

Infectious Diseases and Global Instability: A Study
The Association between Infectious Diseases, Mental Impairments, Violent Behavior, and Global Instability
Robert C Bransfield, MD, DLFAPA¹²
- Hackensack Meridian School of Medicine, Nutley, NJ 07110, USA.
- Rutgers-Robert Wood Johnson Medical School, Piscataway, NJ 08854, USA.
https://orcid.org/0000-0002-9326-6478
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Bransfield, RC., 2025. The Association between Infectious Diseases, Mental Impairments, Violent Behavior, and Global Instability. Medical Research Archives, [online] 13(1).
https://doi.org/10.18103/mra.v13i1.6178
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6178
ISSN 2375-1924
ABSTRACT
It is necessary to better understand and prevent all contributors to violence. A 2017 hypothesis stated—if a pandemic causing mental impairments increasing the risk of violence occurred, it could contribute to global instability. The association between infectious disease, mental impairments, violence, and global instability has never been adequately researched. A review is performed to evaluate all the facets of this possible association.
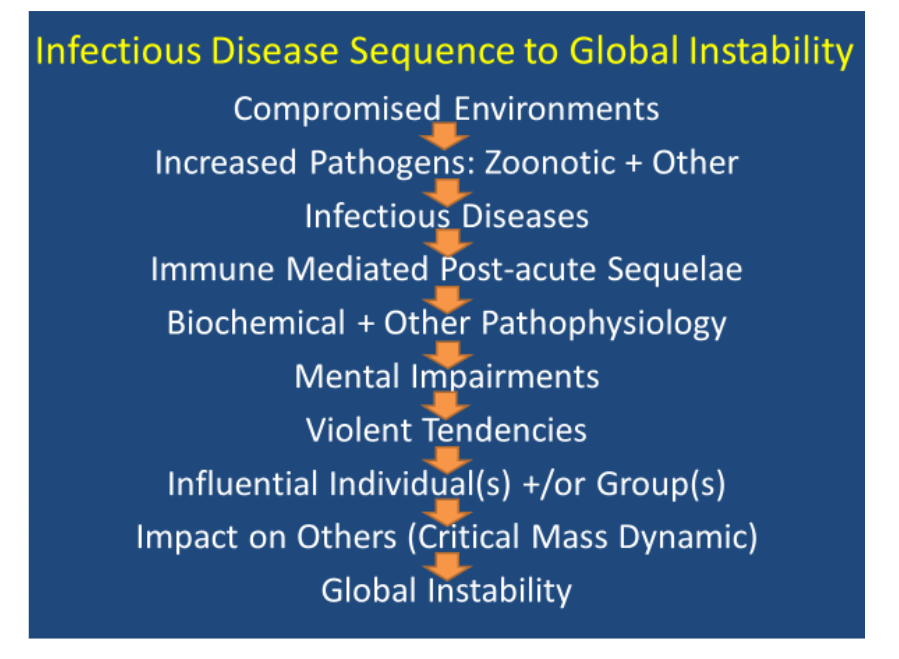
A sequence of events contributes to the association between infectious diseases and global instability. Degraded environments are conducive to emerging and expanding infectious diseases. Infections can alter brain functioning by immune system mediated and other pathophysiological mechanism that can increase the risk of mental impairments contributing to mental illnesses and/or violent behavior. Parasites, particularly zoonotic and vector-borne, sometimes manipulate their host in a manner that propagates their survival (Manipulation Hypothesis). Through this, or other pathophysiology, infectious diseases can contribute to violent behavior in both animals and humans. When influential individuals or groups of influential individuals acquire infectious diseases that contribute to violent tendencies, it can have greater societal and global impact (critical mass dynamic). Infectious diseases are not equally distributed throughout the world. Countries and geographic areas with greater infections and vector-borne zoonotic disease burdens correlate with a higher prevalence of violence. In a global community, this can contribute to global instability.
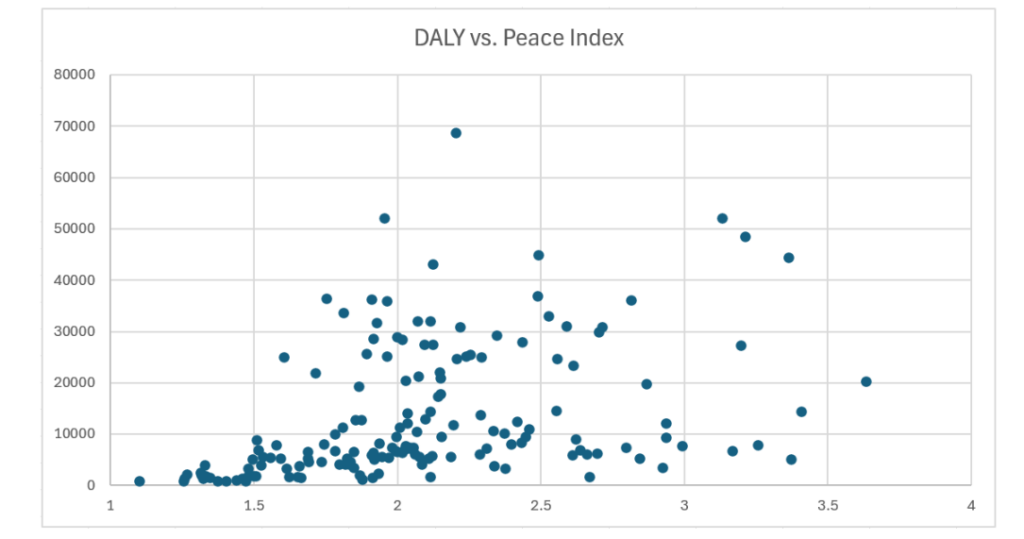
Impairments from the SARS-CoV-2 pandemic are associated with an increased risk of mental impairments and violent behavior. Global violence and instability have increased following the pandemic based upon changes in the Global Peace Index.
Although the data reviewed has limitations, evidence suggests infectious diseases, including the recent SARS-CoV-2 pandemic, may contribute to mental impairments with resultant increased risk of violence and global instability. A collaborative One Health research and intervention approach can help prevent violence both regionally and globally.
Keywords: Afghanistan, Borrelia, COVID, Iceland, Lyme disease, Malaria, One Health, Peace, Relapsing Fever Borrelia, SARS-CoV-2, Syphilis, Violence, War
References
1. Bransfield RC. Could a Pandemic Causing Mental Dysfunction Contribute to Global Instability? Paper presented at: International Lyme and Associated Diseases 7th European Conference; May 19, 2017; Paris, France.
2. Institute for Economics & Peace. Global Peace Index: Global peace deteriorates as violence costs world $19.1 trillion in 2023. 11 June 2024 Available online: https://efe.com/en/portada-america/2024-06-11/global-peace-deteriorates-as-violence-costs-world-19-1-trillion-in-2023/#:~:text=Global%20Peace%20Index:%20Violence%20Costs,trillion%20in%202023%20%2D%20EFE%20Noticias&text=The%20economic%20impact%20of%20violence,No%20Sales (Accessed 21 October 2024.)
3. Bransfield RC. Aggressiveness, violence, homicidality, homicide, and Lyme disease. Neuropsychiatr Dis Treat. 2018;14:693-713. doi: 10.2147/NDT.S155143.
4. Fazel S, Philipson J, Gardiner L, Merritt R, Grann M. Neurological disorders and violence: a systematic review and meta-analysis with a focus on epilepsy and traumatic brain injury. J Neurol. 2009;256(10):1591-602. doi: 10.1007/s00415-009-5134-2.
5. Elliott FA. Violence: The Neurologic Contribution: An Overview. Arch Neurol. 1992;49 (6):595–603. doi:10.1001/archneur.1992.0053030 0027006.
6. Lewis DO, Pincus JH, Feldman M, Jackson L, Bard B. Psychiatric, neurological, and psychoeducational characteristics of 15 death row inmates in the United States. Am J Psychiatry. 1986;143(7):838-45. doi: 10.1176/ajp.143.7.838.
7. Feldman M, Mallouh K, Lewis DO. Filicidal abuse in the histories of 15 condemned murderers. Bull Am Acad Psychiatry Law. 1986;14(4):345–352.
8. Blomström Å, Kosidou K, Kristiansson M, Masterman T. Infection during childhood and the risk of violent criminal behavior in adulthood. Brain Behav Immun. 2020;86:63-71. doi: 10.1016/j.bbi.2 019.02.026.
9. Bransfield RC, Mao C, Greenberg R. Microbes and Mental Illness: Past, Present, and Future. Healthcare (Basel). 2023;12(1):83. doi: 10.3390/healthcare12010083.
10. Vision of Humanity. Overall GPI Score. Available online:
https://www.visionofhumanity.org/maps/#/ (Accessed 24 October 2024).
11. IHME, Global Burden of Disease (2024) – with minor processing by Our World in Data. “DALY rates from communicable, neonatal, maternal & nutritional diseases” [dataset]. IHME, Global Burden of Disease, “Global Burden of Disease – Deaths and DALYs” [original data]. Available online: https://ourworldindata.org/grapher/burden-of-disease-rates-from-communicable-neonatal-maternal-nutritional-diseases (Accessed 26 October 2024).
12. Mahon MB, Sack A, Aleuy OA, et al. A meta-analysis on global change drivers and the risk of infectious disease. Nature. 2024;629, 830–836. https://doi.org/10.1038/s41586-024-07380-6.
13. Kilpatrick AM, Randolph SE. Drivers, dynamics, and control of emerging vector-borne zoonotic diseases. Lancet. 2012;380(9857):1946-55. doi: 10.1016/S0140-6736(12)61151-9.
14. Feinmann J. Analysis reveals global post-covid surge in infectious diseases. BMJ. 2024;385: q1348. doi: 10.1136/bmj.q1348.
15. Rana MS, Usman M, Alam MM, et al. Changes in the prevalence of infectious diseases before and after the COVID-19 pandemic in Pakistan. J Infect. 2023;86(4):415-416. doi: 10.1016/j.jinf.2023.01.020.
16. Rubin R. Syphilis Has Surged for Reasons That Go Beyond the Pathogen That Causes It. JAMA. 2024;332(2):92–95. doi:10.1001/jama.2024.2978.
17. Haider N, Rothman-Ostrow P, Osman AY et al. COVID-19-Zoonosis or Emerging Infectious Disease? Front Public Health. 2020;8:596944. doi: 10.3389/fpubh.2020.596944.
18. Esposito MM, Turku S, Lehrfield L, Shoman A. The Impact of Human Activities on Zoonotic Infection Transmissions. Animals (Basel). 2023;13 (10):1646. doi: 10.3390/ani13101646.
19. WHO. Vector-borne diseases. 26 September 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/vector-borne-diseases (Accessed 26 October 2024).
20. Thompson A. Plants Are the World’s Dominant Life-Form. Scientific American. 1 August 2018. Available online:
https://www.scientificamerican.com/article/plants-are-the-worlds-dominant-life-form/ (Accessed 25 October 2024).
21. Ihara F, Nishimura M, Muroi Y, et al. Toxoplasma gondii Infection in Mice Impairs Long-Term Fear Memory Consolidation through Dysfunction of the Cortex and Amygdala. Infect Immun. 2016; 84(10):2861-70. doi: 10.1128/IAI.00217-16.
22. Alvarado-Esquivel C, Estrada-Martínez S, Ramos-Nevárez A, et al. Is Toxoplasma gondii Infection Associated with Sexual Promiscuity? A Cross-Sectional Study. Pathogens. 2021;10(11): 1393. doi:10.3390/pathogens10111393.
23. Jackson AC. Diabolical effects of rabies encephalitis. J Neurovirol. 2016;22(1):8-13.
doi: 10.1007/s13365-015-0351-1.
24. Flegr J. Influence of latent Toxoplasma infection on human personality, physiology and morphology: pros and cons of the Toxoplasma-human model in studying the manipulation hypothesis. J Exp Biol. 2013;216(Pt 1):127-33. doi: 10.1242/je b.073635.
25. Steffen HM. Wie beeinflussen Parasiten das Verhalten ihres Wirts? Die parasitäre Manipulations hypothese [Behavioural Changes Caused by Parasites: The Parasite Manipulation Hypothesis]. Dtsch Med Wochenschr. 2020;145(25):1848-1854. German. doi: 10.1055/a-1220-8737.
26. Poulin R. Parasite manipulation of host behavior: an update and frequently asked questions. Adv. Study Behav. 2010;41:151–186. doi: 10.101 6/S0065-3454(10)41005-0.
27. Moore J. An overview of parasite-induced behavioral alterations—and some lessons from bats. J Exp Biol. 2013;216:11–17. doi: 10.1242/je b.074088.
28. Hart BL. Behavioural defences in animals against pathogens and parasites: parallels with the pillars of medicine in humans. Phil Trans R Soc. 2011;B 366:3406–3417. doi: 10.1098/rstb.2011.0092.
29. Klein SL. Parasite manipulation of the proximate mechanisms that mediate social behavior in vertebrates. Physiol Behav. 2003;79:441–449. doi: 10.1016/S0031-9384(03)00163-X).
30. Poulin R. ‘Adaptive’ changes in the behaviour of parasitized animals: a critical review. Int J Parasitol. 1995;25:1371–1383. doi: 10.1016/0 020-7519(95)00100-X).
31. Ashby B, Boots M. Coevolution of parasite virulence and host mating strategies. Proc Natl Acad Sci. USA. 2015;112, 13 290–13 295. doi: 10.1073/p nas.1508397112.
32. Natarajan D, Caramaschi D. Animal violence demystified. Front Behav Neurosci. 2010;4:9. doi: 10.3389/fnbeh.2010.00009.
33. Raihani NJ, Bell V. An evolutionary perspective on paranoia. Nat Hum Behav. 2019;3(2):114-121. doi: 10.1038/s41562-018-0495-0.
34. Bransfield RC, Goud Gadila SK, Kursawe LJ, Dwork AJ, Rosoklija G, Horn EJ, Cook MJ, Embers ME. Late-stage borreliosis and substance abuse. Heliyon. 2024;10(10):e31159. doi: 10.1016/j.heliyo n.2024.e31159.
35. Sariaslan A, Lichtenstein P, Larsson H, Fazel S. Triggers for violent criminality in patients with psychotic disorders. JAMA Psychiatry. 2016;73(8): 796–803.
36. Volavka J. Triggering violence in psychosis. JAMA Psychiatry. 2016;73(8):769–770.
37. Thornhill R, Fincher CL. Parasite stress promotes homicide and child maltreatment. Philos Trans R Soc Lond B Biol Sci. 2011;366(1583):3466–3477.
38. Lester D. Toxoplasma gondii and homicide. Psychol Rep. 2012;111(1):196–197.
39. Stahl SM, Morrissette DA, Munter N. Stahl’s Illustrated Violence. Cambridge UK: Cambridge University Press; 2014.
40. Stahl SM. Deconstructing violence as a medical syndrome: mapping psychotic, impulsive, and predatory subtypes to malfunctioning brain circuits. CNS Spectr. 2014;19(5):357–365.
41. Heath NM, Chesney SA, Gerhart JI, et al. Interpersonal violence, PTSD, and inflammation: potential psychogenic pathways to higher C-reactive protein levels. Cytokine. 2013;63(2):172–178.
42. Copeland WE, Wolke D, Lereya ST, Shanahan L, Worthman C, Costello EJ. Childhood bullying involvement predicts low-grade systemic inflammation into adulthood. Proc Natl Acad Sci U S A. 2014;111(21):7570–7575.
43. Bob P, Raboch J, Maes M, et al. Depression, traumatic stress and interleukin-6. J Affect Disord. 2010;120(1–3):231–234.
44. Heyes MP, Brew BJ, Martin A et al. Quinolinic acid in cerebrospinal fluid and serum in HIV-1 infection: relationship to clinical and neurological status. Ann Neurol. 1991;29(2):202-9. doi: 10.1002/ana.41029 0215.
45. Halperin JJ, Heyes MP. Neuroactive kynurenines in Lyme borreliosis. Neurology. 1992; 42(1):43-50. doi: 10.1212/wnl.42.1.43.
46. Hunt NH, Too LK, Khaw LT et al. The kynurenine pathway and parasitic infections that affect CNS function. Neuropharmacology. 2017; 112(Pt B):389-398. doi: 10.1016/j.neuropharm.201 6.02.029.
47. Huang YS, Ogbechi J, Clanchy FI, Williams RO, Stone TW. IDO and Kynurenine Metabolites in Peripheral and CNS Disorders. Front Immunol. 2020;11:388. doi: 10.3389/fimmu.2020.00388.
48. Bransfield RC. The psychoimmunology of Lyme/tick-borne diseases and its association with neuropsychiatric symptoms. Open Neurol J. 2012; 6:88–93.
49. Coccaro EF, Lee R, Coussons-Read M. Elevated Plasma Inflammatory Markers in Individuals with Intermittent Explosive Disorder and Correlation with Aggression in Humans. JAMA Psychiatry. 2014;71(2):158–165. doi:10.1001/jamapsychiatry.2013.3297
50. Shamay-Tsoory SG, Tomer R, Berger BD, Aharon-Peretz J. Characterization of empathy deficits following prefrontal brain damage: the role of the right ventromedial prefrontal cortex. J Cogn Neurosci. 2003;15(3):324–337.
51. Adolphs R, Tranel D, Damasio H, Damasio A. Impaired recognition of emotion in facial expressions following bilateral damage to the human amygdala. Nature. 1994;372(6507):669–672.
52. Adolphs R, Baron-Cohen S, Tranel D. Impaired recognition of social emotions following amygdala damage. J Cogn Neurosci. 2002;14(8):1264–1274.
53. Siever LJ. Neurobiology of aggression and violence. Am J Psychiatry. 2008;165(4):429–442.
54. Davidson RJ, Putnam KM, Larson CL. Dysfunction in the neural circuitry of emotion regulation – a possible prelude to violence. Science. 2000;289(5479):591–594.
55. Lane SD, Kjome KL, Moeller FG. Neuropsychiatry of aggression. Neurol Clin. 2011; 29(1):49-64, vii. doi: 10.1016/j.ncl.2010.10.006.
56. Hillis AE. Inability to empathize: brain lesions that disrupt sharing and understanding another’s emotions. Brain. 2014;137(Pt 4):981-97. doi: 10.10 93/brain/awt317.
57. Muzambi, R., Bhaskaran, K., Rentsch, C.T. et al. Are infections associated with cognitive decline and neuroimaging outcomes? A historical cohort study using data from the UK Biobank study linked to electronic health records. Transl Psychiatry. 2022;12;385. doi: 10.1038/s41398-022-02145-z.
58. Jaywant A, Gunning FM, Oberlin LE, et al. Cognitive Symptoms of Post–COVID-19 Condition and Daily Functioning. JAMA Netw Open. 2024; 7(2):e2356098. doi:10.1001/jamanetworkopen.2023.56098.
59. Hernandez-Ruiz V, Letenneur L, Fülöp T, Helmer C et al. Infectious diseases and cognition: do we have to worry? Neurol Sci. 2022;43(11):62 15-6224. doi: 10.1007/s10072-022-06280-9.
60. Reis PA, Castro-Faria-Neto HC. Systemic Response to Infection Induces Long-Term Cognitive Decline: Neuroinflammation and Oxidative Stress as Therapeutical Targets. Front Neurosci. 2022;15: 742158. doi: 10.3389/fnins.2021.742158.
61. Bransfield, R.C. Neuropsychiatric Lyme Borreliosis: An Overview with a Focus on a Specialty Psychiatrist’s Clinical Practice. Healthcare (Basel). 2018;6:104. doi: 10.3390/healthcare6030104.
62. Bransfield RC, Aidlen DM, Cook MJ, Javia S. A Clinical Diagnostic System for Late-Stage Neuropsychiatric Lyme Borreliosis Based upon an Analysis of 100 Patients. Healthcare (Basel). 2020;8 (1):13. doi: 10.3390/healthcare8010013.
63. Friedman KJ, Ruhoy IS, Fennell PA. The Possible Infectious Origins of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Fibromyalgia and Other Infectious Diseases Causing Cognitive Consequences’, in Hedges DW, Gale SD, Erickson LD (eds), Infectious Diseases in Neurocognitive and Neuropsychiatric Medicine. Oxford Academic, 24 Oct. 2024), doi:10.1093/oso/9780192870414.003.0001
64. Bantjes J, Rabie S, Almirol E et al. Associations between violence, criminality, and cognitive control deficits among young men living in low resource communities in South Africa. Aggress Behav. 2020; 46(1):5-15. doi: 10.1002/ab.21867.
65. Frisell T, Pawitan Y, Långström N. Is the association between general cognitive ability and violent crime caused by family-level confounders? PLoS One. 2012;7(7):e41783. doi: 10.1371/journa l.pone.0041783.
66. Wallinius M, Nordholm J, Wagnström F, Billstedt E. Cognitive functioning and aggressive antisocial behaviors in young violent offenders. Psychiatry Res. 2019;272:572-580. doi: 10.1016/j.p sychres.2018.12.140.
67. Liang CS, Bai YM, Hsu JW et al. The Risk of Sexually Transmitted Infections Following First-Episode Schizophrenia Among Adolescents and Young Adults: A Cohort Study of 220 545 Subjects. Schizophr Bull. 2020;46;795–803.
68. Saini HS, Sayre M, Saini I, Elsharkawy N. Neurosyphilis Presenting as Intermittent Explosive Disorder and Acute Psychosis. Cureus. 2019;11, e6337.
69. Taki El-Din Z, Iqbal H, Sharma A. Neurosyphilis-Induced Psychosis: A Unique Presentation of Syphilis with a Primary Psychiatric Manifestation. Cureus. 2023;15, e36080.
70. Kaplan RM. Syphilis, sex and psychiatry, 1789-1925: Part 1. Australas Psychiatry. 2010;18(1): 17-21. doi: 10.3109/10398560903295709.
71. Wright AD. Venereal disease and the great. Br J Vener Dis. 1971;47:295–306. doi: 10.1136/st i.47.4.295.
72. Weissfeld AS. Infectious Diseases and Famous People Who Succumbed to Them Clinical Microbiology Newsletter. Clinical Microbiology Newsletter. 2009;31:169–172.
73. Brinch O. The medical problems of Henry VIII. Centaurus. 1958;5(3-4):339-69.
74. Shrewsbury JF. Henry VIII: a medical study. J Hist Med Allied Sci. 1952;7(2):141-85. doi: 10.109 3/jhmas/vii.2.141.
75. Sands K, Dennis M, Venkatesh R. “Fr02-06 Down the Chute”. The Journal of Urology. 2020; 203 (203): 293–294. doi:10.1097/JU.0000000000000851.06. S2CID 218949508.
76. Santing CG, Raimond-Waarts L. Sex a Cardinal’s Sin. Punished by Syphilis in Renaissance Rome. Leidschrift Historisch Tijdschrift, 2010;25: 169-182. Available online:
https://research.rug.nl/en/publications/sex-a-cardinals-sin-punished-by-syphilis-in-renaissance-rome (Accessed 26 October 2024).
77. O’Malley CD. Some episodes in the medical history of Emperor Charles V; an imperial problem and the problem of an emperor. J Hist Med Allied Sci. 1958;13(4):469-82. English, French.
78. Salmon M. Evidence for the Presence of Treponemal Disease, Including Syphilis, in Late Medieval Europe. The Medieval Globe. 2021;7(2); 37-87. Available online: https://muse.jhu.edu/article/842358 (Accessed 26 2024).
79. Tampa M, Sarbu I, Matei C, Benea V, Georgescu SR. Brief history of syphilis. J Med Life. 2014;7(1):4-10.
80. Zanello M, Roux A, Gavaret M, et al. King Charles VIII of France’s Death: From an Unsubstantiated Traumatic Brain Injury to More Realistic Hypotheses. World Neurosurg. 2021;156: 60-67. doi: 10.1016/j.wneu.2021.09.056.
81. Morton RS. Did Catherine the Great of Russia have syphilis? Genitourin Med. 1991;67(6):498-502. doi: 10.1136/sti.67.6.498.
82. Staff. Wane State University School of Medicine. Did syphilis really cause John Wilkes Booth to assassinate Abraham Lincoln? April 17, 2018. Available online:
https://today.wayne.edu/medicine/news/2018/04/17/did-syphilis-really-cause-john-wilkes-booth-to-assassinate-abraham-lincoln-23684#:~:text=%22With%20all%20the%20women%20in%20his%20life%2C%20including,and%20what%20finally%20put%20him%20over%20the%20edge.%22 (Accessed 24 October 2024).
83. Bergreen L. Capone: The Man and the Era. New York: Simon and Schuster Paperbacks. ISBN 978-0-684-82447-5. 1994.
84. Sefton AM. The Great Pox that was…syphilis. J Appl Microbiol. 2001;91(4):592-6. doi: 10.1046/j. 1365-2672.2001.01494.x.
85. Weissfeld AS. Infectious Diseases and Famous People Who Succumbed to Them. Clin Microbiol Newsl. 2009;22(31):169-72.
86. Keatley P. Obituary: Idi Amin. The Guardian. August 17, 2003. Available online:
https://www.theguardian.com/news/2003/aug/18/guardianobituaries (Accessed 25 October 2024).
87. Retief FP, Wessels A. Did Adolf Hitler have syphilis? S Afr Med J. 2005;95(10):750, 752, 754, 756.
88. Hayden, Deborah. Pox: Genius, Madness, And the Mysteries of Syphilis. Basic Books. ISBN 978-0786724130. OCLC 50725392. 2008.
89. Sacks O. Awakenings. New York: Harper Perennial; 1973.
90. Chivers, C. J. “A Retrospective Diagnosis Says Lenin Had Syphilis”. The New York Times. 22 June 2004
91. Brinn D. Israeli researchers solve mystery of Lenin’s death. July 25, 2004, Updated September 13, 2012. Available online:
https://www.israel21c.org/israeli-researchers-solve-mystery-of-lenins-death/ (Accessed on 24 October 2024).
92. Manaev G. What happened to Lenin’s brain after death? October 01, 2020. Available online: https://www.rbth.com/history/332791-what-happened-to-lenins-brain (Accessed 24 October 2024).
93. Bhattacharyya KB. Adolf Hitler and His Parkinsonism. Ann Indian Acad Neurol. 2015;18(4): 387-90. doi: 10.4103/0972-2327.169536.
Wright AD. Venereal disease and the great. Br J Vener Dis. 1971;47:295. doi: 10.1136/sti.47.4.295.
94. Auden GA. Behaviour changes supervening upon encephalitis in children. Lancet. 1922;200: 901–904.
95. Ruiz V. ‘A disease that makes criminals’: Encephalitis lethargica (EL) in children, mental deficiency, and the 1927 Mental Deficiency Act. Endeavour. 2015;39:44–51.
96. Gupta R, Kim C, Agarwal N, Lieber B, Monaco EA 3rd. Understanding the Influence of Parkinson Disease on Adolf Hitler’s Decision-Making during World War II. World Neurosurg. 2015;84 (5):1447-52. doi: 10.1016/j.wneu.2015.06.014.
97. Tselis A, Booss J. Behavioral consequences of infections of the central nervous system: with emphasis on viral infections. J Am Acad Psychiatry Law. 2003;31(3):289-98.
98. Bhattacharyya KB. Adolf Hitler and His Parkinsonism. Ann Indian Acad Neurol. 2015;18(4): 387-90. doi: 10.4103/0972-2327.169536.
Wright AD. Venereal disease and the great. Br J Vener Dis. 1971;47:295. doi: 10.1136/sti.47.4.295.
99. Lickiewicz, J., Piotrowicz, K., Makara-Studzińska, M. (2023). The Weather, Aggression, and Aggressive Behavior in Psychiatric Hospitals. In: Martin, C., Preedy, V.R., Patel, V.B. (eds) Handbook of Anger, Aggression, and Violence. 2023, Springer, Cham. https://doi.org/10.1007/978-3-030-98711-4_65-1
100. Mikutta CA, Pervilhac C, Znoj H, Federspiel A, Müller TJ. The Impact of Foehn Wind on Mental Distress among Patients in a Swiss Psychiatric Hospital. Int J Environ Res Public Health. 2022, 19(17):10831. doi: 10.3390/ijerph191710831.
101. Greve F, Kanz KG, Zyskowski M, von Matthey F, Biberthaler P, Muthers S, Matzarakis A, Lefering R, Huber-Wagner S. The influence of foehn winds on the incidence of severe injuries in southern Bavaria – an analysis of the TraumaRegister DGU®. BMC Musculoskelet Disord. 2020, 21(1):568.
doi: 10.1186/s12891-020-03572-z.
102. Forum on Global Violence Prevention; Board on Global Health; Institute of Medicine; National Research Council. Contagion of Violence: Workshop Summary. Washington (DC): National Academies Press (US); 2013 Feb 6. II.9, Violence is a Contagious Disease. Available online:
https://www.ncbi.nlm.nih.gov/books/NBK207245/ (Accessed 24 October 2024).
103. Iacopini I, Petri G, Baronchelli A. et al. Group interactions modulate critical mass dynamics in social convention. Commun Phys. 2022;5:64. doi: 10.1038/s42005-022-00845-y
104. Collins, R. Theorizing the time-dynamics of violence. Violence: Int Jl. 2020;1(1), 166-184. https://doi.org/10.1177/2633002420907768.
105. Malthaner, S. Processes of Political Violence and the Dynamics of Situational Interaction. IJCV. 2017;11, 1-10. doi: 10.4119/UNIBI/ijcv.627.
106. Ecology Drives the Global Distribution of Human Diseases. PLoS Biol. 2004;2(6):e186.
doi: 10.1371/journal.pbio.0020186.
107. Møller AP. Evidence of Larger Impact of Parasites on Hosts in the Tropics: Investment in Immune Function within and outside the Tropics. Oikos. 1998;82(2), 265–270. https://doi.org/10.2307/3546966.
108. Infectious diseases in Afghanistan: Report by the Global Disaster Information Network (GDIN). 7 Nov 2001. Available online:
https://reliefweb.int/report/afghanistan/infectious-diseases-afghanistan-report-global-disaster-information-network-gdin (Accessed 24 October 2024).
109. Wallace MR, Hale BR, Utz GC, et al. Endemic Infectious Diseases of Afghanistan, Clinical Infectious Diseases. 2002;34:S171–S207. doi: 10.1086/340704
110. Burki T. Infectious diseases in Yemen. Lancet Infect Dis. 2021;21(5):610-611. doi: 10.1016/S1473-3099(21)00218-8.
111. The Lancet Infectious Diseases. Cholera in Yemen: war, hunger, disease…and heroics. Lancet Infect Dis. 2017;17(8):781. doi: 10.1016/S1473-30 99(17)30406-1.
112. USAID. Disease vector Hazard Report: Yemen chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://vectormap.si.edu/downloads/VHazardReports/DVHR_Yemen.pdf.
113. WHO update on health situation and needs in Yemen at today´s UN bi-weekly press briefing in Geneva. 21 Apr 2023. Available online:
https://reliefweb.int/report/yemen/who-update-health-situation-and-needs-yemen-todays-un-bi-weekly-press-briefing-geneva (Accessed 24 October 2024).
114. USAID. Health and the People of South Sudan. Available online:
https://www.usaid.gov/south-sudan/global-health#:~:text=Malaria%2C%20HIV/AIDS%2C%20and,increase%20access%20to%20clean%20water. (Accessed 24 October 2024).
115. Tarnas MC, Almhawish N, Karah N, Sullivan R, Abbara A. Communicable diseases in northwest Syria in the context of protracted armed conflict and earthquakes. Lancet Infect Dis. 2023;23(11): e477-e481. doi: 10.1016/S1473-3099(23)00201-3.
116. Marou, V., Vardavas, C.I., Aslanoglou, K. et al. The impact of conflict on infectious disease: a systematic literature review. Confl Health. 18;27 (2024). https://doi.org/10.1186/s13031-023-00568-z
117. State of Health in the EU Iceland Country Health Profile 2022. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://health.ec.europa.eu/system/files/2021-12/2021_chp_is_english.pdf (Accessed 24 October 2024).
118. Vigfusson HB, Hardarson HS, Ludviksson BR, Gudlaugsson O. Lyme disease in Iceland – Epidemiology from 2011 to 2015. Laeknabladid. 2019;105(2):63-70. Icelandic. doi: 10.17992/lbl.20 19.02.215.
119. Christie S, Tobias M. The burden of infectious disease in New Zealand. Aust N Z J Public Health. 1998;22(2):257-60. doi: 10.1111/j.1467-842x.199 8.tb01184.x.
120. Hvidberg MF, Johnsen SP, Davidsen M, Ehlers L. A Nationwide Study of Prevalence Rates and Characteristics of 199 Chronic Conditions in Denmark. Pharmacoecon Open. 2020;4(2):361-380. doi: 10.1007/s41669-019-0167-7.
121. IISS. The Armed Conflict Survey 2022: Sub-Saharan Africa Regional Analysis. 18th November 2022. Available online:
https://www.iiss.org/online-analysis/online-analysis/2022/11/acs-2022-sub-saharan-africa/ (Accessed 17 November 2024).
122. ACLED. Regional Overview Latin America and the Caribbean October 2024. 8 November. Available online: 32024.
https://acleddata.com/2024/11/08/latin-america-and-the-caribbean-overview-october-2024/ (Accessed 17 November 2024).
123. Bransfield RC. Intrusive symptoms and infectious encephalopathies. Neurol Psychiatry Brain Res. 2016;22:3–4.
124. Mead P. Epidemiology of Lyme Disease. Infect Dis Clin North Am. 2022;36(3):495-521.
doi: 10.1016/j.idc.2022.03.004.
125. Dong Y, Zhou G, Cao W, et al. Global seroprevalence and sociodemographic characteristics of Borrelia burgdorferi sensu lato in human populations: a systematic review and meta-analysis. BMJ Glob Health. 2022;7(6):e007744. doi: 10.1136/bmjgh-2021-007744.
126. Madhi DK, Issa AH, Al-Luaibi Y, Al-Maliki QN. First report of Borrelia spp. and Borreliella spp. in blood, urine, and buccal cavity of patients with psychiatric disorder in Basra Province, Iraq. Drug Invention Today. 2019;11(11):2927-2932.
127. Eppig C, Fincher CL, Thornhill R. Parasite Prevalence and the Worldwide Distribution of Cognitive Ability. In: Institute of Medicine (US) Forum on Microbial Threats. The Causes and Impacts of Neglected Tropical and Zoonotic Diseases: Opportunities for Integrated Intervention Strategies. Washington (DC): National Academies Press (US); 2011. A3. Available from: https://www.ncbi.nlm.nih.gov/books/NBK62514/ (Accessed 24 October 2024).
128. Proceedings B editorial team. Retraction: ‘Parasite prevalence and the worldwide distribution of cognitive ability’ (2010), by Eppig, Fincher and Thornhill. Proc Biol Sci. 2024;291(2017):20240463. doi: 10.1098/rspb.2024.0463.
129. Letendre K, Fincher CL, Thornhill R. Does infectious disease cause global variation in the frequency of intrastate armed conflict and civil war? Biol Rev. 2010;85:669-83. doi: 10.1111/j.1469-185X.2010.00133.x.
130. Bransfield RC. Did Infections Caused by World War I Contribute to Causing World War II? Contagion Live. January 5, 2018. Available online: https://www.contagionlive.com/view/did-infections-caused-by-world-war-i-contribute-to-causing-world-war-ii (Accessed 24 October 2024).
131. Varney NR, Roberts RJ, Springer JA, Connell SK, Wood PS. Neuropsychiatric sequelae of cerebral malaria in Vietnam veterans. J Nerv Ment Dis. 1997;185(11):695-703. doi: 10.1097/000 05053-199711000-00008.
132. Nicolson GL, Nasralla MY, Haier J, Pomfret J. High frequency of systemic mycoplasmal infections in Gulf War veterans and civilians with Amyotrophic Lateral Sclerosis (ALS). J Clin Neurosci. 2002;9(5):525-9. doi: 10.1054/jocn.2001.1075.
133. Nicholson G. Chronic Mycoplasmal Infections in Gulf War Veterans’ Children and Autism Patients. Medical Veritas. 2005;2:383-387 2005. doi: 10.1588/medver.2005.02.00047
134. Wood, G.K., Sargent, B.F., Ahmad, ZUA. et al. Post-hospitalisation COVID-19 cognitive deficits at one year are global and associated with elevated brain injury markers and grey matter volume reduction. Nat Med. 2024. doi: 10.1038/s41591-024-03309-8.
135. Ladds E, Darbyshire JL, Bakerly ND, Falope Z, Tucker-Bell I. Cognitive dysfunction after covid-19. BMJ. 2024;384:e075387. doi: 10.1136/bmj-20 23-075387.
136. Zhao S, Martin EM, Reuken PA, et al. Long COVID is associated with severe cognitive slowing: a multicentre cross-sectional study. EClinicalMedicine. 2024;68:102434. doi: 10.1016/j.eclinm.2024.102434.
137. Miskowiak KW, Fugledalen L, Jespersen AE, et al. Trajectory of cognitive impairments over 1 year after COVID-19 hospitalisation: Pattern, severity, and functional implications. Eur Neuropsychopharmacol. 2022;59:82-92. doi: 10.1016/j.euroneuro.2022.04.004.
138. Hampshire A, Azor A, Atchison C, et al. Cognition and Memory after Covid-19 in a Large Community Sample. N Engl J Med. 2024;390(9): 806-818. doi: 10.1056/NEJMoa2311330.
139. Cheetham NJ, Penfold R, Giunchiglia V, et al. The effects of COVID-19 on cognitive performance in a community-based cohort: a COVID symptom study biobank prospective cohort study. EClinicalMedicine. 2023;62:102086. doi: 10.1016/j.eclinm.2023.102086.
140. Al-Aly Z, Rosen CJ. Long Covid and Impaired Cognition – More Evidence and More Work to Do. N Engl J Med. 2024;390(9):858-860. doi: 10.1056/NEJMe2400189.
141. Clemente-Suárez VJ, Martínez-González MB, Benitez-Agudelo JC, et al. The Impact of the COVID-19 Pandemic on Mental Disorders. A Critical Review. Int J Environ Res Public Health. 2021;18(19):10041. doi: 10.3390/ijerph181910041.
142. Nakamura, Z.M., Nash, R.P., Laughon, S.L. et al. Neuropsychiatric Complications of COVID-19. Curr Psychiatry Rep. 2021;23:25. doi: 10.1007/s11920-021-01237-9.
143. Temirpulotovich TB, Uzokboevich TA, Murodullaevich KR, Bahtiyarovich AR, Xazratovich KZ, Toshevich RH. The Impact of Medical and Social Factors on Alcohol Abuse in Patients with Alcoholism During the Covid-19 Pandemic. Journal of Pharmaceutical Negative Results. 2022;8195-8200. doi: 10.47750/pnr.2022.13.S09.959.
144. Melamed OC, Hauck TS, Buckley L, Selby P, Mulsant BH. Article Commentary: COVID-19 and Persons with Substance use Disorders: Inequities and Mitigation Strategies. Substance Abuse. 2020;41(3):286-291. doi: 10.1080/08897077.202 0.1784363
145. Polo, Sara M.T. “A Pandemic of Violence? The Impact of COVID-19 on Conflict” Peace Economics, Peace Science and Public Policy. 2020;26(3):202 00050. doi: 10.1515/peps-2020-0050
146. Whiteman PJ, Macias-Konstantopoulos WL, Relan P, Knopov A, Ranney ML, Riviello RJ. Violence and Abuse: A Pandemic Within a Pandemic. West J Emerg Med. 2023;24(4):743-750. doi: 10.5811/w estjem.58405.
147. Sutherland M, McKenney M, Elkbuli A. Gun violence during COVID-19 pandemic: Paradoxical trends in New York City, Chicago, Los Angeles and Baltimore. Am J Emerg Med. 2021;39:225-226. doi: 10.1016/j.ajem.2020.05.006.
148. de Oliveira SMT, Galdeano EA, da Trindade EMGG, et al. Epidemiological Study of Violence against Children and Its Increase during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021;18(19):10061. doi: 10.3390/ijerph181910061
149. Boserup B, McKenney M, Elkbuli A. Alarming trends in US domestic violence during the COVID-19 pandemic. Am J Emerg Med. 2020,38(12):2753-2755. doi: 10.1016/j.ajem.2020.04.077.
150. Filipska K, Biercewicz M, Wiśniewski A, et al. High Rate of Elder Abuse in the Time of COVID-19—A Cross Sectional Study of Geriatric and Neurology Clinic Patients. J. Clin. Med. 2021;10, 4532. doi: 10.3390/jcm10194532
151. Institute for Economics & Peace. Global Peace Index 2024: Measuring Peace in a Complex World, Sydney, June 2024. Available from: http://visionofhumanity.org/resources (accessed 25 August 2024).
152. Buch Institute. COVID-19: The Past, Present and Future of Pandemics. April 5, 2021. Available online: https://www.buckinstitute.org/blog/covid-19-the-past-present-and-future-of-pandemics/?utm_source=google&utm_campaign=9875367091&utm_content=114572789704&utm_term=&utm_medium=460160308540&gad_source=1&gclid=Cj0KCQjwu8uyBhC6ARIsAKwBGpQ9_V7OPRIPaJUicES9zy8G3jrCgLCbecLvdh9mwFsQe3fyFxw-c0UaAtT9EALw_wcB (Accessed 24 October 2024).
153. Sam, Regi. “TRACKING THE CHRONOLOGY OF EPIDEMICS AND PANDEMICS”. Journal of Natural Remedies. 2022;21 (3):100–105.
154. UNECO. The spread of Disease along the Silk Roads: Smallpox. Available online:
https://en.unesco.org/silkroad/content/spread-disease-along-silk-roads-smallpox#:~:text=By%20the%207th%20century,Northern%20Africa%2C%20Spain%20and%20Portugal (Accessed 11 November 2024).
155. Dalekou S, Michaleas SN, Tsitsika AK, Karamanou M. Comparative study of pandemics and their impact on children and adolescents: COVID-19 and Spanish Flu. Infez Med. 2023;31(2): 131-139. doi: 10.53854/liim-3102-1.
156. Roberts JD, Tehrani SO. Environments, Behaviors, and Inequalities: Reflecting on the Impacts of the Influenza and Coronavirus Pandemics in the United States. Int J Environ Res Public Health. 2020;17(12):4484. doi: 10.3390/ijerph1712 4484.
157. Auden, G.A. Behaviour changes supervening upon encephalitis in children. Lancet 1922;200: 901–904.
158. Ruiz, V. ‘A disease that makes criminals’: Encephalitis lethargica (EL) in children, mental deficiency, and the 1927 Mental Deficiency Act. Endeavour. 2015;39:44–51.
159. Singer EJ, Thames AD. Neurobehavioral Manifestations of Human Immunodeficiency Virus/AIDS: Diagnosis and Treatment. Neurol Clin. 2016;34(1):33-53. doi: 10.1016/j.ncl.2015.08.003.
160. Klot JF, Auerbach JD, Berry MR. Sexual violence and HIV transmission: summary proceedings of a scientific research planning meeting. Am J Reprod Immunol. 2013;69 Suppl 1(0 1):5-19.
doi: 10.1111/aji.12033.
161. Ijeoma Aniekwu N, Atsenuwa, A. Sexual Violence and HIV/AIDS in Sub-Saharan Africa: An Intimate Link. Local Environment, 2007;12(3), 313–324. doi: 10.1080/13549830601098289.
162. Cohn SK. Pandemics: waves of disease, waves of hate from the Plague of Athens to A.I.D.S. Hist J. 2012;85(230):535-555. doi: 10.1111/j.1468-2281.2012.00603.x.
163. Jedwab R, Khan AM, Russ J, Zaveri ED. Epidemics, pandemics, and social conflict: Lessons from the past and possible scenarios for COVID-19. World Dev. 2021;147:105629. doi: 10.1016/j.w orlddev.2021.105629.
164. Bransfield RC. Can High Disease Burden Make Some Parts of the World More Prone to Violence’ 11 Jan 2018. Available online: www.contagionlive.com/videos/can-high-disease-burden-make-some-parts-of-the-world-more-prone-to-violence (Accessed 28 December 2024).
165. Bransfield RC. Can Infectious Disease Physicians Help Prevent Violence? Contagion Live. 17 April 2018. Available online:
https://www.contagionlive.com/view/can-infectious-disease-physicians-help-prevent-violence (Accessed 28 December 2024).
166. Mackenzie JS, Jeggo M. The One Health Approach-Why Is It So Important? Trop Med Infect Dis. 2019;4(2):88. doi: 10.3390/tropicalmed4020088.
167. Matteo Cervellati, Elena Esposito, Uwe Sunde; Epidemic Shocks and Civil Violence: Evidence from Malaria Outbreaks in Africa. Rev. Econ. Stat. 2022; 104 (4): 780–796. doi: https://doi.org/10.1162/rest_a_01050
168. Koren O, Bukari KN. (Re)Emerging disease and conflict risk in Africa, 1997-2019. Nat Hum Behav. 2024;8(8):1506-1513. doi: 10.1038/s41562-024-01929-1.
169. Paaijmans KP, Read AF, Thomas MB. Understanding the link between malaria risk and climate. Proc Natl Acad Sci U S A. 2009;106(33): 13844-9. doi: 10.1073/pnas.0903423106.
170. Ssenkusu JM, Hodges JS, Opoka RO, Idro R, Shapiro E, John CC, Bangirana P. Long-term Behavioral Problems in Children With Severe Malaria. Pediatrics. 2016;138(5):e20161965. doi: 10.1542/p eds.2016-1965. Erratum in: Pediatrics. 2017;140(5): e20172709. doi: 10.1542/peds.2017-2709.
171. Idro R, Kakooza-Mwesige A, Asea B, Ssebyala K, Bangirana P, Opoka RO, Lubowa SK, Semrud-Clikeman M, John CC, Nalugya J. Cerebral malaria is associated with long-term mental health disorders: a cross sectional survey of a long-term cohort. Malar J. 2016;15:184. doi: 10.1186/s12936-016-1233-6.
172. Ssemata AS, Nakitende AJ, Kizito S, Thomas MR, Islam S, Bangirana P, Nakasujja N, Yang Z, Yu Y, Tran TM, John CC, McHenry MS. Association of severe malaria with cognitive and behavioural outcomes in low- and middle-income countries: a meta-analysis and systematic review. Malar J. 2023;22(1):227. doi: 10.1186/s12936-023-04653-9.
173. Dworkin MS, Schwan TG, Anderson DE Jr, Borchardt SM. Tick-borne relapsing fever. Infect Dis Clin North Am. 2008;22(3):449-68, viii. doi: 10.1016/j.idc.2008.03.006.
174. Goubau PF. Relapsing fevers. A review. Ann Soc Belg Med Trop. 1984;64(4):335-64.
175. Boodman C, Fongwen N, Pecoraro AJ, Mihret A, Abayneh H, Fournier PE, Gupta N, van Griensven J. Hidden Burden of Bartonella Quintana on the African Continent: Should the Bacterial Infection Be Considered a Neglected Tropical Disease? Open Forum Infect Dis. 2023;11(2):ofad672. doi: 10.1093/ofid/ofad672.
176. Adegboye O, Gayawan E, James A, Adegboye A, Elfaki F. Bayesian spatial modelling of Ebola outbreaks in Democratic Republic of Congo through the INLA-SPDE approach. Zoonoses Public Health. 2021;68(5):443-451. doi: 10.1111/zph.12828.
177. Cheslock MA, Embers ME. Human Bartonellosis: An Underappreciated Public Health Problem? Trop Med Infect Dis. 2019;4(2):69. doi: 10.3390/tropicalmed4020069.