





Assessment and Training of Central Facial Palsy Post-Stroke
Assessment and Training of Central Facial Palsy Following Stroke: Results from a Nation-Wide Danish Survey
Pernille Nielsen¹, Jesper Fabricius¹²
- Hammel Neurorehabilitation Centre and University Research Clinic, Hammel, Denmark.
- Department of Clinical Medicine, Aarhus University, Aarhus, Denmark.
OPEN ACCESS
PUBLISHED: 31 March 2026
CITATION: Nielsen, P., Fabricius, J., 2026. Assessment and Training of Central Facial Palsy Following Stroke: Results from a Nation-Wide Danish Survey. Medical Research Archives, [online] 14(3).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Background/Objective: Central facial palsy is common following stroke. Although spontaneous alleviation is seen among some individuals, there are still a large proportion who suffer long-lasting consequences. The objective of this study was to investigate the current practice for assessment and training of individuals with central facial palsy in Denmark and thus shed light on potential focus areas for research.
Methods: A national survey among Danish occupational therapists, who according to Danish practice, are responsible for management of central facial palsy. The survey was distributed to members of two professional nation-wide societies.
Results: A total of 211 occupational therapists who worked with central facial palsy completed the survey. The median age was 45, and 52% had >15 years of experience. A total of 59% worked in the municipalities, 37% worked in public hospitals, and 4% worked in private practice. In assessment of central facial palsy, 86% used Facial Oral Tract Therapy, 46% used subjective evaluations concomitantly, while the House-Brackmann and Sunnybrook scales were rarely used. The most common training methods were mimical exercises, which was used by 88% of responders, while neuromuscular electrical stimulation and Kinesio taping were used by 57% and 55% respectively.
Conclusion: Findings showed that current practice for management of central facial palsy lack validated scales, with possibilities for tracking progress. Furthermore, training methods lack scientific evidence, which is a warranted focus area for research. Results are likely generalizable to other countries, since the lack of validated assessment tools and evidence-based training protocols are a global concern.
Keywords: Central Facial Palsy; Stroke; Assessment; National; Survey; Practice.
1.0 Introduction
Central facial palsy (CFP) is a common sequela following stroke, which significantly impacts both functional capacity and psychosocial well-being. CFP arises from upper motor neuron lesions and is classically defined by contralateral weakness in the lower facial muscles, with preservation of upper facial function. Characteristic clinical features of CFP include drooping and uneven smile, often accompanied by drooling, dysarthria and reduced muscle tone on the lips, tongue and pharynx. These impairments further compromise oral motor function, leading to dysphagia. Beyond its somatic presentation, CFP exerts a profound influence on emotional wellbeing, social engagement, and overall quality of life. Research has demonstrated that individuals with CFP experience elevated rates of depression and social anxiety compared to healthy individuals, underscoring the need for consensus on clinical assessment and treatment to alleviate symptoms. While spontaneous recovery occurs in some cases, a substantial proportion of individuals experience persistent long-lasting consequences. However, research on this topic is lacking. Recent research has begun addressing major gaps in post-stroke CFP care, which remains absent from national and international stroke guidelines. Two systematic reviews highlight the lack of standardized assessment and treatment protocols, leading to inconsistent clinical management. Moreover, inconsistent approaches create disparities in care depending on geography and clinician expertise. Accurate assessment and treatment are essential not only for determining prevalence and alleviating physical and psychological burden, but also for evaluating the efficacy of rehabilitation initiatives aimed at reducing CFP-related impairments. Effective management is therefore vital in improving quality of life among stroke survivors. This study aims to address this gap by investigating how Danish occupational therapists assess and train CFP in individuals with stroke, with the goal of enriching the research agenda on CFP.
2.0 Materials and Methods
2.1 DESCRIPTION OF THE QUESTIONNAIRE
A structured online survey on management of CFP was sent to occupational therapists, who according to Danish practice, are responsible for assessment and training of CFP. The survey was distributed in May 2024 to members of two professional nation-wide societies for neurorehabilitation and dysphagia. The survey was inspired by insights from a preceding systematic review, and consisted of 13 questions. Initially, responders were asked about their age and years of professional experience, along with their current professional setting. Respondents were then asked whether they conducted assessment of CFP in individuals with acquired brain injury. Participants who confirmed were subsequently asked to specify which assessment tools they employed. A similar structure was applied to questions regarding interventions. Participants were first asked whether they provided therapeutic training for individuals with CFP, and those who confirmed were asked to indicate which types of therapeutic approaches they used, for example, neuromuscular electrical stimulation (NMES), heat or cold therapy, facial exercises, Kinesio taping, acupuncture, stroking (with a brush or similar), or other techniques. In addition, respondents were asked to report the number of clients with CFP they provided therapy for, as well as the average number of training sessions conducted per client. Finally, the questionnaire included an item where participants rated the extent to which they perceived that training improved clients’ facial palsy.
2.2 DATA PROCESSING AND ANALYSIS
Quantitative data were processed using descriptive statistics in Excel and Stata. Frequencies and percentages were calculated for categorical variables, while continuous variables were summarized using median and interquartile ranges (IQR) to reflect central tendency and variability. Missing responses were excluded from statistical calculations on a per-item basis. Qualitative responses from open-ended questions were analyzed thematically. Recurring concepts and treatment modalities were grouped into categories based on clinical similarity and terminology. This approach enabled the identification of commonly used techniques beyond predefined survey options, providing a richer understanding of clinical practice patterns. The study was exploratory in nature and did not involve hypothesis testing.
3.0 Results
3.1 DESCRIPTION OF OCCUPATIONAL THERAPISTS
A total of 211 occupational therapists who worked with individuals with CFP completed the survey. As seen in table 1, respondents represented a broad spectrum of clinical backgrounds, work settings, and levels of experience in the management of CFP.
| Characteristic | n=211 |
|---|---|
| Age group | 20–29 years 10 (5%) 30–39 years 69 (33%) 40–49 years 72 (34%) 50–59 years 49 (23%) 60+ years 10 (5%) |
| Years of clinical experience | 0–3 years 7 (3%) 4–7 years 23 (11%) 8–11 years 39 (19%) 12–15 years 33 (16%) >15 years 108 (51%) |
| Setting | Municipal rehabilitation 121 (58%) Hospital-based rehabilitation 80 (38%) Private practice 8 (4%) Municipal rehabilitation Day rehabilitation centers 52 (43%) Home rehabilitation 32 (26%) Inpatient rehabilitation units 23 (19%) Other 13 (12%) Hospital-based rehabilitation Acute stroke units 25 (31%) Specialized, severe acquired brain injury 17 (21%) Regional, moderate acquired brain injury 24 (30%) General, mild acquired brain injury 11 (14%) Other hospital settings 3 (4%) Private practice Self-employed 5 (62.5%) Inpatient rehabilitation facility 2 (25%) Missing 1 (12.5%) |
3.2 ASSESSMENT TOOLS USED FOR CFP
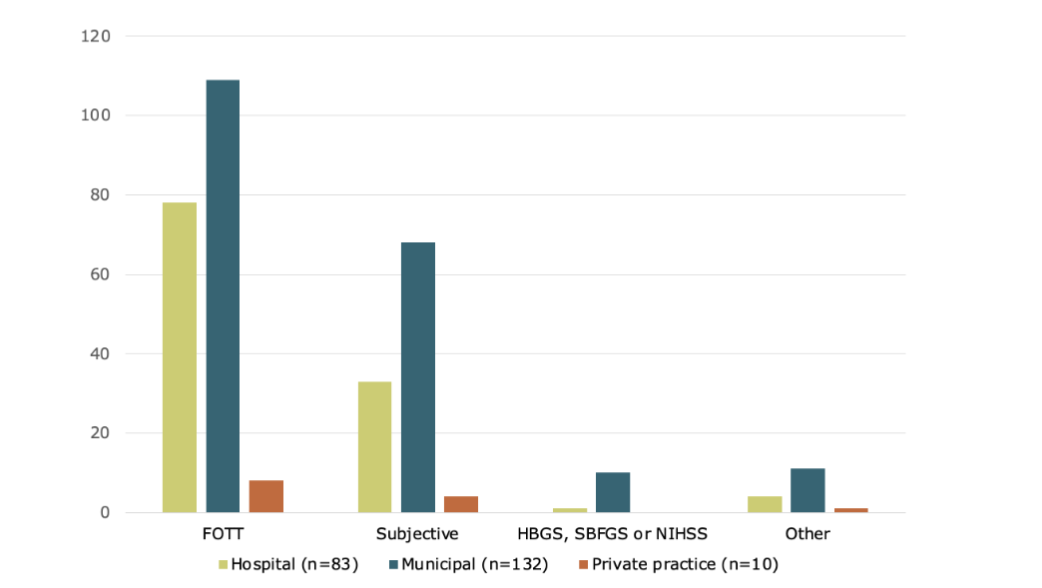
Participants reported using a broad range of assessment tools to evaluate CFP as seen in figure 1. The Facial-Oral Tract Therapy (FOTT) approach was the most frequently used (86%, n=196). Subjective clinical evaluation was also common (46%, n=105). Standardized scales such as the House-Brackmann Scale (HBGS), Sunnybrook Facial Grading Scale (SBFGS), and National Institute of Health Stroke Scale (NIHSS) were rarely applied. A small proportion (7%, n = 17) reported using other tools, including locally developed instruments.
3.3 TREATMENT APPROACHED USED FOR CFP
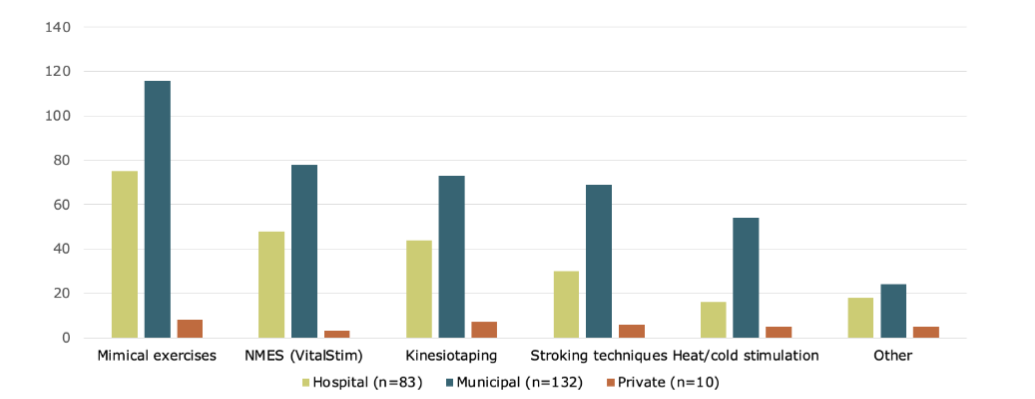
Across all healthcare settings, mimical exercises were the most frequently applied intervention for CFP (88%, n=200) as seen in figure 2. NMES (57.3%, n=130) and Kinesio taping (55%, n=125) were also widely utilized. Stroking techniques (46% n=105) and heat/cold stimulation (33.5%, n=76) were applied more often in municipal settings compared to hospitals.
In addition to the predefined treatment options, a variety of other training modalities were reported (21%, n=47). These approaches reflect a broad spectrum of manual, sensorimotor, and activity-based techniques. Several respondents described working within the FOTT framework, including oral intake training and activity-related training contexts. Manual techniques were frequently mentioned, such as tissue mobilization, myofascial release and mobilization of the facial nerve. The use of neuromuscular oral training devices was also common, alongside oral placement therapy-based interventions such as vibration, inhibition of the unaffected side, and home-based training. Other modalities included craniosacral therapy, mirror therapy, self-training, manual stimulation or dampening, and Castillo Morales techniques. A few respondents described using electric toothbrushes or finger-based vibration stimuli as part of sensory stimulation.
3.4 CLIENT VOLUME AND NUMBER OF SESSIONS
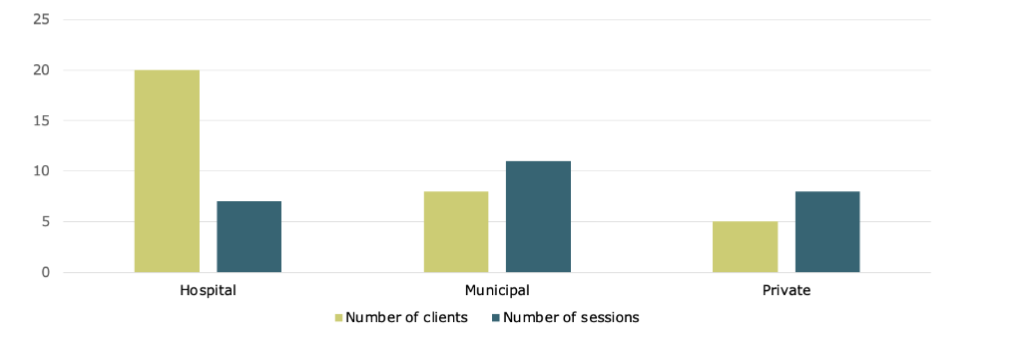
Respondents were asked to estimate both the number of clients with CFP they treated annually, and the average number of training sessions provided per client. The reported median number of clients per year was 10, with an IQR of 5-20. However, few responders reported caseloads exceeding 100 clients per year. The median number of sessions per client was 10, with an IQR of 6-15. As seen in figure 3, hospital-based services had the highest number of clients yet offered relatively few sessions per client. Municipal services showed a more balanced distribution, with fewer clients and more sessions. Private practices in general served few clients annually.
3.5 PERCEIVED EFFECT OF TRAINING
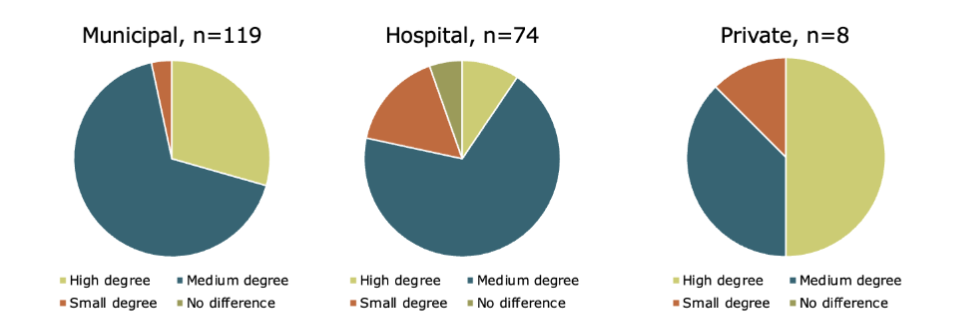
Figure 4 presents the distribution of responses to the question: “To what extent do you perceive that training in CFP improves the clients’ degree of facial palsy?” Across all settings, most respondents reported a medium degree of perceived improvement. In municipal settings, this was followed by high degree, small degree, and a minimal proportion indicating no difference. Hospital-based respondents also predominantly reported a medium degree of improvement, though small degree was slightly more frequent than high degree. Among private practitioners, responses were more evenly distributed between high and medium degree, with no reports of no difference.
4.0 Discussion
The present survey provides a nation-wide overview of occupational therapists’ practices in the assessment and rehabilitation of CFP following stroke, in Denmark. FOTT and subjective evaluation were most widely used in assessment of CFP, while standardized scales were rarely applied. Training methods were diverse, with mimical exercises most frequently used, supplemented by NMES and Kinesio taping. The findings also revealed a high level of variation in client volume, treatment intensity, and perceived effectiveness of training.
The predominance of the FOTT assessment, together with the frequent use of subjective clinical evaluation, reflects a strong reliance on functional, activity-oriented, and hands-on approaches to assessment. Standardized grading scales such as the HBGS and SBFGS, were seldom applied, which is understandable based on the development and validation for clients with peripheral facial palsy rather than CFP. This limited use of formal tools for CFP creates inconsistency in assessment and documentation, making it difficult to compare outcomes across settings or evaluate treatment efficacy systematically.
The high reported use of mimical exercises in treatment indicates that targeted facial movement training constitutes a core component in CFP rehabilitation across settings. NMES, which was applied by more than half of the respondents, still lacks the scientific evidence to support the application for facial palsy, and CFP particularly. There was a broad range of additional modalities reported (mirror therapy, myofascial release, neurodynamic techniques, oral placement therapy, neuromuscular oral training, sensory stimulation, etc.), demonstrating clinical creativity and integration of multimodal methods. At the same time, this diversity underscores the absence of a shared, evidence-based framework for CFP rehabilitation across sectors, resulting in an array of diverse treatment packages shaped by clinician experts in the respective rehabilitation facilities rather than evidence-based and standardized protocols.
The data illustrates marked variation in both the number of clients treated and the number of sessions delivered across settings. Hospital-based therapists reported the highest client volumes, yet provided relatively few sessions per client, consistent with acute and sub-acute rehabilitation. In contrast, municipal and private practitioners treated fewer clients but offered a higher number of sessions per client, consistent with long-term rehabilitation. This disparity highlights the absence of standardized treatment dosage for CFP and suggests that current practice is shaped more by institutional context than by clinical consensus. In this context, the variability in session numbers across settings may reflect broader organizational and resource-related constraints, as has been observed in general stroke rehabilitation research. These workplace differences have practical implications: acute hospital may prioritize screening and brief interventions, whereas municipal services may be better placed to deliver longitudinal, dose-intensive rehabilitation, an important consideration for designing intervention trials and national care pathways. These findings underscore the need for further research into optimal session frequency and outcome evaluation strategies tailored to CFP rehabilitation, particularly approaches that remain feasible across both high- and low-volume service environments.
The findings related to perceived effect should be interpreted with caution. Although respondents across hospital, municipal, and private settings generally reported a medium degree of perceived improvement following training in CFP, these self-reported perceptions provide limited insight into the actual effectiveness of specific interventions. Importantly, the data does not capture which combinations of assessment tools and therapeutic approaches were applied by individual practitioners, nor how these intervention packages were structured or adapted over time. Given the wide range of possible combinations and clinical strategies, it is not possible to attribute perceived improvements to specific components of practice. As such, the results do not allow for meaningful conclusions regarding which interventions are perceived as most relevant or effective. Differences across practice settings should also be interpreted carefully. For example, hospital-based practitioners may have shorter patient contact periods, potentially limiting opportunities to observe functional improvements over time. This may influence perceived relevance and should not be interpreted as an indication of lower clinical effect.
The results of the Danish survey align closely with a UK survey by Eroglu et al. (2025), which similarly reported a predominant reliance on informal, observational assessments and orofacial exercises, with limited use of standardized tools. The findings from both surveys suggest that CFP remains an under-researched and inconsistently managed area, potentially due to the lack of standardized assessment tools and evidence-based treatment protocols. The findings further indicate that validated scales originally developed for PFP are rarely applied in CFP contexts, pointing to a shared gap in the use of outcome measures. The two surveys reveal differences in intervention strategies. UK practice was largely characterized by reliance on clinical observation, whereas Danish practice showed a prevailing use of FOTT as a structured framework for assessment and training. Despite these differences, both contexts demonstrate a limited use of standardized scales originally developed for CFP. The reason for this is that scales and tools for detecting progress and supporting clinical decision-making in CFP are currently lacking. While UK practice is primarily led by speech and language therapists and physiotherapists, Danish practice is dominated by occupational therapists. Despite these professional differences, both surveys reveal a reliance on subjective, hands-on, activity-based and experience-based strategies rather than structured, evidence-based protocols. Taken together, the two surveys provide complementary insights into European practice, pointing to a broader international need for CFP-specific assessment tools and treatment guidelines.
The questionnaire was designed to provide a comprehensive overview of current Danish practices in the management of CFP by collecting demographic background data, quantifiable measures of practice (frequency of interventions, client volumes, session counts), and qualitative input on clinical approaches and perceived barriers. This mixed approach allowed us to 1) characterize the respondent pool, 2) quantify common assessment and treatment choices, and 3) capture clinicians’ perceptions of relevance and effectiveness, information that is essential when proposing practice guidelines or targeted training. Furthermore, such data enhances the generalizability of the findings by allowing comparisons across different healthcare contexts. Emphasis was placed on identifying which assessment tools and treatment options were used. The inclusion of open-ended questions allowed for deeper insights into clinical reasoning and perceived gaps in service provision. Together, these elements facilitate a nuanced understanding of how occupational therapists in Denmark manage CFP, informing both research and development of potential clinical guidelines.
Participants were recruited solely through professional societies on neurorehabilitation and dysphagia, under the Danish Association of Occupational Therapists. This focused recruitment strategy strengthened relevance by targeting clinicians likely to encounter CFP but may also introduce selection bias: therapists outside these professional societies, particularly occupational therapists who are not specialized in neurorehabilitation and/or dysphagia may be under-represented, which could limit the generalizability of the findings. While selection bias cannot be excluded due to the recruitment strategy, it is contextually appropriate given the study’s scope and does not substantially undermine the conclusions regarding specialized neurorehabilitation practices.
Strengths of the study include a large sample size for this clinical area, inclusion of clinicians across sectors, and detailed mapping of assessment and intervention practices. Despite limitations in transferability, the dataset provides a timely and clinically relevant overview of CFP management in Denmark and a strong foundation for future research agendas for CFP.
The findings underscore the need for greater awareness and use of standardized assessment tools, as well as stronger evidence for the efficacy of commonly applied treatment modalities. Given occupational therapists predominant reliance on FOTT and subjective evaluation, assessment and outcome measures specifically adapted to CFP are needed to improve consistency in clinical documentation and research reporting. Standardized tools with sufficient sensitivity to detect intervention-related changes are essential to support clinical decision-making and strengthen evidence-based practice. Combined with interdisciplinary collaboration, such standardization may enhance coherence of care and optimize outcomes across clinical settings. The pronounced differences between healthcare settings further suggest that service models and guidelines should be flexible and context-sensitive, while acute hospital pathways may emphasize screening, early information and short-term interventions, municipal and private rehabilitation services may be better suited to deliver longer and higher-dose interventions. The limited adoption of formalized tools and the widespread uncertainty regarding treatment effects underscore the need for clinical guidelines.
5.0 Conclusions
This study provides a comprehensive overview of current practices in the assessment and rehabilitation of CFP following stroke in Denmark. The findings reveal diverse treatment modalities, and substantial variation in client volume and intervention intensity across settings. The limited use of standardized and validated assessment tools specific to CFP highlight a critical gap in research on CFP. There is a clear need for national guidelines, structured protocols, and targeted evidence-based training and assessment to support therapists across settings. Results from the study are likely generalizable to other countries, since the lack of validated assessment tools and evidence-based training protocols are a global concern.
Author Contributions
Conceptualization; Jesper Fabricius
Methodology; Pernille Nielsen, Jesper Fabricius.
Formal analysis; Pernille Nielsen, Jesper Fabricius.
Investigation; Pernille Nielsen, Jesper Fabricius.
Resources; Jesper Fabricius.
Data curation; Pernille Nielsen, Jesper Fabricius.
Writing—original draft preparation; Pernille Nielsen, Jesper Fabricius
Writing—review and editing; Pernille Nielsen, Jesper Fabricius.
Visualization; Pernille Nielsen, Jesper Fabricius
Supervision; Jesper Fabricius
Project administration; Jesper Fabricius
Funding acquisition; NA
Funding
No external funding was received for this study.
Institutional Review Board Statement
According to Danish legislation this type of study does not require ethical approval.
Informed Consent Statement
No health data are presented, and data presented are anonymized. Therefore, no informed consent for publication is required according to Danish legislation.
Data Availability Statement
The raw data can be made available on reasonable request.
Acknowledgments
We acknowledge the contribution of professional societies to distribute the survey for their participants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Yew KS, Cheng EM. Diagnosis of acute stroke. Am Fam Physician. 2015;91(8):528-536.
- Hotton M, Huggons E, Hamlet C, et al. The psychosocial impact of facial palsy: A systematic review. Br J Health Psychol. 2020;25(3):695-727.
- Pouwels S, Beurskens CHG, Kleiss IJ, Ingels KJAO. Assessing psychological distress in patients with facial paralysis using the Hospital Anxiety and Depression Scale. J Plast Reconstr Aesthet Surg. 2016;69(8):1066-1071.
- Konecny P, Elfmark M, Urbanek K. Facial paresis after stroke and its impact on patients’ facial movement and mental status. J Rehabil Med. 2011;43(1):73-75.
- Dominika Dulak, Imama A. Naqvi. Neuroanatomy, Cranial Nerve 7 (Facial). NationalLibraryofMedicine. July 2023.
- Wongwandee M, Hongdusit K. Analysis of Upper Facial Weakness in Central Facial Palsy Following Acute Ischemic Stroke. Neurol Int. 2025;17(1). doi:10.3390/neurolint17010012
- Fabricius J, Kothari SF, Kothari M. Assessment and rehabilitation interventions for central facial palsy in patients with acquired brain injury: a systematic review. Brain Inj. 2021;35(5):511-519.
- Eroglu HS, Bowen A, Checketts M, Mitchell C. Managing Facial Palsy After Stroke: Results From an Online Survey of Health Professionals. Int J Lang Commun Disord. 2025;60(5). doi:10.1111/1460-6984.70127
- Geschwind N. The Organization of Language and the Brain. Science (1979). 1970;170(3961):940-944. https://doi.org/10.1126/science.170.3961.940.
- Krumhuber EG, Skora LI, Hill HCH, Lander K. The role of facial movements in emotion recognition. Nature Reviews Psychology. 2023;2(5):283-296. doi:10.1038/s44159-023-00172-1
- Konecny P, Elfmark M, Horak S, et al. Central facial paresis and its impact on mimicry, psyche and quality of life in patients after stroke. Biomedical Papers. 2014;158(1):133-137. doi:10.5507/bp.2013.014
- Winstein CJ, Stein J, Arena R, et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169. doi:10.1161/STR.0000000000000098
- Alt Murphy M, Munoz-Novoa M, Heremans C, et al. European Stroke Organisation (ESO) guideline on motor rehabilitation. Eur Stroke J. 2025;10(4):1160-1188. doi:10.1177/23969873251338142
- Vaughan A, Gardner D, Miles A, Copley A, Wenke R, Coulson S. A systematic review of physical rehabilitation of facial palsy. Front Neurol. 2020;11. doi:10.3389/fneur.2020.00222
- Müller D, Meyer-Königsbüscher J. Eating and Drinking – Involves More Than Swallowing. In: Nusser-Müller-Busch R, Gampp Lehmann K, eds. Facial-Oral Tract Therapy (F.O.T.T.): For Eating, Swallowing, Nonverbal Communication and Speech. Springer; 2021:73-114. doi:10.1007/978-3-030-51637-6
- Hägg M, Morris NR. Introducing IQoro: A Clinically Effective Oral Neuromuscular Treatment for Dysphagia. Dysphagia – New Advances. 2021. doi:10.5772/intechopen.101144
- Castillo-Morales R. Die Orofaziale Regulationstherapie. München: Pflaum Verlag; 1998.
- House JW, Brackmann DE. Facial nerve grading system. Otolaryngology – Head and Neck Surgery. 1985;93(2):146-147. doi:10.1177/019459988509300202
- Ross BG, Fradet G, Nedzelski JM. Development of a Sensitive Clinical Facial Grading System. Otolaryngology–Head and Neck Surgery. 1996;114(3):380-386. doi:10.1016/s0194-59989670206-1
- Guarin DL, Yunusova Y, Taati B, et al. Toward an Automatic System for Computer-Aided Assessment in Facial Palsy. Facial Plast Surg Aesthet Med. 2020;22(1):42-49.
- Yoo MC, Kim JH, Kim YJ, et al. Effects of Electrical Stimulation on Facial Paralysis Recovery after Facial Nerve Injury: A Review on Preclinical and Clinical Studies. J Clin Med. 2023;12(12). doi:10.3390/jcm12124133
- Veerbeek JM, Van Wegen E, Van Peppen R, et al. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS One. 2014;9(2). doi:10.1371/journal.pone.0087987