





Surgical Technique for Treating Bone Defects in Knee Arthroplasty
Description of a Surgical Technique for the Treatment of Bone Defects in Knee Arthroplasties: Modified Stonehenge
João Gabriel de Cerqueira Campos Villardi¹,³, Caio Lima de Mello¹, Leonardo Calaza Machado⁵, Matheus Weihermann Guesser⁷, Rafael Erthal de Paula¹,³, Raphael Serra Cruz³,⁶,⁷, Tiago Carminatti¹,³, Alfredo Marques Villardi²,³,⁴
- MD; Member of the Knee Surgery Group at Hospital São Vicente de Paulo, Rio de Janeiro, Brazil.
- Head of the Knee Surgery Group at Hospital São Vicente de Paulo, Rio de Janeiro, Brazil.
- MSc.
- PhD.
- Medical Academic – Vassouras University
- MD; Hospital Vera Cruz – Hospital Regional de Piracicaba São Paulo, Brazil.
- Former Member of the Knee Surgery Group at Hospital São Vicente de Paulo, Rio de Janeiro, Brazil.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Villardi, JGDCC., Mello, CLD., et al., 2024. Description of a Surgical Technique for the Treatment of Bone Defects in Knee Arthroplasties Modified Stonehenge. Medical Research Archives, London 12(11).
https://doi.org/10.18103/mra.v12i11.6030
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.6030
ISSN 2375-1924
ABSTRACT
Bone loss can be a major problem in knee arthroplasties. Although bone defects are more common in revision arthroplasties, the need for bone reconstruction and removal of material, they can also occur in primary arthroplasties, due to some factors, such as inflammatory arthropathies, long waiting times for surgery, sequelae of fractures or infection, among others. There are several classifications described in the literature that can be useful, not only for planning bone loss in arthroplasties, but also to serve as a treatment guide. The AORI classification is one of the most used and it is the one we prefer because it has good reproducibility and gives a better understanding of how to fill defects and the indication of the technique to be used. Lombardi’s classification, in addition to defining the depth of the defects, describes the characteristics of the defect and its containment. In this report, we describe a surgical technique for the treatment of bone defects in knee arthroplasties, which we call the Modified Stonehenge technique, and we present its advantages and disadvantages.
Keywords: bone defects, knee arthroplasties, surgical technique, Modified Stonehenge
Introduction
Bone loss can be a major problem in knee arthroplasties. Although bone defects are more common in revision arthroplasties, due to loosening, infection and removal of material, they can also occur in primary arthroplasties, due to some factors, such as inflammatory arthropathies, long waiting times for surgery, sequelae of fractures or infection, among others. There are several classifications described in the literature that can be useful, not only to quantify bone loss in arthroplasties, but also to serve as a treatment guide. The AORI classification¹ is one of the most used and it is the one we prefer because it has good reproducibility² and guides the treatment on how to fill defects and indicates the degree of implant constriction and the use of intramedullary stem. Lombardi’s classification³, in addition to considering the depth of the defects, also considers the difference between contained or not contained defects, depending on the integrity of the bone ring. This also serves as a treatment guide, by combining these two requirements, through the algorithm proposed by the author.
There are several proposals for correcting the bone defect, according to its extent, depth and containment, including bone cement, cement with metal support, homologous or heterologous bone grafting, metal wedges, trabeculated metal cones and sleeves. Given the numerous available options, it is worth highlighting the importance of pre-operative planning, especially in complex primary arthroplasties or arthroplasty revisions, to choose the best method of correcting bone defects. This includes considering the possible need to use stems, fill large metaphyseal or meta-diaphyseal defects with cones or sleeves made of porous material, or even determining the degree of constriction of the implant, based on bone loss and ligament integrity. Therefore, it is important to have the necessary materials available during surgery for each case, ensuring an adequate regular support surface for the prosthesis components in order to allow correct alignment of the knee and stability of its components, thus guaranteeing a long-lasting arthroplasty.
The original technique described by Keblish⁴ was based on the principle of cortico-cancellous strut autografting, which resembled vertical support piles, reminiscent of the Stonehenge structure located on Salisbury Plain, in the county of Wiltshire, England, hence the name of the technique.
One of the most important modifications we propose to the original technique consists of using a single graft, preferably cortico-cancellous, modeled according to the area to be filled, impacted, and regularized, providing a greater support area, as it is one continuous surface and not multiple support points. The other modification we introduce is the deepening of the defect in its entirety, removing as much as possible of the sclerotic bone in the bed and its walls. In those not contained, we perform oblique drilling, following the orientation of the residual wall, thus preventing vertical drilling from weakening the bone wall and reducing the risk of fractures.
The objective of this report is to describe a personal surgical technique, the “Modified Stonehenge”, that allows the correction of bone defects whether contained or not, using autologous grafting with bone fragments resulting from bone cuts, which can be used in both the femur and tibia, during primary arthroplasties and revisions.
Description of the Technique
We routinely make bone cuts considering that the thickness of the cut must match the thickness of the component that will be implanted. In the tibia, we consider that the thickness of the cut must correspond to the smallest thickness of polyethylene available in each system. We are guided by the side with the least compromise to determine the height of the cut and not by the most compromised side or bone defects (Fig. 1).
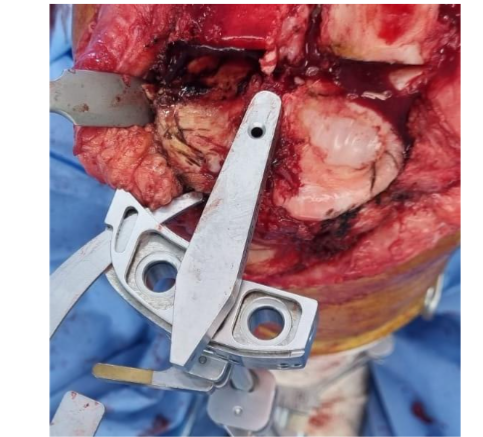
Figure 1: Positioning of the tibial cutting guide corresponding to the smallest polyethylene thickness of the system used, based on the least compromised plateau.
Source: Authors’ personal archive
We begin the Modified Stonehenge technique by evaluating the magnitude of the defect and its containment characteristics (Figs. 2 and 3).
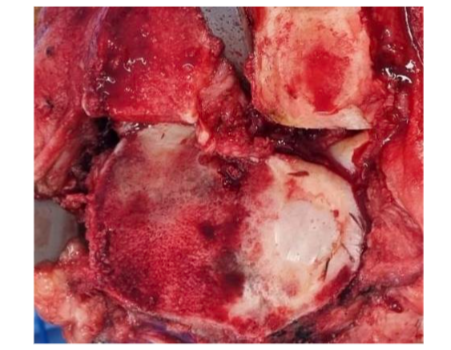
Figure 2: Tibial contained defect. The integrity of the entire bone rim is observed
Source: Authors’ personal archive
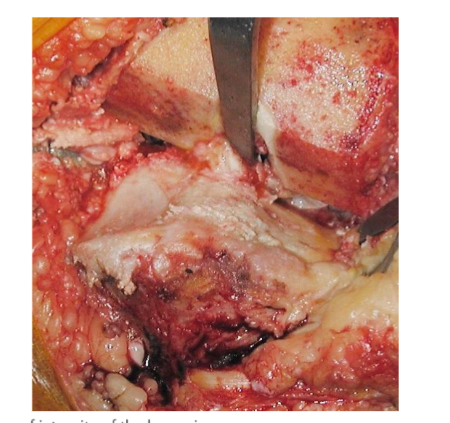
Figure 3: Uncontained tibial defect. Loss of integrity of the bone rim.
Source: Authors’ personal archive
Preparing the Bone Defect
Multiple perforations 5 to 10 mm deep are made in the defect bed, removing as much of the sclerotic bone as possible and obtaining a more vascularized and uniform defect floor for graft impaction, thereby avoiding dead space between the graft and the corresponding recipient area. Drilling can be carried out with drills available for the medullary canal or patellar pegs. (Fig. 4)
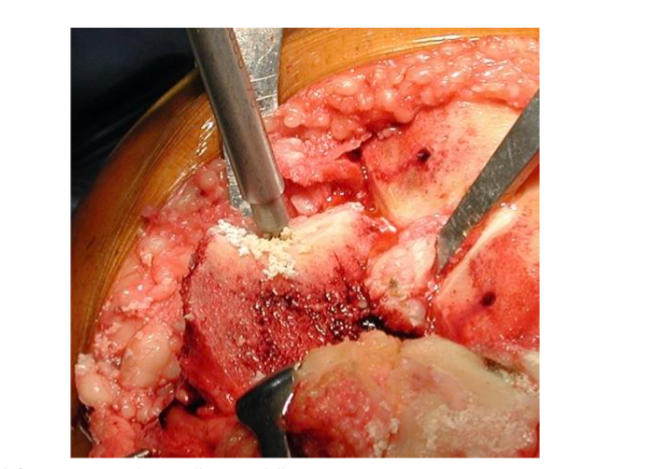
Figure 4: Drilling of the defect area using the patella pegs drill.
Source: Authors’ personal archive
Residual bone bridges formed between the perforations must be removed with gouges, osteotomes or high-speed burrs, which provide a better finish to the recipient area. (Fig. 5)
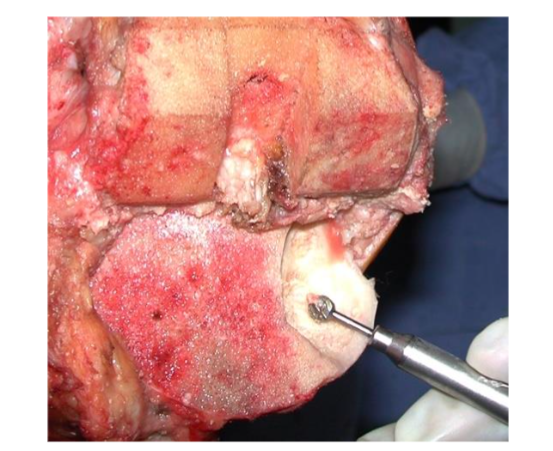
Figure 5: Preparation of the defect bed with high-speed burr.
Source: Authors’ personal archive
In uncontained defects, drilling must be carried out while respecting the angle of the entire wall below the defect. In this area, vertical perforations must be avoided to prevent perforating the wall underlying the defect and avoid the possibility of fractures in this area. (Fig. 6)
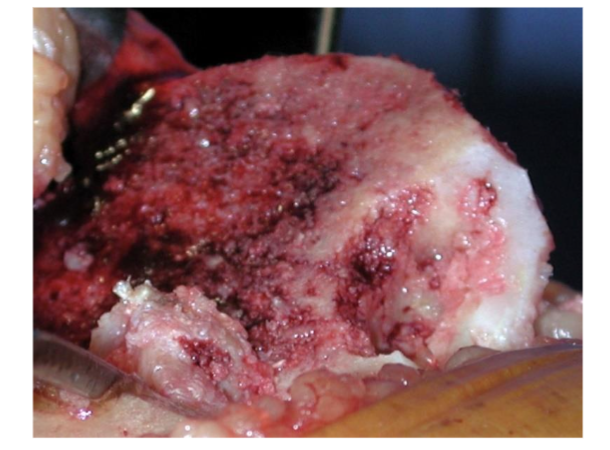
Figure 6: Final aspect of the defect bed. Perforations respect the angulation of the tibial wall.
Source: Authors’ personal archive
Preparing the Graft
The graft to be used can be obtained from residual bone from any bone cut. However, the fragments resulting from the cut of the posterior stabilization box and those from the femoral chamfers are the most frequently used. (Fig.7)
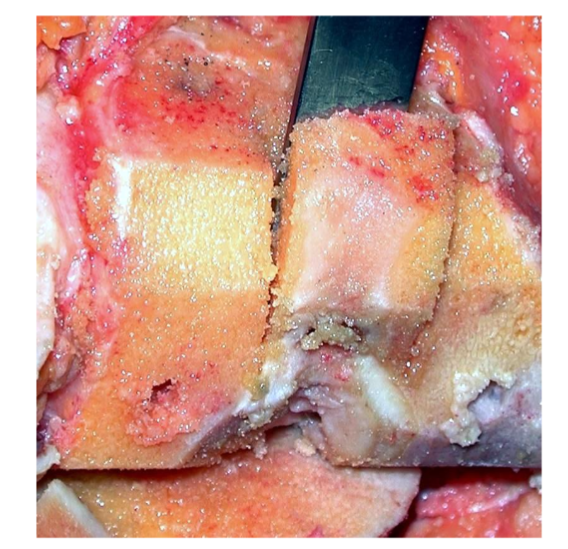
Figure 7: Bone fragment resulting from the cut of the posterior stabilization box.
Source: Authors’ personal archive
We perform mechanical cleaning of the bone fragment, which will be used as a graft, removing cartilage and soft tissues that may be adhered to the bone. The graft must be shaped into a conical shape, with sufficient height to reach the floor of the defect and exceed the cut surface. (Fig.8)
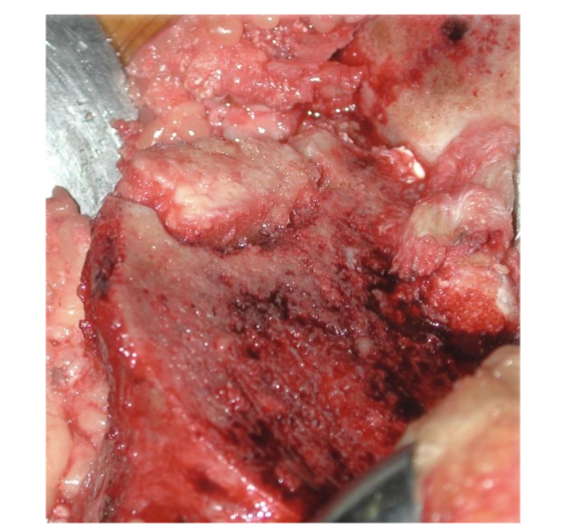
Figure 8: Graft positioned, supported on the defect bed and extending above the bone surface level.
Source: Authors’ personal archive
The width of the graft must be 1 to 2 mm greater than the width of the defect, so that the filling of the defect is press-fit. (Fig.9)
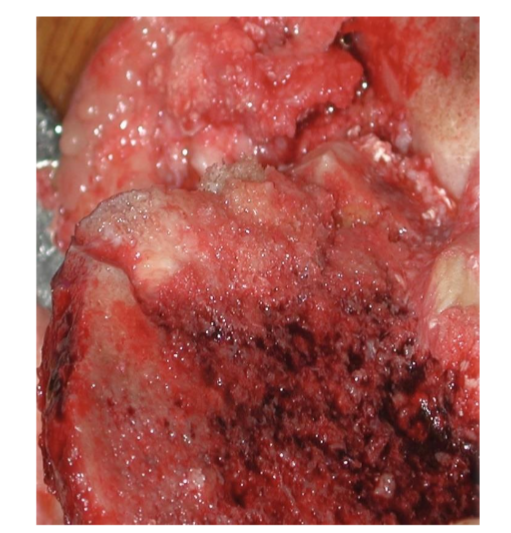
Figure 9: Graft positioned 1 to 2 mm wider than the defect.
Source: Authors’ personal archive
Impaction and Regularization of the Graft
The graft shaped is placed and then must be impacted under pressure, using an impactor wider than the graft to avoid its fracture. (Fig.10)
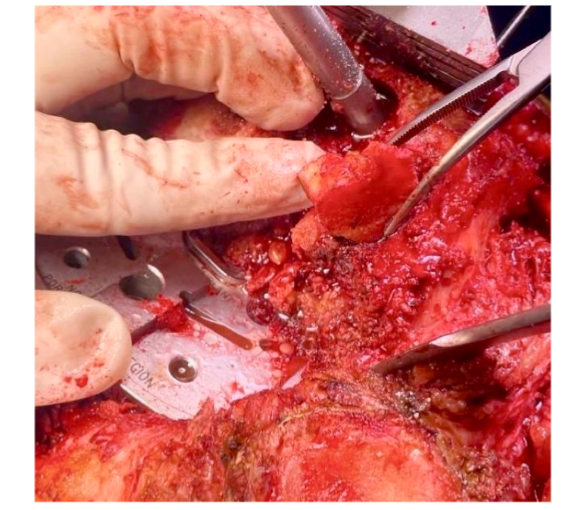
Figure 10: Placement of the shaped graft on the lateral femoral condyle in revision arthroplasty.
Source: Authors’ personal archive
Preferably, a polyethylene impactor available in different arthroplasty systems is used, or even a wide osteotome, in a horizontal position, on which the graft will be impacted until it is level with the bone surface. (Fig.11)
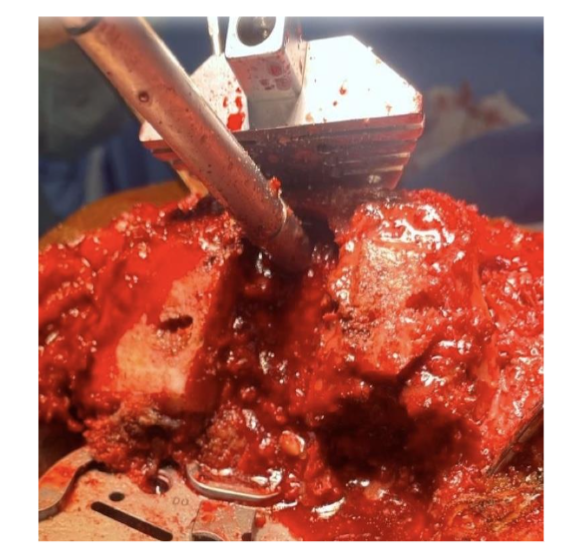
Figure 11: Impacted graft in the lateral femoral condyle.
Source: Authors’ personal archive
If, even after impaction, the graft remains above the bone surface, an oscillating saw must be used to level the graft. (Fig.12)
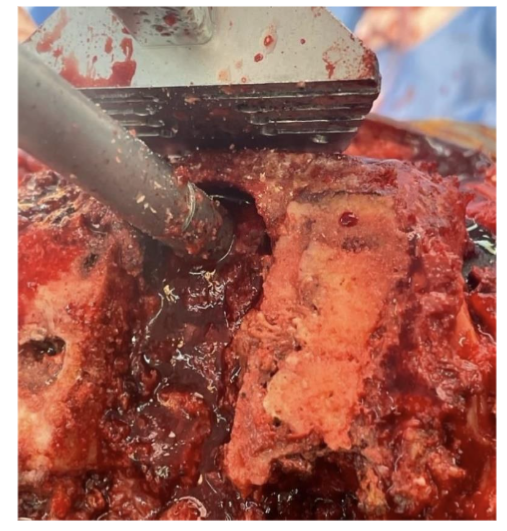
Figure 12: Graft levelled using the oscillating saw.
Source: Authors’ personal archive
If there is still a gap in the recipient area, small fragments of cancellous bone must be impacted until the defect is completely covered. (Fig.13)
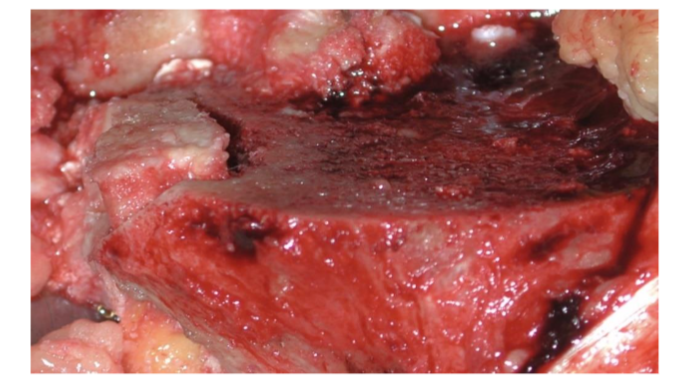
Figure 13: Graft flush with the cut surface. The space between the tibial plateau and the graft must be filled with impacted bone fragments. The appearance of the graft resembles the structure of Stonehenge.
Source: Authors’ personal archive
Once the proximal tibial bone cut is flush, using the Modified Stonehenge technique, the preparation of the tibial component bed must be carried out in the conventional way, with drilling for the stem and preparation for the delta of the definitive component, with no risk of fracture of the graft or loss of the positioning obtained. Cementation of the definitive component is also performed conventionally, with no need to modify the standardized technique, due to grafting.
Discussion
The technique described (Modified Stonehenge) allows the correction of bone defects whether contained or not, using autologous grafting, with bone fragments resulting from bone cuts, which can be used in both the femur and tibia. As advantages, we highlight the small increase in surgical time, which is around 10 minutes. The technique does not require any specific instruments to perform it, as the drills and impactor are available in any arthroplasty system. In this technique, it is also unnecessary to use synthetic materials, used for grafts in blocks or orthopedic cement structures reinforced by screws. When compared to metal wedges, the technique we describe presents two major advantages: maintaining bone stock and reducing the final cost of surgery, since if the defect is filled using the technique we are describing, there is no need to add the cost of metal wedges or even tibial trays that support the use of wedges to the final cost of the surgery.
One limitation of this technique is that it is intended only for the filling of epiphyseal and some metaphyseal defects, and is not suitable for meta-diaphyseal or broad metaphyseal defects that must be addressed in other ways, including increasing the constraint of the implant to be placed and the need for stems use.
Conclusions
The technique we propose, despite not being able to treat all types of bone defects, is another option in the surgical arsenal, offering advantages over other techniques. It has proven to be very useful, reproducible, and safe in the situations for which it is intended, contributing to the treatment of bone defects in complex primary arthroplasties and knee revisions.
Conflict of Interest:
The authors declare that there are no conflicts of interest related to this article
Funding Statement:
None.
Acknowledgements:
None.
References
- Engh, G. A.; Parks, N. L. The management of bone loss in revision TKA: it’s a changing world. Orthopedics, 33-39, 2010.
- Pecora, J. R. et al.; Intersobserver correlation in classification of bone loss in total knee arthroplasty. Acta Ortopédica Brasileira, v. 19, 368-372, 2011.
- Lombardi Jr, Adolph V., Keith R. B., Joanne B. A. Management of bone loss in revision TKA: it’s a changing world. Orthopedics, 33-39, 2010.
- Kelbish, P.A.; Prosthetic fixation in cementless total knee arthroplasty. Influences of techniques, prosthetic design and bone graft enhancement. Biomecânica, 2, 46-50, 2011.