





Outpatient Monitoring for High-Risk Pregnancies
Outpatient Monitoring of High-Risk Pregnancies: An Update of Management in a Tertiary Obstetric Center and Review of the Literature
Joanna I. Choi-Klier¹, Stephanie M. Masters¹, Danielle S. Lewis¹, Hari Eswaran², Nirvana Manning², Everett F. Magann¹²*
- Departments of Obstetrics and Gynecology, Virginia Tech Carilion School of Medicine, Roanoke, Virginia
- Departments of Obstetrics and Gynecology, University of Arkansas for the Medical Sciences, Little Rock, Arkansas
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Choi-Klier, J.I., Masters, S.M., et al., 2024. Outpatient Monitoring of High Risk Pregnancies: An Update of Management in a Tertiary Obstetric Center and Review of the Literature. Medical Research Archives, [online] 12(11).
https://doi.org/10.18103/mra.v12i11.6086
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.6086
ISSN 2375-1924
ABSTRACT
Importance:
Hospital closures and the increasing lack of maternity care in rural areas is leading to greater distances traveled for obstetric care, delivery and specialized obstetric care particularly in rural areas of the United States.
Objectives:
The aim of this study was to update management in a tertiary obstetric center and review the literature on antenatal management of high-risk pregnancies on an outpatient versus inpatient basis.
Evidence Acquisition:
Electronic databases (PubMed, OVID, and EMBASE) were searched from 1990 – 9/2024 for English language abstracts. Studies were selected which examined outpatient compared with inpatient management of pregnancy at risk for adverse maternal and/or perinatal outcomes.
Results:
The evolution of our program from the first publication that covered 9/2007 to 12/2012 is updated through 12/20/23. Basic services, admitting diagnosis, costs, maternal fetal outcomes, benefits and drawbacks to patients and families, and new developments are brought up to date. Our literature review identified 282 abstracts of which 28 articles became the basis of this review. Pregnancy outcomes comparing inpatient versus outpatient management include hypertension, preterm premature rupture of the membranes, preterm labor, diabetes, hyperemesis gravidarum, cost, psychological impact, and satisfaction.
Conclusions:
Our outpatient program has evolved since 2012 into a low-cost, efficient monitoring program for our referred high-risk pregnancies. A review of outpatient/day care units demonstrates that they can safely provide monitoring for high-risk pregnancies.
Introduction
The management of pregnancies at risk for adverse pregnancy outcomes referred to tertiary obstetric centers from rural hospitals is problematic and increasing. The distances that must be traveled by patients for obstetric care also is increasing. A recent report from Becker Hospital Review revealed that 703 United States hospitals are at risk for closure. In our state, 25 hospitals are at risk of closure in the next 6–7 years and 13 are at immediate risk of closure in the next 2–3 years¹. These closures will result in greater distances traveled for obstetric care and delivery. A recent report from the March of Dimes titled “Do you live in a maternity care desert?” emphasizes the increasing lack of maternity care in parts of the US with over 35% of counties not having birth hospitals, birth centers offering obstetric care, or obstetric providers².
High risk pregnancies referred for obstetric management and/or delivery, if not delivered soon after arrival but the reason for referral persists, may need to be monitored and managed at a tertiary center. Likewise, even low-risk patients who travel long distances for obstetric care may have obstetrical complications occurring during the pregnancy that necessitate the patients be managed either in the hospital or as an outpatient near the hospital rather than traveling back and forth over long distances to their homes. A study found that overall, 8.7% of women were hospitalized during their pregnancy. Of these, 5.7% were hospitalized and discharged while pregnant, 0.8% experienced extended stays before a live birth³. Women in both groups, if they can be managed as outpatients near the referral hospital can then be managed safely and cost effectively within a structured antenatal management program⁴. Antenatal day care units were introduced in the 1980s as an alternative to inpatient care for women with pregnancy complications such as mild and moderate hypertension and preterm prelabor rupture of membranes⁵. These units offer comprehensive care with medical support staff on site and women undergo the same testing as they would as an inpatient with the thought to reduce overnight hospital stays and costs. A Cochrane review comparing these units and hospital admission for women with pregnancy complications showed a reduction in length of antenatal hospital stays for women in the day care units with similar maternity and perinatal outcomes and overall satisfaction in quality of care; however, women preferred antepartum units to hospital admissions⁵. Similarly, the Maternal fetal medicine service at Albany Medical Center Hospital lodged 41 selected antepartum patients at Ronald McDonald House (RMH) to avoid costs of hospitalization and provide a more home-like environment as an alternative to inpatient care and found no adverse perinatal outcomes and was a cost-effective alternative⁶.
The purpose of the review is to update our program for the outpatient monitoring of high-risk pregnancies in the state’s only tertiary obstetric center. This study will also do a comprehensive review on the management of high-risk pregnancies on an outpatient basis versus inpatient monitoring of at-risk pregnancies.
Materials and Methods:
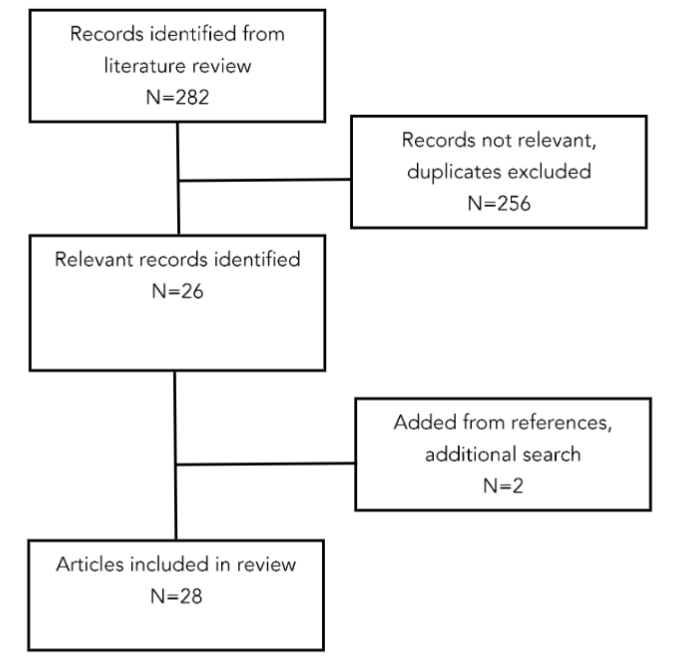
A literature search was undertaken by our university librarian using the search engines Medline, OVID, and EMBASE. Search terms used included “Antenatal management (Mother’s house and Ronald McDonald house)” OR Antenatal care OR Obstetric OR “Day care” OR “antenatal hospitalization” OR “residence” OR “residential facilities” AND “Pregnancy, High Risk” OR “Eclampsia” OR “Labor, premature” OR “Childbirth” OR “Management of labor” OR Pregnancy complications OR Fetal abnormalities OR “Congenital hereditary, and Neonatal Diseases and Abnormalities” OR “Polyhydramnios” OR Oligohydramnios OR “Abruption Placenta”. The years searched were 1990 – 9/2024. The only limitation was that the articles had to be in English. There were 282 articles identified. Two of the authors (JCK, EFM) reviewed the abstracts for relevance to monitoring high risk patients on an outpatient basis or in the hospital. Full articles of the identified relevant abstracts were read. Inclusion criteria for this review included articles that discussed high risk pregnancies and compared outpatient versus inpatient management. The references of the selected articles were reviewed for additional applicable articles. There were 28 articles selected as the basis for this review. (Figure 1)
Figure 1:
The Continuing Antenatal Management Program (CAMP)
We first reported on the first four years of our program, September 2007 through December 2012, in 2015⁴. This program continues and has evolved since our publication in December of 2015, and we now report that progression.
Basic Services Provided at CAMP (Continuing Antenatal Management Program)
Several hotels have been used for our CAMP services. These hotels agree to provide 24-hour transportation to the University Hospital and to weekly or bi-weekly visits to our maternal fetal medicine (MFM) clinics. All patients receive their care through our MFM clinic while a patient is at CAMP. All the hotels we have used are within 3 km of the University hospital and clinics. There is daily contact with one of our outreach nurses to monitor the patient’s progress and for any concerns of the patient. The patients are also given a nurse contact number that they can call 24 hours a day. In the beginning patients could only have one adult stay with her in CAMP. This has now been modified to allow the patient’s children to visit but there must always be another adult to care for the children if the patient must urgently go to the hospital.
Admitting Diagnosis
The admitting diagnoses in the original study were preterm labor, fetal anomalies, maternal cardiac disease, autoimmune disorders, genetic conditions, preterm premature rupture of the membranes, fetal growth restriction, monochorionic monoamniotic twin pregnancy and oligohydramnios. Since the original study, additional admitting diagnoses include twin and triplet pregnancies, gestational hypertension with superimposed preeclampsia, rule out preeclampsia, and placental abnormalities. The number of women who are admitted with pregnancies that have fetal anomalies has increased considerably. The State’s children’s hospital is not located on the same campus as the University Hospital but is only a few miles away and both hospitals are linked by a specialized neonatal transportation system. The children’s hospital does not do deliveries and those pregnancies with anomalies or those who will need immediate care in a specialized children’s hospital are delivered at the University hospital and subsequently transferred to the children’s hospital.
Many of these pregnancies with anomalies may need immediate surgery or specialized care after delivery that cannot be offered at smaller hospitals. To ensure that these deliveries occur in the University hospital when the patient may live many hours away, these patients are housed in CAMP during their final days or weeks of their pregnancies.
Costs
The average daily cost at CAMP from 2007 through December of 2012 was $92 per day (cost of the hotel and 3 meals), which has changed minimally since 2012. The cost in September 2024 was a hotel cost of $71 per day and the cost of meals was $25 per day. If the patient is diabetic, the cost increases to $30 per day. There is also a delivery fee of $25 per day no matter how many meals are delivered. All costs for CAMP are paid by the University, and there are no costs to the patient for meals and lodging. The in-hospital cost in our original study averaged $1782 per day.
Current cost estimates for inpatient hospital care at our hospital range from $3537.33 to $5157.72 per day. If we calculate the cost of CAMP versus inpatient management the differences are substantial. Since December of 2012, there were 1023 women housed in CAMP for an average of 34.5 days (about 1 month 8 days). The comparison of cost between CAMP is for the housing and meals for 35,293.5 days. The CAMP cost calculated with the $5 diabetes surcharge included for all women but without the $25 charge for delivery of the meals is $3,529,300. A calculation charge of 35,293 in hospital patient days using the lowest hospital cost would be $124,831,341, a difference in savings of over $121,000,000.
Maternal Fetal Outcomes
In the initial CAMP assessment of 426 pregnant women housed in CAMP there were no adverse maternal or perinatal outcomes and no intrauterine fetal demises. In our follow up evaluation of an additional 1023 pregnant women, we have had no adverse maternal or perinatal outcome, no intrauterine fetal demises, and no events requiring emergency transport back to the hospital.
Benefits to the patient:
For those patients whose pregnancy is complicated by diabetes and/or hypertension, they receive additional training and information about their disease process as they are counseled daily. This reinforces positive steps toward better control and with less stress compared to that in the hospital setting. The patients have extremely easy and quick access to transportation to and from the hospital and to their clinic appointments, which provides decreased overall travel time and expenses for food and lodging.
Drawbacks to patient and family:
The primary drawback occurs if the patient has other children who cannot stay with their mother. Other children may visit but there must always be another adult present who can take care of the children if the mother must go to the hospital at a moment’s notice. Additionally, the mother is not there for household management and/or help with their children’s activities, cannot work (unless she can work remotely) and is not near her family and support groups which could cause sleep issues or stress.
What is new in CAMP? (Continuing Antenatal Management Program)
Remote patient monitoring (RPM) is well-suited for a CAMP based program. With several devices available including remote blood pressure, glucose and NST (non-stress test) monitoring, it is possible to provide continuous monitoring and care in a location outside of the hospital setting. The data from most of the RPM devices are aggregated in a single portal and is accessible in the electronic health record, which is EPIC in our case. This provides seamless monitoring of the patient by the clinical staff or the call center where alarms and alerts are received if there are any adverse conditions. We believe this model, backed up by our 24/7 nurse call center, would help improve patient safety and satisfaction. We have implemented a small pilot in CAMP and are working on optimizing this approach.
Patient satisfaction survey data:
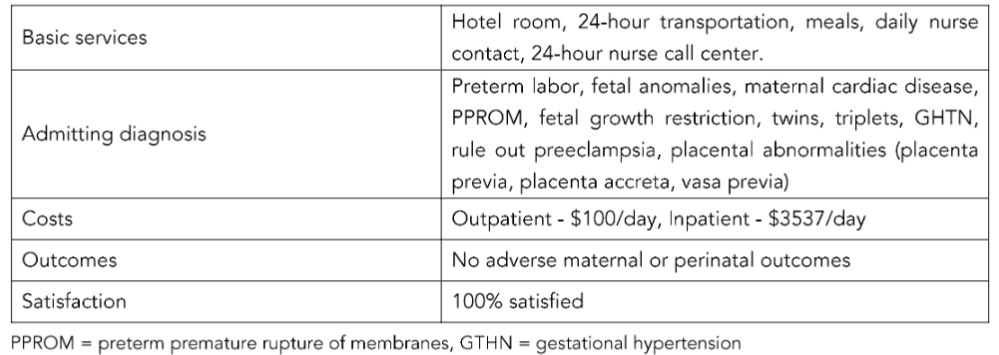
In our last survey of satisfaction with CAMP in July 2023, all 109 surveys gave the program a 100% satisfaction score. (Table 1)
Table 1: CAMP Services (Continuing Antenatal Management Program)
Discussion:
High risk antepartum care is critical yet costly. Antenatal day care units are an alternative to inpatient management without compromising maternal or fetal well-being. Some facilities have adopted this concept to reduce overall health care costs but should be considered at other tertiary care systems. Implementation of this concept can help contribute towards solving the maternity desert issue.
These antenatal daycare facilities are not limited to the United States. Countries that have a high maternal mortality rate have implemented this concept through maternity waiting homes as a strategy to decrease maternal mortality. Important causes of perinatal deaths in developing countries include obstructed labor, prematurity, and antepartum hemorrhage. Additionally, many barriers exist in countries such as Cuba, Haiti, Zambia, and Zimbabwe in accessing care. The World Health Organization (WHO) considers maternity waiting homes (MWH) as an essential element of maternity care. These homes have been suggested in rural areas where women live far from a health facility and transport is poor and often impossible when complications of labor occur. The implementation of a maternity waiting home in Zambia showed that in more high-risk pregnancies, the outcome was not worse compared to the non-waiter group and perinatal mortality was similar.
trial showed that outpatient monitoring might be as safe as a hospital admission¹⁵.
The most recent Cochrane Systematic Review compared antenatal day care units with hospital admissions for women with high blood pressure and those with preterm pre-labor rupture of the membranes. Only 3 trials with 504 participants were identified that met the review criteria. The review found that women receiving daycare had to make more visits to the hospital but were less likely to stay in the hospital overnight. Overall maternal and neonatal outcomes were similar among groups suggesting no major differences in clinical outcomes between groups. Evidence about the cost was mixed. Although the hospital stay length was reduced in the group in the daycare units, this did not translate into reduced healthcare costs¹⁶.
Similar findings have been reported in patients with pregnancy-related hypertensive disorders. Twaddle compared the efficiency of management of hypertension in pregnancy between a daycare model and traditional inpatient management. They found no difference between groups for gestation at delivery, mode of delivery, birthweight, Apgar scores, and admission to the special care baby unit¹⁷.
Giannubilo et al., found that patients with gestational hypertension that were managed in ambulatory day centers had higher gestational age at delivery (38 ± 1.7 vs 35.5 ± 2.3 weeks; p < 0.001), higher birth weight (3251 ± 389 vs 2271 ± 759.1 g; p < 0.001), longer time to delivery (62.0 ± 4.8 vs 31.3 ± 5.4 days; p < 0.001), and lower NICU admission (21.3% vs 0%; p < 0.001) than patients with the same medical conditions that were managed inpatient¹⁸.
Outcomes were noted to be similar for patients with mild preeclampsia who were managed outpatient compared to those with inpatient management for gestational age at delivery (37 ± 1.2 vs 34.4 ± 1.7 weeks), birth weight (3168 ± 363 vs 2196 ± 685.17 g), time to delivery (55.4 ± 6.9 vs 35.3 ± 4.5 days), and lower NICU admission (15.6% vs 35.5%)¹⁹.
Another consideration in assessing the benefit of outpatient centers is the cost in comparison to traditional inpatient management for antenatal care. A study by Barton et al compared differences in cost for patients with a diagnosis of pregnancy-related hypertension managed as an outpatient compared to those managed inpatient. Of those included in the study, 14.3% of patients had progression to severe preeclampsia and 24.8% required eventual antenatal hospital admission. When comparing patients with similar clinical status, inpatient antepartum charges averaged $10,327 vs. $5,439 for patients in the antenatal outpatient program²⁰.
Similarly, an Australian retrospective analysis was conducted to compare outcomes and cost-effects between patients with hypertension that received surveillance and assessment in a day stay facility and those who had inpatient stay. Since the development of the outpatient facility, Pregnancy Day Care Centre, the authors found a reduction in the number of antenatal ward admissions. They also noted reduced total cost in the outpatient group with the average cost being $684.85 less than inpatient antenatal admission. A survey reported that the majority of patients in the outpatient group preferred short day care as it was less disruptive to their personal lives than inpatient stay²¹. This supports the idea that outpatient centers can provide not only monetary relief but also less disruption of patients’ personal lives.
DIABETES
Hyperglycemia has also been studied in an inpatient versus outpatient setting. Cavassini et al., examined the cost-benefit relationship and social profitability ratio of hospitalization compared with outpatient management for pregnant women with pregestational and gestational diabetes or mild hyperglycemia. Treatment success was assessed based on the following maternal and perinatal parameters: mean glycemia ≤ 120 mg/dl, vaginal delivery, gestational age at birth ≥ 37 weeks, weight adequate for gestational age (AGA), ponderal index < 2.5, infant rooming-in, no maternal mortality and no perinatal mortality. The mean maternal glycemia, cesarean delivery rate and ponderal index in infants born to mothers with diabetes or hyperglycemia were higher among inpatients than among outpatients.
The analyses on both the inpatient and the outpatient care provided to pregnant women with diabetes or mild hyperglycemia revealed that the benefits in monetary units were greater than the investment costs. The cost-benefit analysis indicated that managing diabetic pregnant women on an outpatient basis was economically more advantageous than hospitalization and should be encouraged²².
HYPEREMESIS GRAVIDARUM
Day management of nausea and vomiting was introduced at a London hospital in 2003. This small prospective study discharged all patients within 24 hours with no readmissions. The satisfaction rate was 88% on a satisfaction survey. The authors suggested that day management was feasible and should be encouraged²³. A randomized controlled trial compared day care compared with inpatient care for treatment of nausea and vomiting of pregnancy. In the day care arm compared to the inpatient arm, the time of resolution of the nausea and vomiting was significantly shorter (p < 0.001), the total number of inpatient admissions was less (p < 0.001) and there was no difference in the women’s satisfaction of their treatment (p = 0.73)²³. A third trial was a cost effectiveness study of day care compared with inpatient management of nausea and vomiting in Ireland and determined that day care was 70% more cost effective than inpatient management²⁴.
PSYCHOSOCIAL IMPACT
Overall, the overwhelming view of daycare is positive. A study carried out at Glasgow Royal Maternity Hospital examined women’s perceptions of the care they received for hypertension during pregnancy at a daycare unit. The report indicated that none of the women would rather be hospitalized with the majority (57%) stating that they were prepared to attend day care five times a week to avoid admission. Women expressed an emphasis on reassurance and monitoring as a main benefit in coming to day care¹⁷. Similarly, a study investigating perceptions of bed rest by women with high-risk pregnancies showed that a predominant concern among hospitalized women was separation from home and family, in addition to lack of privacy, negative experiences with roommates, negative emotional experiences like depression and loneliness, and difficulties with partner relationships. Although women at home enjoyed being able to spend more time with their children, they also expressed the frustration in letting other caregivers take over home responsibilities, role reversals, and temptation to do more than recommended by their doctor. Although inpatient versus outpatient treatment has disadvantages and advantages, bed rest in the hospital appeared to be associated with more sources of stress²⁵.
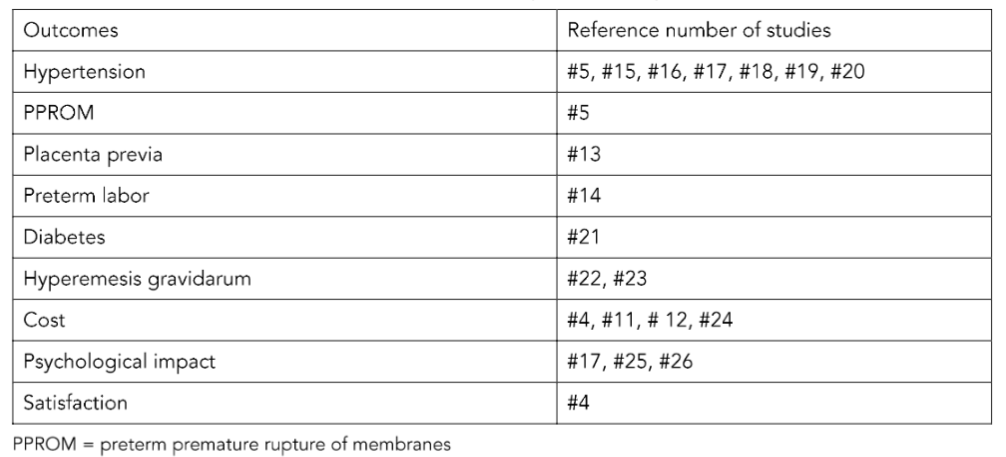
Turnbull et al., examined the psychosocial outcomes of antenatal day care for three medical complications of pregnancy including non-proteinuric hypertension, proteinuric hypertension, and preterm premature rupture of membranes (PPROM), where the trial participants were randomly assigned in a ratio of two to one between day care and antenatal ward. In relation to safety, it found no significant differences in maternal or perinatal outcomes. The cost of an episode of care and cost per day appeared similar across the two groups, which provided evidence that day care was at least as cost effective and more so than standard care, given that the outcomes were similar or favored the day-care group. Overall, it concluded that day care can reduce antenatal and overall stay without sacrificing reassurance or increasing stress²⁶. (Table 2)
Table 2: Review of Pregnancy Outcomes Evaluated: Outpatient vs. In patient
Conclusion
In summary, day care units provide access to intensive monitoring for high risk, obstetric patients. Multiple studies have shown this concept of antenatal day care units to be a safe and effective alternative. These units can be a safety net facility for community-based services; however, these units require senior obstetrical supervision and review²⁷. Similarly, maternity waiting homes seem in developing countries are appropriate in certain settings, but it does require a high degree of coordination between peripheral prenatal care services and second and third level health care facilities²⁸. The impact of this outpatient antenatal care model is reflected in better maternal and neonatal outcomes, lower costs, and overall better patient satisfaction in the current literature when comparing it to traditional inpatient management.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
There was no funding for this work.
Acknowledgements:
We would like to thank Donna Eastham, BA for her help in gathering information, editing, and submission. We would like to thank Susan H. “Beth” Fogleman and Wanda L. Standridge for their work in compiling data.
References
1. Gamble, M. (2024, August 5). 703 hospitals at risk of closure, state by state. Becker’s Hospital CFO Report. https://www.beckershospitalreview.com/finance/703-hospitals-at-risk-of-closure-state-by-state.html
2. Stoneburner A, Lucas R, Fontenot J, Brigance C, Jones E, DeMaria AL. Nowhere to Go: Maternity Care Deserts Across the US. (Report No 4). March of Dimes. 2024. https://www.marchofdimes.org/ maternity-care-deserts-report
3. Gazmararian, J. A., Petersen, R., Jamieson, D. J., Schild, L., Adams, M. M., Deshpande, A. D., & Franks, A. L. (2002). Hospitalizations during pregnancy among managed care enrollees. Obstetrics and gynecology, 100(1), 94–100. https://doi.org/10.1016/s0029-7844(02)02024-0
4. Hughes, D. S., Ussery, D. J., Woodruff, D. L., Sandlin, A. T., Kinder, S. R., & Magann, E. F. (2015). The continuing antenatal management program (CAMP): Outpatient monitoring of high-risk pregnancies. Keeps patients safe, costs low and care nearby. Sexual & reproductive healthcare: official journal of the Swedish Association of Midwives, 6(2), 108–109. https://doi.org/10.1016/j.srhc.2015.01.001
5. Dowswell, T., Middleton, P., & Weeks, A. (2009). Antenatal day care units versus hospital admission for women with complicated pregnancy. The Cochrane database of systematic reviews, 2009(4), CD001803. https://doi.org/10.1002/14651858.CD001803.pub2
6. Dexter, S. C., Klein, K. A., Clark, D. A., Ross, S. L., & Veille, J. C. (2004). The Ronald McDonald House as an alternative to antepartum hospitalization. Journal of perinatology : official journal of the California Perinatal Association, 24(10), 623–625. https://doi.org/10.1038/sj.jp.7211166
7. van Lonkhuijzen, L., Stegeman, M., Nyirongo, R., & van Roosmalen, J. (2003). Use of maternity waiting home in rural Zambia. African journal of reproductive health, 7(1), 32–36.
8. Hossain, Semonti K. BS; Porter, Emily L. BA; Redden, Lisa M. BA; Pearlmutter, Mark D. MD. Maternity Waiting Home Use and Maternal Mortality in Milot, Haiti. Obstetrics & Gynecology 123():p 149S, May 2014. | DOI: 10.1097/01.AOG. 0000447136.92802.2a
9. Gorry C. (2011). Cuban maternity homes: a model to address at-risk pregnancy. MEDICC review, 13(3), 12–15. https://doi.org/10.37757/MR2011V13.N3.4
10. Chandramohan, D., Cutts, F., & Millard, P. (1995). The effect of stay in a maternity waiting home on perinatal mortality in rural Zimbabwe. The Journal of tropical medicine and hygiene, 98(4), 261–267.
11. Bivins, H. A., Jr, McCallum, O. J., & Roegge, D. D. (2007). The Mother’s House: a new concept in antepartum care. American journal of obstetrics and gynecology, 197(2), 201.e1–201.e201004. https://doi.org/10.1016/j.ajog.2007.04.045
12. Droste, S., & Keil, K. (1994). Expectant management of placenta previa: cost-benefit analysis of outpatient treatment. American journal of obstetrics and gynecology, 170(5 Pt 1), 1254–1257. https://doi.org/10.1016/s0002-9378(94)70136-9
13. Wing, D. A., Paul, R. H., & Millar, L. K. (1996). Management of the symptomatic placenta previa: a randomized, controlled trial of inpatient versus outpatient expectant management. American journal of obstetrics and gynecology, 175(4 Pt 1), 806–811. https://doi.org/10.1016/s0002-9378(96)80003-2
14. Ambrose, S., Rhea, D. J., Istwan, N. B., Collins, A., & Stanziano, G. (2004). Clinical and economic outcomes of preterm labor management: inpatient vs outpatient. Journal of perinatology : official journal of the California Perinatal Association, 24(8), 515–519. https://doi.org/10.1038/sj.jp.7211139
15. Bekker, M. N., Koster, M. P. H., Keusters, W. R., Ganzevoort, W., de Haan-Jebbink, J. M., Deurloo, K. L., Seeber, L., van der Ham, D. P., Zuithoff, N. P. A., Frederix, G. W. J., van den Heuvel, J. F. M., & Franx, A. (2023). Home telemonitoring versus hospital care in complicated pregnancies in the Netherlands: a randomised, controlled non-inferiority trial (HoTeL). The Lancet. Digital health, 5(3), e116–e124. https://doi.org/10.1016/S2589-7500(22)00231-X
16. Dowswell, T., Middleton, P., & Weeks, A. (2009). Antenatal day care units versus hospital admission for women with complicated pregnancy. The Cochrane database of systematic reviews, 2009(4), CD001803. https://doi.org/10.1002/14651858.CD001803.pub2
17. Twaddle S. (1995). Day care for women with high-risk pregnancies. Nursing times, 91(4), 46–47.
18. Giannubilo, S. R., Bezzeccheri, V., Landi, B., Battistoni, G. I., Stortoni, P., Vitali, P., & Tranquilli, A. L. (2012). PP047. Outpatient management of pregnancy complicated by mild hypertensive disorders. Pregnancy hypertension, 2(3), 267. https://doi.org/10.1016/j.preghy.2012.04.158
19. Barton, J. R., Istwan, N. B., Rhea, D., Collins, A., & Stanziano, G. J. (2006). Cost-savings analysis of an outpatient management program for women with pregnancy-related hypertensive conditions. Disease management: DM, 9(4), 236–241. https://doi.org/10.1089/dis.2006.9.236
20. Dunlop, L., Umstad, M., McGrath, G., Reidy, K., & Brennecke, S. (2003). Cost-effectiveness and patient satisfaction with pregnancy day care for hypertensive disorders of pregnancy. The Australian & New Zealand journal of obstetrics & gynaecology, 43(3), 207–212. https://doi.org/10.1046/j.0004-8666.2003.00061.x
21. Cavassini, A. C., Lima, S. A., Calderon, I. M., & Rudge, M. V. (2012). Cost-benefit of hospitalization compared with outpatient care for pregnant women with pregestational and gestational diabetes or with mild hyperglycemia, in Brazil. Sao Paulo medical journal = Revista paulista de medicina, 130(1), 17–26. https://doi.org/10.1590/s1516-31802012000100004
22. Alalade, A. O., Khan, R., & Dawlatly, B. (2007). Day-case management of hyperemesis gravidarum: Feasibility and clinical efficacy. Journal of obstetrics and gynaecology : the journal of the Institute of Obstetrics and Gynaecology, 27(4), 363–364. https://doi.org/10.1080/01443610701327396
23. McCarthy, F. P., Murphy, A., Khashan, A. S., McElroy, B., Spillane, N., Marchocki, Z., Sarkar, R., & Higgins, J. R. (2014). Day care compared with inpatient management of nausea and vomiting of pregnancy: a randomized controlled trial. Obstetrics and gynecology, 124(4), 743–748. https://doi.org/10.1097/AOG.0000000000000449
24. Murphy, A., McCarthy, F. P., McElroy, B., Khashan, A. S., Spillane, N., Marchocki, Z., Sarkar, R. K., & Higgins, J. R. (2016). Day care versus inpatient management of nausea and vomiting of pregnancy: cost utility analysis of a randomised controlled trial. European journal of obstetrics, gynecology, and reproductive biology, 197, 78–82. https://doi.org/10.1016/j.ejogrb.2015.10.022
25. Heaman, M., & Gupton, A. (1998). Perceptions of bed rest by women with high-risk pregnancies: A comparison between home and hospital. Birth (Berkeley, Calif.), 25(4), 252–258. https://doi.org/10.1046/j.1523-536x.1998.00252.x
26. Turnbull, D. A., Wilkinson, C., Gerard, K., Shanahan, M., Ryan, P., Griffith, E. C., Kruzins, G., & Stamp, G. E. (2004). Clinical, psychosocial, and economic effects of antenatal day care for three medical complications of pregnancy: a randomised controlled trial of 395 women. Lancet (London, England), 363(9415), 1104–1109. https://doi.org/10.1016/S0140-6736(04)15893-5
27. Walker J. J. (1993). Day care obstetrics. British journal of hospital medicine, 50(5), 225–226.
28. Figà-Talamanca I. (1996). Maternal mortality and the problem of accessibility to obstetric care; the strategy of maternity waiting homes. Social science & medicine (1982), 42(10), 1381–1390. https://doi.org/10.1016/0277-9536(95)00286-3