





Improving Microbiota to Combat Chronic Inflammation
How to improve microbiota to harness chronic inflammation and prevent cancer, cardiovascular or neurodegenerative diseases? A transversal qualitative review
Donatini Bruno1 and Le Blaye Isabelle1
- Medecine Information Formation (Research). 40 rue du Dr Roux, 51350 Cormontreuil; France
OPEN ACCESS
PUBLISHED: 31 March 2026
CITATION: Donatini, B. and Le Blaye, I., 2026. How to improve microbiota to harness chronic inflammation and prevent cancer, cardiovascular or neurodegenerative diseases? A transversal qualitative review. Medical Research Archives, [online] 14(3).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Background: Dysbiosis should be controlled since it is implicated in metabolic syndrome, cancer occurrence or prognosis, inflammatory bowel diseases, periodontitis, as well as in systemic, neurological, or cardiovascular chronic inflammation. Eradication strategies with antibiotics are in conflict with new proposals of a diversified diet to magnify the diversity of the microbiome. Probiotic use does not meet expectations.
Objective: Reconcile the different and sometimes divergent – medical recommendations. Suggest an integrative and preventive approach that uses as little antibiotic therapy as possible, to improve the flora and to reduce silent chronic inflammation (SCI). Elaborate a simple flow chart to be used in ambulatory practice.
Methods: Identify the most frequent life-threatening diseases associated (bidirectional perspective) with altered microbiota and SCI. Specify the bacteria or viruses involved. Select the most appropriate methods to detect, to quantify and to follow such SCI-associated dysbiosis, in usual and ambulatory practice. Suggest inexpensive and innocuous treatments of SCI induced by dysbiosis. Build a general model that can optimize flora quality and inflammation control, while adapting to current official recommendations.
Results: Cancer, cardiovascular and neurodegenerative diseases are the most prevalent preventable causes of death. They are frequently associated with Fusobacterium nucleatum, Porphyromonas gingivalis, herpes viruses (herpes simplex type 1, Epstein-Barr virus or cytomegalovirus) or human papillomavirus infections. A low diversity of microbiota with low levels of hydrogen sulphide may exacerbate SCI. SCI and dysbiosis can be detected with a breath test, detection of calprotectine and pyruvate kinase M2 in saliva. A simple flow chart may be used in ambulatory practice to control SCI. Treatment with diet, mouth cleaning, tiny amount of essential oils and natural immunostimulating agents could improve the oral and foregut microbiota and therefore SCI.
Conclusion: Cost-effective detection and prevention of SCI could be implemented in usual practice. Its usefulness could be evaluated in a second step according to the figures available in reliable meta-analyses.
Keywords:
- dysbiosis
- Calprotectin
- breath test
- PKM2
List of abbreviations:
- CLP: calprotectin;
- CMV: cytomegalovirus;
- COVID: coronavirus 19;
- EBV: Epstein-Barr virus;
- FN: Fusobacterium nucleatum;
- FODMAP: low fermentable oligosaccharides, disaccharides, monosaccharides and polyols;
- H2O2: hydrogen peroxide;
- H2S: hydrogen sulphide;
- HPV: Human Papillomavirus;
- HSV1/2: herpes simplex virus types 1 or 2;
- IU: international unit;
- NDD: neurodegenerative diseases;
- NLR: neutrophils/lymphocytes ratio;
- NO: nitric oxide;
- PDL1: Programmed death-ligand 1;
- PG: Porphyromonas gingivalis;
- PKM2: Pyruvate kinase M2;
- SCI: Silent chronic inflammation.
Introduction
Silent chronic inflammation (SCI) is implicated in numerous local or systemic diseases. The microbiota is defined as all the micro-organisms living on and in the human body. A pathogenic microbiota – dysbiosis – can harbour inappropriate bacteria, viruses, yeasts or parasites, leading to SCI. Silent chronic inflammation is rarely restricted to a single organ and is rather a wide-spread issue. Therefore, in addition to its main target-organ, SCI frequently also involves the cardiovascular or the central nervous system.
For example, periodontitis is associated with SCI, leading to many severe diseases. It may concern up to 70% of US adults aged 65 years and older and is associated with more than 50 systemic inflammatory disorders and comorbidities, including cancers, neurodegenerative diseases (NDD) or cardiovascular diseases. Causal relationships are not yet established. However a bidirectional effect is currently admitted.
Cancers are largely attributable to at least 30 modifiable risk factors including nine infectious agents accounting for 10.2% of cases, just behind smoking (15.1%), however far ahead alcohol consumption (3.2%). Strengthening efforts to reduce modifiable exposures remain central to global cancer prevention. Alterations in the gut microbiota frequently exist in patients with autoimmunity such as multiple sclerosis, lupus, Sjögren s disease, autoimmune thyroidis, or inflammatory bowel diseases and could contribute to the severity of inflammatory flare-ups. Decreased diversity of microbiota can also be considered as a kind of dysbiosis and is frequently detected in inflammatory diseases, disease, overweight, as well as neutrophilic or eosinophilic diseases.
Many diseases such as Alzheimer s disease, Parkinson s disease or depression – are associated with small intestinal bacterial overgrowth, leaky gut syndrome and vagal-mediated inflammation currently classified as gut-brain axis disorders. Epstein-Barr virus (EBV) and human papillomaviruses (HPV) are known to favour many types of cancers. The association of viruses with bacteria triggers deleterious inflammation. For example, EBV may worsen Helicobacter pylori-induced SCI. EBV, HPV and Helicobacter pylori are the most frequently reported infectious oncogenic germs. There is currently no attempt to identify and list all bacteria and viruses implicated in SCI and subsequently no attempt to treat oral dysbiosis in patients with cancer, cardiovascular, central nervous system or auto-immune diseases. Silent chronic inflammation is usually controlled with systemic and symptomatic anti-inflammatory or immunosuppressive drugs which may induce severe adverse events or favour immunosuppression and consequently opportunistic infections or cancers.
The most frequent recognized types of chronic inflammation are: visceral fat, chronic viral, or bacterial infections (periodontitis or dysbiosis). Etiological treatments of chronic infections – such as control of dysbiosis – should be started as early as possible in order to prevent alterations of specific organs: e.g. joints, heart, arteries, skin, central nervous system, etc.. Any alleviation or control of any type of chronic inflammation should be considered as an appropriate anti-inflammatory therapy, and therefore performed in parallel with classical medical care. In addition, destruction of inappropriate germs may have important consequences on anticancer or antiviral immunity.
For example encouraging results have been reported after the improvement of microbiota due to faecal graft in patients with melanoma, renal carcinoma or non-small cell lung cancer. These improvements are attributed to the destruction of inappropriate bacteria rather than actual implantation of beneficial germs. The severity of SCI is usually not quantified before immunosuppressant therapy and is not evaluated during or after immunosuppressive therapy. More individualised clinical decision-making models should be explored. For example, white blood cell counts and exhaled-nitric oxide (NO) could be taken into account, as well as neutrophils lymphocytes (NLR) ratio.
Efficient, inexpensive and easy-to-use detection tools are now available to physicians who may evaluate dysbiosis and chronic inflammation. Calprotectin (CLP) is a simple and inexpensive marker to detect oral neutrophil-induced inflammation. Saliva CLP is increased in patients with periodontitis. Pyruvate kinase M2 (PKM2) has received increasing attention because of its role in tumour cell energy supply or proliferation, epithelial-mesenchymal transition, invasion and metastasis. Its detection in saliva has been associated with colorectal polyps, dysplasia of the stomach or of the uterine cervix, as well as multiple sclerosis or Parkinson s disease. Hydrogen sulphite (H2S) is a gasotransmitter which could significantly reduce chronic and degenerative diseases especially, brain, cardiovascular or kidney diseases. Inducible-NO is a marker of mucosal inflammation. Exhaled inducible-NO is a recognized marker of asthma, chronic cough or allergic chronic rhinitis. H2S and inducible-NO production, estimated through the H2S and inducible-NO levels in exhaled breath, are associated with CPL level and PKM2 detection. Increasingly precise and numerous guidelines are available to manage bacterial or viral infections, or chronic inflammatory diseases. However, they do not always take into consideration the quality of the microbiota or the respect for the environment. In addition they are specific to one single disease or organ system and they do not take transversal medical issues into consideration: e.g. destruction of diversity of flora after Helicobacter pylori s eradication with an increased risk of multiple sclerosis or Crohn s diseases.
We intended to identify and list the main bacteria and viruses undoubtedly implicated in SCI, as well as in the most frequent and severe life-threatening diseases in Europe. The scope of the study is deliberately as broad as possible since bacteria, virus or visceral fat can involve multiple organs, impair immunity or reach functional systems such as the cardiovascular system, the autonomic nervous system or the endocrine system. As a consequence, the study may include all specific or systemic diseases which have been associated with periodontitis. The approach is integrative and transversal. The red thread of the study is to identify the germs involved in the occurrence of life-threatening diseases associated with usually undiagnosed dysbiosis-induced chronic inflammation. We investigated what could be the place of dietetic advices, sport, antibiotic therapy or antiviral therapy to control chronic dysbiosis and how the currently available recommendations, quality of microbiota and environment could be merged respectfully. We will try to build an algorithm for screening and management in ambulatory medicine that takes into account all the collected elements. In a second time and in a second article, we will try to quantify the possible benefit of such a preventive global integrative approach.
Material and methods
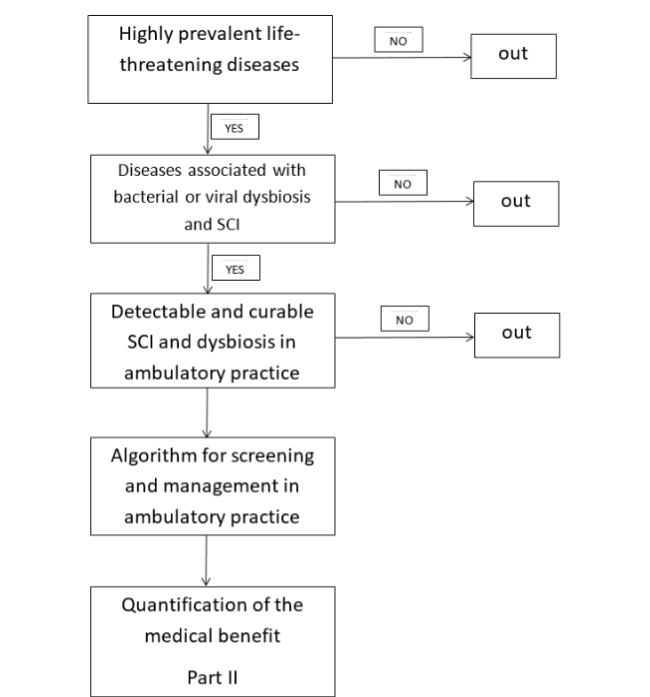
Only medical issues associated with frequent (prevalence >1/10.000) and potentially life-threatening diseases were included. The most recent French and European statistics, from 2022, were used. Only diseases potentially induced by chronic bacterial or viral infections, or gut dysbiosis were included. We searched meta-analysis and review articles in PubMed database. Only recent articles (less than 5 years) were included. The literature search was conducted on February 2026. Only diseases with detectable SCI during usual outpatient medical practice were included. It can be a blood or salivary test, as well as a breath test for the detection of intestinal dysbiosis. Only preventable causes of SCI were considered. Decrease visceral fat (dietetic, physical activity, GLP1 agonists), treatment of periodontitis, treatment of dysbiosis (diet, tiny amount of essential oils, fibres), treatment of viruses such as herpes viruses (valaciclovir, immunostimulating agents), treatment of mycotoxins (decrease intake, inhibitors) will be suggested for each type of dysbiosis. We searched meta-analysis and randomized clinical trials in PubMed database. Only recent articles (less than 5 years) were included. The literature search was conducted on February 2026. The scientific approach will be based on the following steps. See figure 1.
- Identify convincing reviews and/or meta-analyses on the most frequent life-threatening diseases which may be favoured by bacterial or viral dysbiosis.
- Identify convincing reviews and/or meta-analyses on SCI associated with such dysbiosis.
- Identify convincing reviews and/or meta-analyses on easily detectable and curable SCI in ambulatory practice. Infections which could be controlled with current innocuous and inexpensive therapy will be identified.
- Build an algorithm for screening and management of SCI in ambulatory medicine that takes into account all the collected elements. The algorithm should not lead to any lack of screening or management of at-risk condition according to available European guidelines.
Benefits which may be achieved as well as percentages of patients who may be concerned will be quantified in another work (part II).
Results
1. SELECTION OF THE MOST FREQUENT AND SEVERE DISEASES ASSOCIATED WITH SILENT CHRONIC INFLAMMATION AND DYSBIOSIS
The first cause of death in France and Europe is cancer, especially lung, colon-rectum or breast. Lung cancer is mainly attributed to tobacco or microparticles and is poorly influenced by overweight. Some infectious diseases may favour its occurrence such as tuberculosis, or some viruses. For example cytomegalovirus (CMV), EBV and HPV are frequently associated with adenocarcinoma or non-small cell lung cancer. Polyomavirus is also frequently found in lung cancer, as well as hepatitis C virus. A systematic review and meta-analysis demonstrated a significant association between periodontal disease and the incidence of lung cancer. Although further studies are required to eliminate confounding factors, an implication of oral bacteria is possible. Fusobacterium nucleatum (FN) has been particularly implicated.
Since FN, EBV, CMV and HPV are implicated in lung cancer, this disease is selected for this study. Colorectal cancer – occurrence or prognosis – is associated with dysbiosis, in particular with Periodontitis and FN which is now considered as the major drivers of malignant tumorigenesis in the distal colon. Fusobacterium nucleatum is probably also implicated in the occurrence of pancreatic cancer. Periodontitis is associated with the occurrence of colorectal cancer. In gastric cancers, a biphasic course may explain that Helicobacter pylori is found only at early stages of mild mucosal atrophy without dysplasia, whereas FN is found in later stages with dysplastic lesions. Helicobacter pylori infection causes a decreased secretion of stomach acid, making it easier for oral bacteria to colonize the stomach. Solid evidences have revealed the association between oral and gastric commensal microbes other than Helicobacter pylori and the development of gastric cancer. The incidence of gastric cancer is decreasing over time in France and in Europe. The role of Helicobacter pylori is currently debated although eradication guidelines remain similar. A test for Helicobacter pylori infection with a positive result in adults implies an indication of treatment. The decision regarding a possible eradication treatment is therefore made before requesting diagnostic tests. Eradication Guidelines only concern Helicobacter pylori despite the probable role of viruses such as HPV, EBV or CMV. Eradication is based on antibiotic therapy despite the ineluctable antibiotic resistance over time. The eradication recommendations are restricted to patients with atrophic or lymphocytic gastritis or gastric ulcer, malt-lymphoma, or thrombocytopenia. However, Helicobacter pylori-eradication is widely over-prescribed. Periodontitis is associated with gastric cancer. Oral and other digestive cancers – Oesophageal carcinoma is also associated with high levels of FN. Porphyromonas gingivalis (PG) and FN, contribute to oral squamous cell carcinoma progression through mechanisms involving inflammation, epithelial-mesenchymal transition, and immune evasion. Fusobacterium nucleatum is more frequently detected and in higher abundance in oral/head and neck cancer samples when compared to non-cancer samples. Porphyromonas gingivalis could also play an important role in or oral squamous cell carcinoma development and could be involved in three different stages: epithelial-mesenchymal transition, neoplastic proliferation, and tumour invasion. Periodontitis is associated with an increase in oral, oesophageal, pancreatic, hepatic, and in general all digestive cancers. Most of digestive cancers are associated with oral bacteria or viruses (HPV, EBV, CMV and FN) and are therefore selected for further investigation. Helicobacter pylori has only been implicated in some types of gastric cancer, which is infrequent in Europe. Breast cancers have been associated with viruses (EBV, CMV, HPV, mouse mammary tumour virus), especially coinfection with HPV and EBV or aggressive bacteria (FN, PG). Lack of anti-programmed death-ligand 1 (anti-PDL1) effect, attributed to inappropriate intestinal microbiota for example post-antibiotic therapy, is well-established. Control of microbiota has been suggested to improve the efficacy of immunotherapy in oncological treatments.
2. HOW TO DETECT AND QUANTIFY SILENT CHRONIC INFLAMMATION IN AMBULATORY USUAL PRACTICE? PROPOSED ALGORITHM.
Clinical anamnesis and examination This part will not be developed since it relies on basic clinical knowledge. The physician will look for a medical history of cancer, severe viral infections, herpetic flares, herpes zoster, HPV positive cervical smear, cardiovascular clinical signs of allergic, inflammatory or autoimmune diseases: polyarthritis, psoriasis, endometriosis, oral or genital lichen, asthma, chronic obstructive pulmonary disease, overweight with increased waist diameter, as well as periodontitis.
Chronic viral infections The most reliable method would be the detection of replication of virus with quantitative Polymerase Chain Reaction. It is possible in research, for EBV, CMV and HSV1 or HPV in routine. However, it is expensive and time consuming. It cannot be performed in usual practice especially for all previously pointed infectious agents (i.e. FN/PG, oral HPV, CMV or EBV, HSV1), particularly since viruses could be detected only a few days/month despite their implication, as it has been observed in periodontitis. On the contrary oral detection of HPV may spuriously generate anxiety although the virus is most likely transient and is, most of the time, not associated with an increased risk of oral cancer. For example, it appears that there is no established link between chronic HPV infection and oral cancer. The detection of oral HPV is therefore not recommended in usual practice. Therefore, we suggest relying on a meticulous clinical examination and chairside tools. Quantification of inflammation and detection of dysbiosis will complete the screening.
Basic biology For general inflammation Absolute neutrophil count or the Systemic Immune-Inflammation Index, derived from platelet, neutrophil, ×neutrophils/lymphocytes), could be used to evaluate obesity-related inflammation. Systemic Immune-Inflammation Index may better reflect the interplay between systemic inflammation and immune suppression. The NLR and the systemic Immune-Inflammation Index are derived from routine blood tests cost-effective and accessible for resource-constrained settings and capture complementary pathophysiological dimensions: The NLR reflects neuro-inflammation via neutrophil-lymphocyte balance, while SII integrates platelets to reflect inflammation-thrombosis crosstalk. These parameters are predictive of the outcome of stroke. The NLR predicts the cardiovascular outcome in diabetic patients, peripheral artery diseases, depression, inflammatory bowel disease, or patients with cancer. The NLR may serve as a convenient tool in monitoring psoriasis treatment and indicator of systemic inflammation. The NLR may be used to evaluate the risk of hip fracture or of sarcopenia. The NLR may quantify the severity of periodontitis, and is increased in patients with Alzheimer s disease. The NLR is therefore considered in this study. The cut-off value of 2.0 should be assumed as an alert threshold.
For metabolic syndrome Waist circumference or perhaps waist to hip ratio are very good parameters to quantify and follow a metabolic syndrome. It is associated with the global risk of death. A large waist circumference is an independent factor of diabetes type 2.
Detection of dysbiosis
Breath tests could be used for the detection of dysbiosis, especially the dosage of inducible-NO and H2S. We previously suggested that H2S and inducible-NO could be reliably detected for the screening of SCI or oral/foregut dysbiosis in patients with clinical periodontitis. The suggested cut-of values were 0.11 ppm for inducible-NO and 0.10 ppm for H2S.
New markers Salivary calprotectine Calprotectine is mainly synthesized by neutrophils and is a good marker of neutrophil-induced inflammation. Faecal CLP is a recognized marker of inflammatory bowel disease with an established cut-off around 50 international units (IU)/ml. Saliva CLP is increased in periodontitis, and in numerous severe pathologies such as cancer, metabolic syndrome, psoriasis, bone loss, dementia, or cardiovascular diseases, rheumatoid arthritis, inflammatory bowel disease or oral lichen planus. Oral CLP may also be increased in infant with Helicobacter pylori infection. The dosage of CLP in saliva can be carried out during a simple medical consultation. Although the threshold remains to be refined, the salivary CLP could already be recognized as a reliable marker of oral inflammation. Three previous observational studies identified 750 IU/ml as a possible threshold for severe inflammation and 450 IU/ml as a possible threshold for mild inflammation. Therefore, CPL appears to be an excellent new marker for the detection of SCI or to follow the therapeutic response.
Pyruvate kinase M2 (PKM2) Pyruvate kinase M2 is a key enzyme for glycolysis and is closely related to tissue repair and regeneration. The switch to PKM2 modifies the glucose metabolism toward the Warburg effect which favours transformation, invasion, metastasis, and cell proliferation. Pyruvate kinase M2 in stools is a recognized marker of dysplastic polyps of the colon-rectum. Pyruvate kinase M2 switch could also be involved in gastric cancer development. Pyruvate kinase M2 can also be measured in the saliva and is strongly correlated with oral squamous cell carcinoma progression. Pyruvate kinase M2 in saliva is also associated with colorectal polyps, dysplasia of the stomach or of the uterine cervix, as well as multiple sclerosis or Parkinson s disease. There is a clear association between PKM2 detection and high CLP or inducible-NO levels, or low H2S levels. The detection of PKM2 in saliva can also be carried out during a simple medical consultation. It is only qualitative. There is no published information on any quantitative approach in saliva. There is no evidence that a quantitative measure has a medical interest. This measure might be reserved for patients with high levels of CLP in saliva.
Other tests Oral quantitative polymerase chain reaction for oral bacteria or viruses (EBV, CMV, HSV1 or HPV) may be performed. However, no consensus has been yet accepted for their use in routine detection. In addition, they are expensive and cannot help for a quick decision of further screening. Fusobacterium nucleatum or PG may be detected by clinical examination and simple fluorescence, as well as Cutibacterium acnes. Endotest® is a very expansive test which cannot be used in routine ambulatory consultation. In France, Endotest® is only offered to few young women with a strong suspicion of endometriosis. Salivary proteins – such as IL1β, IL6, IL8 or TNF-α – can be used as inflammatory markers of the oral cavity. However none of them can be measured by a simple inexpensive ambulatory test. We therefore suggest relying on a thorough clinical examination with a Wood lamp and a blue light, a breath test, as well as low-cost CLP and PKM2 kits for all outpatients with a history of periodontitis.
Proposed algorithm for the detection of silent chronic inflammation
We previously suggested a practical ambulatory approach in all patients with oral or digestive symptoms in order to detect SCI. See figure 2. First step: Breath test and oral examination should be performed in all patients with abdominal complaints. Second step: Salivary CLP dosage should be performed in all patients with periodontitis and abnormal breath test results. Third step: The detection of PKM2 will be reserved for patients with CLP levels 750 IU/l. This screening is innocuous and inexpensive. It may enable early detection of severe ongoing inflammatory stage and stop there evolution toward cancers, cardiovascular/metabolic or neurodegenerative diseases. It may also have beneficial effects on other severe dysbiosis-associated diseases. For example, FN and PG control may reduce the risk of inflammatory bowel disease, especially of haemorrhagic colitis, of endometriosis, of periodontitis and all associated diseases. The control of viruses may also decrease the risk of transformation of asymptomatic monoclonal gammapathies in myeloma or lymphoma. Joint pain or depression may also be alleviated by the improvement of gut microbiota.
3. IDENTIFICATION OF INNOCUOUS AND INEXPENSIVE THERAPY TO CONTROL SILENT CHRONIC INFLAMMATION. PROPOSED GLOBAL INTEGRATED TREATMENT.
Treatments to be selected should have a very favourable risk/benefit ratio for the patients, for the environment and low cost because they should be used on a long term period, for a large part of the population, without severe life-threatening diseases yet. The treatments should not induce germ-resistance or any destruction of the microbiota which may end to low diversity, decreased immunity or overweight. Goals are entangled: clear periodontitis, reduce visceral fat and improve diversity of microbiota with an increase of NO (without inducible-NO increase) and H2S, as well as PDL1 inhibition. This will decrease chronic inflammation, immunosuppression and chronic systemic damages. The stimulation of immunity will help to control herpes viruses or HPV.
Treatments should act synergically, based on firstly harmless tiny doses, secondly the same narrow target tackled simultaneously, thirdly adapted to a large diversity of situation which represents the diversity of enterotypes, immunotypes and systemic inflammation/organ defects encountered in real life medicine. For all these prerequisites, we try to select natural products, considered as food, spices or aromatic natural products rather than medications or foods complements which may firstly induce adverse events, secondly contain excipients or contaminants and thirdly contain no or low amount of fibres and are devoid of natural beneficial endobiota. Such products should be consumed in tiny amounts on a long term basis. They should fit into a global lifestyle change with diet, brain training, decreased stress and increased physical activity.
Probiotics have failed to control cancer, overweight, cardiovascular diseases, NDD, viral infections. In addition they cannot be considered as natural products.
Clear periodontitis = Control Fusobacterium nucleatum, Porphyromonas gingivalis and herpes viruses Fusobacterium nucleatum and PG are anaerobic bacteria implicated in periodontitis. Periodontitis can be controlled by non-surgical treatment with mechanical mouth cleaning, photobiomodulation, or mouth wash with 1% hydrogen peroxide (H2O2). Hydrogen peroxide is also efficacious against SARS-COV-2 and herpes simplex. Vitamin D supplementation may promote autophagy of PG. We selected personal mechanical mouth cleaning, hydrogen peroxide mouth wash and vitamin D supplementation.
Reduce visceral fat with diet or lipase inhibition Low carb and low caloric diets are necessary to control visceral fat. Diet or the use of medications such as GLP1 agonist will not be discussed here. Intermittent fasting with low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) intake could be suggested. Overweight and visceral fat is associated with decreased microbial diversity. Increased diversity cannot be achieved by destruction of the remaining flora but with diversification of fibres and therefore vegetables. An increased intake of organic vegetables is a well-established recommended diet for body weight, CV diseases or cancer. The intake of fibres is also beneficial in Crohn s disease. Tiny amount of essential oils may decrease the amount of undesirable bacteria and increase diversity. For example, Cinnamomum verum or Origanum vulgare could be efficacious against FN and periodontitis at very low dose.
Oral microbiota produces nitrite leading to the synthesis nitric oxide. Nitric oxide possesses antiviral (SARS-CoV-2, herpes, HPV). Altered endogenic NO production may favour breast or prostatic cancer occurrence. An improvement of diversity will improve the efficacy of PDL1 inhibition. Laetiporus sulphureus or Grifola frondosa are documented inhibitors of lipase. We suggest a low-caloric diet, and low intake of FODMAPs in association with tiny amounts of essential oils such as Origanum vulgare, Cinnamomum verum or Citrus lemon, zinziber officinale in association with either Grifola frondosa (maitake) or Laetiporus sulphureus.
Stimulation of immunity will help to control herpes viruses or human papillomavirus. Coriolus versicolor is a well-documented immunostimulating mushroom. It may increase the survival of patients with adenocarcinoma, especially of the stomach or of the colon. It has anti-viral properties against HPV, EBV, herpes simplex, or even SARS-CoV-2. The association valaciclovir + Coriolus versicolor is associated with a decreased risk of myeloma or lymphoma in asymptomatic monoclonal gammapathy. However the long term use of valaciclovir does not belong to usual recommendations. Coriolus versicolor has also been reported to decrease Alzheimer s disease in a mouse model, and clear prion or intracellular bacteria. It modulates Toll-Like Receptor, and inhibits many mycotoxins. Phellinus linteus could also be a strong immunostimulating agent with anticancer properties. It is efficacious against periodontitis. Ganoderma lucidum could, when added to quercetin, control EBV in mice.
Proposed global integrative treatment with low risk and low cost According to the results, we suggest a very limited number of actions to control SCI. Firstly, mechanical mouth cleaning with hydrogen peroxide mouth wash, Coriolus versicolor +/- Ganoderma lucidum or Phellinus linteus, vitamin D and tiny amounts of essential oils, especially Origanum compactum. Secondly, decrease visceral fat with specific diet, Grifola frondosa, Laetiporus sulphureus and tiny amounts of essential oils, especially Origanum compactum, Cinnamomum verum, Citrus lemon or Zinziber officinale. Thirdly, increase organic food (especially green vegetables and fibres), which probably contains endobiota and natural polyphenols. Please note that food complements do not contain endobiota and cannot increase microbiota diversity. Periodontitis, body weight, waist diameter, NLR, breath test, CLP and when needed PKM2 appear valuable parameters for annual or biannual surveillance.
Discussion
The most frequent causes of death are undisputedly cancers, cardiovascular diseases and neurodegenerative diseases. The currently used classifications may lead to spurious conclusion regarding aetiology. Some diseases are classified according to organs (heart disease), others according to the pathology (cancer), others according to clinical signs (neurodegenerative diseases). In order to prevent disease, it is necessary to tackle the causes. Therefore, an etiological approach is suggested. We focussed on the causes of chronic inflammation, e.g. frequent viral or bacterial infections and/or visceral fat. Tobacco or alcohol abuse, although largely implicated in cancer and cardiovascular diseases does not belong to dysbiosis related causes. The most frequent causes of death are at least partly explained by chronic infections and/or dysbiosis. Surprisingly a very limited number of infectious agents are implicated: few oral bacteria, herpes viruses or HPV, dysbiosis-related visceral fat. According to the Consortium milieu intérieur, the quality of immunity could be evaluated from only three main factors, tobacco, CMV serology and BMI. However, oral inflammation appears to be a corner-stone of SCI and foregut dysbiosis. Periodontitis is associated with silent chronic inflammation and many severe diseases. It may concern up to 70% of US adults aged 65 years and older and is associated with more than 50 systemic inflammatory disorders and comorbidities. Considering that periodontitis treatment or prevention could decrease the frequency and the severity of many systemic infections or chronic diseases, oral evaluation of SCI appears mandatory in all patients. It could start with clinical examination of gums, maybe with the help of a Wood lamp and a blue light.
Oral bacteria build biofilms and conjugate their competence to destroy proteins and to generate permeability, inflammation and immunosuppression leading to excessive repair involving epithelial mesenchymal transition. Viral infections – especially EBV or HPV are able to induce mutations and therefore to increase the risk of tumor.
Global Mechanism of destruction and inflammation. The need of synergic enzymes of deleterious infectious agents
Fusobacterium nucleatum does not possess protease and cannot induce chronic inflammation alone. The destructive process requires proteases from PG or Aggregatibacter actinomycetemcomitans in the mouth or from Gardnerella vaginalis on the cervix to alter the mucosa. This cutting of mucus enables a cross-feeding which supports mutualism. When protease are inhibited, the pathogenic process is disrupted. Aggregatibacter actinomycetemcomitans protects PG from H2O2 produced by commensal beneficial bacteria. Phellinus species are mushrooms which contain strong protease inhibitors, and therefore may protect the gingiva. Coriolus versicolor inhibits Toll-Like-Receptor4 which is a key receptor implicated in oral inflammation induced by anaerobic bacteria. Fusobacterium nucleatum may co-aggregate with Candida albicans, Cutibacterium acnes, or Streptococcus cristatus leading to mutual attenuation of virulence, which promotes a long-term persistence within the oral cavity, especially in endodontic lesions. Long lasting lesions are therefore able to survive to short term treatments. Fusobacterium nucleatum favours the occurrence of HPV-induced intraepithelial neoplasia on the cervix. Fusobacterium nucleatum is able to target sugars of numerous tumours (stomach, prostate, ovary, colon, uterus, pancreas, breast, lung, and oesophagus) and favour tumour spread. Fusobacterium nucleatum in excess is frequently found in patients with severe haemorrhagic colitis. This latter disease dramatically increase the risk of digestive tumours (odd ratio between 3.0 to 6.0).
Table 1: Selected diseases and associated bacterial or viral dysbiosis. Identification of main pathogenic germs to be harnessed in order to control silent chronic inflammation.
| Selected frequent life-threatening diseases | Associated bacterial dysbiosis | Associated viral dysbiosis |
|---|---|---|
| Lung cancer | Tuberculosis | HPV, EBV, CMV, hepatitis C |
| Colorectal, pancreatic, oesophageal cancers | Fusobacterium nucleatum | |
| Gastric cancer | Helicobacter pylori, Fusobacterium nucleatum | HPV, EBV, CMV |
| Oral squamous cell carcinoma | Fusobacterium nucleatum, Porphyromonas gingivalis | HPV |
| Breast cancer | Fusobacterium nucleatum, Porphyromonas gingivalis | HPV, EBV, CMV |
| Prostatic cancer | Fusobacterium nucleatum, Cutibacterium acnes | HPV, HSV1/2, CMV |
| Cervix uterine cancer | Fusobacterium nucleatum | HPV, HSV2, EBV |
| Overweight | Low diversity | CMV, HSV1/2, hepatitis A, adenovirus36 |
| Cardiovascular diseases | Helicobacter pylori, Fusobacterium nucleatum, Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans | EBV, CMV, influenza, SARS-Cov-2 |
| Parkinson | Helicobacter pylori | Hepatitis C |
| Alzheimer/dementia | Porphyromonas gingivalis | HSV1, Herpes zoster ophthalmicus, CMV, hepatitis C, SARS-Cov-2 |
| Cancers, cardiovascular diseases or NDD altogether | Fusobacterium nucleatum, Porphyromonas gingivalis +/- Helicobacter pylori, when Fusobacterium nucleatum and herpes viruses are also involved | HPV, EBV, CMV, HSV1/2 |
2. HOW TO DETECT AND QUANTIFY SILENT CHRONIC INFLAMMATION IN AMBULATORY USUAL PRACTICE? PROPOSED ALGORITHM.
Clinical anamnesis and examination This part will not be developed since it relies on basic clinical knowledge. The physician will look for a medical history of cancer, severe viral infections, herpetic flares, herpes zoster, HPV positive cervical smear, cardiovascular clinical signs of allergic, inflammatory or autoimmune diseases: polyarthritis, psoriasis, endometriosis, oral or genital lichen, asthma, chronic obstructive pulmonary disease, overweight with increased waist diameter, as well as periodontitis.
Chronic viral infections The most reliable method would be the detection of replication of virus with quantitative Polymerase Chain Reaction. It is possible in research, for EBV, CMV and HSV1 or HPV in routine. However, it is expensive and time consuming. It cannot be performed in usual practice especially for all previously pointed infectious agents (i.e. FN/PG, oral HPV, CMV or EBV, HSV1), particularly since viruses could be detected only a few days/month despite their implication, as it has been observed in periodontitis. On the contrary oral detection of HPV may spuriously generate anxiety although the virus is most likely transient and is, most of the time, not associated with an increased risk of oral cancer. For example, it appears that there is no established link between chronic HPV infection and oral cancer. The detection of oral HPV is therefore not recommended in usual practice. Therefore, we suggest relying on a meticulous clinical examination and chairside tools. Quantification of inflammation and detection of dysbiosis will complete the screening.
Basic biology For general inflammation Absolute neutrophil count or the Systemic Immune-Inflammation Index, derived from platelet, neutrophil, ×neutrophils/lymphocytes), could be used to evaluate obesity-related inflammation. Systemic Immune-Inflammation Index may better reflect the interplay between systemic inflammation and immune suppression. The NLR and the systemic Immune-Inflammation Index are derived from routine blood tests cost-effective and accessible for resource-constrained settings and capture complementary pathophysiological dimensions: The NLR reflects neuro-inflammation via neutrophil-lymphocyte balance, while SII integrates platelets to reflect inflammation-thrombosis crosstalk. These parameters are predictive of the outcome of stroke. The NLR predicts the cardiovascular outcome in diabetic patients, peripheral artery diseases, depression, inflammatory bowel disease, or patients with cancer. The NLR may serve as a convenient tool in monitoring psoriasis treatment and indicator of systemic inflammation. The NLR may be used to evaluate the risk of hip fracture or of sarcopenia. The NLR may quantify the severity of periodontitis, and is increased in patients with Alzheimer s disease. The NLR is therefore considered in this study. The cut-off value of 2.0 should be assumed as an alert threshold.
For metabolic syndrome Waist circumference or perhaps waist to hip ratio are very good parameters to quantify and follow a metabolic syndrome. It is associated with the global risk of death. A large waist circumference is an independent factor of diabetes type 2.
Detection of dysbiosis
Breath tests could be used for the detection of dysbiosis, especially the dosage of inducible-NO and H2S. We previously suggested that H2S and inducible-NO could be reliably detected for the screening of SCI or oral/foregut dysbiosis in patients with clinical periodontitis. The suggested cut-of values were 0.11 ppm for inducible-NO and 0.10 ppm for H2S.
New markers Salivary calprotectine Calprotectine is mainly synthesized by neutrophils and is a good marker of neutrophil-induced inflammation. Faecal CLP is a recognized marker of inflammatory bowel disease with an established cut-off around 50 international units (IU)/ml. Saliva CLP is increased in periodontitis, and in numerous severe pathologies such as cancer, metabolic syndrome, psoriasis, bone loss, dementia, or cardiovascular diseases, rheumatoid arthritis, inflammatory bowel disease or oral lichen planus. Oral CLP may also be increased in infant with Helicobacter pylori infection. The dosage of CLP in saliva can be carried out during a simple medical consultation. Although the threshold remains to be refined, the salivary CLP could already be recognized as a reliable marker of oral inflammation. Three previous observational studies identified 750 IU/ml as a possible threshold for severe inflammation and 450 IU/ml as a possible threshold for mild inflammation. Therefore, CPL appears to be an excellent new marker for the detection of SCI or to follow the therapeutic response.
Pyruvate kinase M2 (PKM2) Pyruvate kinase M2 is a key enzyme for glycolysis and is closely related to tissue repair and regeneration. The switch to PKM2 modifies the glucose metabolism toward the Warburg effect which favours transformation, invasion, metastasis, and cell proliferation. Pyruvate kinase M2 in stools is a recognized marker of dysplastic polyps of the colon-rectum. Pyruvate kinase M2 switch could also be involved in gastric cancer development. Pyruvate kinase M2 can also be measured in the saliva and is strongly correlated with oral squamous cell carcinoma progression. Pyruvate kinase M2 in saliva is also associated with colorectal polyps, dysplasia of the stomach or of the uterine cervix, as well as multiple sclerosis or Parkinson s disease. There is a clear association between PKM2 detection and high CLP or inducible-NO levels, or low H2S levels. The detection of PKM2 in saliva can also be carried out during a simple medical consultation. It is only qualitative. There is no published information on any quantitative approach in saliva. There is no evidence that a quantitative measure has a medical interest. This measure might be reserved for patients with high levels of CLP in saliva.
Other tests Oral quantitative polymerase chain reaction for oral bacteria or viruses (EBV, CMV, HSV1 or HPV) may be performed. However, no consensus has been yet accepted for their use in routine detection. In addition, they are expensive and cannot help for a quick decision of further screening. Fusobacterium nucleatum or PG may be detected by clinical examination and simple fluorescence, as well as Cutibacterium acnes. Endotest® is a very expansive test which cannot be used in routine ambulatory consultation. In France, Endotest® is only offered to few young women with a strong suspicion of endometriosis. Salivary proteins – such as IL1β, IL6, IL8 or TNF-α – can be used as inflammatory markers of the oral cavity. However none of them can be measured by a simple inexpensive ambulatory test. We therefore suggest relying on a thorough clinical examination with a Wood lamp and a blue light, a breath test, as well as low-cost CLP and PKM2 kits for all outpatients with a history of periodontitis.
Proposed algorithm for the detection of silent chronic inflammation
We previously suggested a practical ambulatory approach in all patients with oral or digestive symptoms in order to detect SCI. See figure 2. First step: Breath test and oral examination should be performed in all patients with abdominal complaints. Second step: Salivary CLP dosage should be performed in all patients with periodontitis and abnormal breath test results. Third step: The detection of PKM2 will be reserved for patients with CLP levels 750 IU/l. This screening is innocuous and inexpensive. It may enable early detection of severe ongoing inflammatory stage and stop there evolution toward cancers, cardiovascular/metabolic or neurodegenerative diseases. It may also have beneficial effects on other severe dysbiosis-associated diseases. For example, FN and PG control may reduce the risk of inflammatory bowel disease, especially of haemorrhagic colitis, of endometriosis, of periodontitis and all associated diseases. The control of viruses may also decrease the risk of transformation of asymptomatic monoclonal gammapathies in myeloma or lymphoma. Joint pain or depression may also be alleviated by the improvement of gut microbiota.
3. IDENTIFICATION OF INNOCUOUS AND INEXPENSIVE THERAPY TO CONTROL SILENT CHRONIC INFLAMMATION. PROPOSED GLOBAL INTEGRATED TREATMENT.
Treatments to be selected should have a very favourable risk/benefit ratio for the patients, for the environment and low cost because they should be used on a long term period, for a large part of the population, without severe life-threatening diseases yet. The treatments should not induce germ-resistance or any destruction of the microbiota which may end to low diversity, decreased immunity or overweight. Goals are entangled: clear periodontitis, reduce visceral fat and improve diversity of microbiota with an increase of NO (without inducible-NO increase) and H2S, as well as PDL1 inhibition. This will decrease chronic inflammation, immunosuppression and chronic systemic damages. The stimulation of immunity will help to control herpes viruses or HPV.
Treatments should act synergically, based on firstly harmless tiny doses, secondly the same narrow target tackled simultaneously, thirdly adapted to a large diversity of situation which represents the diversity of enterotypes, immunotypes and systemic inflammation/organ defects encountered in real life medicine. For all these prerequisites, we try to select natural products, considered as food, spices or aromatic natural products rather than medications or foods complements which may firstly induce adverse events, secondly contain excipients or contaminants and thirdly contain no or low amount of fibres and are devoid of natural beneficial endobiota. Such products should be consumed in tiny amounts on a long term basis. They should fit into a global lifestyle change with diet, brain training, decreased stress and increased physical activity.
Probiotics have failed to control cancer, overweight, cardiovascular diseases, NDD, viral infections. In addition they cannot be considered as natural products.
Clear periodontitis = Control Fusobacterium nucleatum, Porphyromonas gingivalis and herpes viruses Fusobacterium nucleatum and PG are anaerobic bacteria implicated in periodontitis. Periodontitis can be controlled by non-surgical treatment with mechanical mouth cleaning, photobiomodulation, or mouth wash with 1% hydrogen peroxide (H2O2). Hydrogen peroxide is also efficacious against SARS-COV-2 and herpes simplex. Vitamin D supplementation may promote autophagy of PG. We selected personal mechanical mouth cleaning, hydrogen peroxide mouth wash and vitamin D supplementation.
Reduce visceral fat with diet or lipase inhibition Low carb and low caloric diets are necessary to control visceral fat. Diet or the use of medications such as GLP1 agonist will not be discussed here. Intermittent fasting with low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) intake could be suggested. Overweight and visceral fat is associated with decreased microbial diversity. Increased diversity cannot be achieved by destruction of the remaining flora but with diversification of fibres and therefore vegetables. An increased intake of organic vegetables is a well-established recommended diet for body weight, CV diseases or cancer. The intake of fibres is also beneficial in Crohn s disease. Tiny amount of essential oils may decrease the amount of undesirable bacteria and increase diversity. For example, Cinnamomum verum or Origanum vulgare could be efficacious against FN and periodontitis at very low dose.
Oral microbiota produces nitrite leading to the synthesis nitric oxide. Nitric oxide possesses antiviral (SARS-CoV-2, herpes, HPV). Altered endogenic NO production may favour breast or prostatic cancer occurrence. An improvement of diversity will improve the efficacy of PDL1 inhibition. Laetiporus sulphureus or Grifola frondosa are documented inhibitors of lipase. We suggest a low-caloric diet, and low intake of FODMAPs in association with tiny amounts of essential oils such as Origanum vulgare, Cinnamomum verum or Citrus lemon, zinziber officinale in association with either Grifola frondosa (maitake) or Laetiporus sulphureus.
Stimulation of immunity will help to control herpes viruses or human papillomavirus. Coriolus versicolor is a well-documented immunostimulating mushroom. It may increase the survival of patients with adenocarcinoma, especially of the stomach or of the colon. It has anti-viral properties against HPV, EBV, herpes simplex, or even SARS-CoV-2. The association valaciclovir + Coriolus versicolor is associated with a decreased risk of myeloma or lymphoma in asymptomatic monoclonal gammapathy. However the long term use of valaciclovir does not belong to usual recommendations. Coriolus versicolor has also been reported to decrease Alzheimer s disease in a mouse model, and clear prion or intracellular bacteria. It modulates Toll-Like Receptor, and inhibits many mycotoxins. Phellinus linteus could also be a strong immunostimulating agent with anticancer properties. It is efficacious against periodontitis. Ganoderma lucidum could, when added to quercetin, control EBV in mice.
Proposed global integrative treatment with low risk and low cost According to the results, we suggest a very limited number of actions to control SCI. Firstly, mechanical mouth cleaning with hydrogen peroxide mouth wash, Coriolus versicolor +/- Ganoderma lucidum or Phellinus linteus, vitamin D and tiny amounts of essential oils, especially Origanum compactum. Secondly, decrease visceral fat with specific diet, Grifola frondosa, Laetiporus sulphureus and tiny amounts of essential oils, especially Origanum compactum, Cinnamomum verum, Citrus lemon or Zinziber officinale. Thirdly, increase organic food (especially green vegetables and fibres), which probably contains endobiota and natural polyphenols. Please note that food complements do not contain endobiota and cannot increase microbiota diversity. Periodontitis, body weight, waist diameter, NLR, breath test, CLP and when needed PKM2 appear valuable parameters for annual or biannual surveillance.
Conclusion
Silent chronic inflammation is not due to a single cause, entanglement is almost constant. Several organs are concerned: nervous central system + cardiovascular system + specific organ. A simple flow chart for early detection of dangerous chronic inflammation of the mouth or of the foregut can be applied in ambulatory medicine. We suggest its application in all patients with oral or digestive symptoms. This early detection is essential because treatments to reduce oral inflammation or methods to detect complications are available. Neglecting this simplistic approach could signify heavy loss of chance for a large proportion of the population. However, further studies are required to refine the threshold levels for CPL or H2S/NO levels for example according to the age, underlying vascular conditions or perhaps gastric emptying and gastroesophageal reflux. Long-term observational studies could assess the value of reducing salivary CLP through local care and see the preventive effect of the control of inflammation on gut dysbiosis, body weight, dysplastic mucosal lesions, some cancers, osteoporosis, alveolar bone loss, anxiety-depression episodes, etc.
Conflict of interest:
DFN sarl. Farming business. Production of organic natural flavors
References:
- Asenjo-Lobos C, González L, Bulnes JF, Roque M, Muñoz Venturelli P, Rodríguez GM. Cardiovascular events risk in patients with systemic autoimmune diseases: a prognostic systematic review and meta-analysis. Clin Res Cardiol. 2024; 113(2):246-259. doi:10.1007/s00392-023-02291-4
- Bhagavathula AS, Bentley BL, Woolf B, Dissanayaka TD, Rahmani J. Increased risk of stroke among patients with ankylosing spondylitis: A systematic review and meta-analysis. Reumatol Clin (Engl Ed). 2023;19(3):136-142. doi:10.1016/j.reumae.2023.02.002
- Patrick MT, Li Q, Wasikowski R, et al. Shared genetic risk factors and causal association between psoriasis and coronary artery disease. Nat Commun. 2022;13(1):6565. Published 2022 Nov 2. doi:10.1038/s41467-022-34323-4
- Long S, Chen Y, Meng Y, et al. Peripheral high levels of CRP predict progression from normal cognition to dementia: A systematic review and meta-analysis. J Clin Neurosci. 2023;107:54-63. doi:10.1016/j.jocn.2022.11.016
- Cardisciani M, Di Nicolantonio S, Altamura S, Ortu E, Del Pinto R, Pietropaoli D. Temporal dynamics of early inflammatory markers after professional dental cleaning: a meta-analysis and spline-based meta-regression of TNF-α, IL-1β, IL-6, and (hs)CRP. Front Immunol. 2025;16:1634622. Published 2025 Aug 28. doi:10.3389/fimmu.2025.1634622
- Sulaiman Y, Pacauskienė IM, adzevičienė R, Anuzyte R. Oral and Gut Microbiota Dysbiosis Due To Periodontitis: Systemic Implications and Links to Gastrointestinal Cancer: A Narrative Review. Medicina (Kaunas). 2024;60(9):1416. Published 2024 Aug 29. doi:10.3390/medicina60091416
- Nibali L, Tatarakis N, Needleman I, et al. Clinical review: Association between metabolic syndrome and periodontitis: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2013;98(3):913-920. doi:10.1210/jc.2012-3552
- Dalmády S, Kemény L, Antal M, Gyulai R. Periodontitis: a newly identified comorbidity in psoriasis and psoriatic arthritis. Expert Rev Clin Immunol. 2020;16(1):101-108. doi:10.1080/1744666X.2019.1700113
- Zhang M, Liu Y, Afzali H, Graves DT. An update on periodontal inflammation and bone loss. Front Immunol. 2024;15:1385436. Published 2024 Jun 11. doi:10.3389/fimmu.2024.1385436
- Lee YT, Lee HC, Hu CJ, et al. Periodontitis as a Modifiable Risk Factor for Dementia: A Nationwide Population-Based Cohort Study. J Am Geriatr Soc. 2017;65(2):301-305. doi:10.1111/jgs.14449
- Schulze-Späte U, Wurschi L, van der Vorst EPC, et al. Crosstalk between periodontitis and cardiovascular risk. Front Immunol. 2024;15:1469077. Published 2024 Dec 9. doi:10.3389/fimmu.2024.1469077
- Ferrillo M, Giudice A, Migliario M, et al. Oral-Gut Microbiota, Periodontal Diseases, and Arthritis: Literature Overview on the Role of Probiotics. Int J Mol Sci. 2023;24(5):4626. Published 2023 Feb 27. doi:10.3390/ijms24054626
- Pai SI, Matheus HR, Guastaldi FPS. Effects of periodontitis on cancer outcomes in the era of immunotherapy. Lancet Healthy Longev. 2023;4(4):e166-e175. doi:10.1016/S2666-7568(23)00021-1
- Zhang Z, Wen S, Liu J, et al. Advances in the relationship between periodontopathogens and respiratory diseases (Review). Mol Med Rep. 2024;29(3):42. doi:10.3892/mmr.2024.13166
- Lin EC, Chiang YC, Lin HY, et al. Unraveling the Link between Periodontitis and Coronavirus Disease 2019: Exploring Pathogenic Pathways and Clinical Implications. Biomedicines. 2023;11(10):2789. Published 2023 Oct 14. doi:10.3390/biomedicines11102789
- Fink H, Langselius O, Vignat J, et al. Global and regional cancer burden attributable to modifiable risk factors to inform prevention. Nat Med. Published online February 3, 2026. doi:10.1038/s41591-026-04219-7
- Deng X, Gong X, Zhou D, Hong Z. Perturbations in gut microbiota composition in patients with autoimmune neurological diseases: a systematic review and meta-analysis. Front Immunol. 2025;16:1513599. Published 2025 Feb 6. doi:10.3389/fimmu.2025.1513599
- Wang Y, Wu H, Yan C, et al. Alterations of the microbiome across body sites in systemic lupus erythematosus: A systematic review and meta-analysis. Lupus. 2024;33(12):1345-1357. doi:10.1177/096120332412818891
- Shen Y, Yu X, Wang Q, et al. Association between primary Sjögren’s syndrome and gut microbiota disruption: a systematic review and meta-analysis. Clin Rheumatol. 2024;43(2):603-619. doi:10.1007/s10067-023-06754-x
- Gong B, Wang C, Meng F, et al. Association Between Gut Microbiota and Autoimmune Thyroid Disease: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne). 2021;12:774362. Published 2021 Nov 17. doi:10.3389/fendo.2021.774362
- Sarkar D, Roy P, Saha S. Meta-analysis of faecal microbiome studies followed by machine learning to identify intestinal disease-specific taxonomic signatures. Microb Pathog. 2026;211:108221. doi:10.1016/j.micpath.2025.108221
- Chulenbayeva L, Jarmukhanov Z, Kaliyekova K, Kozhakhmetov S, Kushugulova A. Quantitative Alterations in Short-Chain Fatty Acids in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Biomolecules. 2025;15(7):1017. Published 2025 Jul 15. doi:10.3390/biom15071017
- Wagenaar CA, van de Put M, Bisschops M, et al. The Effect of Dietary Interventions on Chronic Inflammatory Diseases in Relation to the Microbiome: A Systematic Review. Nutrients. 2021;13(9):3208. Published 2021 Sep 15. doi:10.3390/nu13093208
- Spiller AL, Costa BGD, Yoshihara RNY, et al. Ultra-Processed Foods, Gut Microbiota, and Inflammatory Bowel Disease: A Critical Review of Emerging Evidence. Nutrients. 2025;17(16):2677. Published 2025 Aug 19. doi:10.3390/nu17162677
- Starz E, Wzorek K, Folwarski M, et al. The Modification of the Gut Microbiota via Selected Specific Diets in Patients with Crohn’s Disease. Nutrients. 2021;13(7):2125. Published 2021 Jun 22. doi:10.3390/nu13072125
- Wang S, Bao Z, Li Z, Zhao M, Wang X, Liu F. The impact of very-low-calorie ketogenic diets on gut microbiota in individuals with obesity: a systematic review and meta-analysis. Gut Microbes. 2025;17(1):2566305. doi:10.1080/19490976.2025.2566305
- Ojo O, Feng QQ, Ojo OO, Wang XH. The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients. 2020;12(11):3239. Published 2020 Oct 23. doi:10.3390/nu12113239
- Zhao Y, Li L, Zhang W, et al. Associations of indoor airborne microbiome with systemic inflammation in the context of indoor particulate matter pollution and the metabolic mechanisms. J Environ Sci (China). 2026;159:187-198. doi:10.1016/j.jes.2025.04.022
- Barchi A, Massimino L, Mandarino FV, et al. Microbiota profiling in esophageal diseases: Novel insights into molecular staining and clinical outcomes. Comput Struct Biotechnol J. 2023;23:626-637. Published 2023 Dec 27. doi:10.1016/j.csbj.2023.12.026
- Sharma A, Laxman B, Naureckas ET, et al. Associations between fungal and bacterial microbiota of airways and asthma endotypes. J Allergy Clin Immunol. 2019;144(5):1214-1227.e7. doi:10.1016/j.jaci.2019.06.025
- Lin D, Howard A, Raihane AS, et al. Traumatic Brain Injury and Gut Microbiome: The Role of the Gut-Brain Axis in Neurodegenerative Processes. Curr Neurol Neurosci Rep. 2025;25(1):23. Published 2025 Mar 15. doi:10.1007/s11910-025-01410-0
- Braak H, de Vos RA, Bohl J, Del Tredici K. Gastric alpha-synuclein immunoreactive inclusions in Meissner’s and Auerbach’s plexuses in cases staged for Parkinson’s disease-related brain pathology. Neurosci Lett. 2006;396(1):67-72. doi:10.1016/j.neulet.2005.11.012
- Pravin V, Vellapandian C, Naveen Kumar V. The oral-gut-brain axis in periodontitis: microbial signaling in systemic and neuroinflammatory disease. Brain Res. 2026;1875:150168. doi:10.1016/j.brainres.2026.150168
- Zainal Abidin Z, Hein ZM, Che Mohd Nassir CMN, Shari N, Che Ramli MD. Pharmacological modulation of the gut-brain axis: psychobiotics in focus for depression therapy. Front Pharmacol. 2025;16:1665419. Published 2025 Sep 26. doi:10.3389/fphar.2025.1665419
- Karen AA, Elkhalaf AS, Tluli O, et al. Global Prevalence and Cancer Risk of Epstein-Barr Virus and Human Papillomavirus Coinfection in Breast Cancer: A Systematic Review and Meta-Analysis. Viruses. 2025;17(12):1592. Published 2025 Dec 8. doi:10.3390/v17121592
- Bui NN, Huang SC, Tran TNL, et al. Association between Helicobacter pylori and Epstein-Barr virus co-infection and gastric cancer risk: a systematic review and meta-analysis. QJM. 2025;118(8):584-591. doi:10.1093/qjmed/hcaf092
- de Moraes FCA, Wagner PHS, da Silva ABN, Magalhães MCF, Burbano RMR. Does Epstein-Barr Virus Contribute to Breast Cancer Risk Worldwide? A Systematic Review and Meta-Analysis. Clin Breast Cancer. 2026;26(1):229-246.e22. doi:10.1016/j.clbc.2025.07.017
- Yang M, Huo Y, Huang Y, He W, Luo Q, Zhang L. Human papillomavirus (HPV) infection and prevalence of colorectal cancer: an updated systematic review and meta-analysis of global data. Int J Surg. 2026;112(1):1815-1825. doi:10.1097/JS9.0000000000003426
- Cárdenas-Mondragón MG, Carreón-Talavera R, Camorlinga-Ponce M, Gomez-Delgado A, Torres J, Fuentes-Pananá EM. Epstein Barr virus and Helicobacter pylori co-infection are positively associated with severe gastritis in pediatric patients. PLoS One. 2013;8(4):e62850. Published 2013 Apr 24. doi:10.1371/journal.pone.0062850
- Moon S, Choi J, Sung S, et al. Preventable Cancers Caused by Infection in Korea From 2015 to 2030. J Korean Med Sci. 2025;40(26):e143. Published 2025 Jul 7. doi:10.3346/jkms.2025.40.e143
- Collatuzzo G, La Vecchia C, Parazzini F, et al. Cancers attributable to infectious agents in Italy. Eur J Cancer. 2023;183:69-78. doi:10.1016/j.ejca.2023.01.010
- Chupin A, Perduca V, Meyer A, Bellanger C, Carbonnel F, Dong C. Systematic review with meta-analysis: comparative risk of lymphoma with anti-tumour necrosis factor agents and/or thiopurines in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2020;52(8):1289-1297. doi:10.1111/apt.16050
- Wang JL, Yin WJ, Zhou LY, et al. Risk of non-melanoma skin cancer for rheumatoid arthritis patients receiving TNF antagonist: a systematic review and meta-analysis. Clin Rheumatol. 2020;39(3):769-778. doi:10.1007/s10067-019-04865-y
- Sundaram K, Vajravelu LK, Velayutham R, Mohan U. Progression of tuberculosis among patients with rheumatic diseases – A systematic review and meta-analysis. Indian J Tuberc. 2025;72(2):174-182. doi:10.1016/j.ijtb.2023.07.001
- Minozzi S, Bonovas S, Lytras T, et al. Risk of infections using anti-TNF agents in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis: a systematic review and meta-analysis. Expert Opin Drug Saf. 2016;15(sup1):11-34. doi:10.1080/14740338.2016.1240783
- Borren NZ, Ananthakrishnan AN. Safety of Biologic Therapy in Older Patients With Immune-Mediated Diseases: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2019;17(9):1736-1743.e4. doi:10.1016/j.cgh.2018.12.032
- Zalagkitis C, Philippou A, Karatzanos E, Metsios G, Dinas PC. Combined effects of physical activity and diet on chronic inflammation of overweight/obese children and adolescents: A systematic review and meta-analysis. J Sports Sci. 2025;43(22):2841-2857. doi:10.1080/02640414.2025.2561349
- Bulmer C, Avenell A. The effect of dietary weight-loss interventions on the inflammatory markers interleukin-6 and TNF-alpha in adults with obesity: A systematic review and meta-analysis of randomized controlled clinical trials. Obes Rev. 2025;26(7):e13910. doi:10.1111/obr.13910
- Dornas W, Reis JP, Belilo TE, et al. Persistent inflammatory cytokine signature in long Covid-19 patients: a meta-analysis. Inflammopharmacology. 2026;34(1):1-16. doi:10.1007/s10787-025-02033-0
- Mostafaei S, Sayad B, Azar MEF, et al. The role of viral and bacterial infections in the