





Laparoscopic HIPEC for Gastrointestinal Malignancy Treatment
Laparoscopic Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Gastrointestinal Malignancy: A Case Series and Review of the Literature
¹Teresa Moreno Djadou, MD, PhD, ¹Keat Seong Poh, MD, ¹Amandeep Ghuman, MD, MPH, FRCSC, ¹Shlomo Yellinek, MD, ¹Giovanna DaSilva, MD, ²Steven D. Wexner MD, PhD (Hon), ¹Conrad H. Simpfendorfer, MD
- Cleveland Clinic Florida, Department of Colorectal Surgery
- MedStar Georgetown University Hospital, Department of Colorectal Surgery, 3800 Reservoir Road NW, Washington, DC 20007
OPEN ACCESS
PUBLISHED: 30 April 2026
CITATION: Moreno-Djadou, T., Poh, KS., et al., 2026. Laparoscopic Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Gastrointestinal Malignancy: A Case Series and Review of the Literature. Medical Research Archives, [online] 14(4).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
Abstract
Background: We aimed to evaluate laparoscopic cytoreductive surgery/hyperthermic intraperitoneal chemotherapy for patients with gastrointestinal malignancy and peritoneal carcinomatosis.
Methods: This is a single surgeon case series of laparoscopic hyperthermic intraperitoneal chemotherapy procedures from 2013-2018. Inclusion criteria were diagnosis of gastrointestinal malignancy with peritoneal carcinomatosis or high risk of developing peritoneal carcinomatosis after primary tumor resection. Outcomes analyzed included completeness of cytoreduction, postoperative complications, and mortality.
Results: Three patients with gastrointestinal malignancy underwent laparoscopic hyperthermic intraperitoneal chemotherapy [2 males, 1 female; median age: 43 (20-50) years]. Mean body mass index was 21.7 ± 1.3 kg/m² and none had major comorbidities; one patient received preoperative chemotherapy. Two patients had mucinous appendiceal cystoadenocarcinoma and one had cecal adenocarcinoma. Two patients underwent right hemicolectomy with ileocolic anastomosis and one underwent total colectomy with ileorectal anastomosis. All patients had intraperitoneal peritoneal cancer index scores <10 with completeness of cytoreduction (CC = 0 or 1). Mitomycin C was the chemotherapy agent used in all procedures. Median operative time was 7.5 (6.1-9.9) hours. There were no major intra/postoperative complications. Median length of stay was 4 (3-5) days. Mean overall survival was 31 (6-66) months with no mortality. One recurrence was detected at median follow-up of 19 (6-50) months.
Conclusions: Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy is associated with significant morbidity and mortality; laparoscopic cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for gastrointestinal malignancy may be feasible and safe in highly selected patients.
Keywords: Laparoscopy · Peritoneal carcinomatosis · Cytoreductive surgery · Hyperthermic intraperitoneal chemotherapy
Introduction
Peritoneal carcinomatosis (PC) represents the involvement of the peritoneal surface with neoplastic processes. Although the natural history of this disease is not well documented as Elias et al. and other authors determined, the overall prognosis is believed to be extremely poor with a median survival of 6 months. Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) has been utilized successfully for the treatment of this challenging condition. Its role has developed as a locoregional treatment option for primary or secondary peritoneal carcinomatosis of select tumors, such as mesothelial, gynecological, and gastrointestinal origin.
Twenty years ago, PC was considered as advanced metastatic spread and the only treatment options available for patients were systemic chemotherapy and supportive care, as surgery was reserved only for palliation. However, during the past two decades there has been a tremendous interest and increase in the utilization of CRS/HIPEC. This treatment option for patients with terminal stage gastrointestinal malignancy results in an unprecedented median survival of >20 months. Even if this treatment can be considered effective in terms of survival, it is associated with high morbidity and mortality. Therefore, the use of laparoscopy in both therapeutic and diagnostic roles to perform hyperthermic intraperitoneal chemotherapy, may be a valuable option because it may permit reduction of surgical trauma and faster recovery.
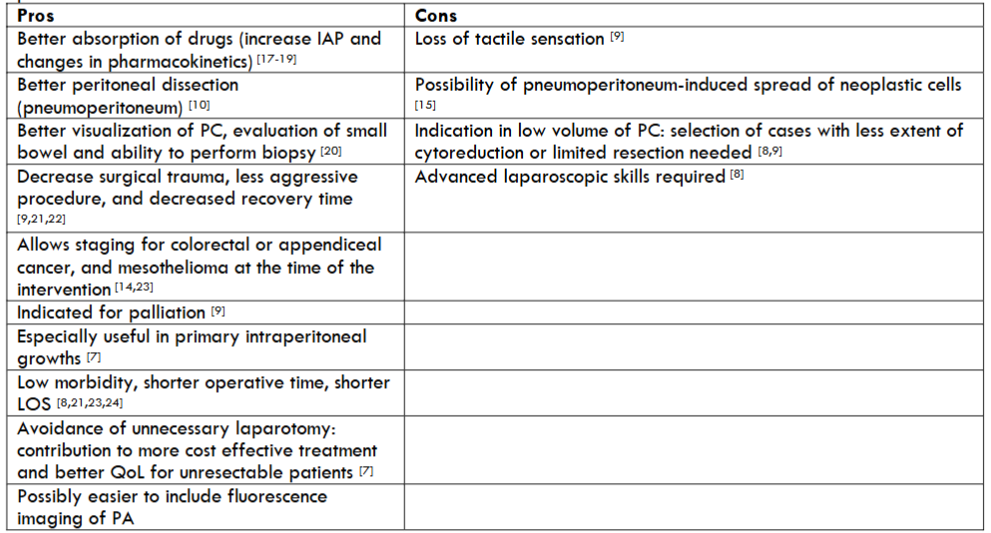
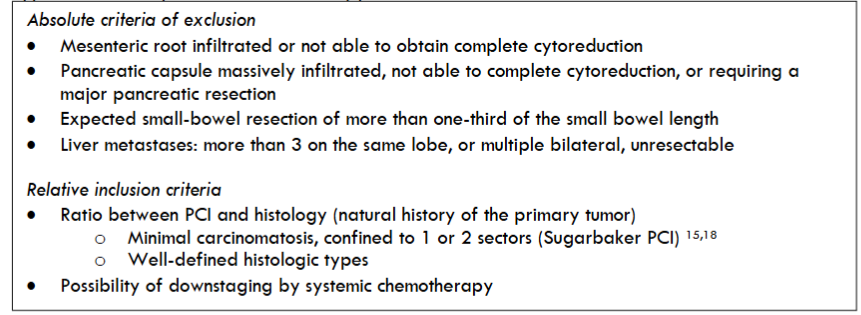
Table 1 shows the advantages and disadvantages of laparoscopic cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Experimental data in pigs established that the presence of pneumoperitoneum makes the identification of the peritoneal layer easier, thus facilitating dissection through the correct anatomical planes. Nonetheless, the loss of tactile sensation, which is fundamental to cytoreductive surgery, and the possibility of spreading neoplastic cells due to pneumoperitoneum, could be a limitation. Experimental data in rats has demonstrated that a higher intra-abdominal pressure (IAP) caused higher systemic absorption and drug penetration in normal and tumoral tissues. Laparoscopic CRS/HIPEC is technically feasible with an acceptable morbidity profile, especially in patients with low tumor load. Hence, the selection of cases for this procedure is very important in order to achieve the best outcomes and minimize morbidity (Table 2). This surgical technique has been proposed most notably with neoadjuvant, adjuvant, and palliative aims. However, for a neoadjuvant or adjuvant aim, it cannot be routinely recommended for wide application because of the lack of efficacy data. The most intriguing application of laparoscopic CRS/HIPEC, with its proven technical feasibility in humans, could be in the adjuvant treatment of tumors at high risk of local or peritoneal recurrence. Furthermore, the palliation of malignant ascites (MA) seems to be the best indication for laparoscopic HIPEC, as the main benefit is derived from optimizing post-procedural quality of life. This palliative therapy indication is an interesting option given its potential low morbidity.
Laparoscopic CRS/HIPEC appears to be a safe and technically effective procedure, which is becoming more popular. The efficacy should be evaluated in relationship to the indication and outcomes. Moreover, its role in combination with adjuvant or neoadjuvant treatment aims has not been well defined. Laparoscopy can logically have an inherent benefit in visualization of peritoneal disease including evaluation of small bowel and ability to perform biopsy. In patients with disease limited to one part of the peritoneal cavity CRS can be accomplished laparoscopically. Among them, in a select subgroup of patients, HIPEC can also be successfully administered by laparoscopic approach and has been found to be safe biopsy. The purpose of this study was to determine the indications and outcomes of laparoscopic cytoreductive surgery with hyperthermic intraperitoneal chemotherapy in patients with the diagnosis of gastrointestinal malignancy and peritoneal carcinomatosis in a single institution.
Patients and methods
PATIENTS
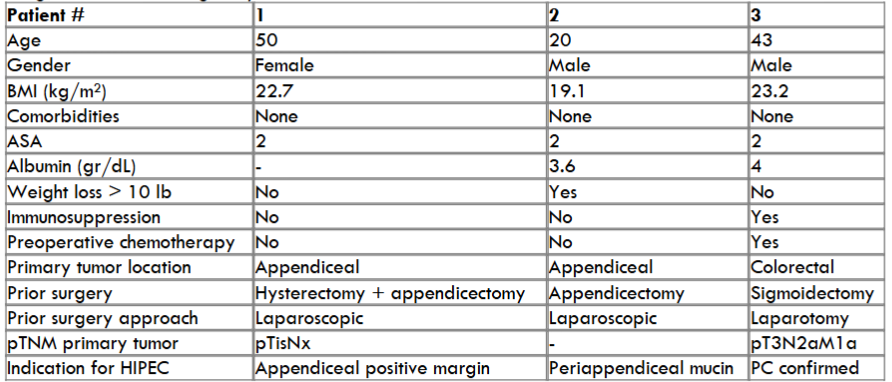
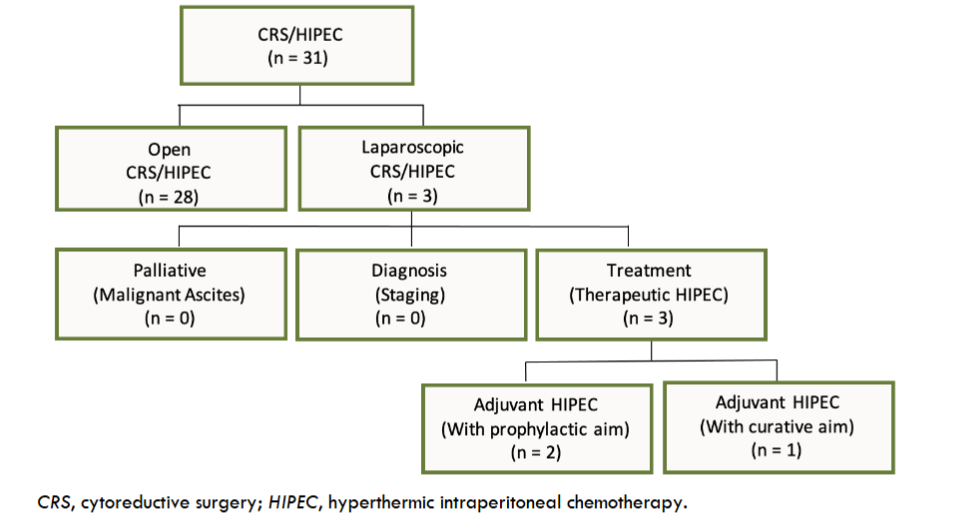
From January 2013 to January 2018, 31 patients with gastrointestinal cancer underwent CRS/HIPEC with curative or palliative intent. Three patients had laparoscopic approach and were included in the study. Indications for the procedure are as follows. One patient had a previous laparoscopic total abdominal hysterectomy and salpingo-oophorectomy for complicated endometriosis with the appendix adherent to the right ovary. The resected specimen revealed a positive appendiceal margin and presence of extra-appendiceal mucin without neoplastic cells. The second patient had a previous laparoscopic appendicectomy for ruptured appendicitis in which the pathology returned as a ruptured appendiceal mucinous cystadenocarcinoma with high risk of developing peritoneal carcinomatosis. The third patient had a known diagnosis of metachronous cecal tumor with confirmed peritoneal carcinomatosis after a previous open resection for sigmoid carcinoma. This was the only patient who had undergone preoperative chemotherapy prior to laparoscopic HIPEC. Suitability of patients for laparoscopic hyperthermic intraperitoneal chemotherapy was determined by a multidisciplinary team including surgeons, oncologists, pathologists and radiologists based upon overall clinical evaluation and cytology, computed tomography. The computed tomography scan of the first patient revealed a well-defined ring shaped calcified appendiceal mass and small amount of ascites around the liver. The computed tomography scan of the third patient who had previously undergone a Hartmann’s procedure with sigmoid resection and end colostomy showed mild wall thickening involving the cecum. The laparoscopic approach was proposed in an attempt to diminish the invasiveness of the procedure in these patients. All patients were informed about the curative vs. palliative role of the procedure. Indications, risks, possible complications and expected benefits were discussed with each one. An informed consent was obtained for all patients. The primary outcomes of analysis were the completeness of cytoreduction (CC), type of postoperative complications, and mortality rate. Management of the surgical technique and outcomes for laparoscopic HIPEC were also described.
PROCEDURE
Patients were carefully positioned in the supine modified lithotomy position in Allen stirrups. Cystoscopy with insertion of bilateral ureteric catheters was performed by the Urology Service. An infra or supraumbilical vertical incision was made through which a 10 mm Hasson cannula was carefully placed. Carbon dioxide pneumoperitoneum of 15 mmHg was achieved after which a 30-degree telescope was introduced. Two additional 10 mm ports were carefully placed through horizontal stab wounds under direct vision; one in the left upper quadrant, another in the left lower quadrant for both right hemicolectomies. For the patient with cecal metachronous who underwent a total colectomy and resection of isolated hepatic metastases, an additional 5-mm trocar was placed in the right upper quadrant. The periumbilical incisions were lengthened to 3 cm through which an Alexis® wound protector (Applied Medical Resources, Rancho Mirage, CA, USA) was placed. The colonic specimen was then extra corporealized and resected by a colorectal surgeon. A second specialized surgeon performed the CRS/HIPEC portions of the operation. The peritoneum was stripped laparoscopically and sent to the Pathology Service, when peritoneal disease was present (n=1). A SutureLasso™ passer (Arthrex Inc, Naples, FL) was laparoscopically introduced and brought out through the 10 mm trocar site at the left side of the abdomen. An inflow cannula was placed at the umbilical port site. The cannulas were placed with the inflow to the upper abdomen and the outflow SutureLasso™ cannula in the pelvis. The hyperthermic intraperitoneal chemotherapy was performed with 40 mg of mitomycin C (MMC) for 60-90 minutes at 42-43 degrees Celsius. At the completion of the HIPEC, irrigation of the abdominal cavity was performed through a closed circuit with 2 L of saline. The intraabdominal fluid was then suctioned and the inflow and outflow cannulas were removed. The trocars were re-introduced and further intraabdominal fluid was suctioned, after which the colorectal team performed the anastomoses (two ileocolic and one ileorectal with a diverting loop ileostomy).
Results
Patient characteristics and results are summarized in Table 3. As shown in Figure 1, the intent of the laparoscopic cytoreductive surgery with hyperthermic intraperitoneal chemotherapy surgery was for prophylaxis in 2 patients, given high risk features at time of index operation (positive margin and tumor spillage) and curative in 1 patient. Prior surgical interventions in this cohort included 1 laparotomy with curative intent and 2 diagnostic laparoscopies.
The extent of the disease was evaluated and documented at the beginning of the operation when the laparoscope was introduced. In the first patient, small bowel mucin in the right pelvic sidewall along with scarring from the previous operation was noted; the remainder of the abdomen demonstrated no evidence of mucinous deposits or carcinomatosis. The second patient, who had acute appendicitis reported as a ruptured appendiceal with peri-appendiceal acellular mucin, did not have any evidence of peritoneal carcinomatosis at the time of the laparoscopic HIPEC. The third patient had a cecal tumor and a solitary posterior right lobe liver metastasis. Two patients underwent a right hemicolectomy with ileocolic anastomosis and one had a total colectomy, ileorectal anastomosis with a diverting loop ileostomy and partial hepatectomy, along with excision and stripping of the pelvic peritoneum due to peritoneal carcinomatosis. Table 4 shows the primary outcome of complete cytoreduction (CC = 0 or CC = 1) and intraoperative peritoneal cancer index (PCI) score of minimal carcinomatosis, which was PCI < 10 for the entire cohort. The median operative time (OT) was 7.5 (range, 6.1-9.9) hours and the estimated blood loss was 150 (range 100-200) mL. There were no major intraoperative or postoperative complications, no transfusions were required, and there were no hospital readmissions, or procedure related mortality. The median length of hospital stay was 4 (range 3-5) days. The overall median survival was 31 (range 6-66) months and one recurrence was detected during a median follow-up time of 19 (range 6-50) months.
Discussion
Hyperthermic intraperitoneal chemotherapy, particularly if associated with extended colorectal surgery is an extensive procedure that can be associated with significant morbidity and mortality. Laparoscopy offers an effective method especially in the cases of primary intraperitoneal growth, which can occur with ascites, diffuse peritoneal nodules, and the involvement of the greater omentum. However, the selection of patients with peritoneal carcinomatosis who could benefit from laparoscopic CRS/HIPEC remains poorly defined. This procedure should be performed at an experienced center, as part of a multimodality treatment involving the optimal chemotherapy regimen after a multidisciplinary discussion of each individual case. At our single academic institution, a highly selected group of 3 patients out of 31 patients who underwent CRS/HIPEC for gastrointestinal malignancy were performed by a laparoscopic approach. The main indications for this laparoscopic procedure have been previously reported for neoadjuvant, adjuvant, or palliative indent. In our case series the principal indication was in the adjuvant setting. Despite reports of high rates of morbidity and mortality, none of these problems were noted in this small pilot series. The 3 patients in our series were offered laparoscopic CRS/HIPEC for concern of local and peritoneal recurrence based on the highly suspicious clinical/pathological finding after their index surgery. Consequently, this surgical technique in 2 of our patients was performed as a prophylactic measure, which has previously been reported as an indication. Another study on systematic open second-look surgery with HIPEC was performed in a group of colorectal cancer patients at high risk of peritoneal recurrence or minimal peritoneal carcinomatosis resected with the primary rupture of the tumor and ovarian metastasis. This management protocol of high-risk patients for peritoneal carcinomatosis revealed recurrent carcinomatosis in 56% of patients in their study with a mean peritoneal cancer index ranging between 5 and 9, which established that this patient population may represent an ideal group for laparoscopic approach.
In our series, the most frequent primary tumor location was appendiceal and peritoneal cancinomatosis was found in one patient at the time of laparoscopic access for CRS/HIPEC. The primary malignancies were considered completely resectable preoperatively, as this was one of the main inclusion criteria for successful laparoscopic surgery and hyperthermic intraperitoneal chemotherapy. In our cohort the laparoscopic HIPEC procedures were performed concomitantly with colorectal surgery, whereas in other published studies, they were performed several weeks after extended open colorectal surgery. In two patients we used three 10 mm trocars and in one patient we used one additional 5 mm trocar; in other studies, laparoscopic CRS/HIPEC required up to 6 trocars. No conversions to laparotomy were necessary in our cohort. One patient had the ileocolic anastomosis performed after the right hemicolectomy and cytoreductive surgery, but prior to hyperthermic intraperitoneal chemotherapy, even though traditionally the surgical reconstruction of the gastrointestinal tract is carried out after completion of HIPEC. This practice of delayed anastomosis until after completion of HIPEC is considered safer and believed to reduce the risk of anastomotic leak. However, one study has reported the anastomotic leakage rate of 13% when anastomoses were performed before HIPEC, and leak rates are similar to those reported rates elsewhere (18% ± 4%). Patients with extensive involvement of small bowel loops that will not allow an adequate cytoreduction are considered unresectable and thus are not candidates for curative CRS/HIPEC. In our series, none of the patients had evidence of small intestine involvement or occlusion, which would have required a small bowel resection. The preoperative peritoneal cancer index scores in our cohort were appropriately staged by preoperative computed tomography, even though of them have been shown to have low peritoneal cancer index predictive accuracy and low sensitivity in assessing small-bowel lesions, especially lesions smaller than 5 mm. The extent of carcinomatosis recorded by the intra-operative PCI in all our patients were less than 10. This classification proved to be appropriate to determine the potential for complete resection in our cohort, bearing in mind that the extent of tumor involving the small intestine has been previously shown to be more relevant than the actual calculated peritoneal cancer index. Thus, laparoscopic peritonectomy may have a role in minimal carcinomatosis, with PCI confined to 1 or 2 sectors of Sugarbaker peritoneal cancer index scoring and well-defined histologic types, such as carcinomas of appendix. Completeness of cytoreduction (CC = 0 or CC = 1) was achieved in the entire cohort. Completeness of cytoreduction is the most important perioperative factor as it has been shown to be a significant independent predictor of survival.
Few studies have investigated the value of laparoscopy to assess tumor resectability prior to performing synchronous cytoreductive surgery with hyperthermic intraperitoneal chemotherapy, but common findings in these few reported cases have included low morbidity, short operative time and quick postoperative recovery. However, upon further evaluation of these case series, mean operative time ranged from 180 to 360 minutes but it was unclear if operative times were for diagnostic or adjuvant laparoscopic surgery with hyperthermic intraperitoneal chemotherapy for specific gastrointestinal cancers. This surgery and concomitant HIPEC was characterized as having shorter operative time, less extensive cytoreduction requirement, and less peritonectomies as compared to an open procedure. Several feasibility studies on laparoscopic CRS/HIPEC have reported no procedure related deaths and only minor complications. The major determining factors of morbidity and mortality in this procedure are the extent of cytoreduction, the number of intestinal anastomoses, extent of peritonectomy, and operative time. In our series, there were no major intraoperative or postoperative complications. The median length of hospital stay (LOS) was 4 days and was favorable compared to the reported median LOS of 9 days after open access of CRS/HIPEC. Esquivel et al. described a case series of 10 laparoscopic procedures of cytoreduction followed by HIPEC for limited and resectable carcinomatosis. They reported a shorter LOS but had higher morbidity compared to an open procedure. Other studies since, such as the one by Valle et al., have instead demonstrated lower morbidity with a laparoscopic approach. Port site metastasis is another concern with laparoscopic HIPEC for patients with peritoneal carcinomatosis, which is a rare occurrence and has an estimated likelihood of 1.1% to 3.9%. It has been demonstrated that a careful laparoscopic procedure can minimize the formation of trocar port site tumor seeding. Our findings are in agreement with this as no neoplastic seeding was detected at the trocar sites in any of our patients. Long-term survival is perhaps one of the most important outcomes to evaluate following CRS/HIPEC. In this series, overall median survival was 31 months. The longest survival time of 66 months was detected in the youngest patient who had a mucinous appendiceal cystadenocarcinoma, whereas the shortest survival time of 6 months was in the oldest patient with a mucinous adenocarcinoma. Regular assessment by clinical examination, carcinoembryonic antigen (CEA) and Positron Emission Tomography/Computed Tomography (PET/CT) imaging, was performed in our cohort and the median follow-up was 19 months during which time no recurrences were detected. Limitations of this study include its small cohort size, single institution and single surgeon experience. Although we were able to capture numerous patients, intraoperative, and postoperative variables, we are limited by our retrospective nature.
Conclusion
The use of laparoscopy to perform cytoreductive surgery with hyperthermic intraperitoneal chemotherapy has been previously shown to be feasible, safe, and effective. In our case series, we have demonstrated laparoscopic procedure may be performed in well selected patients as a reliable and safe method, resulting in reduced surgical burden and quicker recovery time. However, more data are required to validate this minimally invasive approach to hyperthermic intraperitoneal chemotherapy.
Conflict of interest: None
Funding: None
References
- Rosen SA, Buell JF, Yoshida A. Initial Presentation With Stage IV Colorectal Cancer: How Aggressive Should We Be? Arch Surg 2000;135:530-4; discussion 534-5.
- Shaligram A. Management of peritoneal surface malignancies in laparoscopic era: a concise review. Int J Surg Oncol (NY) 2016;1:e05.
- Maggiori L, Elias D. Curative treatment of colorectal peritoneal carcinomatosis: current status and future trends. Eur J Surg Oncol 2010;36:599‐603.
- Teo M, Foo KF, Koo WH, Wong LT, Soo KC. Lessons learned from initial experience with peritonectomy and intra-peritoneal chemotherapy infusion. World J Surg 2006;30:2132‐2135.
- Li Y, Zhou YF, Liang H, et al. Chinese expert consensus on cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal malignancies. World J Gastroenterol 2016;22:6906‐6916.
- Verwaal VJ, van Ruth S, Witkamp A, Boot H, van Slooten G, Zoetmulder FA. Long-term survival of peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol 2005;12:65‐71.
- Sommariva A, Zagonel V, Rossi CR. The role of laparoscopy in peritoneal surface malignancies selected for hyperthermic intraperitoneal chemotherapy (HIPEC). Ann Surg Oncol 2012;19:3737‐3744.
- Esquivel J, Averbach A, Chua TC. Laparoscopic cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in patients with limited peritoneal surface malignancies: feasibility, morbidity and outcome in an early experience. Ann Surg 2011;253:764‐768.
- Facchiano E, Risio D, Kianmanesh R, Msika S. Laparoscopic hyperthermic intraperitoneal chemotherapy: indications, aims, and results: a systematic review of the literature. Ann Surg Oncol 2012;19:2946‐2950.
- Ferron G, Gesson-Paute A, Classe JM, Querleu D. Feasibility of laparoscopic peritonectomy followed by intra-peritoneal chemohyperthermia: an experimental study. Gynecol Oncol 2005;99:358‐361.
- Jacquet P, Stuart OA, Chang D, Sugarbaker PH. Effects of intra-abdominal pressure on pharmacokinetics and tissue distribution of doxorubicin after intraperitoneal administration. Anticancer Drugs 1996;7:596‐603.
- Esquis P, Consolo D, Magnin G, et al. High intra-abdominal pressure enhances the penetration and antitumor effect of intraperitoneal cisplatin on experimental peritoneal carcinomatosis. Ann Surg 2006;244:106‐112.
- Gesson-Paute A, Ferron G, Thomas F, de Lara EC, Chatelut E, Querleu D. Pharmacokinetics of oxaliplatin during open versus laparoscopically assisted heated intraoperative intraperitoneal chemotherapy (HIPEC): an experimental study. Ann Surg Oncol 2008;15:339‐344.
- Garofalo A, Valle M. Laparoscopy in the management of peritoneal carcinomatosis. Cancer J 2009;15:190‐195.
- Valle M, Federici O, Garofalo A. Patient selection for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy, and role of laparoscopy in diagnosis, staging, and treatment. Surg Oncol Clin N Am 2012;21:515‐531.
- Facchiano E, Risio D, Kianmanesh R, Msika S. Laparoscopic hyperthermic intraperitoneal chemotherapy: indications, aims, and results: a systematic review of the literature. Ann Surg Oncol 2012;19:2946‐2950.
- Ba MC, Cui SZ, Lin SQ, et al. Chemotherapy with laparoscope-assisted continuous circulatory hyperthermic intraperitoneal perfusion for malignant ascites. World J Gastroenterol 2010;16:1901‐1907.
- Valle M, Van der Speeten K, Garofalo A. Laparoscopic hyperthermic intraperitoneal peroperative chemotherapy (HIPEC) in the management of refractory malignant ascites: A multi-institutional retrospective analysis in 52 patients. J Surg Oncol 2009;100:331‐334. doi:10.1002/jso.21321.
- Thomas F, Ferron G, Gesson-Paute A, Hristova M, Lochon I, Chatelut E. Increased tissue diffusion of oxaliplatin during laparoscopically assisted versus open heated intraoperative intraperitoneal chemotherapy (HIPEC). Ann Surg Oncol 2008;15:3623‐3624.
- Sugarbaker PH, Van der Speeten K. Surgical technology and pharmacology of hyperthermic perioperative chemotherapy. J Gastrointest Oncol 2016;7:29‐44.
- Facchiano E, Scaringi S, Kianmanesh R, et al. Laparoscopic hyperthermic intraperitoneal chemotherapy (HIPEC) for the treatment of malignant ascites secondary to unresectable peritoneal carcinomatosis from advanced gastric cancer. Eur J Surg Oncol.2008;34:154‐158.
- Knutsen A, Sielaff TD, Greeno E, Tuttle TM. Staged laparoscopic infusion of hyperthermic intraperitoneal chemotherapy after cytoreductive surgery. J Gastrointest Surg 2006;10:1038‐1043.
- Pomel C, Appleyard TL, Gouy S, Rouzier R, Elias D. The role of laparoscopy to evaluate candidates for complete cytoreduction of peritoneal carcinomatosis and hyperthermic intraperitoneal chemotherapy. Eur J Surg Oncol 2005;31:540‐543.
- Laterza B, Kusamura S, Baratti D, Oliva GD, Deraco M. Role of explorative laparoscopy to evaluate optimal candidates for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with peritoneal mesothelioma. In Vivo 2009;23:187‐190.
- Elias D, Goéré D, Di Pietrantonio D, et al. Results of systematic second-look surgery in patients at high risk of developing colorectal peritoneal carcinomatosis. Ann Surg 2008;247:445‐450.
- Chang E, Alexander HR, Libutti SK, et al. Laparoscopic continuous hyperthermic peritoneal perfusion. J Am Coll Surg 2001;193:225‐229.
- Sugarbaker PH. Avoiding Diverting Ileostomy in Patients Requiring Complete Pelvic Peritonectomy. Ann Surg Oncol 2016;23:1481‐1485.
- Zanon C, Clara R, Bortolini M, et al. Chemohyperthermia for advanced abdominal malignancies: a new procedure with closed abdomen and previously performed anastomosis. Int J Hyperthermia 2001;17:456‐464.
- Seshadri RA, Hemanth Raj E. Diagnostic Laparoscopy in the Pre-operative Assessment of Patients Undergoing Cytoreductive Surgery and HIPEC for Peritoneal Surface Malignancies. Indian J Surg Oncol 2016;7:230‐235.
- von Breitenbuch P, Boerner T, Jeiter T, Piso P, Schlitt HJ. Laparoscopy as a useful selection tool for patients with prior surgery and peritoneal metastases suitable for multimodality treatment strategies. Surg Endosc 2018;32:2288‐2294.
- Glehen O, Kwiatkowski F, Sugarbaker PH, et al. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol 2004;22:3284‐3292.
- Pomel C, Appleyard TL, Gouy S, Rouzier R, Elias D. The role of laparoscopy to evaluate candidates for complete cytoreduction of peritoneal carcinomatosis and Lygidakis NJ, Patil A, Giannoulis K, Fukuda T, Kumar R. Laparoscopic hyperthermic intraperitoneal chemotherapy as adjuvant modality following radical surgery for advanced rectal cancer a new look to an old problem. Hepatogastroenterology 2010;57:73‐75.
- Glehen O, Osinsky D, Cotte E, et al. Intraperitoneal chemohyperthermia using a closed abdominal procedure and cytoreductive surgery for the treatment of peritoneal carcinomatosis: morbidity and mortality analysis of 216 consecutive procedures. Ann Surg Oncol 2003;10:863‐869.