





Sleep Disorders in Epileptic Children on Valproate Therapy
Sleep disorders in children with epilepsy receiving valproate therapy
Riya Shah¹, Anju Aggarwal¹*, Manish Narang¹, Sangeeta Sharma², Rajeev Malhotra³
- Department of Pediatrics, University College of Medical Sciences and Guru Teg Bahadur Hospital, New Delhi
- Department of Neuropsychopharmacology, Institute of Human Behaviour and Allied Sciences, Delhi.
- Department of Statistics, Delhi Cancer Registry, Dr. BRAIRCH, AIIMS, New Delhi.
*E mail: [email protected]
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Shah, R., Aggarwal, A., et al., 2024. Sleep disorders in children with epilepsy receiving valproate therapy. Medical Research Archives, [online] 13(1).
https://doi.org/10.18103/mra.v13i1.6094
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6094
ISSN 2375-1924
ABSTRACT
Objective: To assess prevalence of sleep disorders in children with epilepsy who have received at least 6 months of valproate using validated sleep questionnaires.
Study design: Cross-sectional study.
Methods: Developmentally normal children with epilepsy aged 4-12 years who received at least 6 months of valproate monotherapy were evaluated. Of these 30 were evaluated from initiation of therapy to six months. A validated questionnaire, Pediatric sleep questionnaire (PSQ) was used to record information. Sleep Related Breathing Disorder (SRBD) scale was extracted from PSQ (score of >0.33 was significant). Sleep Disturbance Scale for Children (SDSC) was also used to record information (T-score >70 was significant). These were administered in RS language which the parent understood.
Results: Fifty two children (30 males, 22 females) with epilepsy were enrolled. Of them 7(13.5%) children had sleep breathing disorders by SRBD. On using SDSC, 17.3% of children had sleep disorders. Out of the 6 subscales, Sleep-wake transition disorders (SWTD) was seen in 32.7%. Disorders of excessive somnolence (DOES) (23.1%), 15.4% had disorders of initiating and maintaining sleep (DIMS). Disorders of arousal (DA) were seen in 11.5%, sleep hyperhidrosis (SHY) in 7.7%, and 5.8% had sleep breathing disorders (SBD). There was no effect of age, sex, seizure type and valproate dose on sleep disorders (P>0.05). Among 30 children followed up from start of therapy to 6 months 5(16.7%) developed sleep breathing disorders using SRBD scale and 4 (13.3%) using SDSC.
Conclusion: Sleep disorders are prevalent in children with epilepsy receiving valproate therapy which need attention and appropriate management.
Keywords: valproate therapy, sleep disorders, Epilepsy.
Introduction
Epilepsy is a common pediatric illness with cumulative lifetime incidence of 3% more then half of which start in childhood¹. Sleep is highly complex brain generated behaviour. It is a reversible behavioural state of perceptual disengagement from and unresponsiveness to the environment². Sleep disorders are present in about 25% of normal children³. Sleep disorders effect quality of life of the child and family. Problems may vary from daytime sleepiness to headache, behavioural problems, poor school performance and mood disturbances.
Sleep and epilepsy are two well recognized conditions that interact with each other in a complex bi-directional way. One third of epileptic patients have seizures during the sleep. On the other hand, sleep disorders are more prevalent in epileptic children⁴. Some types of epilepsies have increased activity during sleep disturbing it; while sleep deprivation aggravates epilepsy due to decreased seizure threshold. This means that epilepsy disturbs sleep and sleep deprivation aggravates epilepsy due to the decrease in seizure threshold thus forming a vicious cycle⁵.
The epilepsy may affect all sleep parameters and can induce sleep fragmentation, parasomnias, and day time drowsiness. This can result in memory dysfunction, impairment of daytime functioning, and quality of life. The patients may experience daytime tiredness and impaired attention and arousal for years without knowing the reasons⁶.
The sleep disturbances occurring in epileptic children may be in part of the effect of drugs used to treat epilepsy. Valproate which is used as a drug of choice for most of the seizure types is known to cause sleep disturbance. It may increase stage 1 sleep and may worsen obstructive sleep apnea⁷. There are only a few studies on childhood epilepsy and sleep disorders⁸,⁹. Thus, we aim to assess the sleep disorders in epilepsy children on valproate therapy.
Methods
This cross-sectional study was conducted in a tertiary care hospital. An approval from the institutional ethics committee was obtained. Sample size was calculated by Stat Calc Module of Epi Info 7.2.6. Expected frequency was 26% from a study by Roshan S et al⁸. If percentage margin of error is 12%, The Sample size came out to be 51 (for a confidence limit of 95%).
Subjects included consisted of developmentally normal children in 4-12 years of age presenting with generalized seizure or focal motor seizure diagnosed with epilepsy who had received at least 6 months of valproate monotherapy. Children on other anti-epileptic drugs were excluded. Hospital protocol for seizure management was followed. 30 cases were enrolled from beginning of therapy to six months. Sleep disorders were assessed at beginning of therapy and at 6 months in these. Cases with 2nd episode of generalized seizure and 1st episode of focal motor seizure were enrolled. Children were investigated to find out the etiology of epilepsy. A hemogram, liver function tests, kidney function tests, Blood Sugar, lipid levels, chest X- ray and mantoux test were done as indicated. Neuroimaging and EEG were done.
Valproate was prescribed at a dose of 10mg/kg, increased upto 20mg/kg within a week and was continued in the form of tablet or syrup. Albendazole at 15mg/kg/day for 21 days was prescribed in case of NCC or antitubercular drugs for 9 months in case of tuberculoma. In case of repeat seizure, valproate dose was increased and maximum upto 40mg/kg. If seizures remained uncontrolled, another AED were added and the case was excluded.
Developmentally normal patients who had received at least 6 months of valproate monotherapy were enrolled. Patients demographic and clinical details were noted as per performa. Serum valproate levels were done at the time of recruitment in these and at 6 months in those enrolled since beginning. About 3 ml of venous blood sample was collected before the first morning dose, about 12 hours after administration of last dose. Valproate levels were estimated with auto analyzer using enzyme immunoassay system (CEDIA® Valproic acid II assay).
Sensitivity – The minimum detectable concentration for assay was 3.0 mcg/ml and Specificity – Measurement of various antiepileptic drug levels resulted in ≤10% cross reactivity in the presence of other drugs or anti-epileptics at the levels tested. Normal Valproate level was 50-100mg/dl as per laboratories standards.
PEDIATRIC SLEEP QUESTIONNAIRE (PSQ)
A pediatric sleep questionnaire (PSQ) is a multipage questionnaire which consists of closed questions and several open questions on sleep disorder symptoms¹⁰. It was translated into Hindi with permission and when we translated back to English, it remained the same. It has 2 subcomponents – (a) Sleep related breathing disorders (SRBD) scale and (b) PLM/RLS scale.
SRBD scale consists of 22 closed response questions extracted from PSQ and validated against polysomnography and multiple sleep latency tests. The questionnaire was one page questionnaire. We used Hindi version of questionnaire with permission. The answers of questions on SRBD scale was in form of yes/no/don’t know (yes=1, no=2, don’t know=3). SRBD scale score calculated by number of items answered yes divided by number of items answered yes and no. So denominator includes number of items answered yes/no but not includes missing/don’t know. The result is a proportion that range from 0 to 1 and if score ≥ 0.33 is considered positive and suggestive of high risk for a pediatric sleep related breathing disorder. Cut off of SRBD scale score based on validity data suggestive of optimal sensitivity and specificity at this level (≥0.33)¹¹.
SLEEP DISTURBANCE SCALE FOR CHILDREN (SDSC)
To investigate the sleep-wake pattern and occurrence of sleep disorders in previous 6 months we used a questionnaire – sleep disturbance scale for children (SDSC). SDSC was developed by Bruni O et al in 1996 to evaluate sleep disturbances in childhood and adolescence. The internal consistency was high in controls (0.79) and remained at a satisfactory level in sleep disorder subjects (0.71); the test/retest reliability was adequate for the total (r = 0.71) and single item scores¹².
It was retrospective questionnaire and filled by parents/guardians. It consists of 26 questions/items to evaluate sleep in children, each item had score from one to five (1=never, 5=always). The total score varies between 26 and 130. T-score is given on basis of total score (range 38 to 100). Sleep disturbance scale for children provide overall SDSC total score and 6 subscale score to identify sleep disorders like – Disorder of initiating and maintaining sleep (DIMS), sleep breathing disorder (SBD), disorder of arousal (DA), sleep-wake transition disorder (SWTD), disorder of excessive somnolence (DOES) and sleep hyperhidrosis (SHY). To determine the prevalence of sleep disorders, total score and various subscale scores on SDSC were dichotomized as abnormal or normal on basis of T-score >70 and ≤70 respectively. We also determined the prevalence of sleep disorders by taking abnormal pathological T score ≥50 as in studies by Di Pisa V et al¹³ and Cordts KMP et al¹⁴.
Statistical analysis: Prevalence of sleep disorders was calculated by percentage of children with SDSC T-score>70 after at least 6 months of valproate therapy. 6 subscales of SDSC were assessed similarly. Percentage of children with SRBD score>0.33 were also assessed to calculate prevalence. Effects of clinical and demographic profile on the scores were determined by chi-square test for qualitative data and unpaired t-test for quantitative data. Scores in these scales before and after 6 months of valproate therapy were compared by McNemar test in 30 patients.
Results
A total of 52 patients with epilepsy who had received at least 6 months of valproate monotherapy were enrolled with age ranging from 4-12 years (mean 7.98±2.6 years) out of which 57.7% were male and 42.3% were female.
Table 1 shows that 33(63.5%) patients had generalized seizure and 19(36.5%) had focal seizures. Out of 33 patients of generalized seizures 9 had generalized tonic seizures, 19 had impaired awareness, 10 had focal seizures with generalized tonic clonic seizures and 5 had generalized atonic seizures. Out of 19 patients of focal seizures, 3 had focal seizures without impaired awareness and 6 had focal seizures with secondary generalization.
| Seizure Character | Number | ||
|---|---|---|---|
| Seizure type | Generalized | 33 | 63.5% |
| Focal | 19 | 36.5% | |
| Area | Present | 18 | 34.6% |
| Absent | 34 | 65.4% | |
| Duration | < 5 min | 17 | 32.7% |
| > 5 min | 34 | 67.3% | |
| Postictal Drowsiness | Present | 40 | 76.9% |
| Absent | 12 | 23.1% | |
| Sleep Disturbance | Present | 15 | 28.8% |
In our study, 38(73.1%) patients had normal CT/MRI findings while 9(17.3%) had neurocysticercosis and 4(7.7%) had tuberculoma in neuroimaging. One patient had a finding of asymmetry of ventricles. In our study, 19(36.5%) electroencephalogram were done out of which 13(25%) were abnormal.
Table 2 & Fig. 1 shows that 7(13.5%) patients had a significant T-score of >0.33 which implies that 13.5% patients had sleep breathing disorders
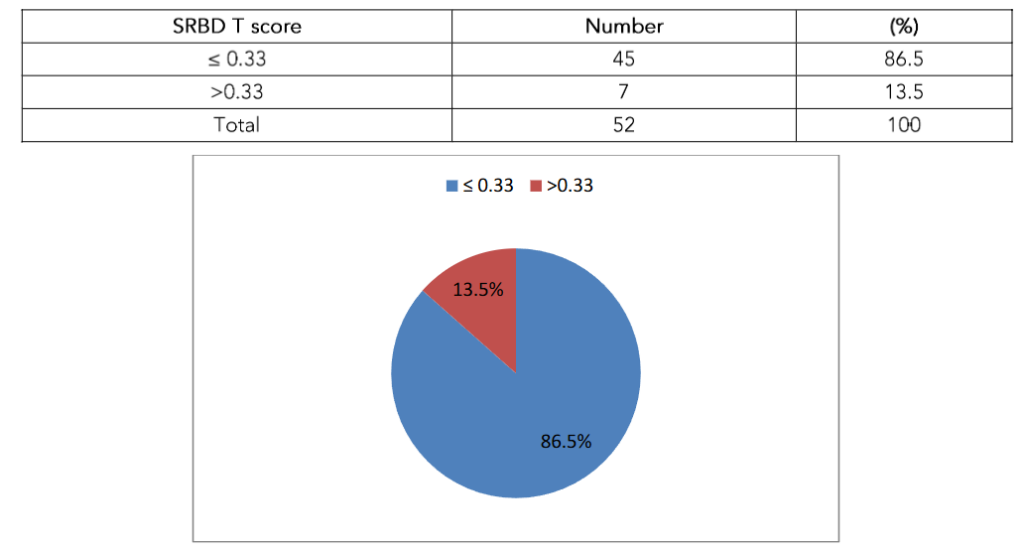
Fig. 1: Pie chart showing SRBD T-score distribution of study subjects
Table 3 & Fig. 2 shows that sleep disorders were present in 17.3% of the patients when sleep disturbance scale for children was used with T-score cutoff >70. Out of the 6 subscales, Sleep-wake transition disorders (SWTD) were most common. Out of 52, 17 (32.7%) had score more than 70 in sleep-wake transition disorders subscale. Disorders of excessive somnolence (DOES) stands second most common. 12 (23.1%) subjects had a score more than 70 in disorders of excessive sleepiness subscale. In our study, we found that 8 (15.4%) suffered from disorders of initiating and maintaining sleep (DIMS). Disorders of arousal (DA) were seen in 6 (11.5%) study subjects. Out of 52, 7.7% study subjects suffered from sleep hyperhidrosis (SHY) and 5.8% suffered from sleep breathing disorders (SBD). When prevalence of sleep disorders is low by cut off 70, T-score of 50 can be taken as cut off as done in previous study by Di Pisa V et al¹³ and Cordts KMP et al¹⁴. When T score of >50 was used, sleep disturbances were seen in 71.2% children. We found that most frequent sleep disorders were sleep-wake transition disorders (65.4%), followed by disorders of excessive somnolence (59.6%) and sleep hyperhidrosis. Sleep breathing disorders and Disorders of arousal were seen in 32.7% of the subjects. We found that 25% of the patients had disorders of initiating and maintaining sleep.
Table 3 Sleep Disturbance Scale for Children (SDSC) T-score of study subjects
SDSC T-score | Number(n) | (%)
DIMS
≤70 | 44 | 84.6
70 | 8 | 15.4
SBD
≤70 | 49 | 94.2
70 | 3 | 5.8
DA
≤70 | 46 | 88.5
70 | 6 | 11.5
SWTD
≤70 | 35 | 67.3
70 | 17 | 32.7
DOES
≤70 | 40 | 76.9
70 | 12 | 23.1
SHY
≤70 | 48 | 92.3
70 | 4 | 7.7
SDSC Total
≤70 | 43 | 82.7
70 | 9 | 17.3
DIMS (disorder of initiating and maintaining sleep), SBD (sleep breathing disorder), DA (disorder of arousal), SWTD (sleep wake transition disorder), DOES (disorder of excessive somnolence) and SHY (sleep hyperhidrosis).
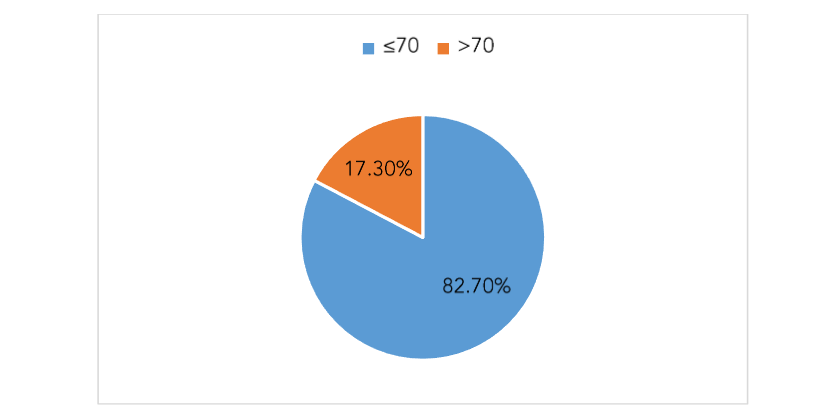
Fig. 2: Pie chart showing SDSC T-score distribution of study subjects
Table 4 shows that no clinical parameter like age, sex, parents’ education, or weight had any effect on sleep disorders. Neither seizure characteristics had any effect on sleep disorders when SDSC score was used. Similarly, when SRBD scale was used, no correlation was found between clinical parameters and seizure characteristics with sleep disorders (P>0.05).
Table 4 Effect of clinical parameters on Sleep Disturbance Scale for Children (SDSC) T-score >70
Parameters | ≤70 | >70 | p-value
Age (years)
4–6 | 14 | 1
7–9 | 14 | 3
10–12 | 15 | 5 | 0.383
Sex
Male | 24 | 6
Female | 19 | 3 | 0.717
Address
Delhi | 32 | 8
Outside Delhi | 11 | 1 | 0.436
Mother’s Education
Illiterate/Primary | 18 | 0
Middle/High School | 20 | 8
Graduate/Postgraduate | 5 | 1 | 0.030
Father’s Education
Illiterate/Primary | 12 | 1
Middle/High School | 22 | 5
Graduate/Postgraduate | 9 | 3 | 0.495
Birth Asphyxia
Present | 2 | 0
Absent | 41 | 9 | 1.000
Weight for Age Z score
Between +2 to -3 | 38 | 9
Less than -3 | 5 | 0 | 0.573
Total | 43 | 9
P value <0.05 by Pearson chi-square
We had 30 children who were recruited from beginning of valproate therapy. They were administered these questionnaires at the beginning of therapy as well as at 6 months of valproate therapy. The number of children with sleep disorders at beginning of therapy and at 6 months is shown in Tables. In Sleep Related Breathing Disorder (SRBD) scale, at the initiation of valproate therapy, no patient had a T-score of >0.33 but after 6 months of valproate therapy, 5 patients developed a T-score of >0.33. This implies that 5 out of 30 patients suffered from sleep breathing disorders after at least 6 months of valproate therapy.
Table 5 Evaluation with SDSC T-score with 50 as cut off
T-score (At initiation of valproate therapy) | T-score (after 6 months of valproate therapy) | p-value
>50 ≤50
Total SDSC
50 | 6 | 2
≤50 | 14 | 8 | 0.004
DIMS
50 | 1 | 2
≤50 | 7 | 20 | 0.180
SBD
50 | 3 | 2
≤50 | 8 | 17 | 0.109
DA
50 | 7 | 4
≤50 | 3 | 16 | 1.000
SWTD
50 | 11 | 4
≤50 | 8 | 7 | 0.388
DOES
50 | 1 | 0
≤50 | 13 | 16 | 0.000
SHY
50 | 14 | 2
≤50 | 2 | 12 | 1.000
DIMS (disorder of initiating and maintaining sleep), SBD (sleep breathing disorder), DA (disorder of arousal), SWTD (sleep wake transition disorder), DOES (disorder of excessive somnolence) and SHY (sleep hyperhidrosis). Significant p-value <0.05 by McNemar test.
In Sleep Disturbance Scale for Children (SDSC), at the initiation of valproate therapy, no patient had a T-score of >70, but after 6 months of valproate therapy, 4 patients developed an SDSC T-score of >70 implying the presence of sleep disorders in patients receiving valproate therapy. There was significant change in number of children with overall sleep disorders at 6 months of valproate therapy compared to baseline, based on SDSC T-score cut off 50 (table 5). Among the subscales significant change in numbers was seen in disorder of excessive somnolence (P<0.05).
Discussion
This study was done to assess the sleep disorders in children with epilepsy on valproate therapy by using validated sleep questionnaires. We enrolled 52 patients of epilepsy who had received at least 6 months of valproate monotherapy. The age group varied from 4–12 years, out of which 30 were males
and 22 were females. In our study, we found that 13.5% children had sleep breathing disorders by Sleep Related Breathing Disorders (SRBD) scale. On using Sleep Disturbance Scale for Children (SDSC), 17.3% of children had sleep disorders.
Prevalence of sleep disorder in patients receiving valproate monotherapy was comparable to previous study by Legros B et al⁷ which assessed the effects of different antiepileptic drugs on sleep architecture in 39 adult patients with localization-related epilepsy. Patients with no AEDs were included as controls. Overnight polysomnography was recorded and was scored according to the standard method. According to the study, sleep disorders were seen in 16.8±9.8% of patients using valproate.
Another study by Cortesi et al¹⁵ from Rome 1999 assessed sleep problems and daytime behavior in childhood idiopathic epilepsy on valproate monotherapy. A Sleep Behaviour Questionnaire (SBQ) was used to assess problems in 89 children (6-14 years) with idiopathic epilepsy on valproate monotherapy (blood levels ranging from 80 to 100µg/ml) for comparison with 49 siblings and 321 healthy control children. Sleep disorders were found in 11.7% of the patients.
Sleep and epilepsy interact with each other in a very complex bi-directional manner. Some epilepsy have increased paroxysmal activity during sleep causing sleep disturbance which further aggravates epilepsy due to decreased seizure threshold. Sleep disorders are very common in patients with epilepsy. Seizures can decrease sleep efficiency and increasing periods of wakefulness in patients with generalized or focal epilepsy. Increased sleep fragmentation and instability can happen on seizure-free nights as well. Polysomnograph may reveal increase in sleep onset latency, increase in the wake time after sleep onset, increased instability of sleep stages, increased stage N1 and N2 NREM sleep (light sleep) and decrease in REM sleep in patients with epilepsy.
On the other hand, Epileptiform discharges can itself be activated or inhibited in different stages of sleep. Typically epileptiform discharges propagate during NREM sleep, as it is a more synchronized state. Generalized epileptiform discharges increase with deepening of NREM sleep. Most of the focal onset seizures occur in sleep. A vast majority of sleep-related seizures (82.4%, 76.5% asymptomatic) are followed by awakenings or arousals¹⁶. This leads to sleep disruption making them prone to suffer sleep disorders.
In our study, we used 2 questionnaires to assess the sleep disorders. Sleep Related Breathing Disorders (SRBD) scale. We could not find any literature on sleep disorders in children with epilepsy on valproate therapy using SRBD scale.
Other questionnaire which was used in our study was Sleep Disturbance Scale for Children (SDSC) to evaluate sleep disturbances in childhood. Children with SDSC T-score >70 have pathological sleep disorders. SDSC score has been translated in many languages and used multiple times to assess sleep disorders in children with epilepsy. A study by Zambrelli E et al¹⁷ studied sleep disturbances in Italian children and adolescents with epilepsy by Sleep Disturbances Scale for Children (SDSC) and Child Behavior Checklist (CBCL) in 84 patients aged between 6 and 17 years old. An abnormal total sleep score was found in 23.8% subjects with epilepsy compared with 4.4% of control group (P < 0.001). 48 patients (57.1%) had an abnormal score in at least one SDSC factor: disorders in initiating and maintaining sleep (DIMS; 13.1%), sleep breathing disorders (SBD; 13.1%), disorders of arousal (DA; 5.9%), sleep-wake transition disorders (SWTD; 15.5%), disorders of excessive somnolence (DOES; 20.2%), and sleep hyperhidrosis (SHY; 5.9%). In our study, the most common sleep disorder was Sleep-wake transition disorders (SWTD; 32.7%), followed by Disorders of excessive somnolence (DOES; 23.1%).
Present study highlights the prevalence of sleep disorders in 4-12 year children receiving valproate monotherapy for focal motor and generalized epilepsy for at least 6 months. Sleep disorders were seen in 13.5% according to SRBD scale and in 17.3% according to SDSC scale. Age sex, type
of seizure, etiology, parents education or valproate dose did not affect the sleep disorders (p >0.05). Counselling and management of sleep disorders becomes very important in such children to ensure compliance and to improve the quality of life.
Conclusion
Valproate therapy for epilepsy in child has detrimental effect on sleep. Hence sleep related issues need to be addressed to for better epilepsy control and quality of life. Further studies with different epilepsy types, different antiseizure medication and varied durations of therapy are required for conclusive results and guidelines.
Funding Statement:
None.
Acknowledgments:
None.
Contributions:
RS and AA conceptualized the idea. RS collected data in supervision of AA and MN. RS, AA, MN, RM were involved in protocol, review of the manuscript.
Conflict of Interest:
None.
References
1. Mikati MA, Hani AJ. Seizures in childhood. In: Kliegman RH, Stanton BF, Geme JW< Schor NF. Eds. Nelson’s Textbook of Pediatrics,20th ed. Elsevier.2016:2823-2858.
2. Carskadon MA, Dement WC. Normal human sleep: an overview. Principles and Practice of sleep medicine,2nd Ed, Philadelphia, PA:Saunders1994:16-26
3. Maski K, Owens JA. Insomnia, parasomnias, and narcolepsy in children: clinical features, diagnosis, and management. Lancet Neurol. 2016 Oct;15(11): 1170-81. doi: 10.1016/S1474-4422(16)30204-6. P MID: 27647645.
4. Wirrell E, Blackman M, Barlow K, Mah J, Hamiwka L. Sleep disturbances in children with epilepsy compared with their nearest-aged siblings. Dev Med Child Neurol. 2005 Nov;47(11):754-9. doi: 10.1017/S0012162205001581. PMID: 16225739.
5. Baxter P. Epilepsy and sleep. Dev Med Child Neurol. 2005 Nov;47(11):723. doi: 10.1017/S0012 162205001519. PMID: 16225732.
6. Bazil CW. Epilepsy and sleep disturbance. Epilepsy Behav. 2003 Oct;4 Suppl 2:S39-45. doi: 10.1016/j.yebeh.2003.07.005. PMID: 14527482.
7. Legros B, Bazil CW. Effects of antiepileptic drugs on sleep architecture: a pilot study. Sleep Med. 2003 Jan;4(1):51-5. doi: 10.1016/s1389-9457(02)0 0217-4. PMID: 14592360.
8. Roshan S, Puri V, Chaudhry N, Gupta A, Rabi SK. Sleep abnormalities in juvenile myoclonic epilepsy-A sleep questionnaire and polysomnography based study. Seizure. 2017 Aug;50:194-201. doi: 10.1016/j.seizure.2017.06.021. Epub 2017 Jun 28. PMID: 28704743.
9. Krishnan P, Sinha S, Taly AB, Ramachandraiah CT, Rao S, Satishchandra P. Sleep disturbances in juvenile myoclonic epilepsy: a sleep questionnaire-based study. Epilepsy Behav. 2012 Mar;23(3):305-9. doi: 10.1016/j.yebeh.2011.12.018. Epub 2012 Feb 25. PMID: 22366052.
10. Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000 Feb 1;1(1):21-32. doi: 10.1016/s 1389-9457(99)00009-x. PMID: 10733617.
11. Sleep-Related Breathing Disorder Scale (SRBD Scale), from Pediatric Sleep Questionnaire, to Identify Symptoms of Obstructive Sleep Apnea in Children. Available from: http://inventions.umich.edu/technologies/3773/sleep-related-breathing-disorder-scale-srbd-scale-from-pediatric-sleep-questionnaire-to-identify-symptoms-of-obstructive-sleep-apnea-in-children. Assessed on 24th Aug2019
12. Bruni O, Ottaviano S, Guidetti V, Romoli M, Innocenzi M, Cortesi F, Giannotti F. The Sleep Disturbance Scale for Children (SDSC). Construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J Sleep Res. 1996 Dec;5(4):251-61. doi: 10.1111/j.13 65-2869.1996.00251.x. PMID: 9065877
13. Pisa V, Provini F, Ubertiello S, Bonetti S, Ricci E, Ivanovski I, Caraffi SG, Giordano L, Accorsi P, Savasta S, Raviglione F, Boni A, Grioni D, Graziano C, Garavelli L, Cordelli DM. Sleep in Mowat-Wilson Syndrome: a clinical and video-polysomnographic study. Sleep Med. 2019 Sep;61:44-51. doi: 10.1016/j.sleep.2019.04.011. Epub 2019 Apr 26. PMID: 31285160.
14. Poppert Cordts KM, Hall TA, Hartman ME, Luther M, Wagner A, Piantino J, Guilliams KP, Guerriero RM, Jara J, Williams CN. Sleep Measure Validation in a Pediatric Neurocritical Care Acquired Brain Injury Population. Neurocrit Care. 2020 Aug;33(1):196-206. doi: 10.1007/s12028-019 -00883-5. PMID: 31797275; PMCID: PMC7266703.
15. Cortesi F, Giannotti F, Ottaviano S. Sleep problems and daytime behavior in childhood idiopathic epilepsy. Epilepsia. 1999 Nov;40(11):1 557-65. doi: 10.1111/j.1528-1157.1999.tb02040.x. PMID: 10565583.
16. Peter-Derex L, Klimes P, Latreille V, Bouhadoun S, Dubeau F, Frauscher B. Sleep Disruption in Epilepsy: Ictal and Interictal Epileptic Activity Matter. Ann Neurol. 2020 Nov;88(5):907-920. doi: 10.1002/ana .25884. Epub 2020 Sep 21. PMID: 32833279.
17. Zambrelli E, Turner K, Vignoli A, La Briola F, Dionisio S, Malanchini S, Galli F, Canevini MP. Sleep disturbances in Italian children and adolescents with epilepsy: A questionnaire study. Epilepsy Behav. 2020 May;106:107014. doi: 10.1016/j.yebeh.2020. 107014. Epub 2020 Mar 28. PMID: 32229412.