





COVID-19 Risk Perceptions Among Community Health Workers
Community health workers’ knowledge, attitudes, and perceptions of risk for COVID-19: A cross-sectional survey in Haiti, Malawi and Rwanda
Kobel Dubique¹, Stephanie Armbruster², Erick Baganizi³, Stefanie A. Joseph⁴, Nadege Belizaire¹, Maurice Junior Chery¹, Peterson Abnis Faure¹, Jimmy Jean Baptiste¹, Emmanuel Demosthene¹, Frank Gondwe³, Benson Chabwera³, Tumusime Musafiri⁵, Jean Claude Mugunga⁴, Dale A. Barnhart²,⁴, Mary Clisbee¹, Bethany Hedt-Gauthier²,⁶, Fabien Munyaneza³
- Partners in Health and Zanmi Lasante (ZL), Mirebalais, Haiti
- Department of Biostatistics, Harvard T.H. Chan School of Public Health, Boston, MA, USA
- Partners In Health, Abwenzi Pa Za Umoyo (APZU), Neno, Malawi
- Partners In Health, Boston, MA, USA
- Partners In Health, Inshuti Mu Buzima (IMB), Kigali, Rwanda
- Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA, USA
These authors contributed equally.
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: Dubique, K., Armbruster, S., et al., 2024. Community health workers’ knowledge, attitudes, and perceptions of risk for COVID-19: A cross-sectional survey in Haiti, Malawi and Rwanda. Medical Research Archives, 12(12).
https://doi.org/10.18103/mra.v12i12.6012
COPYRIGHT: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6012
ISSN: 2375-1924
ABSTRACT
Background:
Community health workers (CHWs) are a trusted source of health care information for rural communities in many low- and middle-income countries. This became particularly relevant during the COVID-19 pandemic when individuals had restricted access to facilities and required sufficient knowledge to prevent infection. This paper assesses CHWs’ level of knowledge, attitudes, and risk awareness towards COVID-19 and willingness for and concerns about vaccination against COVID-19 among CHWs in Rwanda, Malawi and Haiti.
Methods:
Between June 2023 and October 2023, we surveyed 525 CHWs – 175 CHWs per country in Haiti, Malawi, and Rwanda – affiliated with 54 health care facilities. Data on CHWs’ demographics, COVID-19 knowledge, attitudes, risk perceptions, and vaccine intention were collected. Participants indicated on a Likert scale their perception of COVID-19 in terms of its risk-worry-severity-control. We analyzed mean trust scores, correct answer rates and answer frequencies and reported global p-values, assessing any difference and pairwise p-values, assessing country-specific differences, using rank-based and ANOVA tests.
Results:
Across all countries, CHWs perceived COVID-19 as a relatively controllable disease of little worry and considered their risk of contracting the virus lower than on average as compared to other diseases. In Rwanda and Haiti, CHWs showed strong knowledge of COVID-19 and the COVID-19 vaccine (correct answer rate Rwanda: 87.5%; Haiti: 81.3%), while CHWs knew considerably less in Malawi (correct answer rate: 12.9%). The vast majority of CHWs believed COVID-19 presents a serious threat to the public (Haiti: n=168, 96.0%; Malawi: n=159, 91.0%; Rwanda: n=173, 99.0%) and were confident that their country would win the battle against the COVID-19 virus (Haiti: n=149, 85.0%; Malawi: n=133, 76.0%; Rwanda: n=171, 98.0%).
Conclusions:
The knowledge of COVID-19 and the COVID-19 vaccine among CHWs, along with their attitudes and perceptions of the virus, varies across countries and is likely influenced by cultural and political factors. Given the CHWs’ roles to disseminate knowledge among communities in Haiti, Malawi, and Rwanda, targeted CHW education and communication training could improve community responsiveness in the future.
Keywords: COVID-19 vaccines, health risks, community health workers, public health, global health, misinformation.
1. Introduction
COVID-19 was one of the deadliest pandemics of the 21st century, with an estimated death toll ranging from 5 to 17 million people¹. The COVID-19 mortality rate has varied across time, areas, and among countries due to socioeconomic and political disparities², with low- and middle-income countries (LMICs) having a higher mortality rate and shorter length of time from infection to death compared to high-income countries during the second and third waves³. Further, rural communities experienced a higher COVID-19 mortality rate compared to urban communities because of longstanding healthcare disparities that contributed to delays in accessing healthcare⁴.
Vaccines for COVID-19 have proven to be one of the best health strategies to stop the spread of the virus and reduce mortality⁵. However, LMICs have not achieved the full benefits of COVID-19 vaccines. One issue is in-country access to vaccines, with more than 10 billion COVID-19 vaccines largely distributed in high-income countries⁶,⁷. Specific socioeconomic and political conditions in low-income countries further contribute to disparities in both vaccine administration and acceptance⁸. A second issue is an individual’s willingness to be vaccinated, which requires an awareness of COVID-19 risk and the benefits of the vaccines.
Community health workers (CHWs), who are often individuals elected by their communities to serve as a link between the homes and health facilities, are an important part of the health sectors in many LMICs⁹–¹¹. While CHWs cannot increase vaccine availability on a national level, these individuals are an important and trusted source of health-related information who could help educate community members on COVID-19 risks and the vaccine¹²,¹³.
Partners In Health (PIH) is a non-profit organization that works closely with governments in 11 countries, including Haiti, Malawi, and Rwanda, to provide quality healthcare and accompaniment with a preferential option for the poorest communities¹⁴. The organization champions care delivery in low-income countries using a community-based approach and the accompaniment model that engage community health workers in the provision of medicines, in social support, in education, and in the linkage of care between communities and health facilities¹⁵,¹⁶.
When the COVID-19 pandemic devastated the world, PIH used its past experiences in combating infectious disease outbreaks and responding to disasters to launch a comprehensive effort to support COVID-19 response across country sites around the world¹⁷. The Global Coronavirus Response plan by Partners In Health addressed several key areas, including testing, provision of care, support for local government responses, mobilization of community health workers, and research development and capacity building¹⁷.
The study focused on Haiti, Malawi, and Rwanda for several key reasons. An invitation to participate in leveraging CHWs to combat misinformation was extended to all sites in PIH’s cross-site COVID-19 research network, which includes Haiti, Malawi and Rwanda. The three countries self-selected to participate due to their established CHW programs, interest in scientific research, and capacity to engage in the study. Their diverse geographic locations, spanning different continents, offered valuable insights into how local contexts, cultures, and experiences shape the response to the COVID-19 pandemic. Finally, at the inception of the study, country partners had identified both significant vaccine hesitancy and high levels of trust in CHWs, rendering Haiti, Malawi and Rwanda ideal candidate countries to explore the role of CHWs in addressing vaccine-related challenges¹⁸–²⁰.
In this paper, we describe the COVID-19 knowledge, attitude, and vaccination perceptions among CHWs in the rural areas of three different LMICs – Haiti, Malawi, and Rwanda. This study informs overall community awareness and activities related to COVID-19, using CHWs as a litmus for their communities, as well as potential areas to target for future CHW interventions. By exploring across three different countries, we gain a better understanding of the variability in COVID-19 knowledge, attitude, and vaccination perceptions that can support future CHW-driven initiatives and promote successful cross-site research collaboration.
2. Methods
Study Setting
This is a cross-sectional study of CHWs in the rural areas of Haiti, Malawi, and Rwanda that assessed the knowledge, perception and attitude towards COVID-19 and its vaccine. CHWs were selected from the catchment areas of PIH, namely Zanmi Lasante in Haiti, Abwenzi Pa Za Umoyo in Malawi, and Inshuti Mu Buzima in Rwanda. In all three countries, these PIH organizations support health care delivery in underserved rural areas. Health systems in these areas rely on CHWs to connect communities to health facilities.
In the Central Plateau and Lower Artibonite regions of Haiti, the CHW program, supported by PIH, operates in alignment with Haiti’s national CHW framework. CHWs can either focus on specific diseases or provide general health care support. Overall, PIH supports approximately 2,500 Haitian CHWs in total, serving a population of roughly 3.3 million people²¹.
In Neno district, the PIH-supported area in Malawi, PIH implements a household model for CHW care, where a CHW provides support to all members of a household irrespective of their health status. The PIH community health department in Malawi has trained 629 CHWs to serve over 19,000 households, with the goal of ensuring faster access to health care, higher retention, and treatment adherence, as well as greater prevention and economic development²²,²³.
In the Kirehe and Southern Kayonza districts of Rwanda, the CHWs supported by PIH are integrated into the national system, which was established in 2007²⁴. Each CHW has designated responsibilities, focusing either on the treatment of childhood diseases, malnutrition, providing care during pregnancy, and facilitating delivery at health care centers²⁰. In these two districts, PIH supports over 1,200 CHWs, serving approximately 48,000 households²².
Study Design and Data Collection
This study, conducted from June 2023 to October 2023, included 525 eligible CHWs (175 CHWs per country). Participants were eligible for the survey if they were over 18 years old and actively working in the country’s target catchment area (Haiti: 289 eligible CHWs, Malawi: 1232 eligible CHWs, Rwanda: 3499 eligible CHWs). In each country, 205 eligible CHWs (175 + 30 backup) were randomly sampled from the group of eligible CHWs, and the first 175 CHWs who agreed to participate were recruited.
The CHW survey was conducted in the local language – Haitian Creole in Haiti, Chichewa in Malawi and Kinyarwanda in Rwanda. The survey was administered by trained enumerators, who directly entered the data into REDCap using tablets. The CHW survey lasted 30 to 90 minutes and comprised of questions about COVID-19 infection and vaccine history, reasons for or against the intention to vaccinate, knowledge of the COVID-19 virus and vaccine, as well as perceived danger of a COVID-19 infection and overall attitude towards the pandemic. The survey also collected personal demographic information from each CHW.
Data Analysis
The data were exported from REDCap, cleaned, and analyzed using STATA v15.1. Figures were generated in R v4.3.2. We summarized categorical variables by percentages and counts or medians and interquartile range (IQR), and continuous variables by means and standard deviations. Using the method of Wang et al.²⁵, we visualized the perceptions of CHWs about COVID-19 about risk, worry, severity and control in a boxplot, stratified by country, with each country team being able to modify their priority disease comparison list.
On each plot, we display the median responses for other reference diseases assessed in the survey, namely:
(1) infectious diseases: cholera, tuberculosis, HIV/AIDS, malaria, and typhoid (Haiti only), Ebola (Rwanda only);
(2) non-communicable diseases: diabetes, cardiovascular diseases, asthma, malnutrition, hypertension (Rwanda and Haiti only);
(3) mental health diseases
anxiety, depression, suicidal ideation (Haiti only).
We tested for a global difference in answer distribution in COVID-19 responses with a Kruskal-Wallis test and pairwise differences between countries with a Mann-Whitney U-test.
We quantified the COVID-19 related knowledge among CHWs based on the success rate, indicating the proportion of correct affirmations or rejections of 10 statements surrounding COVID-19 and the COVID-19 vaccine. Such knowledge assessment was used in previous research²⁶,²⁷. The statements referred to common COVID-19 related misconceptions and stigma. The success rates were compared across countries in a bar plot. We tested for pairwise country-wise differences in knowledge in a Chi-squared test.
We captured attitudes towards COVID-19 using a 3-level agreement Likert scale – (1) (Strongly) Disagree, (2) Neutral, (3) (Strongly) Agree – to 10 statements surrounding worry about health, beliefs in effectiveness of public health measures, development and controllability of the pandemic, as well as trust in governmental public health management²⁷. Pairwise country-wise differences were visualized in a Likert plot and tested for by an unpooled t-test based on the mean attitude towards COVID-19 across statements.
Depending on their vaccination status, the CHWs were prompted to indicate the reasons for or against receiving a COVID-19 vaccination. All CHWs were asked about their intention and reasons to receive vaccine boosters. The answers were attributed to a predefined category (multiple answers possible) or indicated in an “Other” category, following standard procedure²⁸. The answer frequencies were analyzed in a bar plot.
ETHICS
The study received ethical approval from the Harvard Internal Review Board (IRB# 11-1339), the Malawi National Committee on Research in the Social Sciences and Humanities (IRB# 11/22/694), the Haiti Zanmi Lasante Institutional Review Board (IRB# 11082022), and the Rwanda National Research Ethics Committee (IRB# 00001497). All CHWs provided informed consent prior to study participation. Participants received a baseline compensation of $5 to $10, as well as additional country- and time-specific compensation and reimbursement for travel.
3. Results
Demographic Characteristics
This study included 525 CHWs, divided equally across countries (Table 1). Nearly two-thirds were female in Malawi (n=117, 66.9%) and Rwanda (n=115, 65.7%), but only one-third were female in Haiti (n=66, 37.7%). The mean age was 44.7 years (standard deviation (s.d.) ± 10.2 years). The majority of CHWs (n=457, 90.7%) had at least one child who was ≤18 years old. The median number of children ≤18 years old across countries was 2 (IQR: 1–3); for those children ≤18 years old, the mean age was 8.5 years (s.d. ± 6.8 years).
Table 1: Demographics among community health workers in Rwanda, Malawi and Haiti
Number of community health workers involved in survey
- Rwanda: n=175 (33.33%)
- Malawi: n=175 (33.33%)
- Haiti: n=175 (33.33%)
- Total: n=525 (100%)
Sex (Female)
- Rwanda: 115 (65.70%)
- Malawi: 117 (66.90%)
- Haiti: 66 (37.70%)
- Total: 298 (56.80%)
Children (Have children)
- Rwanda: 174 (99.40%)
- Malawi: 170 (97.10%)
- Haiti: 164 (93.70%)
- Total: 508 (96.80%)
Yes, and at least one child ≤18 years
- Rwanda: 160 (92.50%)
- Malawi: 153 (91.10%)
- Haiti: 144 (88.30%)
- Total: 457 (90.70%)
Yes, but all children are >18 years
- Rwanda: 13 (7.40%)
- Malawi: 15 (8.60%)
- Haiti: 19 (10.90%)
- Total: 47 (9.00%)
Age (years), mean (STD)
- Rwanda: 42.9 (9.9)
- Malawi: 42.5 (10.5)
- Haiti: 48.7 (9.0)
- Total: 44.7 (10.2)
Number of children ≤18 years, median (IQR)
- Rwanda: 2 (1.0–3.0)
- Malawi: 2 (2.0–3.0)
- Haiti: 2 (1.0–3.0)
- Total: 2 (1.0–3.0)
Age of child ≤18 years (mean, STD)
- Rwanda: 7.9 (7.2)
- Malawi: 8.7 (6.5)
- Haiti: 8.8 (6.6)
- Total: 8.5 (6.8)
Perceptions of Health Risk–Worry–Severity–Control of COVID-19
The perception of COVID-19 controllability among CHWs varied significantly across countries (p<0.001) (Figure 1A). The highest belief in COVID-19 controllability was registered in Rwanda (median=5 indicating “Strongly agree”, IQR: 3–5; Malawi: median=4 indicating “Agree”, IQR: 3–5; Haiti: median=4 indicating “Agree”, IQR: 3–5). The median controllability value for COVID-19 aligned with the median across all reference diseases, indicating similar perceptions of controllability.
Perceived risk of a COVID-19 infection varied significantly by country (p<0.001):
- Rwanda: median=1 (“Much lower than average”, IQR: 1–2)
- Malawi: median=3 (“Average”, IQR: 2–4)
- Haiti: median=2 (“Lower than average”, IQR: 1–5)
In Rwanda, CHWs perceived the median risk of contracting a reference disease as “Lower than average” for COVID-19. In Malawi and Haiti, the median risk perception for reference diseases aligned with COVID-19 risk perception.
The perception of the severity of a COVID-19 infection differed significantly between Rwanda and Malawi versus Haiti (p<0.01). In Malawi, CHWs considered COVID-19 a more serious disease than reference diseases (median=4 indicating “Agree”, IQR: 4–5). The perception of severity aligned for Rwanda and Haiti.
The CHWs worried little about contracting COVID-19 (median=1 indicating “Not at all”, Rwanda: IQR 1; Haiti/Malawi: IQR 1–2). The perceptions of worry varied significantly across countries (p<0.05 for Haiti and Malawi, p<0.001 otherwise). Participants did not worry more or less about COVID-19 compared to reference diseases.
Knowledge About COVID-19 and COVID-19 Vaccine Among Community Health Workers
In Rwanda and Haiti, CHWs were very knowledgeable, while they were less so in Malawi (COVID-19 knowledge: Malawi-Haiti / Malawi-Rwanda p<0.001; Rwanda-Haiti p=0.429; COVID-19 vaccine knowledge: Rwanda-Malawi / Rwanda-Haiti / Malawi-Haiti p<0.001).
In Rwanda and Haiti, CHWs showed more knowledge on the effectiveness of preventive measures (facemasks, avoid crowded places, immediate isolation of contact person) than CHWs in Malawi:
- Facemasks: Haiti n=151 (86.3%); Malawi n=1 (0.6%); Rwanda n=168 (96.0%)
- Avoid crowded places: Haiti n=163 (93.1%); Malawi n=5 (2.9%); Rwanda n=157 (89.7%)
- Immediate isolation of contact person: Haiti n=156 (89.1%); Malawi n=9 (5.1%); Rwanda n=164 (93.7%)
Popular COVID-19 myths seemed widely disseminated in Malawi; 42 (24.0%) CHWs believed that a virus transmission cannot happen without fever; only 64 (36.4%) CHWs correctly rejected the statement that contracting COVID-19 disease was safer than receiving the vaccine; 3 (1.7%) CHWs correctly rejected the belief that the COVID-19 vaccine can cause infertility; and only 10 (5.7%) correctly rejected that a vaccination can lead to an infection with COVID-19.
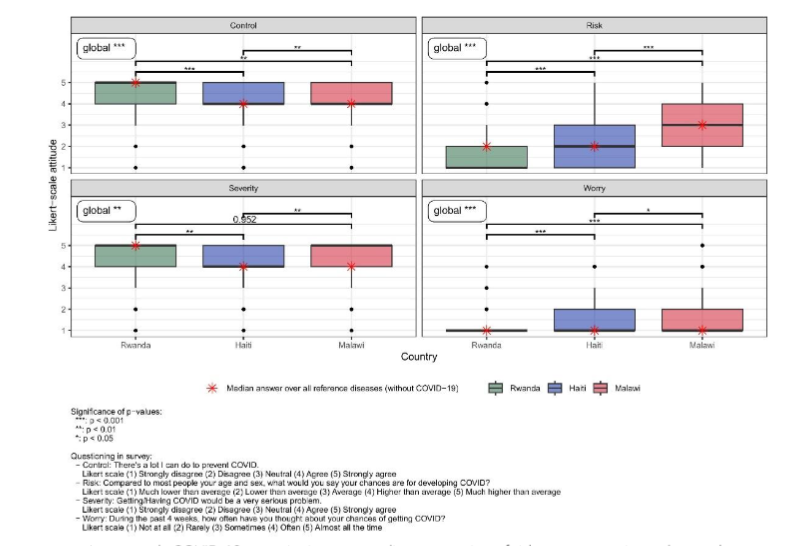
Figure 1: Danger perception towards COVID-19; positioning surrounding risk, worry, severity and control among community health workers in Rwanda, Malawi and Haiti
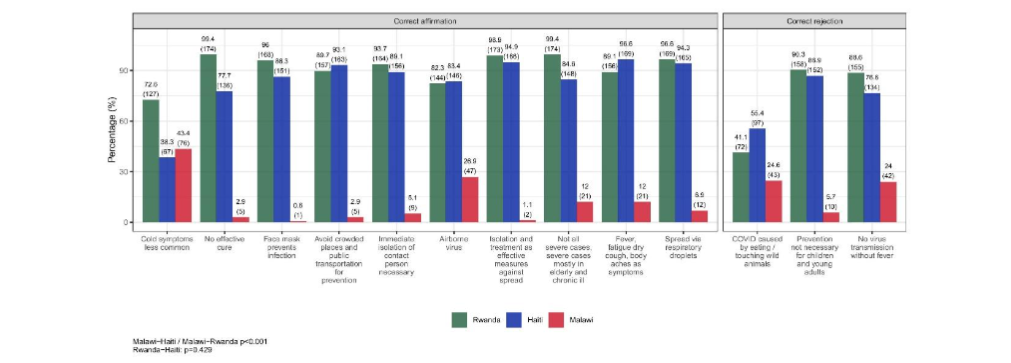
Figure 2A: Correct answer rate for statements surrounding COVID-19 virus among community health workers in Rwanda, Malawi and Haiti; absolute numbers in brackets
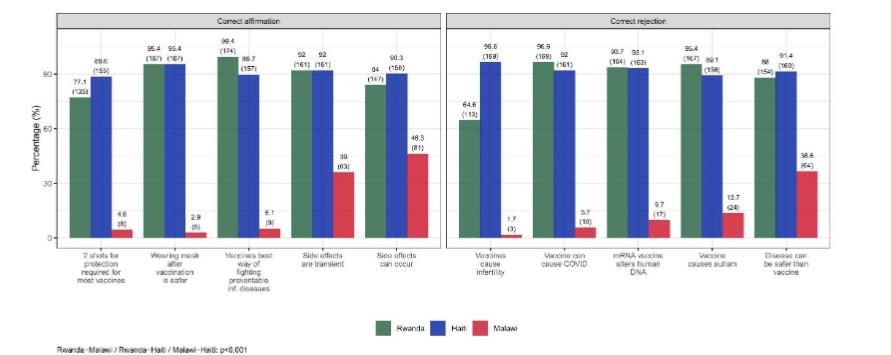
Figure 2B:
Correct answer rate for statements surrounding COVID-19 vaccine among community health workers in Rwanda, Malawi and Haiti; absolute numbers in brackets
Attitudes About COVID-19 Among Community Health Workers in Haiti, Malawi, and Rwanda
The mean attitude across countries differed significantly across countries (Rwanda–Malawi: p<0.001; Rwanda–Haiti: p<0.001; Malawi–Haiti: p=0.0013).
Most CHWs acknowledged the threat COVID-19 posed to the public:
- Haiti: n=168, 96.0%
- Malawi: n=159, 90.9%
- Rwanda: n=173, 98.9%
They also agreed on the efficacy of social distancing to control COVID-19:
- Haiti: n=162, 93.6%
- Malawi: n=170, 97.7%
- Rwanda: n=160, 94.7%
Participants were confident in the ability of their country to overcome the COVID-19 virus:
- Haiti: n=149, 85.1%
- Malawi: n=133, 76.4%
- Rwanda: n=171, 97.7%
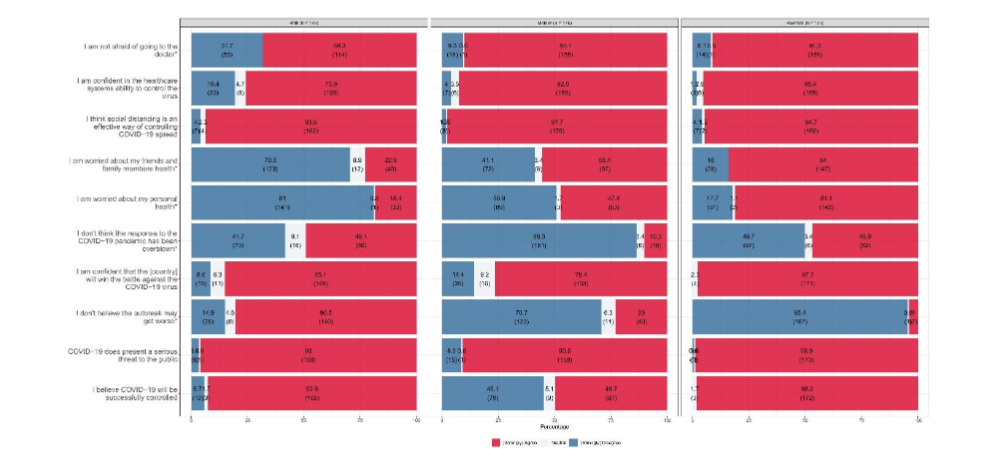
Figure 3:
Attitude of community health workers towards the COVID-19 pandemic and its management in Rwanda, Malawi and Haiti; absolute numbers in brackets
In Haiti and Malawi, CHWs expressed little concern for their health as well as for the health of their families and friends:
Personal health concern:
- Haiti: n=141, 81.0%
- Malawi: n=89, 50.9%
- Rwanda: n=31, 17.7%
Concern for family and friends:
- Haiti: n=123, 70.3%
- Malawi: n=72, 41.1%
- Rwanda: n=28, 16.0%
Haitian CHWs expressed fear and doubt about their physicians and healthcare system:
- Unafraid of visiting doctor: n=53, 31.7%
- No belief in healthcare system’s ability to control the virus: n=33, 19.4%
- Yet did not believe the outbreak would worsen: n=140, 80.5%
Rwandan and Malawian CHWs were more pessimistic about the future development of the pandemic:
- (“Strongly agree”/“Agree” outbreak will not get worse):
- Malawi: n=40, 23.0%
- Rwanda: n=7, 4.9%
History of COVID-19 Vaccinations Among Community Health Workers
Most CHWs could not recall a previous infection with COVID-19:
- Haiti: n=167, 95.4%
- Malawi: n=166, 94.9%
- Rwanda: n=172, 98.3%
Many CHWs in Haiti and Rwanda confirmed having received the COVID-19 vaccine:
- Haiti: n=170, 97.1%
- Rwanda: n=175, 100%
However, 58 (33.1%) Malawian CHWs did not receive a COVID-19 vaccine.
Rwanda had the highest vaccination rate with two doses:
- n=134, 76.6%
And the highest booster rate:
- n=133, 99.3%
Booster vaccination was unavailable in Haiti.
Most CHWs across countries would agree to be vaccinated if a third and fourth dose were available at no cost:
- Haiti: n=163, 93.7%
- Malawi: n=155, 88.6%
- Rwanda: n=174, 99.4%
Table 2: Vaccine History and Vaccination Intention
Previous COVID-19 Infection (N=175 each country)
| Response | Rwanda | Malawi | Haiti | Total |
|---|---|---|---|---|
| No | 172 (98.3%) | 166 (94.9%) | 167 (95.4%) | 505 (96.2%) |
| Yes | 3 (1.7%) | 5 (2.9%) | 8 (4.6%) | 16 (3%) |
| Not sure | 0 | 4 (2.3%) | 0 | 4 (0.8%) |
COVID-19 Vaccination History
Have you received a COVID-19 vaccine?
| Response | Rwanda | Malawi | Haiti | Total |
|---|---|---|---|---|
| No | 0 | 58 (33.1%) | 5 (2.9%) | 63 (12%) |
| Yes | 175 (100%) | 117 (66.9%) | 170 (97.1%) | 462 (88%) |
Number of Doses Received
| Dose | Rwanda | Malawi | Haiti | Total |
|---|---|---|---|---|
| One dose | 25 (14.3%) | 40 (34.2%) | 91 (53.5%) | 156 (33.8%) |
| Two doses | 134 (76.6%) | 77 (65.8%) | 79 (46.5%) | 290 (62.8%) |
| Don’t know | 16 (9.1%) | 0 | 0 | 16 (3.5%) |
Booster Dose
| Response | Rwanda | Malawi | Haiti | Total |
|---|---|---|---|---|
| No | 1 (0.7%) | 41 (53.2%) | 79 (100%) | 121 (41.7%) |
| Yes | 133 (99.3%) | 36 (46.8%) | 0 | 169 (58.3%) |
Intention to Vaccinate (3rd/4th Dose if Free)
| Response | Rwanda | Malawi | Haiti | Total |
|---|---|---|---|---|
| No | 0 | 15 (8.6%) | 8 (4.6%) | 23 (4.4%) |
| Yes | 174 (99.4%) | 155 (88.6%) | 163 (93.7%) | 492 (93.9%) |
| Not sure | 1 (0.6%) | 5 (2.9%) | 3 (1.7%) | 9 (1.7%) |
Reasons Against Past Vaccination and Vaccination Intention
In Haiti, CHWs lacked trust, resulting in refusal of vaccination in the past:
- Lack of trust in international donors/foreign governments: n=1 (20%)
- Lack of trust in local government: n=1 (20%)
- Lack of trust in vaccine manufacturers: n=1 (20%)
In Malawi, CHWs expressed safety concerns as the main reason for refusing vaccination:
- Harmfulness of vaccine: n=15 (25.9%)
- Unsafe vaccine/side effects:
n=11, 19.0%; lack of trust in vaccine manufacturers: n=4, 6.9%; concern about vaccine types: n=5, 8.6% (Figure 4A). All CHWs in Rwanda were vaccinated.
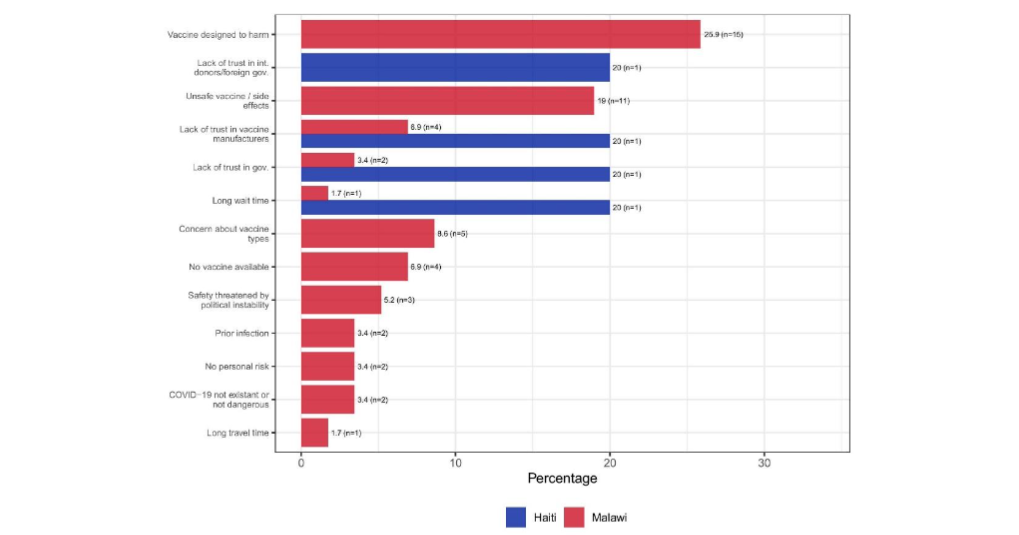
Figure 4A:
Reasons against vaccination among community health workers in Haiti (n=5) and Malawi (n=58); no community health workers in Rwanda reported being unvaccinated; absolute numbers in brackets
Reasons for Expressing No Intention to Get Vaccinated
In Haiti, reasons included:
- Vaccine availability (n=2, 18.2%)
- Unsafe vaccine (n=1, 9.1%)
- Belief that COVID-19 did not exist or was not dangerous (n=1, 9.1%)
In Malawi, safety concerns were the primary reason to refuse additional vaccination:
- Unsafe vaccine: n=5 (25.0%)
- Concerns about vaccine types: n=2 (10.0%)
- Vaccine designed to harm: n=2 (10.0%)
In Rwanda, one CHW considered themselves not at risk for COVID-19.
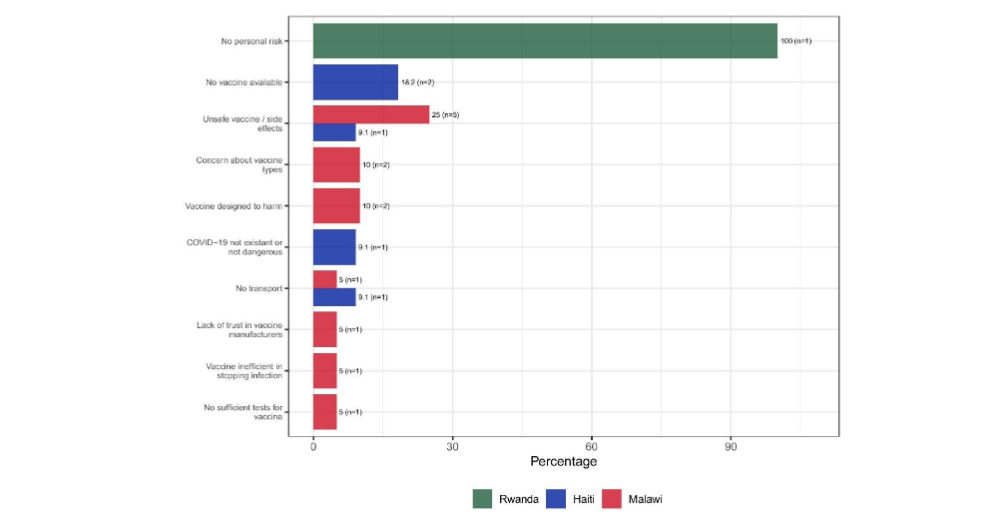
Figure 4B:
Reasons against intention to vaccinate among community health workers in Rwanda (n=1), Haiti (n=11) and Malawi (n=20); absolute numbers in brackets
Reasons for Intention to Vaccinate
Personal health, the health of family, and community protection were the main reasons across countries:
Personal health:
- Haiti: n=153, 93.9%
- Malawi: n=140, 90.3%
- Rwanda: n=159, 91.4%
Family health:
- Haiti: n=72, 44.2%
- Malawi: n=39, 25.2%
- Rwanda: n=83, 47.7%
Community health:
- Haiti: n=52, 31.9%
- Malawi: n=24, 15.5%
- Rwanda: n=63, 36.2%
Another reason: desire to stop the COVID-19 pandemic:
- Haiti: n=30, 18.4%
- Malawi: n=38, 24.5%
- Rwanda: n=120, 69.0%
In Rwanda, government and Ministry of Health recommendations, as well as travel requirements, incentivized vaccination:
- Government recommendation: Rwanda n=71, 40.8%; Haiti n=11, 6.8%; Malawi n=2, 1.3%
- Travel requirements: Rwanda n=58, 33.3%; Haiti n=3, 1.8%; Malawi n=2, 1.3%
Recommendations from healthcare workers strongly motivated:
- Haiti: n=18, 11.0%
- Malawi: n=19, 12.3%
- Rwanda: n=11, 6.3%
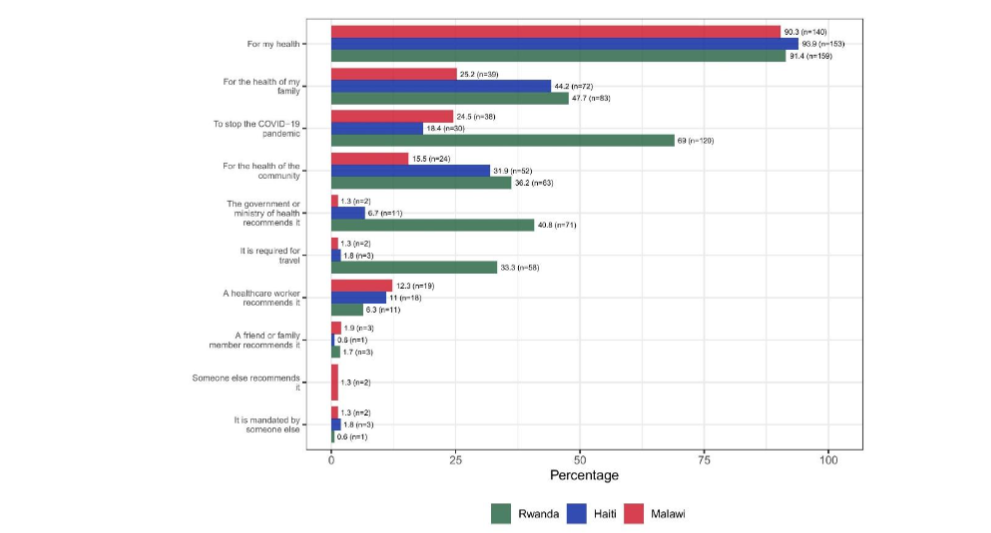
Figure 4C:
Reasons for intention to vaccinate among community health workers in Rwanda (n=174), Malawi (n=155) and Haiti (n=163); absolute numbers in brackets
Discussion
The study investigated differences in CHWs’ risk perception, knowledge, and attitude towards COVID-19 and COVID-19 vaccination efforts across three LMICs: Rwanda, Malawi, and Haiti.
Overall, CHWs considered COVID-19 a serious public health threat and expressed support for adherence to public health interventions; yet, they did not perceive the virus as an immediate threat to their personal health. They voiced doubt about the intensity and effectiveness of national pandemic responses. Knowledge around COVID-19 as well as vaccination rates depended on national settings.
Rwandan CHWs exhibited a strong sense of control over COVID-19, with little worry about contracting the disease. Early in the pandemic, the Rwandan government (including the Ministry of Health, Biomedical Center, and Surveillance Response Division) implemented a comprehensive Coronavirus National Preparedness and Response Plan aimed at containing the spread of the virus and combating misinformation²⁹. Strategies included drones, robots, and social media for rapid dissemination of public health information, as well as transparent communication to build trust³⁰. Most Rwandans received at least two doses of the COVID-19 vaccine, contributing to confidence in the healthcare system³¹.
In Haiti and Malawi, weaker health infrastructure and misinformation may have negatively affected risk perceptions of COVID-19³²–³⁴. Participants in Malawi considered COVID-19 a more uncontrollable, severe disease and expressed a pessimistic outlook. However, many also perceived their personal risk as low. These perceptions may stem from limited training opportunities, lack of practical training, and lack of equipment for CHWs in remote areas³⁵.
Overall, lack of knowledge in Malawi likely contributed to perceiving COVID-19 as less concerning compared to Haiti and Rwanda, where CHWs showed better knowledge. Previous studies support these findings, indicating differences in knowledge across countries³⁶,³⁷. Factors contributing to low knowledge in Malawi include rural location, education gaps, limited training opportunities, and poor access to information³⁸,³⁹.
Conversely, CHWs from Haiti demonstrated strong awareness of the infectious nature of COVID-19 and expressed concern about infection. However, many were hesitant to seek healthcare due to mistrust in the system. Political instability, violence, and limited healthcare access further worsened the situation⁴². Haiti faced challenges such as inadequate biosecurity, testing infrastructure, and misinformation, all of which hindered pandemic response.
Rwandan CHWs’ optimism and trust in government response aligned with effective national strategies and strong public health communication. Malawi CHWs, however, questioned the controllability of the virus and perceived the response as excessive, reflecting differences in national policy and communication approaches.
held, openly violating the public health guidance⁴⁷. This caused severe mistrust in the government and undermined the relevance of the COVID-19 prevention measures⁴⁷. The Malawian High Court overruled the country’s lockdown after nationwide protests against lockdown policies⁴⁷. The opposition to movement restrictions in Malawi might have resulted from its direct consequences on livelihoods⁴⁸.
As our results showed, a substantial proportion of CHWs in Haiti, Malawi, and Rwanda supported adherence to social distancing measures as an effective intervention to mitigate the spread of COVID-19. At the time of the initial COVID-19 outbreak, stringent restrictions were observed to forestall virus propagation. These findings align with studies across multiple countries, showing communities’ favorable attitudes toward public health directives to contain COVID-19.
Furthermore, an online survey in China revealed that many respondents were concerned about crowded places and complied with mask-wearing guidelines⁴⁴. Adherence to such guidelines correlated with reduced high-risk behaviors associated with COVID-19 transmission.
Vaccination coverage among CHWs, including number of doses and booster uptake, varied across Rwanda, Malawi, and Haiti. Rwanda had the highest vaccination rate, with most CHWs receiving at least two doses of the COVID-19 vaccine³¹. This success was attributed to high confidence in Rwanda’s healthcare system.
From early vaccination efforts, Rwanda had sufficient vaccine supply and later aimed for herd immunity through booster doses³¹. These efforts are reflected in the study data, showing Rwanda had the highest proportion of CHWs receiving booster doses.
In Haiti, vaccine supply depended on international donations⁵⁰, and many campaigns failed due to shortages. Haiti prioritized first and second doses for high-risk groups, and no data were available on booster coverage.
In March 2021, Malawi received 360,000 doses of AstraZeneca vaccines for priority groups⁵². However, vaccine hesitancy limited the campaign’s success⁵²,⁵³. Key reasons for hesitancy included mistrust in vaccine safety, lack of knowledge, and limited access in rural areas.
Previous research highlights that education level, socioeconomic status, exposure to misinformation, and trust in public health authorities strongly influence vaccine hesitancy⁵⁵–⁵⁹. When PIH implemented its COVID-19 vaccination strategy, willingness to vaccinate increased across sites⁶⁰.
Healthcare workers, including CHWs, are among the most trusted sources of vaccine information⁶¹. The findings that most CHWs across Rwanda, Haiti, and Malawi were willing to receive additional vaccine doses provide optimism.
Limitations
Several limitations should be considered:
- The survey relied on self-reported data without verification of vaccination records.
- National context (economic, cultural, political) may influence responses.
- Findings may not be fully comparable or generalizable to other LMICs.
- PIH’s involvement in vaccination efforts may have increased willingness among participants.
- The study only included adult CHWs.
Despite these limitations, the study provides valuable insights into leveraging CHWs as trusted sources of information and promoters of public health interventions.
Conclusion
Risk perception, knowledge of COVID-19 and vaccines, and attitudes toward the pandemic among CHWs differed across Rwanda, Malawi, and Haiti.
Overall:
- CHWs consider COVID-19 a serious disease
- But do not perceive it as an immediate personal threat
Key factors influencing outcomes:
- National policies and communication
- Training opportunities
- Vaccine availability
- Trust in institutions
Lack of trust was a major cause of vaccine hesitancy.
Recommendation:
Targeted education, transparent communication, and strengthening CHW capacity are essential to improve public health responses and community compliance.
Conflict of Interest
The authors have no conflicts of interest to declare.
Funding Statement
This research was funded by the Social Science Research Council’s Mercury Project, with additional support from:
- Rockefeller Foundation
- Robert Wood Johnson Foundation
- Craig Newmark Philanthropies
- Alfred P. Sloan Foundation
Acknowledgements
Special thanks to:
- Ximena Tovar
- Kathryn Hanly
- Caitlin Roman
For leadership and support during the project.
The authors also acknowledge the contributions of participants, staff, and leadership from the three participating countries.
Target Journal
Challenges and Opportunities in COVID-19
Special issue from the European Society of Medicine
References
1. Prabhu M, Gergen J. History’s Seven Deadliest Plagues. VaccinesWork. November 15, 2021. Accessed August 15, 2024. https://www.gavi.org/vaccineswork/historys-seven-deadliest-plagues
2. Sorci G, Faivre B, Morand S. Explaining among-country variation in COVID-19 case fatality rate. Sci Rep. 2020;10(1):18909. doi:10.1038/s41598-020-75848-2
3. Yao L, Aleya L, Howard SC, et al. Variations of COVID-19 mortality are affected by economic disparities across countries. Sci Total Environ. 2022;832:154770. doi:10.1016/j.scitotenv.2022.154770
4. Grome HN, Raman R, Katz BD, et al. Disparities in COVID-19 Mortality Rates: Implications for Rural Health Policy and Preparedness. J Public Health Manag Pract. 2022;28(5):478-485. doi:10.1097/PH H.0000000000001507
5. Moghadas SM, Vilches TN, Zhang K, et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin Infect Dis. 2021;73(12):2257-2264. doi:10.10 93/cid/ciab079
6. Our World in Data. Total COVID-19 vaccine doses administered. Our World in Data. Accessed August 15, 2024. https://ourworldindata.org/grapher/cumulative-covid-vaccinations?tab=map
7. Ahlberg BM, Bradby H. Ethnic, racial and regional inequalities in access to COVID-19 vaccine, testing and hospitalization: Implications for eradication of the pandemic. Front Sociol. 2022;7:809090. doi:10.3389/fsoc.2022.809090
8. Bayati M, Noroozi R, Ghanbari-Jahromi M, Jalali FS. Inequality in the distribution of Covid-19 vaccine: a systematic review. Int J Equity Health. 2022;21(1):122. doi:10.1186/s12939-022-01729-x
9. World Health Organization. WHO Guideline on Health Policy and System Support to Optimize Community Health Worker Programmes.; 2018.
10. Ahmed S, Chase LE, Wagnild J, et al. Community health workers and health equity in low- and middle-income countries: systematic review and recommendations for policy and practice. Int J Equity Health. 2022;21(1):49. doi:10.1186/s12939-021-01615-y
11. Mukherjee J, Farmer P. An Introduction to Global Health Delivery: Practice, Equity, Human Rights. 2nd ed. Oxford University PressNew York; 2021. doi:10.1093/oso/9780197607251.001.0001
12. Ballard M, Johnson A, Mwanza I, et al. Community Health Workers in Pandemics: Evidence and Investment Implications. Glob Health Sci Pract. 2022;10(2):e2100648. doi:10.97 45/GHSP-D-21-00648
13. Oliver J, Ferdinand A, Kaufman J, Allard N, Danchin M, Gibney KB. Community health workers’ dissemination of COVID-19 information and services in the early pandemic response: a systematic review. BMC Health Serv Res. 2024;24 (1):711. doi:10.1186/s12913-024-11165-y
14. Countries. Partners In Health. Accessed November 14, 2024. https://www.pih.org/countries
15. Mukherjee JS, Barry D, Weatherford RD, Desai IK, Farmer PE. Community-Based ART Programs: Sustaining Adherence and Follow-up. Curr HIV/AIDS Rep. 2016;13(6):359-366. doi:10.1007/ s11904-016-0335-7
16. 5 Unique Elements Driving Partners In Health’s Work. Partners In Health. June 8, 2021. Accessed November 14, 2024. https://www.pih.org/article/5-unique-elements-driving-partners-healths-work
17. Global Coronavirus Response. Partners In Health. March 13, 2020. Accessed November 14, 2024. https://www.pih.org/article/global-coronavirus-response
18. Chery MJ, Dubique K, Higgins JM, et al. COVID-19 vaccine acceptance in three rural communes in Haiti: A cross-sectional study. Hum Vaccines Immunother. 2023;19(1):2204048. doi:10. 1080/21645515.2023.2204048
19. Aron MB, Connolly E, Vrkljan K, et al. Attitudes toward COVID-19 Vaccines among Patients with Complex Non-Communicable Disease and Their Caregivers in Rural Malawi. Vaccines. 2022;10(5) :792. doi:10.3390/vaccines10050792
20. Niyigena A, Girukubonye I, Barnhart DA, et al. Rwanda’s community health workers at the front line: a mixed-method study on perceived needs and challenges for community-based healthcare delivery during COVID-19 pandemic. BMJ Open. 2022;12(4):e055119. doi:10.1136/bmjopen-2021-055119
21. Partners In Health. Haiti. Partners In Health. Accessed May 1, 2024. https://www.pih.org/country/haiti
22. Partners In Health. Malawi. Partners In Health. Accessed May 5, 2024. https://www.pih.org/country/malawi
23. Admon AJ, Bazile J, Makungwa H, et al. Assessing and improving data quality from community health workers: a successful intervention in Neno, Malawi. Public Health Action. 2013;3(1):56-59. doi:10.5588/pha.12.0071
24. Condo J, Mugeni C, Naughton B, et al. Rwanda’s evolving community health worker system: a qualitative assessment of client and provider perspectives. Hum Resour Health. 2014; 12(1):71. doi:10.1186/1478-4491-12-71
25. Wang C, O’Neill SM, Rothrock N, et al. Comparison of risk perceptions and beliefs across common chronic diseases. Prev Med. 2009;48 (2):197-202. doi:10.1016/j.ypmed.2008.11.008
26. Lee SK, Sun J, Jang S, Connelly S. Misinformation of COVID-19 vaccines and vaccine hesitancy. Sci Rep. 2022;12(1):13681. doi:10.1038/ s41598-022-17430-6
27. Bakdash T, Marsh C. Knowledge, Attitudes, and Beliefs Regarding the COVID-19 Pandemic Among Women in Kansas. J Community Health. 2021;46(6):1148-1154. doi:10.1007/s10900-021-00994-1
28. Joseph SA, Jerome JG, Boima F, et al. Attitudes toward COVID-19 Vaccination: Staff and Patient Perspectives at Six Health Facilities in Sierra Leone. Vaccines. 2023;11(8):1385. doi:10.3390/ vaccines11081385
29. Musanabaganwa C, Cubaka V, Mpabuka E, et al. One hundred thirty-three observed COVID-19 deaths in 10 months: unpacking lower than predicted mortality in Rwanda. BMJ Glob Health. 2021;6(2):e004547. doi:10.1136/bmjgh-2020-004547
30. Karim N, Jing L, Lee JA, et al. Lessons Learned from Rwanda: Innovative Strategies for Prevention and Containment of COVID-19. Ann Glob Health. 2021;87(1):23. doi:10.5334/aogh.3172
31. Uwizeyimana T, Manirambona E, Saidu Musa S, Uwiringiyimana E, Bazimya D, Mathewos K. Achieving COVID‐19 herd immunity in Rwanda, Africa. Public Health Chall. 2023;2(1):e75. doi:10. 1002/puh2.75
32. Louis-Jean J, Cenat K, Sanon D, Stvil R. Coronavirus (COVID-19) in Haiti: A Call for Action. J Community Health. 2020;45(3):437-439. doi:10. 1007/s10900-020-00825-9
33. Chilumpha M, Chatha G, Umar E, et al. ‘We stay silent and keep it in our hearts’: a qualitative study of failure of complaints mechanisms in Malawi’s health system. Health Policy Plan. 2023;38(Supple ment_2):ii14-ii24. doi:10.1093/heapol/czad043
34. United Nations. Overcoming COVID myths and fears in Malawi. United Nations News: Global perspective Human stories. May 2, 2021. Accessed August 16, 2024.https://news.un.org/en/story/2021/05/1090972
35. Olaniran A, Banke-Thomas A, Bar-Zeev S, Madaj B. Not knowing enough, not having enough, not feeling wanted: Challenges of community health workers providing maternal and newborn services in Africa and Asia. Tappis H, ed. PLOS ONE. 2022;17(9):e0274110. doi:10.1371/journal. pone.0274110
36. Wake AD. The Acceptance Rate Toward COVID-19 Vaccine in Africa: A Systematic Review and Meta-analysis. Glob Pediatr Health. 2021;8:23 33794X2110487. doi:10.1177/2333794X211048738
37. Feldman M, Lacey Krylova V, Farrow P, et al. Community health worker knowledge, attitudes and practices towards COVID-19: Learnings from an online cross-sectional survey using a digital health platform, UpSCALE, in Mozambique. Di Gennaro F, ed. PLOS ONE. 2021;16(2):e0244924. doi:10.1371/journal.pone.0244924
38. Li Y, Liu G, Egolet RO, Yang R, Huang Y, Zheng Z. Knowledge, Attitudes, and Practices Related to COVID-19 Among Malawi Adults: A Community-Based Survey. Int J Environ Res Public Health. 2021;18(8):4090. doi:10.3390/ijerph18084090
39. Kainja J, Makhumula C, Twabi HS, Gunde AM, Ndasauka Y. Cultural determinants of COVID-19 vaccines misinformation in Malawi. Humanit Soc Sci Commun. 2024;11(1):1193. doi:10.1057/s415 99-024-03743-6
40. Magagula A. Level of knowledge about COVID-19 and vaccines among CHWs in Malawi. Published online July 25, 2024.
41. Faure JA, Wang CW, Chen CHS, Chan CC. Assessment of the Functional Capacity and Preparedness of the Haitian Healthcare System to Fight against the COVID-19 Pandemic: A Narrative Review. Healthcare. 2022;10(8):1428. doi:10.3390/ healthcare10081428
42. Miller J. Sustaining Health Care as Crisis in Haiti Escalates. Harvard Medical School. March 21, 2024. Accessed October 26, 2024. https://hms.harvard.edu/news/sustaining-health-care-crisis-haiti-escalates
43. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, Attitude and Practice Toward COVID-19 Among the Public in the Kingdom of Saudi Arabia: A Cross-Sectional Study. Front Public Health. 2020;8:217. doi:10.3389/fpubh.2020.00217
44. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745-1752. doi:10.7150/ijbs.45221
45. Yoseph A, Tamiso A, Ejeso A. Knowledge, attitudes, and practices related to COVID-19 pandemic among adult population in Sidama Regional State, Southern Ethiopia: A community based cross-sectional study. Erbil N, ed. PLOS ONE. 2021;16(1):e0246283. doi:10.1371/journal. pone.0246283
46. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. Tu WJ, ed. PLOS ONE. 2020;15 (5):e0233668. doi:10.1371/journal.pone.0233668
47. Kaungav SB. How have Malawi’s courts affected the country’s epidemic response? The London School of Economics and Political Science (LSE). November 13, 2020. https://blogs.lse.ac.uk/africaatlse/2020/11/13/how-have-malawis-courts-law-affected-epidemic-response/
48. Mzumara GW, Chawani M, Sakala M, et al. The health policy response to COVID-19 in Malawi. BMJ Glob Health. 2021;6(5):e006035. doi:10.1136 /bmjgh-2021-006035
49. Moradzadeh R, Nazari J, Shamsi M, Amini S. Knowledge, Attitudes, and Practices Toward Coronavirus Disease 2019 in the Central Area of Iran: A Population-Based Study. Front Public Health. 2020;8:599007. doi:10.3389/fpubh.2020.599007
50. Pan American Health Organization (PAHO). Haiti receives 500,000 vaccines donated by the United States through COVAX. PAHO: Pan American Health Organization. Accessed July 8, 2024. https://www.paho.org/en/stories/haiti-receives-500000-vaccines-donated-united-states-through-covax
51. World Health Organization. WHO COVID-19 dashboard. World Health Organization Data. Accessed October 26, 2024. https://data.who.int/dashboards/covid19/vaccines
52. Nkambule E, Mbakaya BC. COVID-19 vaccination hesitancy among Malawians: a scoping review. Syst Rev. 2024;13(1):77. doi:10.1186/s1364 3-024-02499-z
53. Sethy G, Chisema MN, Sharma L, et al. ‘Vaccinate my village’ strategy in Malawi: an effort to boost COVID-19 vaccination. Expert Rev Vaccines. 2023;22(1):180-185. doi:10.1080/14760 584.2023.2171398
54. Bwanali AN, Lubanga AF, Mphepo M, Munthali L, Chumbi GD, Kangoma M. Vaccine hesitancy in Malawi: a threat to already-made health gains. Ann Med Surg. 2023;85(10):5291-5293. doi:10.1097/ MS9.0000000000001198
55. Goel K, Sen A, Goel P, et al. Assessment of COVID-19 Vaccination Intention Among Community Health Workers: a Web-based Cross-sectional Survey During the First Wave of the Pandemic in India. Published online July 8, 2021. doi:10.21203 /rs.3.rs-675407/v1
56. Avahoundje EM, Dossou JP, Vigan A, et al. Factors associated with COVID-19 vaccine intention in Benin in 2021: A cross-sectional study. Vaccine X. 2022;12:100237. doi:10.1016/j.jvacx. 2022.100237
57. Eyal K, Njozela L, Köhler T, et al. Correlates of COVID-19 vaccination intentions and opinions about mandates among four groups of adults in South Africa with distinct vaccine intentions: evidence from a large national survey. BMC Public Health. 2023;23(1):1767. doi:10.1186/s12889-023-16584-w
58. Nomura S, Eguchi A, Yoneoka D, et al. Reasons for being unsure or unwilling regarding intention to take COVID-19 vaccine among Japanese people: A large cross-sectional national survey. Lancet Reg Health – West Pac. 2021;14:100223. doi:10.1016/j. lanwpc.2021.100223
59. Sánchez-González L, Major CG, Rodriguez DM, et al. COVID-19 Vaccination Intention in a Community Cohort in Ponce, Puerto Rico. Am J Trop Med Hyg. 2022;107(2):268-277. doi:10.4269/ ajtmh.22-0132
60. PIH’s Strategy for Achieving Equity in COVID-19 Vaccination. Partners In Health. Accessed November 14, 2024. https://www.pih.org/learning-collaborative/pihs-strategy-achieving-equity-covid-19-vaccination
61. Warren AM, Bennett MM, Da Graca B, et al. Intentions to receive COVID-19 vaccines in the united states: Sociodemographic factors and personal experiences with COVID-19. Health Psychol. 2023;42(8):531-540. doi:10.1037/hea0001225