





Multidisciplinary Ambulatory Arthroplasty Program Outcomes
Design, Implementation, and Early Safety Outcomes of a Multidisciplinary Ambulatory Arthroplasty Program With Structured Home-Based Care in a Medium-Complexity Setting
Ivan Agudelo. MD. HSSE1, Liliana Ceballos. RN. HSSE2*, Silvia Arango. MD3*, Claudia Acosta. RN. HCQ4*, Ana Milena Herrera Torres. MD. MSc. Ph.D.5**
- Medical and scientific director. Department of medical and clinical direction. Clínica del Campestre. Medellín. Colombia
- Nursing director. Department of nursing and patient’s safety. Clínica del Campestre. Medellín. Colombia
- Medical coordinator. Department of medical and clinical direction. Clínica del Campestre. Medellín. Colombia
- Quality director. Department of Healthcare auditing and quality. Clínica del Campestre. Medellín. Colombia
- Epidemiologist. Department of epidemiology and clinical research. Clínica del Campestre. Medellín. Colombia
These authors contributed equally to this work
OPEN ACCESS
PUBLISHED: 30 April 2026
CITATION: Agudelo, I., Ceballos, L., et al., 2026. Design, Implementation, and Early Safety Outcomes of a Multidisciplinary Ambulatory Arthroplasty Program With Structured Home-Based Care in a Medium-Complexity Setting. Medical Research Archives, [online] 14(4).
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Background: Ambulatory joint arthroplasty has expanded worldwide as a safe and efficient alternative to inpatient care for selected patients. However, same-day discharge shifts postoperative risk from the hospital to the home, posing patient safety challenges—particularly in medium-complexity institutions without continuous inpatient monitoring. Many outpatient arthroplasty programs emphasize perioperative optimization but provide limited description of structured post-discharge safety strategies.
Local problem: Our institution sought to expand ambulatory shoulder and knee arthroplasty while maintaining high safety standards in a secondary-level private orthopedic center. The absence of inpatient observation required a reliable system to detect and manage early postoperative complications in the home setting.
Methods: We designed and implemented a multidisciplinary ambulatory arthroplasty program incorporating rigorous patient selection, standardized perioperative safety protocols, and structured home-based care. Patient eligibility was assessed by orthopedics, internal medicine, anesthesiology, and infectology. Interventions included multimodal anesthesia and analgesia, infection-prevention bundles, same-day discharge criteria, in-home nursing visits, early supervised home rehabilitation, daily postoperative telephone follow-up, and scheduled outpatient assessments. This quality improvement initiative was evaluated using descriptive analysis of early safety outcomes. Data gathering was carried out between February 2024 and July 2025. The primary outcome was the occurrence of major adverse events within 30 days (death, unplanned readmission, reoperation, thromboembolism, or deep surgical site infection).
Results: 41 consecutive ambulatory joint replacements (35 shoulder and 6 knee arthroplasties) were performed under the program. Adherence to perioperative and post-discharge protocols was complete. No major adverse events, readmissions, thromboembolic complications, or deep infections were observed within 30 days. Minor postoperative issues were identified early through home-based monitoring and resolved without sequelae. All patients demonstrated satisfactory functional recovery and reported high satisfaction with care.
Conclusions: A deliberately designed ambulatory arthroplasty program that integrates multidisciplinary patient selection with structured home-based nursing and rehabilitation can support safe same-day discharge in medium-complexity settings. Home-based care functioned as a critical safety control after discharge and may enhance the reliability of outpatient joint replacement programs. This framework may be adaptable to other institutions seeking to expand ambulatory surgical capacity while prioritizing patient safety.
Keywords: Arthroplasty, Replacement, Shoulder; Arthroplasty, Replacement, Knee; Outpatient Clinics, Hospital; Patient Safety; Quality Assurance, Health Care.
Introduction
Ambulatory joint arthroplasty has expanded rapidly over the past decade as advances in perioperative care have enabled safe same-day discharge for carefully selected patients. Compared with inpatient pathways, outpatient arthroplasty is associated with comparable complication and readmission rates, high patient satisfaction, and potential cost savings. These benefits have supported its adoption for both shoulder and knee replacement procedures in a wide range of health care systems.
However, same-day discharge fundamentally redistributes postoperative risk from the inpatient environment to the home. Early complications that would traditionally be identified during hospital observation, such as uncontrolled pain, wound complications, early infection, thromboembolic events, or functional decline, must instead be detected and managed after discharge. This transition poses particular challenges for medium-complexity and secondary-level institutions, which often lack inpatient orthopedic units, extended postoperative monitoring capacity, or immediate access to tertiary-level resources.
In such settings, expanding ambulatory arthroplasty without a deliberate post-discharge safety strategy may increase the risk of delayed complication recognition, unplanned readmissions, and patient harm. Despite the growing adoption of outpatient shoulder and knee arthroplasty, there is limited published guidance describing how non-tertiary institutions can design reliable systems to ensure postoperative safety once patients leave the facility.
Multiple observational studies and systematic reviews have demonstrated that outpatient shoulder and knee arthroplasty can achieve complication, readmission, and satisfaction outcomes comparable to inpatient procedures when strict perioperative protocols are applied.
Key contributors to successful outpatient pathways include careful patient selection, advances in regional anesthesia and multimodal analgesia, standardized infection-prevention strategies, and enhanced recovery protocols promoting early mobilization. While these elements are well described, most outpatient arthroplasty programs focus primarily on perioperative optimization and same-day discharge criteria. Post-discharge follow-up is frequently limited to scheduled outpatient visits or patient-initiated contact, with relatively sparse reporting of structured, proactive safety mechanisms during the early postoperative period at home. As a result, the literature provides limited practical insight into how outpatient programs, particularly those operating outside high-resource tertiary centers, can systematically monitor patients and mitigate risk after discharge.
We hypothesized that structured home-based care, including early nursing assessment, supervised rehabilitation, and proactive communication, could function as a critical post-discharge safety control, analogous to inpatient observation in traditional arthroplasty pathways. Previous studies in surgical and medical populations suggest that early home-based monitoring and coordinated follow-up can facilitate timely identification of complications, improve adherence to care plans, and enhance patient experience. However, these strategies have not been consistently integrated or evaluated as core components of ambulatory arthroplasty safety systems.
To address this gap, our institution designed an ambulatory arthroplasty program that integrates multidisciplinary patient selection, standardized perioperative safety protocols, and coordinated home-based postoperative care into a single, unified system. This approach was intended to enhance reliability, reduce variability, and mitigate the patient safety risks inherent to outpatient joint replacement in a medium-complexity setting.
The aim of this improvement initiative was to design, implement, and evaluate a multidisciplinary ambulatory arthroplasty program for shoulder and knee replacement that incorporates structured home-based nursing and rehabilitation as central safety elements. This report describes the program framework and examines early safety outcomes following implementation, with the goal of providing a reproducible model for institutions seeking to expand ambulatory arthroplasty while prioritizing patient safety.
Materials and Methods
This report follows the Revised Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) guidelines for reporting system-level initiatives to improve the quality and safety of health care.
CONTEXT
This improvement initiative was conducted at a private, secondary-level orthopedic center in Colombia specializing in ambulatory musculoskeletal surgery. The institution performs elective orthopedic procedures but does not operate as a tertiary referral hospital and does not provide routine inpatient orthopedic ward care. As such, postoperative monitoring following ambulatory surgery relies on structured outpatient and home-based services rather than prolonged in-hospital observation.
Prior to implementation of the ambulatory arthroplasty program, joint replacement procedures were performed exclusively under inpatient pathways or referred to higher-complexity institutions. Institutional leadership identified outpatient shoulder and knee arthroplasty as a strategic priority to improve patient-centered care and optimize surgical capacity, provided that patient safety could be reliably maintained after same-day discharge.
INTERVENTION
Program Design Overview
We designed a multidisciplinary ambulatory arthroplasty program integrating three core components:
- Rigorous, multidisciplinary patient selection
- Standardized perioperative safety protocols
- Structured home-based postoperative care
These components were implemented as an integrated system rather than as independent interventions.
Preoperative Phase: Patient Selection and Optimization
Patients considered for ambulatory shoulder or knee arthroplasty were initially identified by the treating orthopedic surgeon and subsequently underwent mandatory evaluation by internal medicine, anesthesiology, and infectology. Preoperative assessment focused on identifying comorbidities and social factors associated with increased postoperative risk, including smoking, alcohol use, diabetes, chronic kidney or liver disease, chronic obstructive pulmonary disease, anemia, malnutrition, obesity, prior thromboembolic events, cognitive impairment, and adequacy of home support. Laboratory testing included complete blood count, serum creatinine, fasting glucose, electrocardiogram, and additional tests as clinically indicated. Methicillin-resistant Staphylococcus aureus (MRSA) screening was routinely performed.
Eligibility criteria included American Society of Anesthesiologists (ASA) physical status I or II, or ASA III with stable and well-controlled comorbidities, adequate caregiver support at home, and willingness to participate in home-based nursing and rehabilitation. Absolute contraindications included uncontrolled medical conditions, bleeding disorders, chronic anticoagulation that could not be safely managed perioperatively, body mass index greater than 40 kg/m², hypoalbuminemia, active infection, or severe cognitive impairment.
Patients identified as MRSA carriers underwent preoperative decolonization and received targeted perioperative antibiotic prophylaxis.
Intraoperative Phase: Standardized Safety Protocols
All procedures were performed in operating rooms prepared according to institutional infection-prevention standards, including terminal cleaning and restricted traffic during prosthetic implantation. Standardized surgical attire, hand hygiene, and surgical-site preparation protocols were applied. Anesthetic management followed a multimodal approach, combining general anesthesia with regional techniques when appropriate, alongside non-opioid and opioid-sparing analgesic strategies. Prophylactic antibiotics were administered within recommended time windows before incision and re-dosed when indicated. Tranexamic acid was routinely used unless contraindicated. Intraoperative normothermia and glycemic control were actively maintained.
Postoperative Phase: Structured Home-Based Care
Patients were observed in the post-anesthesia care unit for a minimum of four hours. Same-day discharge criteria included hemodynamic stability, adequate pain control, tolerance of oral intake, ability to ambulate with assistance, and availability of a responsible caregiver.
Post-discharge care constituted a central component of the intervention and included:
- A scheduled in-home nursing visit within 12–24 hours for wound assessment, vital sign monitoring, medication reconciliation, and reinforcement of postoperative instructions
- Initiation of supervised home-based physical therapy within 24 hours
- Daily proactive telephone follow-up during the first postoperative week
- Scheduled outpatient evaluations at 1, 2, and 4 weeks, with additional visits as clinically indicated
This home-based care model was designed to function as an extension of postoperative monitoring and to facilitate early detection and management of complications.
STUDY OF THE INTERVENTION
This initiative was evaluated using a prospective observational design as part of an institutional quality improvement effort. The study focused on describing early safety outcomes following implementation of the ambulatory arthroplasty program rather than on hypothesis testing or comparison with inpatient pathways. The project was reviewed by the institutional oversight body and determined to constitute quality improvement activity; therefore, formal institutional review board approval was not required. Data gathering was carried out between February 2024 and July 2025. All patients provided informed consent for participation in the ambulatory pathway and follow-up.
MEASURES
Primary Outcome
The primary outcome was the occurrence of major adverse events within 30 days of surgery, defined as death, unplanned hospital readmission, reoperation, deep surgical site infection, or thromboembolic events.
Secondary Outcomes
- Minor postoperative complications
- Effectiveness of pain control
- Functional recovery, assessed using validated instruments; American Shoulder and Elbow Surgeons (ASES) score for shoulder arthroplasty and Knee Injury and Osteoarthritis Outcome Score (KOOS) for knee arthroplasty
- Patient-reported satisfaction with care
Process measures included adherence to preoperative screening protocols, completion of scheduled home-based nursing and rehabilitation visits, and completion of planned follow-up contacts.
ANALYSIS
Data were summarized using descriptive statistics. Categorical variables are presented as absolute numbers and percentages, and continuous variables are reported as medians with ranges. Given the improvement-focused nature of the initiative and the absence of a comparison group, no inferential statistical testing was performed to assess associations between interventions and outcomes.
ETHICAL CONSIDERATIONS
Ethical considerations focused on patient safety, informed consent, and protection of patient confidentiality. The ambulatory arthroplasty pathway was implemented with the intent to reduce harm and improve continuity of care. No external funding was received for this initiative, and no conflicts of interest are declared.
Results
IMPLEMENTATION AND PROGRAM UPTAKE
Following implementation of the ambulatory arthroplasty program, consecutive patients meeting eligibility criteria were enrolled without protocol deviation. A total of 41 ambulatory joint replacement procedures were performed under the program, including 35 shoulder arthroplasties and 6 knee arthroplasties. All procedures were completed with same-day discharge as planned. Adherence to the multidisciplinary screening process was complete. All patients underwent preoperative evaluation by orthopedics, internal medicine, anesthesiology, and infectology, and all met predefined clinical and social eligibility criteria for ambulatory care.
PATIENT CHARACTERISTICS
The median patient age was between the eight and seventh decades of life, and the majority of patients were females. Most patients were classified as ASA physical status II, with a smaller proportion classified as ASA III with stable, well-controlled comorbidities. Body mass index values reflected a normal or overweight but not morbidly obese population. All patients had confirmed caregiver support and agreed to participate in home-based nursing and rehabilitation. Baseline demographic and clinical characteristics are summarized in Table 1.
| Reverse Total Shoulder arthroplasty (n=35) | Knee Unicompartimental (n=6) | ||||
|---|---|---|---|---|---|
| Baseline characteristics | |||||
| *Age (years) | 74 (58 – 89) | 60 (46 – 73) | |||
| Sex | Females 26 (74.3%) | Males 9 (25.7%) | 6 (100%) | ||
| DM | 8 (22.9%) | ||||
| Hypertension | 15 (42.9%) | 3 (50%) | |||
| Coronary disease | 3 (8.6%) | 2 (33.3%) | |||
| Diagnosis | GH Arthrosis 17 (48.6%) | RC Arthropathy 10 (28.6%) | MRCT 8 (22.9%) | Gonarthrosis 6 (100%) | |
| *BMI | 28 (21.9 – 35.9) | 28.7 (25 – 29.1) | |||
| Weight category | Normal 19 (54.3%) | Overweight 11 (31.4%) | Obesity 5 (14.3%) | 2 (33.3%) | 4 (66.7%) |
| ASA classification | I 8 (22.9%) | II 22 (62.9%) | III 5 (14.3%) | 6 (100%) | |
| *ASES score PreOP | 33 (27 – 43) | ||||
| *KOOS PreOP | 26.5 (17 – 34) | ||||
| Surgical and immediate postoperative information | |||||
| *Surgical time (minutes) | 180 (120 – 215) | 185.5 (161 – 91) | |||
| Buprenorphine patch | 27 (77.1%) | 4 (66.7%) | |||
| Elastomeric pump (non opioid) | 8 (22.9%) | 2 (33.3%) | |||
| Neurophatic agent | 9 (25.7%) | 5 (83.3%) | |||
| Postoperative 90 days follow-up | |||||
| *ASES score POP | 93 (87 – 98) | ||||
| *KOOS POP | 90 (89 – 92) | ||||
| Patient satisfaction | Very high 29 (82.9%) | High 6 (17.1%) | 5 (83.3%) | 1 (16.7%) |
*Values expressed as medians and range (minimum – maximum). DM: Diabetes Mellitus; GH: Glenohumeral; RC: Rotator Cuff; MRCT: Massive Rotator Cuff Tear; BMI: Body Mass Index; ASA: American Society of Anesthesiologists; ASES: American Shoulder and Elbow Surgeons; KOOS: Knee injury and Osteoarthritis Outcome Score; PreOP: Preoperative; POP: Postoperative
PROCESS MEASURES AND PROTOCOL ADHERENCE
Adherence to standardized perioperative safety protocols was 100% across all cases. This included completion of preoperative laboratory and MRSA screening, application of infection-prevention measures, administration of antibiotic prophylaxis within recommended time windows, use of multimodal anesthesia and analgesia, and application of same-day discharge criteria. All patients received the planned home-based nursing visit within 12–24 hours of discharge. Supervised home-based physical therapy was initiated within 24 hours in all cases. Daily proactive telephone follow-up during the first postoperative week was completed as scheduled for all patients, with additional contacts initiated when clinically indicated.
PRIMARY SAFETY OUTCOMES
No major adverse events were observed within 30 days of surgery. Specifically, there were no deaths, unplanned hospital readmissions, reoperations, deep surgical site infections, or thromboembolic events during the 30-day postoperative period. No patients required escalation of care to inpatient hospitalization following same-day discharge.
SECONDARY OUTCOMES
Minor Postoperative Events
Minor postoperative issues were identified in a small number of patients during home-based monitoring. These included transient pain management challenges and localized discomfort without signs of infection or neurovascular compromise. All minor issues were detected early through scheduled home visits or proactive telephone follow-up and were managed conservatively without progression to major complications or unplanned health care utilization.
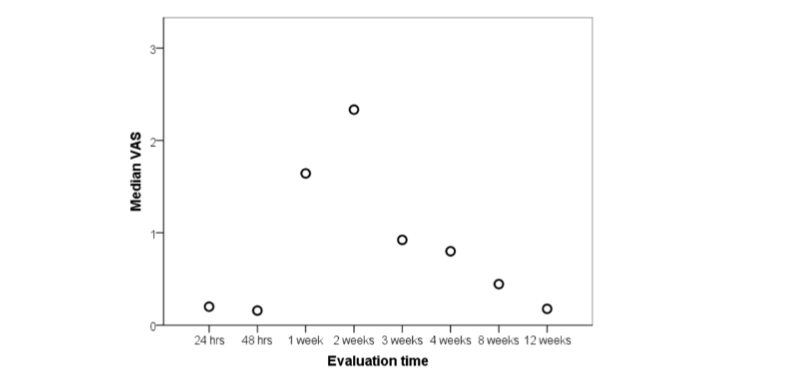
Pain Control
Multimodal analgesia provided adequate postoperative pain control for the majority of patients. In isolated cases where pain exceeded expected levels, additional interventions were implemented promptly following home-based assessment or telephone follow-up, resulting in symptom resolution without sequelae.
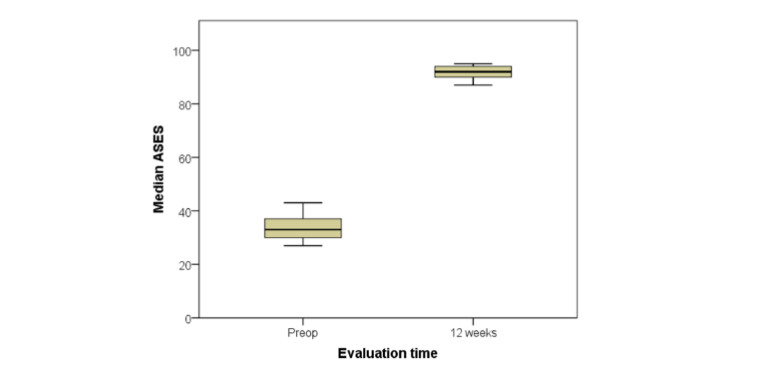
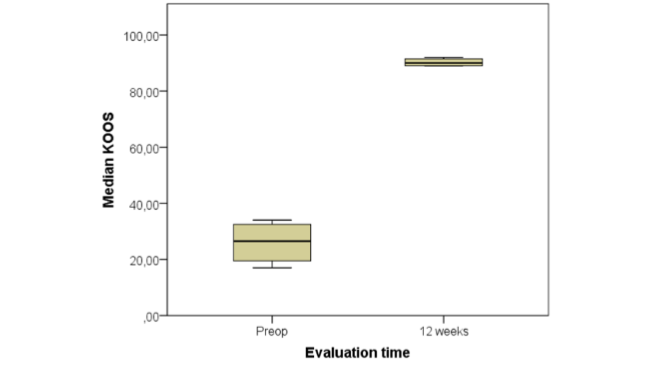
Functional Recovery and Patient Experience
All patients demonstrated satisfactory functional recovery during follow-up, as assessed by procedure-specific validated instruments (ASES and KOOS). Improvements were observed consistently across the cohort during the early postoperative period.
Patient-reported satisfaction with the ambulatory pathway was high. Most patients rated their experience as very satisfactory, citing continuity of care, early functional recovery, and reassurance provided by home-based nursing and rehabilitation as key contributors.
Discussion
STATEMENT OF PRINCIPAL FINDINGS
Implementation of a comprehensive, multidisciplinary outpatient arthroplasty program, integrating rigorous patient selection, perioperative safety measures, and structured home-based recovery, enabled safe same-day discharge for reverse shoulder and unicompartmental knee arthroplasties in a medium-complexity private practice. Among 41 consecutive patients, no major adverse events, readmissions, or infections occurred within 30 days. Functional outcomes improved significantly at 90 days, and satisfaction was high in all patients. These findings confirm that outpatient arthroplasty can be performed safely outside tertiary centers when standardized, multidisciplinary protocols are applied, consistent with prior reports showing comparable safety and efficacy between outpatient and inpatient settings.
INTERPRETATION WITHIN THE CONTEXT OF THE WIDER LITERATURE
Our results align with extensive evidence showing that outpatient shoulder and knee arthroplasties achieve complication rates comparable to inpatient procedures while improving satisfaction and reducing costs. Previous meta-analyses have shown that outpatient shoulder and knee arthroplasty achieves low complication and readmission rates, typically 3–7%, with patient satisfaction exceeding 90%. Several systematic reviews of shoulder arthroplasty reported that outpatient status was not an independent risk factor for complications, and short-term outcomes were even more favorable in outpatient cohorts. Our outcomes compare positively, as no patient experienced perioperative or postoperative complications within 90 days, despite a relatively advanced median age (73 years) and a high prevalence of comorbidities such as hypertension (61.9%) and diabetes (19%). These results emphasize the importance of coordinated perioperative management in minimizing risk. While much of the literature originates from high-volume academic or tertiary centers, our results are particularly significant because they demonstrate the feasibility and safety of outpatient arthroplasty in a smaller specialized practice. These outcomes underscore that rigorous protocols, including careful patient selection, perioperative optimization, and structured home-based care, can deliver safe and effective care.
The home-based recovery model distinguishes our program from traditional outpatient approaches. Multiple meta-analyses support the equivalence of home-based rehabilitation to traditional outpatient or inpatient models in terms of pain relief, functional outcomes, and complication rates. A 2023 systematic review found no significant differences in functional outcomes, readmissions, or complications between unsupervised home-based and outpatient rehabilitation after knee arthroplasty. Similarly, other studies confirmed that supervised or remotely monitored home therapy yields outcomes comparable to conventional care, with additional benefits of cost-effectiveness and reduced reliance on in-person visits. Our model differs by integrating in-home supervised rehabilitation from the first 24 hours after discharge, ensuring adherence to mobility protocols and allowing early detection of issues such as inadequate pain control or wound complications. While this approach may involve higher upfront costs than unsupervised home programs, it aligns with value-based care by potentially reducing preventable complications, unplanned readmissions, and long-term functional impairment.
Observed functional improvements and satisfaction levels parallel those of larger institutional cohorts. Shoulder and knee patients demonstrated marked improvements in standardized scores, consistent with outcomes reported by other studies. Patient satisfaction was uniformly high, with more than 80% of patients rating their satisfaction as very high. Beyond reflecting successful surgical outcomes, this likely reflects the added confidence provided by structured home support, education, and caregiver engagement.
Pain management is another critical determinant of success and fundamental for patient satisfaction. Multimodal analgesia, supported by either buprenorphine transdermal patches or elastomeric infusion pumps, provided effective control in nearly all patients. Two cases of atypical postoperative pain were unrelated to surgery (neuropathic pain from herpes zoster and failure of peripheral block efficacy) and resolved without compromising recovery. These findings emphasize the importance of tailoring analgesic strategies to individual patient needs while maintaining close follow-up for early detection of atypical pain levels.
Ideally, frameworks for outpatient arthroplasty programs should fully integrate the principles of scientific societies into the patient’s home environment. Our framework operationalizes international recommendations from various orthopedic associations that provide evidence-based recommendations for perioperative care.
IMPLICATIONS FOR POLICY, PRACTICE AND RESEARCH
Our experience demonstrates that safe outpatient arthroplasty is achievable outside tertiary centers when standardized, multidisciplinary protocols are applied. It highlights the added value of embedding structured home-based monitoring into outpatient pathways. Also, incorporating structured home-based recovery into national or institutional outpatient pathways could strengthen continuity of care, prevent avoidable readmissions, and enhance patient confidence. Compliance with infection-prevention measures likely reduced the risk of unrecognized complications and infections. Finally, it shows that such models may be particularly relevant in resource-constrained settings, where reducing hospitalization without compromising safety can enhance patient-centered care and improve system efficiency.
Future research should examine the cost-benefit relationship of supervised home recovery versus conventional outpatient rehabilitation, explore digital or telemonitoring adjuncts for remote follow-up, and assess scalability in diverse healthcare systems.
STRENGTHS AND LIMITATIONS
The principal strength of the study and distinctive feature of our program is the formal incorporation of structured home-based recovery as part of the safety model. Unlike many published frameworks that emphasize perioperative optimization but delegate recovery primarily to outpatient visits, our program incorporated early in-home nursing, wound surveillance, daily telephonic monitoring, and supervised physical therapy within 24 hours. This continuous post-discharge oversight likely contributed to the absence of major complications, particularly surgical site infections, and to the uniformly high satisfaction levels observed.
Additional strengths include the program’s comprehensive, evidence-based structure encompassing guideline-driven patient selection, full adherence to infection-prevention protocols, and multimodal anesthesia and analgesia strategies. The multidisciplinary collaboration between orthopedics, internal medicine, anesthesiology, and nursing ensured consistency and accountability across all perioperative phases.
Nonetheless, this study has limitations. The sample size is small, reflecting the early stage of program implementation, and the absence of complications in such a cohort should be interpreted cautiously. Longer follow-up and larger cohorts are needed to confirm safety and effectiveness. Furthermore, most patients were ASA II and had adequate home support, which may limit generalizability to higher-risk populations or health systems with fewer resources for coordinated home-based care. While randomized trials may not be feasible within the structure of our program, prospective observational data remain valuable in demonstrating feasibility and informing best practices.
Conclusion
A structured, multidisciplinary outpatient arthroplasty program that embeds home-based recovery as a central safety element can achieve excellent short-term safety, functional, and satisfaction outcomes. This model demonstrates that with rigorous patient selection, infection prevention, and coordinated multidisciplinary care, outpatient shoulder and knee arthroplasty can be safely implemented in medium-complexity settings. It provides a reproducible framework for institutions seeking to expand outpatient surgical capacity without compromising quality or safety.
Conflict of Interest Statement: None.
Funding Statement: None.
Acknowledgements: None.
References
- Allahabadi S, Cheung EC, Hodax JD, Feeley BT, Ma CB, Lansdown DA. Outpatient Shoulder Arthroplasty—A Systematic Review. J Shoulder Elb Arthroplast. 2021;5:247154922110280. doi:10.1177/24715492211028025
- Barra MF, Kaplan NB, Balkissoon R, Drinkwater CJ, Ginnetti JG, Ricciardi BF. Same-Day Outpatient Lower-Extremity Joint Replacement. JBJS Rev. 2022;10(6):1-12. doi:10.2106/JBJS.RVW.22.00036
- Calkins TE, Mosher ZA, Throckmorton TW, Brolin TJ. Safety and Cost Effectiveness of Outpatient Total Shoulder Arthroplasty: A Systematic Review. Journal of the American Academy of Orthopaedic Surgeons. 2022;30(2):e233-e241. doi:10.5435/JAAOS-D-21-00562
- Cozzarelli NF, Longenecker AS, Uhr A, Davis DE, Lonner JH. Unicompartmental Knee Arthroplasty Is Cost-Effective in an Outpatient Setting. Cureus. Published online February 16, 2023. doi:10.7759/cureus.35059
- Kort NP, Bemelmans YFL, van der Kuy PHM, Jansen J, Schotanus MGM. Patient selection criteria for outpatient joint arthroplasty. Knee Surgery, Sports Traumatology, Arthroscopy. 2017;25(9):2668-2675. doi:10.1007/s00167-016-4140-z
- Jenny JY, Gisonni V. Complications of total hip or knee arthroplasty are not significantly more common after ambulatory surgery than after inpatient surgery and enhanced recovery: A case-control study with propensity-score matching. Orthopaedics & Traumatology: Surgery & Research. 2022;108(2):103206. doi:10.1016/j.otsr.2022.103206
- Ponugoti N, Magill H. Safety, efficacy and cost-effectiveness of outpatient versus inpatient joint arthroplasty: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2025;26(1):349. doi:10.1186/s12891-025-08510-5
- Puzzitiello RN, Moverman MA, Pagani NR, Menendez ME, Salzler MJ. Current Status Regarding the Safety of Inpatient Versus Outpatient Total Shoulder Arthroplasty: A Systematic Review. HSS J. 2022;18(3):428-438. doi:10.1177/15563316211019398
- Dong X, Wu CL, YaDeau JT. Clinical care pathways for ambulatory total shoulder arthroplasty. Curr Opin Anaesthesiol. 2022;35(5):634-640. doi:10.1097/ACO.0000000000001174
- Franzoni S, Rossi SMP, Cassinadri A, Sangaletti R, Benazzo F. Perioperative Pain Management in Total Knee Arthroplasty: A Narrative Review of Current Multimodal Analgesia Protocols. Applied Sciences. 2023;13(6):3798. doi:10.3390/app13063798
- Chen Q, Chen E, Qian X. A Narrative Review on Perioperative Pain Management Strategies in Enhanced Recovery Pathways—The Past, Present and Future. J Clin Med. 2021;10(12):2568. doi:10.3390/jcm10122568
- El‐Boghdadly K, Levy NA, Fawcett WJ, et al. Peri‐operative pain management in adults: a multidisciplinary consensus statement from the Association of Anaesthetists and the British Pain Society. Anaesthesia. 2024;79(11):1220-1236. doi:10.1111/anae.16391
- Choi YS, Kim TW, Chang MJ, Kang SB, Chang CB. Enhanced recovery after surgery for major orthopedic surgery: a narrative review. Knee Surg Relat Res. 2022;34(1):8. doi:10.1186/s43019-022-00137-3
- Salamanna F, Contartese D, Brogini S, et al. Key Components, Current Practice and Clinical Outcomes of ERAS Programs in Patients Undergoing Orthopedic Surgery: A Systematic Review. J Clin Med. 2022;11(14):4222. doi:10.3390/jcm11144222
- AAHKS. Outpatient Joint Replacement Position Statement of the American Association of Hip and Knee Surgeons. https://www.aahks.org/position-statements/outpatient-joint-replacement/. 2018. Accessed August 10, 2025.
- Bric JD, Miley EN, Parvataneni HK, et al. Outpatient total hip and knee arthroplasty – Patient expectations versus experience. J Orthop. 2024;51:109-115. doi:10.1016/j.jor.2024.01.014
- Plancher KD, Braun GE, Petterson SC. The outpatient experience in unicompartmental knee arthroplasty: How to perform safely in the ambulatory surgery center. Journal of ISAKOS. 2024;9(6):100350. doi:10.1016/j.jisako.2024.100350
- Danielsen O, Varnum C, Jensen CB, et al. Implementation of outpatient hip and knee arthroplasty in a multicenter public healthcare setting. Acta Orthop. 2024;95:219-224. doi:10.2340/17453674.2024.40185
- Ghoshal S, Salazar C, Duggan J, Howell C, Chen AF, Shah VM. Assessment of Patient Satisfaction and Outcomes After Outpatient Joint Arthroplasty in Academic Medical Centers. Arthroplast Today. 2023;24:101246. doi:10.1016/j.artd.2023.101246
- Ardon AE. Safety Considerations for Outpatient Arthroplasty. Clin Sports Med. 2022;41(2):281-289. doi:10.1016/j.csm.2021.11.005
- Patel O V., Scuderi GR. Update on current enhanced recovery after surgery (ERAS) pathways for hip and knee arthroplasty: a review of the literature. Curr Orthop Pract. 2022;33(2):178-185. doi:10.1097/BCO.0000000000001095
- Morrell AT, Kates SL, Lahaye LA, et al. Enhanced Recovery After Surgery: An Orthopedic Perspective. Arthroplast Today. 2021;9:98-100. doi:10.1016/j.artd.2021.04.019
- Oldrini LM, Sangiorgio A, Nutarelli S, Delcogliano M, Bensa A, Filardo G. Home-Based vs. Conventional Rehabilitation Following Total Knee Arthroplasty. Prosthesis. 2025;7(2):34. doi:10.3390/prosthesis7020034
- Wignadasan W, Haddad FS. Day-case hip and knee arthroplasty: stages of care and the development of an institutional pathway. Br J Hosp Med. 2023;84(12):1-11. doi:10.12968/hmed.2023.0037
- Wignadasan W, Thompson J, Ibrahim M, Kayani B, Magan A, Haddad F. Day-case unicompartmental knee arthroplasty: a literature review and development of a novel hospital pathway. The Annals of The Royal College of Surgeons of England. 2022;104(3):165-173. doi:10.1308/rcsann.2021.0090
- Hoffmann JD, Kusnezov NA, Dunn JC, Zarkadis NJ, Goodman GP, Berger RA. The Shift to Same-Day Outpatient Joint Arthroplasty: A Systematic Review. J Arthroplasty. 2018;33(4):1265-1274. doi:10.1016/j.arth.2017.11.027
- O’Donnell EA, Fury MS, Maier SP, Bernstein DN, Carrier RE, Warner JJP. Outpatient Shoulder Arthroplasty Patient Selection, Patient Experience, and Cost Analyses. JBJS Rev. 2021;9(11):1-9. doi:10.2106/JBJS.RVW.20.00235
- Bemelmans YFL, Keulen MHF, Heymans M, van Haaren EH, Boonen B, Schotanus MGM. Safety and efficacy of outpatient hip and knee arthroplasty: a systematic review with meta-analysis. Arch Orthop Trauma Surg. 2022;142(8):1775-1791. doi:10.1007/s00402-021-03811-5
- Ahmed AF, Hantouly A, Toubasi A, et al. The safety of outpatient total shoulder arthroplasty: a systematic review and meta-analysis. Int Orthop. 2021;45(3):697-710. doi:10.1007/s00264-021-04940-7
- American Academy of Orthopaedic Surgeons. Diagnosis and Prevention of Periprosthetic Joint Infections Evidence-Based Clinical Practice Guideline. https://www.aaos.org/pjicpg. March 11, 2019. Accessed August 20, 2025.
- Malahias MA, Kokkineli S, Gu A, Karanikas D, Kaar SG, Antonogiannakis E. Day case versus inpatient total shoulder arthroplasty: A systematic review and meta-analysis. Shoulder Elbow. 2021;13(5):471-481. doi:10.1177/1758573220944411
- Leroux TS, Zuke WA, Saltzman BM, et al. Safety and patient satisfaction of outpatient shoulder arthroplasty. JSES Open Access. 2018;2(1):13-17. doi:10.1016/j.jses.2017.11.002
- Flurin PH, Abadie P, Lavignac P, Laumonerie P, Throckmorton TW. Outpatient vs. inpatient total shoulder arthroplasty: complication rates, clinical outcomes, and eligibility parameters. JSES Int. 2024;8(3):483-490. doi:10.1016/j.jseint.2023.06.029
- Zhang H, Wang J, Jiang Z, Deng T, Li K, Nie Y. Home-based tele-rehabilitation versus hospital-based outpatient rehabilitation for pain and function after initial total knee arthroplasty: A systematic review and meta-analysis. Medicine. 2023;102(51):e36764. doi:10.1097/MD.0000000000036764
- Goodman D, Ogrinc G, Davies L, et al. Explanation and elaboration of the SQUIRE (Standards for Quality Improvement Reporting Excellence) Guidelines, V.2.0: examples of SQUIRE elements in the healthcare improvement literature. BMJ Qual Saf. 2016;25(12):e7-e7. doi:10.1136/bmjqs-2015-004480
- American Academy of Orthopaedic Surgeons Surgical. Management of Osteoarthritis of the Knee Evidence-Based Clinical Practice Guideline. www.aaos.org/smoak2cpg. December 2, 2022. Accessed August 20, 2025.
- American Association of Hip and Knee Surgeons. Opioids in Total Joint Arthroplasty. https://www.aahks.org/wp-content/uploads/2020/04/Opioids-TJA-Clinical-Guidelines.pdf. March 2020. Accessed August 20, 2025.
- American Association of Hip and Knee Surgeons AS of RA and PMAA of OSTHS and TKS. Anesthesia and Analgesia in Total Joint Arthroplasty. (Endorsed by the American Academy of Orthopaedic Surgeons). https://www.aaos.org/globalassets/quality-and-practice-resources/external-quality-products/anesthesia-and-analgesia-in-total-joint-arthroplasty.pdf. June 14, 2021. Accessed August 20, 2025.
- American Association of Hip and Knee Surgeons. Tranexamic Acid in Total Joint Arthroplasty: The Clinical Practice Guides. (Endorsed by the American Academy of Orthopaedic Surgeons Board of Directors). https://www.aaos.org/globalassets/quality-and-practice-resources/external-quality-products/aahks-transexamic-acid-final.pdf? June 6, 2018. Accessed August 20, 2025.
- ACR/AAHKS. Optimal Timing of Total Hip and Knee Arthroplasty Clinical Practice Guidelines. https://rheumatology.org/indications-for-total-hip-and-knee-arthroplasty-guideline#2023-total-hip-knee-arthroplasty-guideline. 2023. Accessed August 20, 2025.
- AAHKS. Nonsteroidal Anti-Inflammatory Drugs in Total Joint Arthroplasty | Clinical Practice Guidelines. https://www.aahks.org/wp-content/uploads/2020/04/AAHKS-CPG-NSAIDs-Guidelines-in-TJA-March-2020.pdf. March 2020. Accessed August 20, 2025.
- ACR/AAHKS. Perioperative Management Guideline. https://rheumatology.org/perioperative-management-guideline. 2022. Accessed August 20, 2025.
- Grossi P. Enhanced Recovery After Surgery (ERAS) Protocols in Orthopaedic Surgery: Opioids or Not Opioids? J Pain Res. 2025;Volume 18:1683-1695. doi:10.2147/JPR.S496891