





Diagnostic Transience in Autism: A 10-Year Study in Brazil
Autistic Disorder (DSM-IV) by Gender/Sex and Brazilian Public Health System: A 10-Year Retrospective Study
Walter Camargos
OPEN ACCESS
PUBLISHED: 30 April 2026
CITATION: Camargos, W., 2026. Autistic Disorder (DSM-IV) by Gender/Sex and Brazilian Public Health System: A 10-Year Retrospective Study. Medical Research Archives, [online] 14(4).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
Abstract
Background: Diagnostic stability in Autistic Disorder (AD) remains a relevant and underexplored topic, particularly in public health systems of middle-income countries.
Objective: To investigate whether diagnostic transience of AD, according to DSM-IV criteria, is associated with origin of care within the public, Brazilian Public Health System versus private service (out of pocket, Non-SUS), and gender/sex.
Methods: Retrospective analysis of medical records from children evaluated between 2009 and 2020 at a tertiary public pediatric hospital and a private psychiatric office in Minas Gerais, Brazil. Inclusion required a DSM-IV diagnosis of AD for at least 36 months. Statistical analyses included Chi-square, Fisher s Exact, Mann Whitney, and Kaplan Meier survival estimates.
Results: Among 906 records analyzed, 186 were excluded, 68 had a transience diagnosis (average 9%): 1F:14M in the BPHS group versus 6F:47M in the non-BPHS group. No statistically significant association was found between diagnostic outcome and BPHS/non-BPHS origin or gender/sex (p > 0.05). Diagnostic transience was associated with a greater number of consultations (older age).
Discussion: Some results were consistent with the literature, such as the higher prevalence of male gender/sex (82.34%), the high frequency of environmental disorders and the median transience percentage (9%) by the 5-year-old median age. The new one is the lack of outcome differences between sex/gender and healthcare systems: BPHS, private, and international literature. The absence of difference in these outcomes is one of the most striking findings, as they differ substantially in access pathways, frequency and intensity of non-medical interventions, and professional specialization in ASD.
Conclusion: Diagnostic transience of AD occurred at similar rates regardless of healthcare origin or gender/sex. These findings raise questions about the importance of all biological markers that can complement clinical assessment and identify the most effective therapeutic methods for each individual affected by ASD. Further longitudinal and biologically integrated studies are necessary to clarify predictors of diagnostic stability and long-term outcomes.
Keywords
Autism, Autism Spectrum Disorder, sex/gender, outcome, diagnostic
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that affects social interaction, communication, and behavior. Its symptoms begin in early childhood and more frequently affect boys, with an average ratio of 4:1, following a chronic course. It is known that other medical conditions with developmental delays clinically mimic ASD, making accurate diagnosis difficult. Recent prevalence estimates indicate 1 in every 54 children aged 8 years or younger in the United States.
In everyday life, most professionals are still guided by concepts that are not scientifically grounded, such as the impossibility of diagnostic transience, that autism in women is less frequent and presents more severe clinical conditions, and that better outcomes depend on early diagnosis and treatment. The transience of diagnosis still appears to be a fact of little relevance, as evidenced by the limited dissemination and exploration of the topic itself, especially in countries such as Brazil, where there are no publications on the subject, nor on the relationship with gender/sex, nor related to the Brazilian Public Health System (BPHS), where the majority of the population is treated.
Proportionally to the thousands of publications on various topics, there are still very few on this subject in international journals, considering that the first was almost 60 years ago, when Rutter et al. reported that 9 out of 63 patients (14%) could no longer be classified under the term autistic at follow-up. The topic is not directly addressed in terms of its importance, a fact reflected in its absence in diagnostic manuals DSM s and ICD s.
The importance of widely disseminating the possibility of diagnostic transience goes beyond the mere transmission of information, reaching at least three dimensions: those of healthcare professionals, the family, and science. In the first group, it challenges the still deeply rooted notion that autism has an irreversibly negative outcome, thus changing this paradigm. For families, when it occurs, it resolves doubts about the initial autism diagnosis, both for families and for the physicians themselves a situation that still persists today. For science, it fosters a sense of progress in knowledge and motivates further investigation.
Studies reveal the transience diagnosis presence in themes such as diagnostic mobility, which is multidirectional: 1) migration from AD to PDD-NOS, from PDD-NOS to AD, or from any diagnosis to no diagnosis; 2) transience; 3) changes to non-ASD diagnoses, such as Other Developmental Disorders and Reading Disorders; and 6) possible outcome trajectories under DSM-IV. Most studies do not specify the difference between clinical outcomes of Autistic Disorder and Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS), the latter being more likely to represent a transient diagnosis. Earlier studies suggest that girls present with more severe clinical profiles and poorer outcomes, suggesting that such severity is secondary to Intellectual Disability (ID). There are also reports of a higher prevalence of epilepsy, which is positively associated with ID, regardless of an ASD diagnosis, and that they are more likely to present with de novo mutations, a known cause of ID.
Regarding sex/gender and outcomes, there is very little literature. In 2023, Harstad et al. reported that female sex/gender is predictive of a transient diagnosis, based on the Diagnostic and Statistical Manual of Mental Disorders 5th Edition (DSM-5), without specifying severity levels. Another recent study which specifically investigated the transience of an Autistic Disorder diagnosis clinically equivalent to Level 3 in DSM-5, did not find statistically significant differences between sexes/genders.
The clinical criteria for the diagnosis of Autistic Disorder (AD) 299.00 as defined in the Diagnostic and Statistical Manual of Mental Disorders 4th Edition (DSM-IV) are considered technically reliable and stable over time although not for children few 36 months of age reported cases of children who were diagnosed only at 36 months, with no identification in earlier assessments. The “gold standard” for diagnostic quality is the clinical judgment of experienced professionals and clinical diagnosis after 36 months of age shows the highest diagnostic stability for AD.
The Brazilian Public Health System (BPHS) is a nationally integrated public health system that provides free services universally to anyone within Brazilian territory, regardless of nationality, socioeconomic status, or other factors. Outside the SPSB, there are private health insurance plans and services paid directly out-of-pocket. There is a significant quantitative and qualitative gap in the care provided across these three service types.
Management of the BPHS is municipalized, and at the outpatient level, access to any specialty depends on authorization from a public clinical service located in the patient s residential region, designated as Primary Level. The Secondary Level includes all General Hospitals, while Specialized Hospitals constitute the Tertiary Level. In most Brazilian private health plans, clients can seek a specialist directly, without any authorization.
The primary objective of this study is to identify whether there is a correlation between transient clinical diagnosis of AD according to DSM-IV criteria and: a) sex/gender; b) origin from BPHS and non-BPHS. The secondary objective is to determine whether there is a difference in diagnostic outcome for Autistic Disorder based on age and/or number of visits between patients originating from BPHS and non-BPHS.
The significance of this publication lies in the fact that there are no prior studies examining the relationship between diagnostic transience in autism, sex/gender, and the SPSB, indicating that this topic is underexplored and underfunded.
It is important to clarify that in Brazil, there are diagnostic tests that are not authorized for clinical use by the Federal Council of Psychology, such as the Autism Diagnostic Observation Schedule (ADOS). The term sex/gender is used here to reflect the understanding that the effects of biological “sex” and socially constructed “gender” cannot be easily separated, and that the identity of most individuals is shaped by both sex and gender.
Methods
The study is retrospective, where the medical records of children treated at the Infant Development Ambulatory / Autism Spectrum Disorders of a tertiary public pediatric (Hospital Infantil João Paulo II, Fundação Hospitalar de Minas Gerais- FHEMIG), which participates in the Unified Health Brazilian System (BPHS), and at the author’s office, only by the private system (an unknown number of those treated by the private system were receiving non-medical treatments through health insurance), from November 2009 to June 2020 were analyzed. In both locations, only psychiatric medical attendance was provided, and the other proposed treatments were left to the families’ discretion; therefore, there was no control over them. Most patients originated from the capital of the state of Minas Gerais and surrounding cities, a smaller portion from cities throughout the state, and a very small portion from other states. Families/guardians scheduled appointments directly at the hospital, regardless of prior consultation, medical request, or medication use. There were also referrals from the hospital’s neurologists and pediatricians. At the time, scheduling was conducted directly at the hospital, meaning it was not yet under municipal service. Scheduling was only available up to 48 months of age. The patients at the private practice also basically had the same residential background.
The diagnosis of AD was clinical, utilizing the DSM-IV criteria both as an “entry” criterion (from 36 months of age) and as a transitioning criterion for the diagnosis. The M-Chat was used from 24 months of age as a triage for the diagnosis while waiting for the definitive diagnosis. When the diagnosis of AD was positive/BPHS suspicious, families were encouraged to return for clinical follow-up; when not, they were referred to another medical service. There was no active search for patients who failed to return for scheduled appointments, indicating no control over absenteeism.
The data were grouped according to the number of consultations, from the first to the maximum reached by each patient, up to 12 years. The exclusions, entries, and the transitioned cases of AD clinical diagnosis and the abandonment of the Ambulatory occurred at any of those periods.
Patients who presented with any other primary condition that, by itself, caused delays in child development of any kind were excluded, including Active Early-onset Epilepsies, Prematurity, Cerebral Palsy, Perinatal Injury, Genetic Diseases, Deafness, Bipolar Disorder, Down Syndrome, Blindness, Psychotic Disorders, and Profound Intellectual Deficiency. Patients with BPHS suspected non-AD clinical conditions who were referred to other specialists and did not return were also excluded from the “No diagnosis” classification.
Inclusion Criteria:
- Children with suspicions of an AD diagnosis in the first consultation up to 48 months of age;
- Children who were diagnosed with AD by DSM-IV criteria at 36 months of age by a senior child psychiatrist, qualified for the task;
Exclusion Criteria:
- Children with a history, or who received a base/primary diagnosis during the ongoing monitoring, with any disorders or syndromes that cause delays in development: children with a history of birth at less than 32 weeks of gestation, weighting less than 1.5 kg, Apgar below 4 at the 5th or 10th minute, morbid events that occurred up to the complete end of the seventh day of life, chromosomal abnormalities in general, genetic diseases, epilepsy difficult to control by the 2nd year of life, Cerebral Palsy, deafness, blindness, Profound Intellectual Disability, so on;
- Children who presented clinical conditions that did not have a precise diagnosis of another medical disorder that could cause delays in development / differential diagnosis of AD;
- Children who, during follow-up, had psychiatric diagnoses of Bipolar Disorder (BD) and Psychotic Disorder (PD).
Ethical Aspects:
The project was approved under CAAE register No. 49999521.1.0000.5119 (Certificate of Presentation for Ethical Consideration – CPEC), Review No.: 4,861,990 – FHEMIG / Brazil, and no Consent Form was required as it is a retrospective study.
Statistical Analysis
The Chi-Square and Fisher’s Exact tests were used. The Fisher s Exact test provides an alternative approach to the Chi-Square test when the conditions for its applicability are not met, such as in small samples, or when some cells in the contingency table have very low frequencies, to compare the occurrence of other delays in child development, not AD, between sexes.
To compare the exit of the diagnosis within the variables of interest, two approaches were used: the first consisted of using Chi-Square and Fisher’s Exact tests for categorical variables. For numerical variables, the Mann Whitney test was used to compare the distribution of values between groups. This non-parametric test is suitable for small samples or when the data distribution doesn t follow a normal distribution. For the study of the time until the occurrence of transient diagnosis, the Kaplan Meier estimator was used. The analyses were performed in R, version 4.3.1. The level of statistical significance considered was p < 0.05.
Results
Between November 1999 and June 2020, 906 medical records from the Development Outpatient Clinic were analyzed (Table 1): a) 82.33% were of the male gender/sex, b) 73.65% of the excluded patients were also of the male gender/sex, c) 29.47% were from the BPHS: 38.70% were excluded from the study and 39.24% had some medical condition unrelated to AD with the potential to cause developmental delay, d) eighteen children up to 12 months age at the first consultation, the youngest was 2 months and the oldest was at the 117 months at 20st consultation, e) the highest number of consultations was 21 at 109 months of age, f) 9.4% developed Transient Autism until the 21st appointment, g) 86.7% underwent diagnostic transition around the age of 5, h) statistical analyses included Chi-square, Fisher s Exact, Mann Whitney, and Kaplan Meier survival estimates.
| BPHS | Não BPHS | Total | Female | Male | ||
|---|---|---|---|---|---|---|
| 69 | 198 | 91 | 548 | 906 | ||
| Excluded | 29 | 41 | 20 | 96 | 186 | |
| Autistic Disorder* | 40 | 157 | 71 | 452 | 720 | |
| Permanent Autism | 38 | 144 | 64 | 404 | 652 | |
| Transient Autism | 2 | 13 | 6 | 47 | 68 | |
| Excluded | No diagnostic confirmed | 6 | 3 | 7 | 17 | 33 |
| No ASD** | 3 | 2 | 6 | 15 | 26 | |
| ASD no AD | 1 | 2 | 2 | 21 | 26 | |
| Active Early onset epilepsies | 4 | 8 | 1 | 7 | 20 | |
| Prematurity*** | – | 5 | 1 | 13 | 19 | |
| Cerebral Palsy | 4 | 9 | – | 5 | 18 | |
| Perinatal Injury | 3 | 4 | 1 | 9 | 17 | |
| Genic Disease | 6 | 5 | – | 1 | 12 | |
| Deafness, Bipolar Disorder | 2 | 2 | – | 3 | 7 | |
| Down S, Blindness, Psychotic Disorder, Profound Intellectual Deficiency | 1 | 3 | – | 4 | 8 |
*AD: Autistic Disorder (DSM-IV, 299.00); **ASD: Autism Spectrum Disorder; ***Prematurity: gestational age below 32 weeks
As shown in Table 2, there was no statistically significant difference (p-value > 0.050) in the percentage of patients with Permanent or Transient autism between gender/sex and BPHS/non-BPHS origin.
| Stability | Transient | p-value | Variable | N | % | N | % | ||
|---|---|---|---|---|---|---|---|---|---|
| Gender/Sex | Female | Male | 107 | 93.9 | 7 | 6.1 | 61 | 10.1 | 0.254 |
| BPHS | No | Yes | 469 | 89.8 | 53 | 10.2 | 15 | 7.6 | 0.361 |
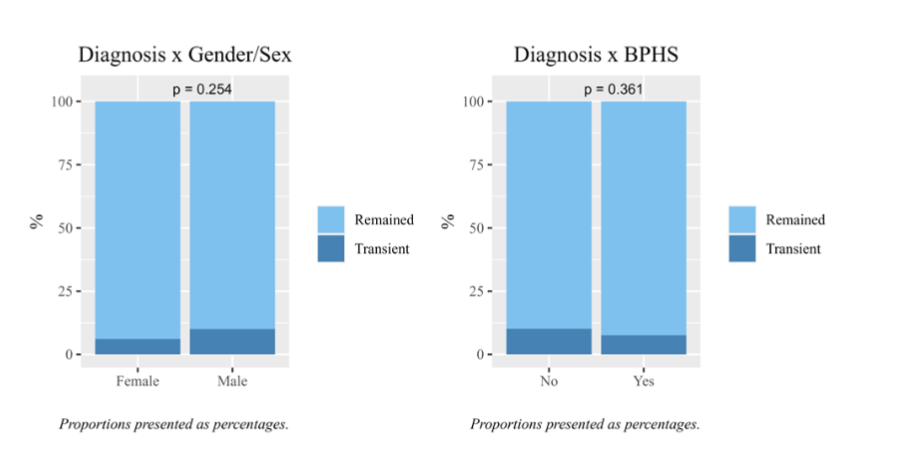
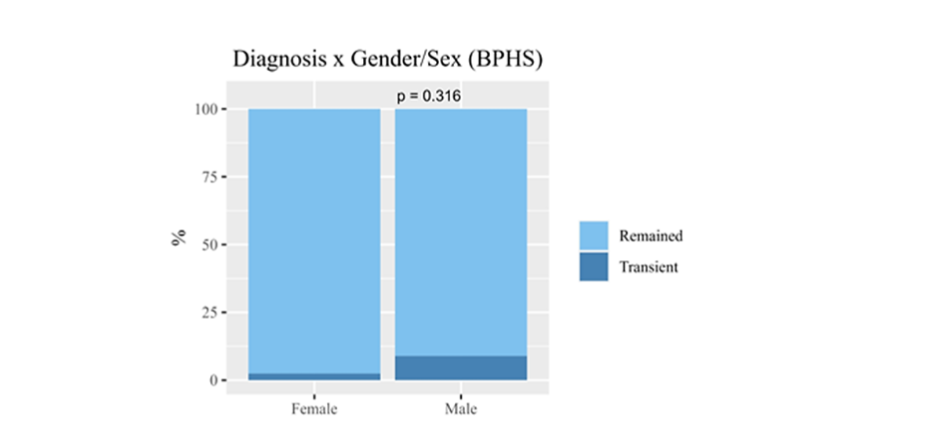
There was no statistically significant difference (p> 0.050) in the percentage of patients who experienced transient diagnosis in the BPHS group (Table 3).
| Stability | Transient | p-value | Variable | N | % | N | % | ||
|---|---|---|---|---|---|---|---|---|---|
| Gender/Sex | Female | Male | 40 | 97.6 | 1 | 2.4 | 14 | 8.9 | 0.316 |
| Variables | N | Média | D.P. | 1ºQ | 2ºQ | 3ºQ | Valor-p |
|---|---|---|---|---|---|---|---|
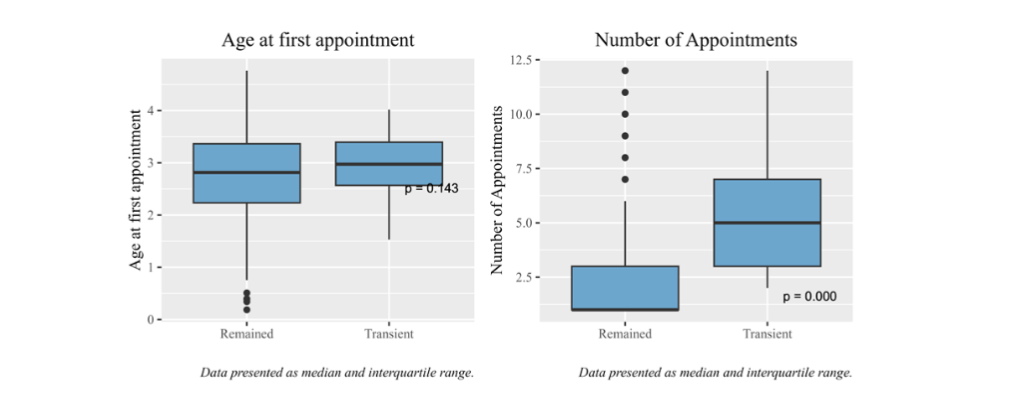
| Inicial age Stability | 652 | 2.78 | 0.74 | 2.23 | 2.82 | 3.37 | 0.143 |
| Appointments Stability | 652 | 2.63 | 2.51 | 1.00 | 1.00 | 3.00 | 0.000 |
Discussion
The possibility of clinical transience diagnosis may still be new information for many professionals, both medical and non-medical, as well as for families. This knowledge reduces the belief in the extreme malignancy of Autistic Disorder (AD), promotes greater optimism in the therapeutic approach for this population and their families, and strengthens engagement in physician patient/family relationships, resulting in both technical and humanistic improvement.
Some results were consistent with the literature, such as the higher prevalence of the male gender/sex (82.34%) in the sample, the high frequency of environmental disorders, including prematurity (10.22%), perinatal injury (9.14%), and cerebral palsy (9.68%) and the higher prevalence of AD, age three at the first consultation, Transient diagnosis was associated with the number of appointments, as shown in Table 4, related to older age, 59 out of 68 experienced transient diagnosis up to the 6th appointment, around 55 months of age, which aligns with Lord et al.: the classifications changed substantially more often from ages 2 to 5 years than from ages 5 to 9 years.
This study shows the absence of statistically significant difference in AD Transience or Permanence diagnosis by BPHS/non-BPHS origin or by gender/sex, using DSM-IV as the diagnostic criterion. In the BPHS group, the gender ratio was 1 female to 14 males, versus 6 females to 47 males in the non-BPHS group. The median age at the first appointment was slightly higher in the Transient group (3.35 years) than in the Permanent group (3.06 years), although the difference was not statistically significant. This may reflect a delay in seeking or accessing specialized services relative to the literature.
Although no statistically significant differences were found between BPHS/non-BPHS origin or gender/sex, the total frequency of diagnostic transience results is similar across Brazilian health systems, public health insurance, private medicine (median 8%), and international data (median 8.5%). These contexts have significantly different resources, which is intriguing: BPHS/Non-BPHS patients were mostly from the Metropolitan Region of Belo Horizonte, Minas Gerais, Brazil, and from the international literature. At the time, BPHS provided services were highly deficient, with limited and low ASD expertise, short-term non-medical treatment durations (sometimes 20-minute sessions), low frequency (sometimes monthly), and inconsistent follow-up. In contrast, non-BPHS patients were mostly treated by private professionals selected by families based on known technical competence, or through private health insurance, where provider choice was limited, and the technical quality was only slightly better than that of BPHS. Meanwhile, international studies typically involved specialized clinics offering the therapies recommended in the scientific literature, with a high standard of care. Given these undeniable differences in treatment quality and quantity, why were the outcomes so similar? This question opens a necessary space for discussion regarding genetics, neurophysiology, psychopathology, current nosology, and treatment approaches related to ASD.
There is also a need for new studies that further explore this subject and develop methodologies for long-term follow-up of transient diagnosis, similar to what was proposed by Margaret H. Sibley et al. for ADHD, a method not applied in the present study.
The strengths of this study include the long follow-up period, significant sample size, diagnosis performed by a senior child psychiatrist using a technically validated tool, as DSM-IV, and the fact that this is the first Brazilian study on the topic conducted within the public health system, where there is no literature on the topic of this article.
The limitations are: (1) diagnosis performed by only one professional, even though senior in the field; (2) lack of tools such as the ADOS, which the Brazilian Federal Council of Psychology authorizes only for research use; (3) lack of data on functional levels, such as expressive/comprehension language or intelligence; (4) absence of diagnosis in 18% of the excluded cases (33/186), classified as no confirmed diagnosis, which may have affected the accuracy of excluded case characterization; and (5) lack of active follow-up for all individuals in the database, limiting understanding of part of this population’s reality.
This is the first research on the Transience BPHS and Permanence of the Autistic Disorder diagnosis in patients from BPHS. A novel finding of this study is the statistical similarity in the Transience BPHS Permanence Autism Disorder diagnostic comparing BPHS and non-BPHS patients and across gender/sex. This opens a new window into a scientifically unexplored territory.
Conclusion
It is particularly noteworthy that similar results have emerged in patients who received treatments that differed both in quality and quantity, whether they were from the Brazilian Public Health System, the private sector, health insurance plans, or those described in international studies.
The results contradict some assumptions: a) women are not affected more severely; b) early diagnosis does not have a decisive impact; c) current treatments may not be as effective as advertised; d) genetic anomalies may have a decisive influence; and e) we need to learn to combine all this information to offer patients truly personalized treatment. From an outcome perspective, current knowledge in psychiatry, psychopathology, and nosology is insufficient, requiring better differentiation between genetic, immunological, and gestational/postpartum etiologies, and something similar applies to treatments in general. Further studies are necessary to clarify the above-mentioned issues.
Conflicts of Interest:
None
Acknowledgements:
I would like to thank Dr. Luciano Amedée Péret Filho for his kindness in reviewing the text.
Abbreviations:
- Autism Spectrum Disorder: ASD
- Autistic Disorder: AD
- Diagnostic and Statistical Manual of Mental Disorders: DSM
- Pervasive Developmental Disorder Not Otherwise Specified: PDD-NOS
- Intellectual Disability: ID
- Bipolar Disorder: BD
- Psychotic Disorder: PD
References:
- Christensen DL, Baio J, Van Naarden Braun K et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years–Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. MMWR Surveill Summ. 2016 Apr 1;65(3):1-23. doi: 10.15585/mmwr.ss6503a1. Erratum in: MMWR Morb Mortal Wkly Rep. 2016 Apr 22;65(15):404. doi: 10.15585/mmwr.mm6515a7. Erratum in: MMWR Morb Mortal Wkly Rep. 2018 Nov 16;67(45):1279. doi: 10.15585/mmwr.mm6745a7. PMID: 27031587; PMCID: PMC7909709.
- Rutter M, Greenfeld D, Lockyer L. A five to fifteen year follow-up study of infantile psychosis: II. Social and behavioural outcome. The British Journal of Psychiatry. 1967 Nov;113(504):1183-99.
- Kleinman JM, Ventola PE, Pandey J, Verbalis AD et al. Diagnostic stability in very young children with autism spectrum disorders. Journal of autism and developmental disorders. 2008 Apr;38(4):606-15. doi: 10.1007/s10803-007-0427-8. Epub 2007 Oct 9.
- Sutera S, Pandey J, Esser EL et al. Predictors of optimal outcome in toddlers diagnosed with autism spectrum disorders. Journal of autism and developmental disorders. 2007 Jan;37(1):98-107. doi: 10.1007/s10803-006-0340-6. Epub 2007 Jan 6.
- Rondeau E, Klein LS, Masse A, Bodeau N, Cohen D, Guilé JM. Is pervasive developmental disorder not otherwise specified less stable than autistic disorder? A meta-analysis. Journal of Autism and Developmental Disorders. 2011 Sep;41(9):1267-76. doi: 10.1007/s10803-010-1155-z.
- Howlin P, Goode S, Hutton J, Rutter M. Adult outcome for children with autism. Journal of child psychology and psychiatry. 2004 Feb;45(2):212-29. doi: 10.1111/j.1469-7610.2004.00215.x.
- Lai MC, Lombardo MV, Ruigrok AN et al. Cognition in males and females with autism: similarities and differences. PLoS One. 2012;7(10):e47198. doi: 10.1371/journal.pone.0047198. Epub 2012 Oct 17. PMID: 23094036; PMCID: PMC3474800.
- Ozonoff S, Young GS, Landa RJ et al. Diagnostic stability in young children at risk for autism spectrum disorder: a baby siblings research consortium study. Journal of Child Psychology and Psychiatry. 2015 Sep;56(9):988-98. doi: 10.1111/jcpp.12421. Epub 2015 Apr 29.
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).
- Lord C, Risi S, DiLavore PS, Shulman C, Thurm A, Pickles A. Autism from 2 to 9 years of age. Archives of general psychiatry. 2006 Jun;63(6):694-701. doi: 10.1001/archpsyc.63.6.694. PMID: 16754843.
- Piven J, Harper J, Palmer PA, Arndt S. Course of behavioral change in autism: A retrospective study of high-IQ adolescents and adults. Journal of the American Academy of Child & Adolescent Psychiatry. 1996 Apr 1;35(4):523-9. doi: 10.1097/00004583-199604000-00019.
- Cox A, Klein K, Charman T, Baird G et al. Autism spectrum disorders at 20 and 42 months of age: Stability of clinical and ADI‐R diagnosis. Journal of Child Psychology and Psychiatry. 1999 Jul;40(5):719-32. PMID: 10433406.
- Stone WL, Lee EB, Ashford L et al. Can autism be diagnosed accurately in children under 3 years?. The Journal of Child Psychology and Psychiatry and Allied Disciplines. 1999 Feb;40(2):219-26. PMID: 10188704.
- Eaves LC, Ho HH. The very early identification of autism: Outcome to age 41/2 5. Journal of autism and developmental disorders. 2004 Aug;34(4):367-78. doi: 10.1023/b:jadd.0000037414.33270.a8.
- Sutera S, Pandey J, Esser EL et al. Predictors of optimal outcome in toddlers diagnosed with autism spectrum disorders. Journal of autism and developmental disorders. 2007 Jan;37(1):98-107. doi: 10.1007/s10803-006-0340-6. Epub 2007 Jan 6.
- Rondeau E, Klein LS, Masse A, Bodeau N, Cohen D, Guilé JM. Is pervasive developmental disorder not otherwise specified less stable than autistic disorder? A meta-analysis. Journal of Autism and Developmental Disorders. 2011 Sep;41(9):1267-76. doi: 10.1007/s10803-010-1155-z.
- Banach R, Thompson A, Szatmari P et al. Brief report: Relationship between non-verbal IQ and gender in autism. Journal of autism and developmental disorders. 2009 Jan;39(1):188-93. doi: 10.1007/s10803-008-0612-4. Epub 2008 Jul 2.
- Amiet C, Gourfinkel-An I, Bouzamondo A et al. Epilepsy in autism is associated with intellectual disability and gender: evidence from a meta-analysis. Biological psychiatry. 2008 Oct 1;64(7):577-82. doi: 10.1016/j.biopsych.2008.04.030.
- Lukmanji S, Manji SA, Kadhim S et al. The co-occurrence of epilepsy and autism: A systematic review. Epilepsy & Behavior. 2019 Sep 1;98:238-48. doi: 10.1016/j.yebeh.2019.07.037. Epub 2019 Aug 6.
- Sebat J, Lakshmi B, Malhotra D et al. Strong association of de novo copy number mutations with autism. Science. 2007 Apr 20;316(5823):445-9. doi: 10.1126/science.1138659. Epub 2007 Mar 15.
- Hamdan FF, Gauthier J, Araki Y et al. Excess of de novo deleterious mutations in genes associated with glutamatergic systems in nonsyndromic intellectual disability. The American Journal of Human Genetics. 2011 Mar 11;88(3):306-16. doi: 10.1016/j.ajhg.2011.02.001. Epub 2011 Mar 3.
- Harstad E, Hanson E, Brewster SJ et al. Persistence of autism spectrum disorder from early childhood through school age. JAMA pediatrics. 2023 Nov 1;177(11):1197-205. doi: 10.1001/jamapediatrics.2023.4003.
- Camargos Jr, W. The outcome of clinical diagnoses for Autistic Disorder by Sex/Gender: A 10-year retrospective study. Ciências da Saúde, 2025 Mar 29(144)
- Kočovská E, Billstedt E, Ellefsen A et al. Autism in the Faroe Islands: diagnostic stability from childhood to early adult life. ScientificWorldJournal. 2013;2013:592371. doi: 10.1155/2013/592371. Epub 2013 Feb 17. PMID: 23476144; PMCID: PMC3586480.
- Volkmar F, Chawarska K, Klin A. Autism in infancy and early childhood. Annu. Rev. Psychol.. 2005 Feb 4;56(1):315-36. doi: 10.1146/annurev.psych.56.091103.070159.
- Westman Andersson G, Miniscalco C, Gillberg C. Autism in preschoolers: does individual clinician s first visit diagnosis agree with final comprehensive diagnosis?. The Scientific World Journal. 2013;2013(1):716267. doi: 10.1155/2013/716267. eCollection 2013.
- Zwaigenbaum L, Bryson SE, Brian J et al. Stability of diagnostic assessment for autism spectrum disorder between 18 and 36 months in a high‐risk cohort. Autism Research. 2016 Jul;9(7):790-800. doi: 10.1002/aur.1585. Epub 2015 Nov 27.
- Losapio MC, Pondé MP. Tradução para o português da escala M-CHAT para rastreamento de autismo. J. Ped. 2008 84(3):250-255.
- Hollander, M., Wolfe, D. A., & Chicken, E. Nonparametric statistical methods. John Wiley & Sons, 2013.
- Kaplan, E. L.; Meier, P. Nonparametric estimation from incomplete observations. Journal of the American statistical association, v. 53, n. 282, p. 457-481, 1958.
- Klein, J.P., & Moeschberger, M.L. (2003). Survival Analysis: Techniques for Censored and Truncated Data. Springer.
- R Core Team (2023). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
- De Giacomo A, Fombonne E. Parental recognition of developmental abnormalities in autism. European child & adolescent psychiatry. 1998 Oct;7(3):131-6. doi: 10.1007/s007870050058.
- Klin A, Lang J, Cicchetti DV, Volkmar FR. Brief report: Interrater reliability of clinical diagnosis and DSM-IV criteria for autistic disorder: results of the DSMIV autism field trial. J Autism Dev Disord.2000 Apr;30(2):163-7. doi: 10.1023/a:1005415823867. PMID: 10832781.
- Turner LM, Stone WL. Variability in outcome for children with na ASD diagnosis at age 2. J Child Psychol Psychiatry. 2007 Aug;48(8):793-802. doi: 10.1111/j.1469-7610.2007.01744.x. PMID: 17683451.
- Itzchak EB, Zachor DA. Change in autism classification with early intervention: Predictors and outcomes. Research in Autism Spectrum Disorders. 2009 Oct 1;3(4):967-76.
- Starr, E.M., Popovic, S. & McCall, B.P. Supporting Children with Autism Spectrum Disorder at Primary School: Are the Promises of Early Intervention Maintained?. Curr Dev Disord Rep. 2016; 3:46 56. https://doi.org/10.1007/s40474-016-0069-7
- Sibley MH, Arnold LE, Swanson JM et al. Variable patterns of remission from ADHD in the multimodal treatment study of ADHD. American Journal of Psychiatry. 2022 Feb;179(2):142-51. doi: 10.1176/appi.ajp.2021.21010032. Epub 2021 Aug 13.