participants towards cross-border malaria prevention measures.
3.4 Factors Associated with Knowledge, Attitudes, and Perceptions of Travelers About Cross-Border Malaria Prevention Measures
Table 4 presents the factors associated with the knowledge of travellers about cross-border malaria and preventive measures. Five factors were found to be statistically significantly associated with knowledge about malaria prevention measures: the participants’ education level (p = 0.028), the primary source of information regarding malaria (p = 0.001), transmission methods of malaria (p = 0.001), personal or familial history of malaria infection (p = 0.001) and awareness of indoor protection against malaria (p = 0.001).
On the other hand, certain factors such as gender, age, country of origin, occupation, the reason for travel, duration of visit, outdoor protection measures, risk level, and the most serious health threat in the destination country did not exhibit any statistically significant associations with knowledge about malaria.
KNOWLEDGE, ATTITUDES, AND PERCEPTIONS OF TRAVELLERS TOWARDS CROSS-BORDER MALARIA
threat in the destination country did not exhibit any statistically significant associations with knowledge about malaria.
Table 4 shows the results of the factors associated with the knowledge of travellers regarding cross-border malaria preventive measures.
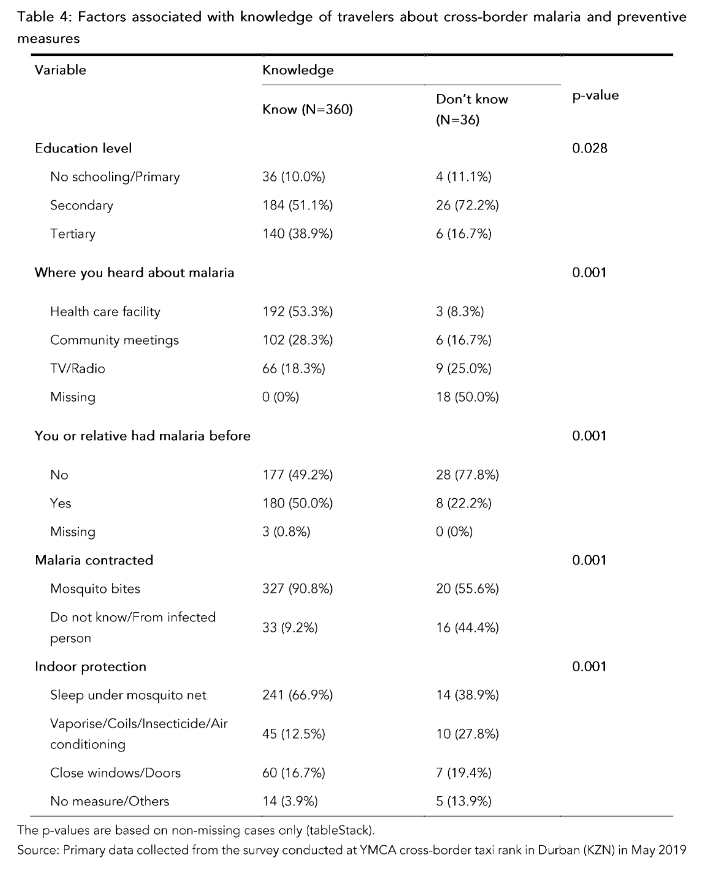
Table 5 shows the results of the factors that were statistically associated with the attitudes of travellers towards cross-border malaria preventive measures. These factors included the destination country (p = 0.033), seeking pre-travel malaria advice (p = 0.004), adherence to a chemoprophylaxis regimen (p = 0.035), and the use of a vector control product (p = 0.014).
Among participants, negative attitudes towards malaria preventive measures were observed in those who primarily travelled to Eswatini and Zimbabwe. These individuals were less likely to seek pre-travel malaria advice and did not adhere to a chemoprophylaxis regimen.Conversely, participants who utilized a vector control product displayed notably positive attitudes towards malaria prevention.However, factors such as gender, age, education level, occupation, travel reason, and duration of the visit were not statistically significantly associated with attitudes towards cross-border malaria preventive measures.3.5 Factors Associated with Attitudes of Travellers Towards Cross-Border Malaria Preventive Measures
Table 5 presents the factors associated with the attitudes of travellers towards cross-border malaria preventive measures.
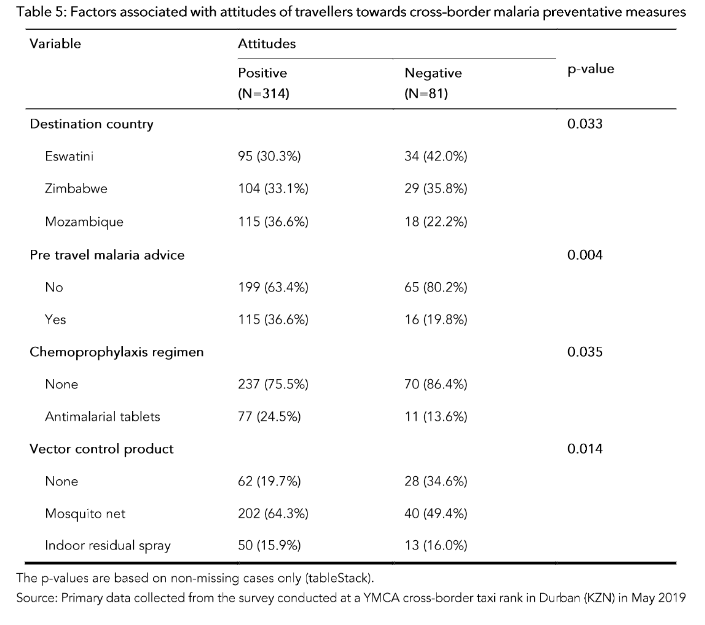
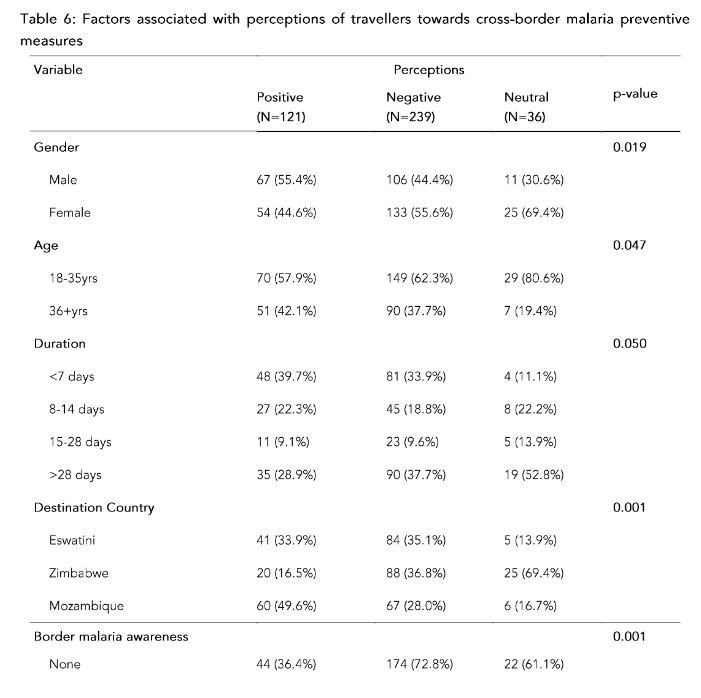
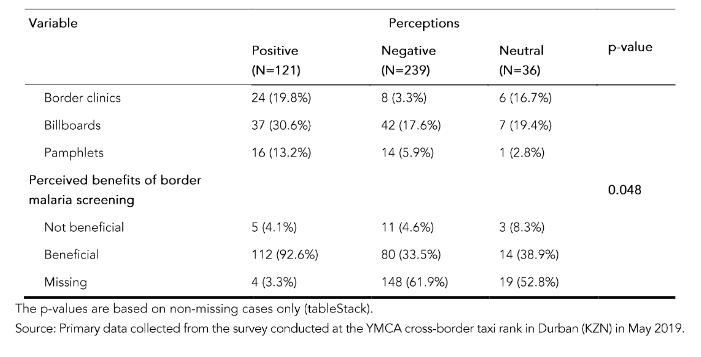
Table 6 presents the factors associated with the perceptions of travellers regarding cross-border malaria preventive measures. Perceptions, gender (p = 0.019), country of destination (p = 0.001), border malaria awareness (p = 0.001), and perceived benefits of malaria screening (p = 0.048).
Males tended to display more positive perceptions, whereas females tended to have negative or neutral perceptions. Furthermore, negative or neutral perceptions were observed among participants aged 18–35 years, those traveling to Eswatini or Zimbabwe, those with a visit duration exceeding 28 days, and those lacking awareness of border malaria screening programs.
In contrast, participants who acknowledged the potential benefits of a border malaria screening program expressed highly positive perceptions. These results indicate that gender plays a role in shaping travellers’ perceptions, with males exhibiting more positive attitudes.
Additionally, specific characteristics such as age, destination country, duration of visit, and awareness of border malaria screening programs influence individuals’ perceptions of cross-border malaria preventive measures.
Furthermore, participants who recognized the advantages of implementing a border malaria screening program exhibited notably positive perceptions.
4. Discussion
The results of the present study reveal that most of the travellers were employed; this agrees with the previous research that suggests that neighboring countries perceived SA as a land of work opportunities where they could go to work and visit their families back home regularly.²¹˒²² This situation underscores the importance of family traditions, shared memories, and values, demonstrating that distance cannot diminish these bonds. However, while this practice strengthens familial ties, it poses challenges for malaria control efforts in SA, especially considering the high prevalence of malaria in neighboring countries.²³
The results on the knowledge of travellers regarding cross-border malaria preventive measures indicate a relatively high level of awareness about malaria, its transmission through mosquito bites, and the importance of using protective measures such as mosquito repellents and mosquito nets. However, there is a need to improve the knowledge regarding the risk levels of malaria in different destinations and to address other significant health threats in travellers’ destination countries, such as HIV. The findings show that travellers generally had good knowledge about malaria, its transmission mode, and the protective measures for indoor protection. This concurs with the study conducted in Shewa Robit Town, North-Eastern Ethiopia, which found that most of the population had good knowledge about malaria, the mode of transmission, and preventive measures.¹¹ This is also similar to a study conducted in the UK among those traveling to malaria-endemic countries.¹⁵
The health facility was the most common source of information about malaria. These results also support studies conducted at the Dutch Schipol Airport² and Johannesburg Airport.¹⁸ Very few participants identified television and radio as their primary sources of information. To address this gap, it is crucial to promote these traditional media channels for disseminating health-related information, as they have the potential to reach a wider audience. Most households are equipped with televisions and radios, making it common for people to tune in for daily news updates.¹⁸
In contrast, a growing majority of the population now turns to the Internet and social media for information, which offers a vast array of content that significantly raises health awareness.²⁴ These digital platforms expose a larger number of individuals to health information compared to those who rely solely on the insights provided at health facilities or during community meetings. This reliance on social media creates an opportunity to reach diverse audiences beyond the more specialized gatherings, which often cater to a limited group of people.
Of greatest concern is the participants’ poor knowledge about malaria risk levels in the country of destination, particularly among those who were bound for Zimbabwe, which is categorized among high-risk malaria areas.²⁵ In addition, not all travellers in the present study considered malaria as the most serious health threat. This finding could be linked to the fact that in some countries like SA, HIV/AIDS is regarded as a national health priority, ranked among the top causes of death, rather than malaria. As a result, most of the health promotion messages, research funding, and interventions are directed towards reducing the burden of HIV/AIDS.²⁶
An analysis of the factors associated with knowledge about malaria preventive measures revealed that knowledge was associated with educational level, source of information about malaria, participants’ or relatives’ history of contracting malaria, knowledge about how malaria is contracted, and knowledge of indoor protection. These factors are similar to what was reported in other studies.²⁷
The data presented in Table 3 provide insights into the attitudes and behaviors of travellers towards malaria preventive measures. The findings indicate a need for increased awareness and adherence to pre-travel health advice, antimalarial regimens, and the utilization of vector control products. The present study found that the participants had mostly negative attitudes concerning the uptake of malaria preventive measures and poor health-seeking behavior. This is demonstrated by the participants’ acknowledgment of the necessity to take anti-malarial tablets while traveling to endemic countries, but not carrying any or seeking pre-travel medical advice.
This finding agrees with studies among travellers in Dubai, which suggest a need for education concerning preventive measures for travellers,¹⁷ but is contrary to a survey done in Schiphol airport, where health-seeking behavior was dependent on the category of travellers. In that study, most of the travellers traveling for business, leisure, and work sought medical advice before traveling, whilst those visiting family and friends did not.²
Similar to the present study, inadequate pre-travel health preparations were found among Hong Kong travellers. The underestimation of malaria risks was a significant barrier to adequate pre-travel health preparations. The study suggested targeted health education and information about risk to improve the levels of travel health preparedness.¹²
The reasons for non-adherence among travellers in Boston included forgetfulness, fear of side effects, peer advice, and not physically seeing mosquitoes.¹⁴ In Johannesburg, some travellers claimed to know what to do, whilst others did not realize they should seek pre-travel advice.¹⁸
The negative attitudes found in the present study could be linked to poor knowledge about the risk level of malaria in the country of destination and the seriousness of malaria as a health threat. The attitudes of participants towards malaria preventive measures were associated with the country of destination, seeking pre-travel malaria advice, chemoprophylaxis regimen, and use of vector control products.
The attitudes of travellers in this study towards malaria preventive measures raise concerns. Most travellers at the taxi rank are from sub-Saharan Africa, where malaria is endemic. They have routinely been exposed to malaria infection as a result. However, they do not perceive it as a risk.
Studies have found that natural immunity develops slowly after many years of exposure; sterile protection is never achieved.²⁸ This means that even though the travellers have developed immunity due to exposure, it does not protect them against malaria infection when travelling to other endemic areas.
They may be asymptomatic, but they are carriers of parasites in their blood that would almost certainly be deadly to non-immune travellers if not detected on time.²⁹ Travellers’ acquired immunity creates reluctance and is perceived as protection against future exposure to malaria infection. Instead, this should act as a wake-up call for them to embrace possible preventive measures against contracting malaria when travelling to an endemic country, because immunity does not mean exemption from malaria infection.
The results concerning malaria awareness and screening at the border underscore a critical gap that necessitates the implementation of effective measures aimed at enhancing malaria prevention strategies for travellers. This study reveals a significant lack of understanding surrounding cross-border malaria prevention among individuals crossing into neighboring regions. Many travellers expressed limited awareness regarding the existence or importance of a malaria screening program in the border areas of KZN. This is in contrast to the views of border authorities who reported that there are cross-border malaria prevention measures.²⁷
Despite this lack of awareness, participants were open to the idea that the introduction of a dedicated border malaria screening program could provide valuable benefits, suggesting a willingness to engage with such initiatives. The participants’ perceptions were shaped by various factors, including age, gender, the country they were traveling to, the duration of their stay, their familiarity with any screening programs, and their views on the potential advantages of such measures.
Notably, the data regarding age and gender support previous studies that indicate younger adults and males represent the most frequent cross-border travellers. This demographic trend underscores the importance of tailoring malaria prevention strategies to engage these groups effectively and raise their awareness about the risks of malaria when traveling across borders.³⁰˒³¹
The authors acknowledge that the study was conducted just before the COVID-19 pandemic and that vigilance and strategies to prevent importation of infectious diseases may have intensified.³² The authors believe that cross-border measures to prevent malaria might have been negatively impacted during the COVID-19 era as resources were shifted, health services reformed, and new priorities set to fight the pandemic.
Current evidence indicates that redirecting resources towards reducing the burden of COVID-19 has resulted in the disruption of malaria control activities, with increased risk and burden of malaria in endemic countries of the Southern African community.³²˒³³ During the COVID-19 pandemic, health education and awareness campaigns have increased significantly, far exceeding efforts for malaria. Communities have engaged more in sharing important information about preventing the virus, getting vaccinated, and practicing hygiene through social media and public workshops.
This shows how important it is for the public to understand COVID-19.¹⁹ Meanwhile, malaria awareness efforts continue but do not receive as much attention, reflecting a change in public health priorities during the COVID-19 crisis.³⁴
It is essential to raise health awareness about malaria, especially in areas near countries where malaria is common. We can learn from the COVID-19 pandemic, where effective communication about malaria prevention happened during that time in Rwanda and Cambodia.³² Education campaigns should explain the life cycle of the malaria parasite, its symptoms, and the benefits of using insecticide-treated mosquito nets.
Communities should be encouraged to seek medical help quickly if they experience symptoms like fever or chills. By using engaging stories and visuals, we can help people understand better and motivate them to take preventive measures, ultimately lowering the number of malaria cases in vulnerable border regions.
5. Study Limitations
The first limitation of this study revolves around the decision to collect data from a single location, the bustling YMCA taxi rank in Durban. This choice was primarily driven by financial constraints, which restricted the researchers from including other potential sites such as bus stations and airports.
Expanding the study to these diverse locations would have enriched the data by providing varied insights into travel destinations and creating a broader spectrum of travellers’ profiles.
Despite this limitation, the YMCA taxi rank serves as an essential hub, recognized as the largest point of departure for travellers heading to Mozambique, Eswatini, and Zimbabwe. Its strategic location makes it highly accessible and convenient for most people departing from the KZN province. However, the fast-paced nature of transportation at this site presents
challenges. Buses headed to these neighboring countries seldom linger at the rank, leaving little time for the researcher to administer their questionnaires effectively. Moreover, the environment at the bus station is far from conducive to conducting detailed research. The constant influx of travellers creates a lack of privacy, making it difficult for participants to engage openly in the study without distractions. Compounding this issue are the overwhelming noise levels generated by the buses and the countless conversations among travellers, which further complicate the ability to gather accurate and focused responses.
Another significant limitation is the exclusion of participants who utilize informal or illegal border crossings. These routes have been identified as major threats to malaria elimination efforts in KZN.³⁴ Recruiting participants from these areas poses unique challenges, as individuals crossing through illegal borders may fear the repercussions of revealing personal information, which include the risk of arrest or denial of entry into their desired province or country.
6. Conclusions and Recommendations
Malaria remains a significant health threat in Africa, with many travellers exhibiting negative attitudes towards preventive measures. This non-compliance often leads to inadequate health-seeking behavior in the face of malaria risks. Knowledge of cross-border malaria prevention is alarmingly low, highlighting the urgent need for targeted education.
Travellers should be informed about standard precautions, such as using insect repellent and sleeping under treated bed nets, and strategies specific to border crossings that can reduce transmission risk. A comprehensive risk management plan is essential to provide accessible information to travellers as they cross borders into and out of SA.
Raising awareness about cross-border malaria measures requires collaboration among health, transport, port health, and communication ministries, using various media platforms for effective information dissemination. Awareness campaigns can include posters at taxi ranks, health workshops at transport hubs, and proactive screening initiatives.
Enhancing public awareness and promoting universal health coverage can protect communities from imported malaria and prevent outbreaks in KZN and throughout SA. Further research on health education and malaria prevention at key border points is essential, along with improved communication among stakeholders to control the spread of the disease.
7. Conflict of Interest
The authors declare no competing interests.
8. Authors’ Contributions
I.M.M. and J.M.T-G conceptualised the study.
I.M.M. collected and processed the data.
I.M.M. and J.M.T-G carried out the analyses and interpretation of the results.
I.M.M. wrote the first draft of the manuscript.
J.M.T-G supervised the study, reviewed the paper, and contributed to the original manuscript.
9. Acknowledgement
The College of Health Sciences, the University of KwaZulu-Natal, for providing a scholarship. The authors also express gratitude to the Biostatistician for assistance with data analysis, the research assistant, and all research participants for availing themselves for this research.
The College of Health Sciences, the University of KwaZulu-Natal, for providing a scholarship. The authors also express gratitude to the Biostatistician for assistance with data analysis, the research assistant, and all research participants for availing themselves for this research.
References
1. Venkatesan P. The 2023 WHO World malaria report. The Lancet Microbe. 2024;5(3):e214.
2. Van Genderen et al. Trends in the knowledge, attitudes, and practices of travel risk groups towards prevention of malaria: results from the Dutch Schiphol Airport Survey 2002 to 2009. Malaria Journal. 2012; (11):179.
3. Al Zahrani MH, Omar AI, Abdoon AM, et al. Cross-border movement, economic development, and malaria elimination in the Kingdom of Saudi Arabia. BMC Medicine. 2018;16(1):98.
4. Wangdi K, Gatton ML, Kelly GC, Clements AC. Cross-border malaria: a major obstacle for malaria elimination. Advances in parasitology. Elsevier; 2015:79-107.
5. Malaria elimination strategic plan for South Africa 2019-2023 (2019).
6. Govere J, Durrheim D, la Grange K, Mabuza A, Booman M. Community Knowledge and Perceptions about Malaria and Practices influencing Malaria control in Mpumalanga Province, South Africa. South African Medical Journal. 2000; (90) 611-16.
7. Sikaala CH, Dlamini B, Lungu A, et al. Malaria elimination and the need for intensive inter-country cooperation: a critical evaluation of regional technical co-operation in Southern Africa. Malaria Journal. 2024;23(1):62.
8. Raman J, Morris N, Frean J, et al. Reviewing South Africa’s malaria elimination strategy (2012–2018): progress, challenges and priorities. Malaria journal. 2016;15(1):438.
9. Maharaj R, Seocharan I, Qwabe B, Mkhabela M, Kissoon S, Lakan V. Decadal epidemiology of malaria in KwaZulu-Natal, a province in South Africa targeting elimination. Malaria journal. 2019; 18(1):368.
10. Brunette GW. CDC Yellow Book 2018: health information for international travel. Oxford University Press; 2017.
11. Abate A, Degarege A, Erko B. Community
knowledge, attitude and practice about malaria in a low endemic setting of Shewa Robit Town, northeastern Ethiopia. BMC public health. 2013; 13(1):312.
12. Kevin K C Hung AKYL, Calvin K Y Cheng, Emily Y Y Chan, Colin A Graham. Pre-travel health preparation for malaria prevention among Hong Kong travellers Postgrad Med J. 2015; 91:127–131.
13. El-Ghitany EM, Abdelmohsen M, Farghaly AG, El-Gawwad A, El-Wahab A, Wassim E. Travel health survey: Risk perception, health-seeking behavior, and subjective evaluation of travel health services in Egypt. International Journal of Travel Medicine and Global Health. 2018;6(1):16-24.
14. Rhett J. Stoney LHC, Emily S. Jentes, Mary E. Wilson, Pauline V. Han, Christine M. Benoit, William B. MacLeod, Davidson H. Hamer, Elizabeth D. Barnett. Malaria Prevention Strategies: Adherence among Boston Area Travellers Visiting Malaria-Endemic Countries. American Society of Tropical Medicine and Hygiene. 2016;94(1):136–142.
15. Behrens RH, Alexander N. Malaria knowledge and utilization of chemoprophylaxis in the UK population and in UK passengers departing to malaria-endemic areas. Malaria journal. 2013;12 (1):461.
16. Odolini S, Gautret P, Parola P. Epidemiology of imported malaria in the Mediterranean region. 2012;4(1):1-8.
17. Fatima Omer NH, Hussain H, Sami Mana, Omer Awad Travel Health, Gaps in Knowledge, Attitudes, and Practices Among Dubai Travellers, Dubai, UAE International Journal of Preventive Medicine Research 2015; (1). 2015:126-131.
18. Toovey S, Jamieson A, Holloway M. Travelers’ knowledge, attitudes and practices on the prevention of infectious diseases: results from a study at Johannesburg International Airport. Journal of Travel Medicine. 2004;11(1):16-22.
19. Silal SP, Little F, Barnes KI, White LJ. Predicting the impact of border control on malaria transmission: a simulated focal screen and treat campaign. Malaria Journal. 2015: (14):1-14.
20. Toovey S. Malaria chemoprophylaxis advice: survey of South African community pharmacists’ knowledge and practices. Journal of travel medicine. 2006;13(3):161-165.
21. Byass P, Collinson MA, Kabudula C, et al. The long road to elimination: malaria mortality in a South African population cohort over 21 years. Global health, epidemiology and genomics. 2017:(2)1-10.
22. Raman J, Gast L, Balawanth R, et al. High levels of imported asymptomatic malaria but limited local transmission in KwaZulu-Natal, a South African malaria-endemic province nearing malaria elimination. Malaria journal. 2020;19:1-13.
23. Li J, Docile HJ, Fisher D, Pronyuk K, Zhao L. Current status of malaria control and elimination in Africa: epidemiology, diagnosis, treatment, progress and challenges. Journal of Epidemiology and Global Health. 2024;14(3):561-579.
24. AlMuammar SA, Noorsaeed AS, Alafif RA, Kamal YF, Daghistani GM. The use of internet and social media for health information and its consequences among the population in Saudi Arabia. Cureus. 2021;13(9):1-12.
25. Mundagowa PT, Chimberengwa PT. Malaria outbreak investigation in a rural area south of Zimbabwe: a case–control study. Malaria journal. 2020;19:1-10.
26. Mayosi BM, Lawn JE, Van Niekerk A, et al. Health in South Africa: changes and challenges since 2009. The Lancet. 2012;380(9858):2029-2043.
27. Fitchett JM, Swatton D-A. Exploring public awareness of the current and future malaria risk zones in South Africa under climate change: a pilot study. International Journal of Biometeorology. 2020:1-11.
28. Barry A, Hansen D. Naturally acquired immunity to malaria. Parasitology. 2016;143(2):12 5-128.
29. Sturrock HJ, Hsiang MS, Cohen JM, et al. Targeting asymptomatic malaria infections: active surveillance in control and elimination. PLoS medicine. 2013;10(6):1-8.
30. Benetsky MJ, Burd CA, Rapino MA. Young Adult Migration: 2007-2009 to 2010-2012. 2015:1-28.
31. Adeola AM, Botai OJ, Olwoch JM, et al. Environmental factors and population at risk of malaria in Nkomazi municipality, South Africa. Tropical Medicine & International Health: TM & IH. 2016;21(5):675-686.
32. Kleinhans I, Mahanjana S, Els F, et al. The prevalence and distribution of malaria in Mpumalanga Province before and during COVID-19 (2017-2022). South African Medical Journal. 2024;114(8):29-36.
33. Maharaj R, Ward A, Didier B, et al. The effect of the COVID-19 lockdown on malaria transmission in South Africa. Malaria journal. 2023;22(1):1-8.
34. Munsense IM, Tsoka-Gwegweni JM. Perceived health system challenges of implementing cross-border Malaria preventive measures at ports of entry in KwaZulu-Natal. Annals of Global Health. 2023;89(1):1-15.