






Chronic Respiratory Diseases in South-East Asia: Overview
Burden, risk factors, and health system response to chronic respiratory diseases in the WHO South-East Asia Region
Aereosonova Khongsit¹, Pradeep Joshi¹, Nalika Gunawardena¹
- WHO Regional Office for South East Asia
[email protected]
OPEN ACCESS
PUBLISHED: 31 March 2026
CITATION: Khongsit, A., Joshi, P., and Gunawardena, N., 2026. Burden, risk factors, and health system response to chronic respiratory diseases in the WHO South-East Asia Region. Medical Research Archives, [online] 14(3).
https://doi.org/10.18103/mra.v14i3.7259
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v14i3.7259
ISSN 2375-1924
ABSTRACT
Background: Chronic respiratory diseases (CRDs), particularly chronic obstructive pulmonary disease (COPD) and asthma, are among the leading noncommunicable diseases (NCDs) in the WHO South-East Asia Region. They cause significant morbidity, mortality, and economic loss. While substantial attention has been given to cardiovascular diseases and cancer, CRDs in low- and middle-income countries remain under-prioritized.
Objective: To provide a comprehensive overview of the burden of chronic respiratory diseases, associated risk factors, projected economic impact, and health system responses in the WHO South-East Asia Region.
Methods: The analysis is based primarily on the data of the Global Burden of Disease (GBD) 2021 and published WHO data sources. A set of key indicators were identified to reflect the different aspects of the status of chronic respiratory diseases to be presented and secondary analysis was conducted to reflect the status of the 10 South-East Asia countries.
Results: In 2021, chronic respiratory diseases affected an estimated 84.03 million people in the Region (pooled prevalence 4.8%). Chronic obstructive pulmonary disease accounted for 45.04 million cases and asthma for 40.31 million. Mortality exceeded 1.46 million deaths, with disproportionately higher rates among women in several countries, which may be attributable, at least in part, to higher exposure to household air pollution. Disability-adjusted life year (DALY) rates for chronic obstructive pulmonary disease ranged from 411 per 100,000 population in Maldives to 2,283 in the Democratic People’s Republic of Korea. Major risk factors—including tobacco use (up to 37%), PM₂.₅ pollution (up to 9× WHO guideline levels), and reliance on polluting fuel (up to 89%)—remain widespread. The projected economic losses between 2020 and 2050 exceed INT$ 584 billion, with India alone accounting for INT$ 418 billion. Availability of spirometry and essential inhaled medicines at the primary care level remains limited across the Region.
Conclusion: Chronic respiratory diseases represent a major and under-recognised public health and economic challenge in the WHO South-East Asia Region. Comprehensive action integrating tobacco control, clean cooking initiatives, air quality management, and strengthened primary care services is urgently needed to reduce the morbidity, premature mortality, and economic losses.
Keywords
Chronic respiratory diseases, COPD, asthma, South-East Asia, mortality, DALY, tobacco, air pollution, WHO.
INTRODUCTION
Chronic respiratory diseases (CRDs) are a group of non-infectious conditions that commonly affect the lungs and airways. They are among the four major noncommunicable diseases prioritized in global health agendas. The most common among CRDs are chronic obstructive pulmonary disease (COPD), asthma and occupational lung diseases (e.g. silicosis, asbestosis). Chronic respiratory diseases are a major cause of morbidity and mortality both globally and in the World Health Organization (WHO) South-East (SE) Asia Region; it is a key public health concern, contributing to millions of deaths and disabilities each year.
Based on WHO Global Health Estimates 2021, an estimated 1.46 million deaths were caused by chronic respiratory diseases, with a higher number reported among women (769,247), compared with men (690,855). It is estimated that around 37% of all CRD deaths occur below the age of 70 years, accounting for approximately 0.58 million deaths globally and are projected to increase due to aging populations, persistent tobacco use, air pollution, and occupational exposures. Most CRDs share common risk factors as their aetiology and are not curable; however, various forms of treatment that help open the air passages and improve shortness of breath can help control symptoms and improve daily life for people living with these conditions. Multiple risk factors are known to contribute to the development of CRDs. The primary risk factors for CRDs fall into environmental, behavioural and metabolic categories. Family history of asthma is also a recognized risk factor. Despite CRDs’ substantial contribution to premature mortality and long-term disability, the conditions have historically received limited programmatic attention.
The WHO South-East Asia Region, comprising 10 diverse countries, is home to over a quarter of the global population. Namely, the 10 countries are Bangladesh, Bhutan, Democratic People’s Republic of Korea (DPR Korea), India, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor-Leste. Seven countries- Bangladesh, Bhutan, India, Nepal, Myanmar, Sri Lanka and Timor-Leste are classified as lower-middle income countries while Democratic People’s Republic of Korea is classified as a low-income country. Chronic respiratory diseases represent a growing public health concern in the WHO South-East Asia Region. The region is exposed to several established risk factors for CRD, including ambient particulate matter 2.5 (PM2.5), air pollution and the use of polluting fuels for household cooking. Addressing CRDs also requires health systems to support early detection and long-term management through components such as access to spirometry, availability of essential medicines, and strong primary care based service delivery.
The present article aims to provide a comprehensive overview of the burden of chronic respiratory diseases and the status of related prevention and management services in the South-East Asia Region and identify patterns and drivers, and assess current health system responses. This analysis has relevance beyond the region; offering insights applicable to other low-and-middle income countries contexts and to global chronic respiratory diseases strategies.
METHODS
Publicly available, published data sources were used to describe the epidemiology of CRDs, associated risk factors, and selected health system indicators across ten countries in the WHO South-East Asia Region. A scoping review was conducted to ensure a comprehensive and accurate assessment of the available regional evidence. Data were extracted from the Global Burden of Disease (GBD) Study 2021 for estimates of CRD prevalence, incidence, mortality, and disability-adjusted life years (DALYs), disaggregated by disease and age group; WHO Global Health Estimates mortality data (2021); WHO databases on tobacco use, household air pollution, and PM2.5 exceedance; and country-reported health system data from the WHO Noncommunicable disease Country Capacity Survey (2023). Additional information was drawn from national surveys and published pooled estimates for comparative purposes. The indicators assessed were organised into four domains. Disease burden indicators included prevalence (percentage and number of cases), incidence (per 100,000 population), mortality (age-standardized per 100,000 population), and DALYs. Risk factor burden indicators comprised the prevalence of key CRD-related risk factors, including tobacco use, household air pollution exposure, and ambient PM2.5 exposure. Economic impact indicators included estimated economic costs expressed in international dollars. Health system response indicators covered selected system-level measures relevant to CRD prevention, diagnosis, and management drawing on available country-reported data. All indicators were disaggregated by sex and country where data were available.
RESULTS
According to GBD 2021, the prevalence of CRDs in the Region, which include COPD, asthma, interstitial lung disease and pulmonary sarcoidosis, pneumoconiosis and other less common respiratory conditions, was estimated at 4.8% in 2021 for both sexes combined.
| Country | CRD | COPD | Asthma |
|---|---|---|---|
| Bangladesh | 6853000 (4.29%) | 4020100 (2.52%) | 2869000 (1.8%) |
| Bhutan | 28000 (3.86%) | 16900 (2.32%) | 11300 (1.56%) |
| DPR Korea | 1898000 (7.5%) | 879500 (3.48%) | 1068900 (4.23%) |
| India | 66761000 (4.81%) | 35819800 (2.58%) | 32054600 (2.31%) |
| Maldives | 16000 (3.27%) | 8200 (1.65%) | 7800 (1.56%) |
| Myanmar | 2260000 (4.11%) | 1295500 (2.36%) | 983000 (1.79%) |
| Nepal | 1188000 (3.95%) | 710500 (2.36%) | 485100 (1.61%) |
| Sri Lanka | 1263000 (5.87%) | 495500 (2.3%) | 808000 (3.75%) |
| Thailand | 3702000 (5.7%) | 1781000 (2.74%) | 1977600 (3.04%) |
| Timor-Leste | 62000 (4.52%) | 19700 (1.45%) | 42100 (3.11%) |
Based on the estimates of GBD 2021 for countries in the Region, the highest prevalence of CRDs was observed in the Democratic People’s Republic of Korea, which stood at 7.5%, while Maldives recorded the lowest prevalence at 3.27%. In terms of absolute numbers, India had the highest number of CRD cases (66.76 million), whereas Maldives had the fewest (16,000 cases).
The total number of asthma cases was estimated at 40.31 million. The distribution pattern of asthma prevalence closely mirrored that of overall CRDs, with DPR Korea recording the highest rate (4.23%) and Bhutan and Maldives the lowest (1.56%). Chronic obstructive pulmonary disease cases were estimated at 45.05 million in the Region, slightly surpassing the number of asthma cases.
In WHO South-East Asia region, CRD account for approximately 12% of all deaths. The two primary conditions ‒ chronic obstructive pulmonary disease and asthma ‒ contribute significantly to disability, premature mortality and economic burden across the Region.
Country-level analysis using Global Health Estimates 2021 shows substantial heterogeneity in COPD mortality across the WHO South-East Asia Region. In 2021, COPD ranked among the top five causes of death in seven of ten countries, compared with four countries in 2000, reflecting a substantial rise in the relative importance of COPD as seen in Table 2.
| Country | Rank 2000 | Rank 2021 |
|---|---|---|
| Bangladesh | 8 | 5 |
| Bhutan | 4 | 2 |
| DPR Korea | 6 | 4 |
| India | 5 | 3 |
| Maldives | 3 | 4 |
| Myanmar | 4 | 5 |
| Nepal | 4 | 4 |
| Sri Lanka | 4 | 4 |
| Thailand | 7 | 10 |
| Timor-Leste | Not in top 10 | 5 |
Among chronic respiratory diseases, COPD emerged as the leading cause of death, accounting for approximately 1.16 million deaths ‒ 589,787 among women and 569,241 among men. Asthma was responsible for 229,885 deaths, with significantly higher mortality among women (141,773) than among men (88,112).
| Country | CRD | COPD | Asthma | Other respiratory diseases |
|---|---|---|---|---|
| Bangladesh | 34359 (Male), 30443 (Female) | 28176 (Male), 23055 (Female) | 4144 (Male), 5633 (Female) | 2039 (Male), 1755 (Female) |
| Bhutan | 215 (Male), 234 (Female) | 183 (Male), 188 (Female) | 22 (Male), 35 (Female) | 10 (Male), 10 (Female) |
| DPR Korea | 15076 (Male), 17206 (Female) | 14243 (Male), 16275 (Female) | 602 (Male), 804 (Female) | 230 (Male), 127 (Female) |
| India | 587407 (Male), 672349 (Female) | 482793 (Male), 513568 (Female) | 74872 (Male), 124805 (Female) | 29742 (Male), 33980 (Female) |
| Maldives | 143 (Male), 125 (Female) | 116 (Male), 105 (Female) | 15 (Male), 11 (Female) | 13 (Male), 9 (Female) |
| Myanmar | 20467 (Male), 18697 (Female) | 16421 (Male), 13415 (Female) | 3752 (Male), 4767 (Female) | 290 (Male), 515 (Female) |
| Nepal | 11557 (Male), 15648 (Female) | 9487 (Male), 12199 (Female) | 1483 (Male), 2711 (Female) | 590 (Male), 738 (Female) |
| Sri Lanka | 6533 (Male), 5961 (Female) | 5357 (Male), 4649 (Female) | 886 (Male), 997 (Female) | 290 (Male), 314 (Female) |
| Thailand | 14851 (Male), 8386 (Female) | 12277 (Male), 6201 (Female) | 2283 (Male), 1951 (Female) | 292 (Male), 234 (Female) |
| Timor-Leste | 247 (Male), 198 (Female) | 188 (Male), 132 (Female) | 53 (Male), 59 (Female) | 5 (Male), 6 (Female) |
In 2021, India recorded the highest number of deaths attributed to CRDs, totalling 1.25 million, of which 672,349 were among women and 587,407 among men. In contrast, Maldives reported the lowest CRD mortality, with only 268 deaths (143 men, 125 women). Notably, female mortality surpassed male mortality in several countries, including Bhutan, Democratic People’s Republic of Korea, India and Nepal. This pattern is unusual, as globally, COPD mortality tends to be higher among men. The higher female mortality in these countries likely reflects high exposure to household air pollution, particularly from use of solid fuels for cooking in poorly ventilated homes.
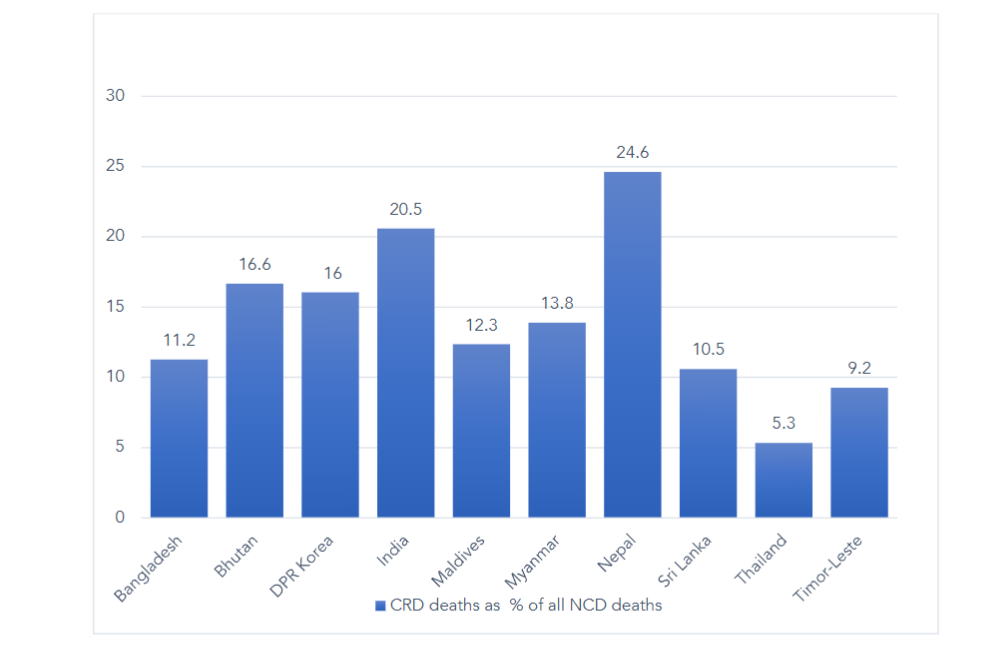
The proportionate mortality from chronic respiratory diseases also varies across the countries. Chronic respiratory diseases contribute to 24.6% of all noncommunicable disease deaths in Nepal, which is the highest, and account for 5.3% of all NCD deaths in Thailand, which is the lowest.
| Country | DALY rate per 100 000 (both sexes), 2021 |
|---|---|
| Bangladesh | 1040.9 (COPD), 270.8 (Asthma) |
| Bhutan | 1264.6 (COPD), 262.0 (Asthma) |
| DPR Korea | 2283.8 (COPD), 279.7 (Asthma) |
| India | 1698 (COPD), 426.9 (Asthma) |
| Maldives | 411.0 (COPD), 117.3 (Asthma) |
| Myanmar | 1524.7 (COPD), 569.1 (Asthma) |
| Nepal | 1961.4 (COPD), 471.5 (Asthma) |
| Sri Lanka | 984.5 (COPD), 327.5 (Asthma) |
| Thailand | 731.3 (COPD), 247.3 (Asthma) |
| Timor-Leste | 605.2 (COPD), 382.2 (Asthma) |
The disability-adjusted life years for both COPD and asthma vary considerably across countries in the WHO South-East Asia Region, reflecting differences in disease burden, health care access and underlying risk exposures. Democratic People’s Republic of Korea has the highest COPD DALY rate (2283.8), indicating a significant burden of disability and premature mortality while Maldives has the lowest (411).
| Country | Exceedance of WHO (PM2.5) guidelines (by a multiple of) (2020) | Prevalence of current tobacco smoking among adults aged 15+ years (2022) | Primary reliance on polluting fuels and technology (%) (2020) |
|---|---|---|---|
| Bangladesh | 9 | 18 | 75 |
| Bhutan | 5 | 6 | 20 |
| DPR Korea | 8 | 17 | 89 |
| India | 9 | 7 | 32 |
| Maldives | 3 | 23 | 1 |
| Myanmar | 5 | 20 | 69 |
| Nepal | 7 | 16 | 65 |
| Sri Lanka | 5 | 9 | 68 |
| Thailand | 5 | 19 | 16 |
| Timor-Leste | 7 | 32 | 65 |
Significant differences in exposure patterns can be seen when comparing the key CRD risk variables among the countries in the WHO South-East Asia Region. Bangladesh, India, and Democratic People’s Republic of Korea have some of the highest WHO PM2.5 exceedances. Bangladesh, DPR Korea, Myanmar, Nepal, Sri Lanka, and Timor-Leste continue to have high levels of reliance on polluting household fuels. In Timor-Leste, Maldives, and Myanmar, tobacco usage is significantly higher, which increases the risk of chronic respiratory diseases. Due to limited studies in the Region, the prevalence of occupational exposure to airborne particulate matter in the Region is difficult to assess.
| Country | Total economic loss (billion INT$) | Proportion of GDP (%) | Per capita Loss (INT$) |
|---|---|---|---|
| Bangladesh | 28.84 (25.50–42.28) | 0.064 (0.056–0.094) | 158 (140–232) |
| Bhutan | 0.33 (0.20–0.55) | 0.106 (0.065–0.175) | 388 (237–643) |
| DPR Korea | 2.33 (1.90–2.88) | 0.190 (0.155–0.236) | 88 (71–108) |
| India | 417.96 (295.69–557.05) | 0.100 (0.071–0.133) | 272 (192–362) |
| Maldives | 0.16 (0.12–0.22) | 0.059 (0.042–0.081) | 300 (215–410) |
| Myanmar | 9.86 (7.83–11.87) | 0.112 (0.089–0.135) | 166 (132–200) |
| Nepal | 5.56 (3.51–8.25) | 0.125 (0.079–0.185) | 165 (104–245) |
| Sri Lanka | 7.14 (4.45–11.52) | 0.086 (0.054–0.139) | 325 (202–524) |
| Thailand | 15.20 (11.28–20.78) | 0.043 (0.032–0.059) | 220 (163–300) |
| Timor-Leste | 0.10 (0.07–0.14) | 0.088 (0.062–0.120) | 61 (43–84) |
Treatment costs for CRDs, encompassing both inpatient and outpatient medical expenses, represent a significant component of the overall economic burden associated with these conditions. A modelling study, which accounted for the disease burden, loss of productivity, absenteeism and diversion of household resources towards out-of-pocket health-care expenditures, estimated the total macroeconomic loss due to COPD in the WHO South-East Asia Region to be INT$ 584 billion over the period of 2020–2050, using a 3% discount rate. International dollars (INT$) were used to enable purchasing power parity-adjusted comparison of economic losses across countries.
| Country | Availability of medicines needed for the treatment of chronic respiratory diseases at the primary health care facilities of the public sector in the WHO South-East Asia Region, 2023 |
|---|---|
| Bangladesh | Steroid inhaler, Combination budesonide-formoterol inhaler, Bronchodilator inhaler, Nicotine replacement therapy, Tobacco cessation aids (e.g. bupropion, varenicline) |
| Bhutan | Generally available: at 50% or more pharmacies |
| DPR Korea | Generally available: at 50% or more pharmacies |
| India | Generally not available: at less than 50% of the pharmacies |
| Maldives | Generally available: at 50% or more pharmacies |
| Myanmar | Generally available: at 50% or more pharmacies |
| Nepal | Generally available: at 50% or more pharmacies |
| Sri Lanka | Generally available: at 50% or more pharmacies |
| Thailand | Generally available: at 50% or more pharmacies |
| Timor-Leste | Generally available: at 50% or more pharmacies |
According to the WHO Noncommunicable diseases Country Capacity Survey 2023, steroid inhalers were reported to be generally available at more than 50% of the pharmacies at the public-sector primary health care facilities in six countries: Bhutan, Democratic People’s Republic of Korea, Maldives, Myanmar, Sri Lanka and Timor-Leste.
The combination inhaler of budesonide-formoterol was reported to be generally available at over 50% of the public-sector pharmacies in Democratic People’s Republic of Korea, Maldives and Myanmar. Bronchodilator inhalers were reported as generally available at more than 50% of the public primary health care pharmacies in all countries, except Bangladesh and Nepal. Despite progress in listing essential CRD medicines, systemic barriers remain across the Region, particularly around affordability, supply chain reliability and rational prescribing. Inhaler technique is often poorly taught and adherence support remains limited, especially in rural and underserved populations, resulting in suboptimal treatment outcomes.
DISCUSSION
The WHO South-East Asia Region faces a dual challenge: a high burden of CRDs driven by largely preventable risk factors, alongside limited health system capacity to respond effectively. The predominance of chronic obstructive pulmonary disease and asthma within national morbidity profiles, combined with their close link to environmental determinants such as biomass fuel use, household air pollution, and air quality, highlights the urgent need for integrated policies that address both noncommunicable disease control and environmental health.
The findings of this article highlight a substantial and multi-faceted burden of chronic respiratory diseases in the Region. With over 84 million affected individuals and more than 1.46 million deaths annually, these conditions represent not only a clinical challenge but also a systemic public health concern.
One notable finding is the higher mortality among women in several countries. Globally, chronic obstructive pulmonary disease mortality is typically higher among men, largely due to higher smoking prevalence. However, in parts of the South-East Asia, women experience disproportionately high exposure due to household air pollution from solid fuel combustion in poorly ventilated homes. This pattern emphasises the importance of addressing gendered environmental risk exposures in policy design.
The heterogeneity in disability-adjusted life year rates across countries suggests that difference in exposure intensity, early diagnosis, access to treatment, and health system performance significantly influence outcomes.
The projected macroeconomic loss of INT$ 584 billion between 2020 and 2050 illustrates the long-term productivity impact of chronic respiratory diseases. These losses arise from premature mortality, workforce attrition, reduced labour productivity, and diversion of household resources toward out-of-pocket expenditure. Framing chronic respiratory diseases as both a health and macroeconomic issue may strengthen political prioritization.
Health system response remains uneven. Although many countries report availability of essential inhaled medicines in primary care settings, access to spirometry, a critical diagnostic tool for chronic obstructive pulmonary disease, remains limited. Without early diagnosis, disease progression continues unchecked, resulting in avoidable hospitalizations and long-term disability.
Experiences from other regions show that integrating standardized clinical pathways into primary health care, ensuring consistent medicine supply, embedding services with universal health coverage benefit packages, and strengthening surveillance systems are associated with improved disease control.
The findings in this article align with evidence from other WHO regions, particularly the WHO European Region, where CRDs are understood to arise from the interaction of environmental, behavioural, and health system determinants rather than from isolated risk factors alone. The WHO European Respiratory Health report highlighted that tobacco use, ambient and household air pollution, and occupational exposures remain central drivers of CRD burden, while delayed diagnosis, fragmented care pathways, and insufficient continuity of long-term management contribute to avoidable morbidity, mortality, and economic losses. Experiences from the European Region further showed that countries reporting more favourable CRD outcomes have emphasised integrated system-level responses, including the use of standardized evidence-based management pathways, strengthened early diagnosis supported by access to spirometry, and assured availability of essential respiratory medicines within primary health care. Embedding CRD services within universal health coverage (UHC) benefit packages, aligning essential medicine lists with clinical guidelines, and organising care across the continuum, from prevention and early detection to long-term management and rehabilitation, have been associated with improved disease control and reduced avoidable hospitalisations.
Investing in CRD surveillance and monitoring through routine health information systems is critical for tracking disease burden, service coverage, and outcomes over time.
These findings highlight an urgent need for integrated prevention strategies, including stronger tobacco control, clean cooking initiatives, and air quality improvement, alongside expanded diagnostic and treatment capacity in primary care. Addressing these gaps is critical not only for reducing premature mortality but also for mitigating the long-term economic and social impact of CRDs in the Region.
CONCLUSION
Though the WHO package of essential noncommunicable (PEN) disease interventions, which provides an integrated approach to strengthening noncommunicable disease care services, including CRDs, in primary health care, is widely implemented in the WHO South-East Asia Region, significant service delivery gaps remain in the early detection and long-term treatment of asthma and COPD.
Chronic respiratory diseases impose a substantial and likely underestimated health and economic burden in the WHO South-East Asia Region. High prevalence, significant premature mortality—particularly among women—and large productivity losses are driven by preventable risk factors, including tobacco use, household air pollution, and ambient particulate matter exposure. Persistent health system gaps, notably the lack of spirometry and limited access to essential inhaled medicines at the primary care level, hinder timely diagnosis and effective management. Urgent action is needed to integrate CRD prevention into broader NCD and environmental health policies, scale up risk reduction measures such as tobacco control and clean cooking initiatives, and strengthen primary care services. These efforts will be critical for reducing disability and premature deaths, improving quality of life, and safeguarding economic productivity in the Region.
LIMITATIONS
The article is based on secondary use of modelled estimates from the Global Burden of Disease 2021 and WHO data sources and is therefore subject to the assumptions and uncertainties inherent in these datasets. Variability in data availability across countries and indicators, reliance on self-reported health system information, and the use of modelled economic loss estimates may limit precision and comparability. The analysis is descriptive in nature and does not permit causal inference between risk factors, health system characteristics, and CRD outcomes.
Conflict of Interest Statement:
The authors declare that they have no competing interests.
Funding Statement:
None.
Acknowledgements:
The content is solely the responsibility of the authors and does not necessarily represent the official views of the World Health Organization.
Data availability statement
The data that support the findings of this study are available in the public domain.
REFERENCES:
- World Health Organization. Global Health Estimates 2021: deaths by cause, age, sex, by country and by region, 2000–2019. World Health Organization; 2021. Accessed December 9, 2025. https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates
- Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2021 data resources. IHME; 2024. Accessed January 8, 2026. https://www.healthdata.org/results/data-visualizations
- World Health Organization. Chronic respiratory diseases. World Health Organization. Accessed December 9, 2025. https://www.who.int/health-topics/chronic-respiratory-diseases#tab=tab_1
- World Health Organization. Asthma. World Health Organization; 2024. Accessed December 10, 2025. https://www.who.int/en/news-room/fact-sheets/detail/asthma
- World Bank. World Bank country and lending groups. World Bank. Accessed January 21, 2026. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-countryand-lending-groups
- World Health Organization. Assessing national capacity for the prevention and control of noncommunicable diseases: report of the 2023 country capacity survey in the WHO South-East Asia Region. World Health Organization; 2025. Accessed January 10, 2026. https://iris.who.int/handle/10665/381772
- World Health Organization. Country Profile GHE110 – South-East Asia Region. World Health Organization. Accessed January 18, 2026. https://ncdportal.org/CountryProfile/GHE110/SEAR
- Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020–50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023; 11(8), e1183–93. https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(23)00217-6/fulltext
- World Health Organization Regional Office for Europe. Chronic respiratory diseases and health equity by 2050: a spotlight on chronic obstructive pulmonary disease and asthma in the WHO European Region. WHO Regional Office for Europe; 2025. Accessed January 21, 2026. https://www.who.int/europe/publications/i/item/WHO-EURO-2025-12340-52112-79990
- World Health Organization. WHO Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care. World Health Organization; 2020. Accessed January 11, 2026. https://www.who.int/publications/i/item/who-package-of-essential-noncommunicable-(pen)-disease-interventions-for-primary-health-care