

Nutritional Management of Acute Infant Diarrhea: Guidelines
Expert recommendations on feeding practices of milk diets in acute infant diarrhea in India: a collaborative position statement
Gut Health Consortium, Shantanu Dutt¹*, Arunaloke Bhattacharya², Arun Fotedar³, Chandan Ray⁴, Jagadish Dhekne⁵, S. Srinivas⁶˒⁷
- Department of Pediatrics, Dr. Dutt Children Hospital, Moradabad, India
- Department of Pediatric Medicine, Institute of Child Health, Kolkata, India
- Department of Pediatrics, RK Hospital, New Delhi, India
- Department of Pediatric Medicine, Bhagyati Neotia Women and Child Care Centre, Kolkata, India
- Department of Pediatrics, Kartik Hospital, Pradhikaran, Pune, India
- Department of Pediatric Gastroenterology, Apollo Childrens Hospital, Chennai, India
- Department of Pediatric Gastroenterology, Kanchi Kamakoti Childs Trust Hospital, Chennai, India
*Corresponding author:
[email protected]
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Consortium, GH., Dutt, S., et al., 2024. Expert recommendations on feeding practices of milk diets in acute infant diarrhea in India: a collaborative position statement. Medical Research Archives, [online] 12(9).
https://doi.org/10.18103/mra.v12i9.5677
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5677
ISSN 2375-1924
ABSTRACT
Acute infant diarrhea has a significant impact on India’s public health landscape, which is characterized by regional disparities and predominantly viral causes that often resolve on their own. The primary management objective of acute infant diarrhea is to ensure quick recovery while maintaining the nutritional intake of affected infants, aiming to reduce weight loss, manage loose stools better, and reduce the duration of diarrhea. Early refeeding, oral rehydration solution (ORS), and zinc supplementation are critical strategies, according to international consensus and scientific validation. Milk-based diets practically form a key part of dietary choices in young children. There was a need to develop an expert position for the nutritional management of acute infant diarrhea in this aspect in the Indian context. Therefore, between July and September 2023, a series of expert meetings across India were dedicated to formulating an evidence-based position for the nutritional management of acute infant diarrhea. The emphasis was on the benefits of continuing feeding and early refeeding as appropriate, and promoting continued breastfeeding. For non-breastfed infants, a strategic approach to selecting suitable milk diets was deliberated, supporting rapid recovery without compromising nutrition. This strategy not only supports the overall developmental well-being of the infant but also addresses potential issues related to alternative diets, such as palatability, potential long-term effects, and the challenges of reverting to standard milk diets. Through these discussions, a comprehensive framework for managing nutrition in acute diarrhea in infants with milk-based diets was established, highlighting the importance of continued nutritional intake along with standard management guidelines.
Keywords: Diarrhea; infant; low lactose; weight loss; early refeeding; secondary lactose intolerance; malnutrition.
1. Introduction
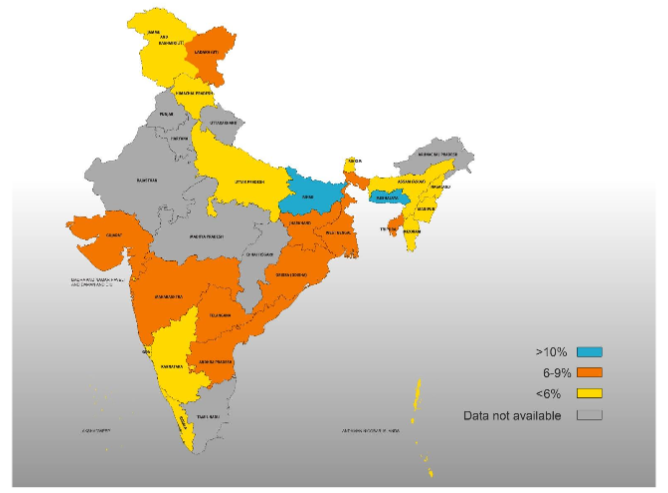
This paper is the outcome of four independent regional meetings that focused on the complex challenges associated with managing the nutritional aspects of acute infantile diarrhea in the diverse dietary landscape of India. Several key factors necessitated the development of this position paper. These include the persistent prevalence of diarrhea among children in India, the concurrent issue of malnutrition, the significance of milk-based diets in children’s nutrition, and the existing guidelines primarily concentrating on diet during prolonged or persistent diarrhea, lacking clear directives regarding milk-based dietary intake in this context¹˒². While the prevalence of childhood diarrhea seemed rooted for nearly a decade³˒⁴, recent statistics in India suggest a positive trend, with a reduction to 7.3% in 2021⁵. This shift may be attributed to improved sanitation infrastructure and the increased access to clean water. However, the tale is far from uniform, as regional disparities paint a complex picture (Figure 1)⁵.
Figure 1: Prevalence of diarrhea in children under 5 years of age in India (5).
Beyond its immediate clinical impact, acute diarrhea, if not managed appropriately, can cause undernutrition/malnutrition, hinder growth and development in children, and affect the quality of life (QoL) of parents⁶˒⁷. Limited awareness of suitable feeding practices during diarrheal episodes contributes to undernutrition in children below the age of 5. Caregivers often lack vital information about appropriate nutritional management during diarrhea, resulting in poor feeding choices. Misguided beliefs are prevalent within the general population, where allowing the gut to rest is mistakenly considered as the management for diarrhea, exacerbating the condition of dehydrating infants⁸⁻¹⁰.
Most cases of acute infant diarrhea are viral in etiology. Rotavirus has historically remained the primary source of severe illness among young children globally. However, norovirus currently accounts for 20% of all instances of infectious diarrhea in developing countries and has been recognized as a prominent contributor to diarrhea within a birth cohort studied in India¹¹˒¹². In the context of viral diarrheal illnesses, the aim is to aid recovery from symptoms and maintain the nutritional status and hydration of the child. The optimal dietary management of acute infantile diarrhea has been a matter of ongoing debate. The major goal of nutritional management in infantile diarrhea apart from preventing dehydration and quick recovery should be to ensure (i) minimal or no weight loss, (ii) manage loose stools, and (iii) shorten the duration of diarrhea. The diet of infants with diarrhea should be easily digestible, gentle on the developing gut, and ensure adequate nutrition¹³. This is important since the infant’s stomach capacity is limited and shared with oral rehydration solution (ORS) intake during diarrhea. The World Health Organization (WHO) and the United Nations International Children’s Emergency Fund (UNICEF) advocate the continuation of breastfeeding alongside the administration of ORS and the supplementation of zinc for the management of acute infantile diarrhea¹⁴. Lactose malabsorption is one of the common problems encountered in prolonged or persistent diarrhea due to the deficiency of the lactase enzyme; this is mostly transient and partial and improves following the resolution of the underlying pathology¹⁵. While a lactose-containing diet may cause repeated dehydration and prolongation of acute diarrhea; a low-lactose diet allows controlled consumption of lactose and shortens the duration of diarrhea. Evidence suggests that a low-lactose diet can effectively manage diarrhea while maintaining a balanced nutrient intake in children with acute gastroenteritis and acute diarrhea¹⁶˒¹⁷.
Drawing on the insights from expert panel discussions, this paper summarizes guidance on implementing the appropriate milk diet for infants as part of managing nutrition in acute infantile diarrhea effectively. Additionally, it provides recommendations to address the multifaceted challenges involved in the nutritional management of infantile diarrhea within the heterogeneous dietary milieu of India.
2. Methodology
Four expert group meetings were conducted region-wise (East, West, North, and South) in India between July and September 2023. The panellists comprised doctors with expertise in child health and nutrition. Each meeting was attended by 12–15 experts from that region. The panel members were selected to best represent the breadth of knowledge and clinical expertise from India. The primary objective of the expert committee meeting was to engage in a comprehensive discussion and formulate expert recommendations regarding the overall nutritional management of infants during diarrhea, with a particular emphasis on the milk feed during acute diarrhea. Discussion areas focused on the approach to dietary choices during diarrhea and the need for a framework for addressing nutrition needs in acute infant diarrhea, are given in Figure 2.
Figure 2: Discussion areas of the meeting.
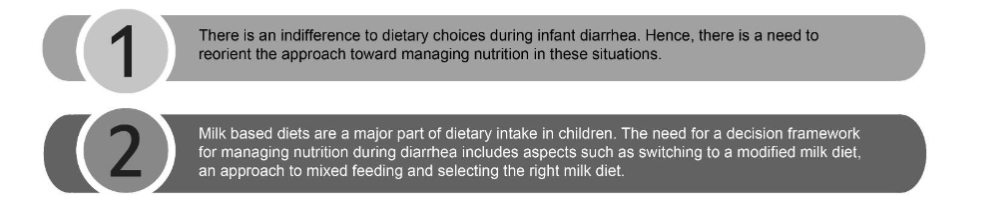
There were key questions for each of the discussion areas: why it is important to manage nutrition in acute infant diarrhea, should lactose intolerance be a concern in acute diarrhea in infants, rationale and advantages of a dietary approach with a low lactose diet, existing guidelines and the necessity to supplement these guidelines with a nutrition-focused perspective to construct a comprehensive decision framework. These questions were discussed with the experts and their opinions were sought. The experts extensively discussed the questions, delving into scientific evidence and guideline recommendations, supplementing their deliberations with clinical expertise to propose practical solutions on (i) current practice patterns; (ii) feeding practices adopted during diarrhea management in infants; (iii) the role of a low lactose infant milk diet in the nutritional management of infantile diarrhea vs. lactose-free or soy-based feeds; and (iv) a clinical approach to the introduction and timing of low lactose feeds. After the group discussion, the expert opinions/recommendations were formulated based on the opinions and agreement of the majority based on a voting pattern. The key highlights of the expert panel discussion and recommendations for each topic was aligned among panel members for the final position statement.
3. Acute diarrhea in infants and malnutrition
Children under 5 years of age in developing countries experience diarrhea an average of 3 times per year, with some locations reporting up to 6–8 occurrences per child per year¹¹. Parental concerns play a pivotal role in the management of diarrhea. A study on the parental perception of the impact of acute infant diarrhea revealed that 72% of parents identified clinical symptoms as one of the most concerning aspects, with the duration and frequency of diarrhea and weight loss as the most meaningful indicators. The survey also indicated that even when diarrhea is clinically mild, it significantly impacts the QoL and how parents perceive the disease burden for their children and themselves¹⁸. Hence, the primary focus in managing acute diarrhea beyond maintaining hydration is to shorten the duration of diarrhea and prevent weight loss¹¹˒¹⁹.
Children with underlying malnutrition are more susceptible to diarrhea. Dehydration and secondary malnutrition are the primary causes of death in these cases. Undernutrition predisposes children to repeated infections, increases the severity of diarrhea, and delays recovery from illness. In addition, repeated infections deplete them of valuable micronutrients required for the functioning of acquired and innate immunity⁷.
Diarrhea and malnutrition have a bidirectional relationship. Diarrheal illness and malnutrition mutually exacerbate one another in a detrimental cycle with the potential for enduring repercussions. Pre-existing malnutrition was often linked to the heightened severity of diarrheal disease²⁰. A long-term Kenyan prospective study by Talbert et al.²¹ demonstrated that the high prevalence of diarrhea in malnourished infants can be attributed to the immunosuppressive impact of malnutrition and, in part, to the compromised integrity of the protective mucosal barrier within the gastrointestinal tract. Diarrhea compromises the intestinal transit time, alters nutrient absorption, and damages the gut epithelium, leading to increased intestinal permeability¹¹˒²¹.
The experts in the panel observed that malnutrition, frequently associated with worsened outcomes in cases of diarrhea, highlights the need to mitigate weight loss and reduce the duration of diarrhea. In the majority of instances involving acute infantile diarrhea, initiating feeds with a reduced lactose content addresses transient lactose intolerance, thereby averting prolonged diarrhea and weight loss. Transient lactose intolerance, prevalent among children with persistent diarrhea, responds well to feeds with reduced lactose levels. Without timely and proper nutritional management, children suffering from persistent diarrhea may experience further weight loss and severe malnutrition, occasionally requiring temporary parenteral nutrition for recovery. Fortunately, such scenarios have become infrequent, largely due to the overall enhancement of infants’ nutritional status 3.1 Clinical approach to acute infant diarrhea
Subramani’s study revealed concerning statistics, indicating that 33% of mothers believed fluids should be ceased during diarrhea, and 42% considered stopping breastfeeding during such episodes¹⁹. These misbeliefs lead to undernutrition, particularly in regions with limited access to healthcare and nutritional guidance. Targeted interventions and caregiver education are urgently needed to address this issue and enhance nutritional outcomes for this vulnerable age group⁸⁻¹⁰. Most acute diarrheal illnesses resolve on their own, and the primary objective of diarrheal management is to prevent dehydration²². Guarino et al.²³ established that the clinical approach adopted to tackle infant diarrhea is markedly dissimilar from the conventional approach used in adults. For infants under 6 months, the focus is on nutritional interventions due to their reliance on breast milk or infant formula for hydration. This contrasts with adults, where nutrition is less emphasized. This difference arises because infants primarily depend on breast milk or infant formula for rehydration, limiting their options. Therefore, promptly resuming feeding and following WHO guidelines is the most effective strategy in cases of acute infant diarrhea. In this context, early refeeding and adherence to the established WHO guidelines constitute the optimal strategy for addressing acute infant diarrhea²³. The practice of initiating refeeding early in the management process yields both clinical and nutritional advantages²⁴.
EXPERTS’ OPINION ON THE ROLE OF NUTRITIONAL MANAGEMENT IN ACUTE INFANT DIARRHEA:
The main objective of nutritional therapy in acute infant diarrhea is to address three fundamental concerns: (i) Mitigating the loss of body weight, (ii) restricting factors leading to the prolongation of diarrhea, and (iii) ensuring speedy recovery of the gut injury. The dietary regimen for infants with diarrhea should prioritize the delicate nature of their developing gastrointestinal tract, ensuring that the food consumed is easily digestible and does not contribute to further irritation of the gut.
Sandhu et al.²⁵, on behalf of the European Society of Paediatric Gastroenterology and Nutrition, conducted a multicenter study comparing early feeding with delayed feeding in infants with acute diarrhea. The study revealed a significantly greater weight gain in the early feeding group than in the delayed feeding group (p=0.001)²⁵. Early refeeding has demonstrated the capacity to stimulate digestive enzymes, enhance nutrient absorption, facilitate enterocyte regeneration, promote disaccharide recovery, shorten diarrhea duration, sustain growth, and ultimately enhance nutritional outcomes. Children without dehydration should maintain their age-appropriate diet and continue feeding, while those with dehydration should resume an age-appropriate diet immediately after rehydration²⁴˒²⁵.
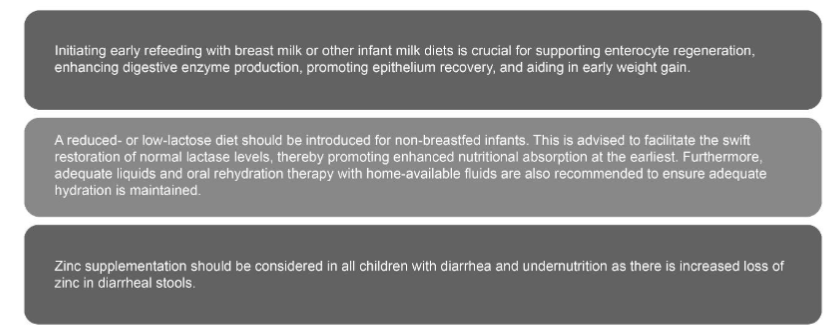
The recommendations of the expert panels regarding the clinical approach to acute infant diarrhea are presented in Figure 3.
Figure 3: Call-to-action: Nutritional management in acute infant diarrhea.
The essential role of nutritional support in the management of acute infant diarrhea stems from the fact that malnutrition and the ensuing dehydration represent the foremost factors contributing to mortality among patients suffering from this condition. Breastfeeding, oral rehydration therapy (ORT) (50–100 mL/kg over 4–6 hours), and appropriate feeds are essential in preventing and treating dehydration and malnutrition consequent to diarrhea²⁶. Research has demonstrated that breastfeeding should be maintained for infants, possibly using ORS as a supplement between feeds²⁰˒²². It is not recommended to provide plain water to infants under 6 months of age. Additionally, there is no necessity to dilute the milk or switch to a lactose-free formula for infants who are being formula-fed²⁰˒²²˒²⁶. It is advisable to avoid fluids with high sugar content, such as commercial carbonated beverages, fruit juices, and sweetened tea, as they can potentially induce osmotic diarrhea²⁷. A pooled analysis by Bhutta et al.²⁷ revealed a significant decrease in the occurrence of diarrhea, with a reduction of approximately 20%, in children who were given zinc supplementation.
3.2 The rationale for the use of a reduced or low lactose infant milk diet
The expert panel provided insights into current trends in feeding practices during episodes of infant diarrhea, that merit additional scrutiny:
- Discontinuing breastfeeding, despite it being imperative to provide all the benefits of breast milk to the infant.
- There is a tendency to use soy-based products as a lactose-free alternative. However, the panelists expressed that guidelines do not recommend a soy-based milk diet as the primary choice for the nutritional management of infant diarrhea. In most cases, a lactose-free diet may not be necessary.
- Avoiding a liquid diet and giving more solids is quite common (especially in infants who are already on complementary food).
Numerous global studies, spanning from Guatemala and Bangladesh to Peru and West Africa, have consistently emphasized the significance of breastfeeding. Infants on complementary food reduced their energy intake by 30% during acute infections, while breastfed infants exhibited a smaller reduction of around 7% in their energy intake. It was also observed that exclusively breastfed infants did not exhibit a diarrhea-induced growth deficit²⁰. Therefore, it can be concluded that exclusive breastfeeding protects an infant from the detrimental nutritional consequences of diarrhea²⁰. There are no misperceptions about the benefits of breast milk, and breastfeeding should be continued particularly during episodes of diarrhea. However, in specific scenarios where breastfeeding is not possible, an alternative nutritional supplement becomes imperative.
A reduced- or low-lactose infant milk diet is a possible alternative in non-breastfed infants during acute diarrhea. Extensive research consistently emphasizes the significance and impact of lactose on infant growth and development. While some studies may suggest a potential association between lactose and osmotic diarrhea, it is crucial to note that such diarrhea typically arises when a substantial quantity of lactose is consumed within a short timeframe, and this is particularly relevant to a subset of children with a high degree of malabsorption²⁸˒²⁹. In contemporary healthcare settings, many hospitals have adopted the practice of administering low or reduced lactose feeds to malnourished infants with acute diarrhea²⁸ because promoting continued breastfeeding while advocating a regimen involving fasting and diluted cow’s milk formula for non-breastfed infants is inconsistent and illogical³⁰.
EXPERTS’ OPINION ON LACTOSE INTOLERANCE AND ADOPTION OF REDUCED LACTOSE DIETS IN INFANTS:
In acute infant diarrhea, lactose intolerance is typically partial, allowing infants to tolerate limited lactose amounts. In the realm of dietary choices, opting for a reduced lactose diet proves more effective than a standard milk diet, as it accommodates the partial loss of lactase activity. In this context, low lactose milk feeds are preferable to diluting regular milk, as dilution risks compromising the balance of essential nutrients. Furthermore, the inclusion of a modest quantity of lactose during acute infant diarrhea proves beneficial because (a) lactose aids in the recovery of the lactase enzyme present on the intestinal brush border and (b) undigested lactose is salvaged by colonic lactic acid bacteria and fermented to produce lactate, short-chain fatty acids (SCFAs), and other metabolites, effectively limiting the proliferation of harmful gut bacteria, particularly valuable during a period when the vulnerable intestinal epithelium is susceptible to invasion.
Lactose intolerance in the context of acute diarrhea in India has been investigated. A study conducted by Veerlapati et al.¹⁶ revealed that among lactose-intolerant infants with diarrhea, those receiving low lactose feeds experienced a shorter duration of hospitalization compared to those on regular lactose-containing feeds (4.82±1.05 days versus 7.59±1.13 days, respectively). Lactose intolerance was found to be more prevalent in cases with malnutrition, although there was no significant correlation with the degree of dehydration. Managing lactose intolerance with low lactose feeds can expedite recovery and enhance positive outcomes in diarrhea cases. This emphasizes the importance of including lactose intolerance in developing more effective diarrhea management guidelines in India¹⁶.
Velarde et al.³¹ have identified additional benefits of consuming lactose through milk. These include shaping the composition of the intestinal microbiota, promoting immune function, and aiding in mineral absorption³¹. Several studies have investigated the impact of substituting lactose-free milk-based diets for lactose-containing diets in managing acute diarrhea²⁰. These studies have concluded that the use of lactose-containing milk is generally safe, particularly among individuals who do not show clinical signs of dehydration. Dehydrated children may experience positive effects from reduced or low lactose consumption and careful monitoring during the initial stages of treatment²⁰˒²⁵.
Lactose further has the potential to be classified as a prebiotic. A study conducted on infants in the age group of 2–12 months with cow’s milk protein allergy (CMA) revealed that lactose alone had a beneficial impact on the gut microbiota composition. A comparative study was conducted between an extensively hydrolyzed lactose-free infant formula and an identical formula containing 38 g/L lactose. Consumption of the lactose-containing formula led to a significant increase in Bifidobacterium and lactic acid bacteria levels, while the levels of Bacteroides and Clostridia decreased²⁸. Owing to the beneficial prebiotic effects of lactose, it has been speculated that infants with low lactase production should consume smaller, more frequent amounts of lactose to obtain benefits and prevent symptoms of lactose intolerance²⁸˒³¹. Lactose, whether supplied as the hydrophilic component of breast milk or as commercially purified lactose, induced the cathelicidin antimicrobial peptide (CAMP) gene, which encodes the human antimicrobial peptide cathelicidin LL-37, in colonic epithelial cells. This induction occurred in a dose- and time-dependent manner. Lactose also triggered CAMP expression in T84 colonic epithelial cells, THP-1 monocytes, and macrophages. These antimicrobial peptides, including CAMP, potentially contribute to developing the neonatal microbiota³¹.
Lactose is the only source of galactose that plays a major role in myelination and a crucial role in facilitating the assimilation of diverse minerals, such as calcium, copper, and manganese²⁸˒³¹. Furthermore, the restriction of lactose intake over a prolonged period has the potential to cause calcium and vitamin B12 insufficiency, which may lead to a reduction in bone mineral density, the development of anemia, and the occurrence of neuropathy³¹.
An extensive review by Alam et al.³³ determined that dehydrated children may benefit from reduced lactose intake (5 g of lactose per 150 kcal), and a low lactose infant milk diet may provide a stimulus for the earlier regeneration of mucosal lactase, which is not attained with a lactose-free diet³³. Infants generally tolerate lactose well, and a lactose-restricted diet is only temporarily required in cases of transient lactase deficiency (secondary lactose intolerance), such as during acute diarrhea, which can be caused by damage to the intestinal epithelium. In addition, research has established that even lactose-intolerant individuals can typically tolerate lactose intake of up to 12 g in a single dose without experiencing significant symptoms³¹. Secondary lactose intolerance often resolves within 6–8 weeks and lactase activity may return to normal after restoring intestinal damage²⁹. Consequently, once the gut health is restored, a reduced lactose diet can be stepped up to resume a standard full-lactose infant milk diet. In the management of acute or persistent diarrhea with secondary lactose intolerance, opting for a low-lactose infant milk diet may be a prudent choice rather than completely eliminating lactose. In a nutshell, the utilization of a low or reduced lactose diet, rather than a lactose-free diet, may serve as a one-step approach to achieving equilibrium between the advantages and potential adverse consequences of lactose in acute infant diarrhea²⁸˒²⁹.
The other alternative to a standard lactose-containing milk diet or modified infant milk diet during acute diarrhea due to secondary lactose intolerance includes a soy-based infant milk diet, which garnered prominence, especially in Western nations in the late 90s. At that time, soy-based formulas were recommended for infants who were unable to consume dairy-based products due to health, cultural, or religious reasons. Over the years, in vitro and animal studies have demonstrated the possibility of the effects of phytoestrogen when consuming a soy-based diet. The isoflavones present in the soy-based infant milk diet may mimic the actions of estradiol, or alter estradiol metabolism, and consequently modify the processes influenced by estradiol³⁴. Additionally, a clinical study had previously documented the occurrence of abnormal thyroid function in infants with congenital hypothyroidism who consumed soy-based formula³⁵. Animal studies have demonstrated a link between phytoestrogen consumption and infertility. In addition, neonatal animals exposed to isoflavones found in soy-based formulas may experience slight changes in the development of sex organs, brain maturation, and the potential to stimulate the development of cancer and immune system malfunction³⁴. Although the results of animal studies cannot be directly extrapolated to human infants, exercising caution in using soy-based diets as the first choice is recommended.
To summarize the experts’ opinion on recommending a reduced lactose milk diet in preference to soy-based infant milk:
a) A low lactose milk diet is ideally suited to treat the transient and partial secondary lactose intolerance that occurs in acute infantile diarrhea. It also acts as a bridge for an easy step-up or step-down approach from a standard milk diet.
b) A low lactose milk diet is preferred over a soy-based milk diet to aid in faster recovery, faster weight gain, reduced duration of diarrhea, and bringing loose stools under control for the following reasons
- The organoleptic and protein profile of milk based formula is better than the soy milk diet.
- Soy-based milk diet has lower palatability and acceptance, which may lead to a slower recovery.
- Soy-based milk often contains sucrose to mask the product’s taste, thus potentially influencing taste preferences in the long term. Hence, transitioning back to the natural standard milk diet from soy-based milk may often pose difficulties.
c) Complementary feeding typically begins at 6 months, but milk feeds are pivotal for infant nutrition during complementary feeding. Infants not consuming milk feeds may struggle with weight gain, a trend that can persist until 2 years of age. Thus, in the context of acute diarrhea, a low or reduced lactose infant milk diet remains a relevant and preferred choice for this age group.
Figure 4 illustrates the diagnostic and management algorithm for addressing acute diarrhea in infants (22,24,36). Expert recommendations concerning low lactose infant milk diets, non-dairy infant diets, and complementary feeding during episodes of diarrhea are detailed in Figure 5.
Figure 4: A decision tree for managing nutrition in acute infant diarrhea.
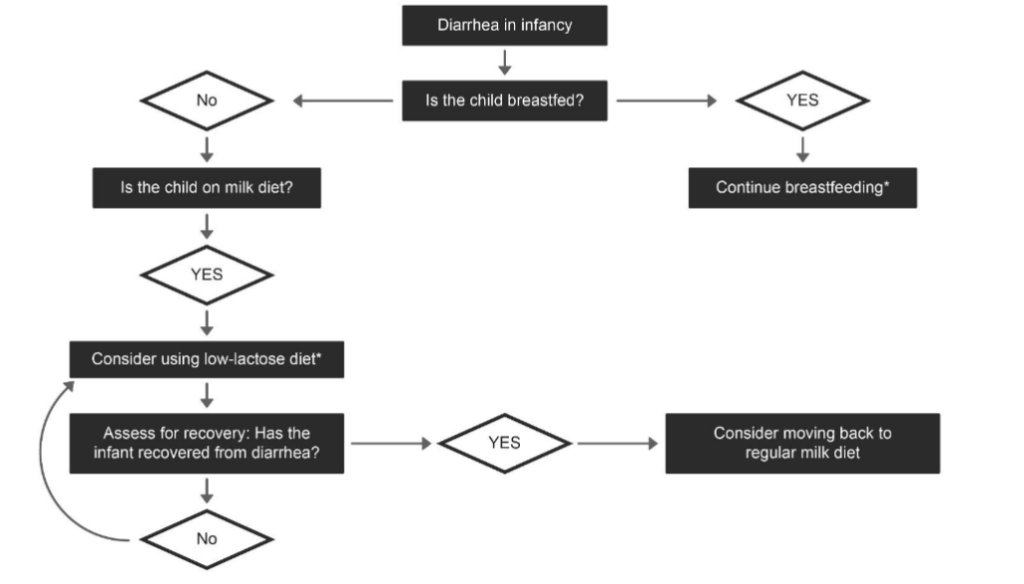
*Along with standard recommendations as per WHO guidelines.
- Consider lactose free alternatives in case of severe lactose intolerance.
- Consider soy based diet only in cases of galactosemia, established CMPA, and ethical considerations. Soy protein should not be used in infants with food allergies during the first 5 months of life.
CMPA: Cow’s milk protein allergy.
WHO: World Health Organization.
Figure 5: Call-to-action: Prefer a low-lactose infant milk diet to a non-dairy infant diet to help manage nutrition in acute infant diarrhea.
CMPA: Cow’s milk protein allergy.
4. Clinical evidence showing the benefit of low lactose milk diets in acute diarrhea
Diarrhea can lead to severe nutritional consequences, especially in vulnerable populations like infants and young children, and the risk of mortality significantly increases when diarrhea becomes persistent³⁷. The experts cited that milk remains the cornerstone of complementary feeding, serving as the primary nutrition source. At 6 months, only one solid food is typically introduced while milk remains the predominant component of meals. Even as additional solid foods are introduced with age, milk plays a significant role in infant nutrition. Infants who are not receiving milk fail to gain sufficient weight despite consuming other foods until they reach two years of age. Additionally, studies recommend a quicker transition to full feeds during acute diarrhea for older children, but more gradually in infants younger than 6 months³⁰. Clinical evidence supports the advantageous effects of a low lactose diet in managing nutrition during diarrhea, both in infants under 6 months old and those older than 6 months¹⁷˒³⁰˒³⁷˒³⁸.
In Wall et al.’s³⁸ study among children up to 2 years old, it was concluded that a low lactose milk diet during refeeding in infants with gastroenteritis could offer benefits, particularly in underweight children where preventing additional weight loss is crucial. Studies have also demonstrated that implementing a low lactose diet during acute diarrhea can lead to reduced symptoms and improved tolerance of dietary intake, contributing to faster recovery and reduced duration of illness. The reduction of lactose intake helps alleviate gastrointestinal distress by reducing the osmotic load and fermentation in the gut, thereby aiding in symptom relief and promoting better absorption of nutrients during the recovery phase¹⁷˒³⁰˒³⁸.
Table 1 summarizes findings from investigations that explore the advantages of a diet with reduced lactose content in the nutritional management of infants experiencing acute diarrhea¹⁷˒²⁹˒³⁰˒³⁸.
Table 1 – Studies on infant milk diets with reduced lactose content.
| Study Title and Year | Study Design | Participants | Main Findings |
|---|---|---|---|
| Sethi et al. 2018²⁹ | Case reports | 4 infants (3 weeks to 11 months old) | Infants with diarrhea were managed with low lactose content milk diets to help maintain energy and nutrient intakes. |
| Wall et al. 1994³⁸ | RCT | 135 infants (1–24 months) | The LCF group was associated with early weight loss and a prolonged duration of diarrhea. The LLF group resulted in a significantly higher rate of weight gain compared with the lactose-free corn syrup-based formula during the initial phase. |
| McClean et al. 1990¹⁷ | RCT | 60 infants (Less than 10 months) | Infants who were given LLF exhibited a tendency toward a greater percentage increase in weight gain and reduction in diarrhea over a 5-day treatment period, in comparison to those who were fed soy-based feeds. Nevertheless, the infants who were given standard feeds or conventional infant formulas experienced an average weight loss of approximately 1.45%. |
| Conway et al. 1989³⁰ | RCT | 200 infants (6 weeks to 12 months) | Infants on a reduced lactose diet had the greatest change in percentage weight gain. |
LCF: Lactose-containing formula; LLF: Low-lactose formula; RCT: Randomized controlled trial.
5. Practical recommendations and guidelines from scientific societies/organisations
Table 2 summarizes the recommendations given by various health agencies worldwide on the nutritional management of acute infant diarrhea¹⁴˒²⁴˒²⁹˒³⁹˒⁴⁰⁻⁴⁴. The expert committee aligns with recommendations from various scientific authorities to prefer low-lactose milk diets during diarrhea and avoid soy-based milk diets as the initial option.
Table 2 – Recommendations for the management of diarrhea in infants
WHO (Global)
- Continued breastfeeding with ORS as a supplement between feedings.
- Do not provide plain water to infants <6 months.
- Do not dilute the formula for non-breastfed infants. In case of persistent diarrhea, a lactose free or low lactose diet is recommended.
- Initial refeeding should involve frequent oral feeds (every 2–3 hours).
- Avoid sweetened drinks, fruit extracts, carbonated beverages, and sweetened tea, as they may lead to osmotic diarrhea.
ESPGHAN (Europe)
- Sustained breastfeeding for breastfed infants without interruption.
- Early refeeding after rehydration is recommended.
- Diluting formula or providing lactose-free formula is not essential during the refeeding process for non-breastfed infants.
- Zinc supplementation is recommended for children over 6 months of age in developing countries with a high prevalence of zinc deficiency.
- Soy milk or soy based infant milk products are not recommended for pre-term infants and infants with food allergies during the first 6 months of life.
- Antibiotics and antimotility agents should not be prescribed to infants for treating acute diarrhea.
AAP (USA)
- Early refeeding following rehydration is recommended to promptly restore nutritional balance.
- ORS is recommended early in the treatment of acute diarrhea.
- Antidiarrheal agents are not recommended in acute diarrhea.
- Soy-based products are not recommended in pre-term infants and infants with food allergies during the first 6 months of life.
IAP (India)
- Continued breastfeeding for breastfed infants.
- Administer low-osmolarity ORS during the intervals between feeds.
- Commence refeeding early.
- Administer zinc promptly upon the onset of symptoms.
- Low-lactose diets can be used in the nutritional management of persistent diarrhea.
CDC (USA)
- Breastfed infants should continue to be nursed on demand.
- ORS and early refeeding are recommended.
- Bottle-fed infants can receive reduced lactose milk diets immediately after rehydration to fulfill energy and nutrient demands.
- Antibiotics and antidiarrheal agents are not indicated in acute diarrhea.
NHS (British)
- It is not advisable to recommend soy products as a first-line option among lactose-intolerant infants, due to a high incidence of soy sensitivity (10%–35%).
- Encourage mothers to continue breastfeeding.
AAP: American Academy of Pediatrics; CDC: Centers for Disease Control and Prevention; ESPGHAN: European Society of Paediatric Gastroenterology, Hepatology, and Nutrition; IAP: Indian Academy of Pediatrics; NHS: National Health Service; ORS: Oral rehydration solution; WHO: World Health Organization.
Health agencies around the globe and the current expert panel are in unanimous consensus that breast milk represents the optimal source of nutrition, and the continuation of breastfeeding is recommended during acute infant diarrhea. Nonetheless, in the case of infants who cannot be breastfed, low lactose milk diets may offer potential benefits²⁹.
Currently, merely 39% of children suffering from diarrhea in developing nations receive the recommended treatment, and the available trend data indicate minimal advancements since 2000⁴⁵. Zinc supplements recommended in most developing countries remain largely inaccessible and underutilized, and the adoption of low-osmolarity ORS has been sluggish, even half a decade after UNICEF and WHO endorsed their inclusion in programs⁴⁵. Therefore, initiating early refeeding and dispelling misconceptions about low lactose infant milk diets during episodes of infantile diarrhea will play a pivotal role in mitigating morbidity and mortality rates among infants and children.
6. Conclusion
This position paper aimed to generate evidence and expert-based recommendations concerning the nutritional management of infants with acute diarrhea, aligning with contemporary scientific understanding and debunking prevalent misconceptions. As applicable, early refeeding or continued feeding is important for appropriate nutritional management strategies to improve outcomes for infants with acute diarrhea. Although breastfeeding remains the primary source of nutrition for infants during acute diarrhea, for those who are not breastfed, a reduced lactose milk diet is supported by cumulative clinical experience, multiple guidelines, and scientific evidence. The expert panel emphasizes the importance of continued breastfeeding and early refeeding in managing acute infantile diarrhea. The expert panel positions and highlights how a milk diet with a reduced lactose content is ideally suited for the management of infantile diarrhea. This dietary adjustment can support appropriate weight gain, help manage loose stools better, and reduce the duration of diarrhea. The panel also highlighted the advantages of low lactose milk diet compared to other milks and how it may be best suited for this condition, acting as a bridge for the effective transition to and from standard infant milk diet.
List of abbreviations
AAP — American Academy of Pediatrics
CDC — Centers for Disease Control and Prevention
CAMP — Cathelicidin antimicrobial peptide
CMPA — Cow’s milk protein allergy
ESPGHAN — European Society of Paediatric Gastroenterology, Hepatology, and Nutrition
ESPGAN — European Society of Pediatric Gastroenterology and Nutrition
IAP — Indian Academy of Pediatrics
LCF — Lactose-containing formula
LLF — Low-lactose formula
NHS — National Health Service
ORS — Oral rehydration solution
ORT — Oral rehydration therapy
SCFAs — Short-chain fatty acids
QoL — Quality of life
Author contributions
SD: Supervision, Validation and Writing-review and editing.
AB, AF, CR, JD, SS: Validation, Writing-review and editing.
All the authors have read, reviewed and approved the final manuscript.
Acknowledgements
We would like to acknowledge BioQuest Solutions Pvt. Ltd., Bangalore, for providing medical writing and editorial support in the preparation of this manuscript. Gut Health Consortium has contributed to the recommendations and opinions on relevant concerns.
Gut Health Consortium, Abhishek Gupta⁸, Akil Mohan⁹, Aliraza Khunt¹⁰, Anil Goyal¹¹, Apurba Banerjee¹², Arun Wadhwa¹³, Arunachalam V¹⁴, Asish Hazra¹⁵, Asraful Mirza¹⁶, Bharat Jain¹⁷, Binay Ranjan¹⁸, Birendra Kumar Singh¹⁹, Chinnu KV²⁰, Daipayan Ghatak²¹, Gokul Krishnan Ramamoorthy²², Jayanta Chakraborty²³, Karthikeyan AG²⁴, Kavitha Sakamuri²⁵, Manjul Vijay²⁶, Manoj Chaturvedi²⁷, Manzur Quader²⁸, Milind Halgekar²⁹, Mohammed Sadique Hussain³⁰, Mohd Arif³¹, Mohit Kulbhushan Vohra³², Mridu Plaban Borah³³, Nanda Kishore³⁴, Naved Akhtar³⁵, Neeraj Jauhri³⁶, Niraj Thapar³⁷, Nirmal Mohakud³⁸, Nomeeta Gupta³⁹, Pankaj Goel⁴⁰, Pinaki Chakraborty⁴¹, Prasanna Nayak⁴², Prashant Moralwar⁴³, Praveen Gokhale⁴⁴, Puneesh Agarwal⁴⁵, Ragavendran N⁴⁶, Rajeev Aggarwal⁴⁷, Rajesh Goel⁴⁸, Rajesh SM⁴⁹, Rakesh Patel⁵⁰, Ravishankar AV⁵¹, Sadashiba Padhy⁵², Sandeep Kumar Singh⁵³, Shivakumar⁵⁴, Sushma Toraskar⁵⁵, Sushil D Nakhate⁵⁶, Vaibhav Shah⁵⁷, Vipul Mehrotra⁵⁸
Affiliations
⁸Department of Pediatrics, Private Practice, Agra, India
⁹Department of Pediatrics, Panchsheel Nursing Home, Mumbai, India
¹⁰Department of Pediatrics, Sehat Children Hospital, Ahmedabad India
¹¹Department of Pediatrics, Alliance Hospital, Mumbai, India
¹²Department of Pediatrics, Private Practice, Kolkata, India
¹³Department of Pediatrics, Wadhwa Clinic, New Delhi, India
¹⁴Department of Pediatrics, V Care Hospital, Tuticorin, India
¹⁵Department of Pediatrics, Private Practice, Medinipur, India
¹⁶Department of Pediatrics, Kisholoy Children’s Hospital, Burdwan, India
¹⁷Department of Pediatrics, Axon Hospital, Panchkula, India
¹⁸Department of Pediatrics, Mahavir Vaatsalya Aspatal, Patna, India
¹⁹Department of Pediatrics, Private Practice, Patna, India
²⁰Department of Neonatology, Sabine Hospital, Muvattupuzha, India
²¹Department of Pediatrics, UMRI Hospital, Kolkata, India
²²Department of Neonatology, Narayana Medical College, Nellore India
²³Department of Pediatrics, Private Practice, Kolkata, India
²⁴Department of Pediatrics, Sai Mother and Child Care, Chennai, India
²⁵Department of Pediatric Endocrinology, Rainbow Hospitals, Hyderabad, India
²⁶Department of Pediatrics, Mediverse Hospital, Gaya, India
²⁷Department of Pediatrics, Shree Krishna Maternity and Child Care Hospital, Mumbai, India
²⁸Department of Pediatric Medicine, Bhagirathi Neotia Woman and Child Care Centre, Kolkata, India
²⁹Department of Pediatrics, Mai Hospital, Belgaum, India
³⁰Department of Pediatrics, Little Champ Childrens Clinic, Bangalore, India
³¹Department of Pediatrics, Kilkari Nursing Home and Clinic, Bijnor, India
³²Department of Pediatrics, Nav Imperial Hospital and Research Centre, Jaipur, India
³³Department of Pediatric Medicine, Apollo Excelcare hospital, Guwahati, India
³⁴Department of Pediatrics, Srinivasa Multi Speciality Children Hospital, Vijayawada, India
³⁵Department of Pediatrics, Smart Hospital, Ghaziabad, India
³⁶Department of Pediatrics, Private Practice, Lucknow, India
³⁷Department of Pediatrics, Suman Hospital, Ludhiana, India
³⁸Department of Pediatrics, Kalinga Institute of Medical Sciences, Bhubaneswar, India
³⁹Department of Pediatrics, Batra Hospital and Medical Research Centre, New Delhi, India
⁴⁰Department of Pediatrics, Mayi Kamli wali Hospital, New Delhi, India
⁴¹Department of Neonatology, Silchar Medical College and Hospital, Silchar, India
⁴²Department of Pediatrics, Keerti Clinic, Kumta, India
⁴³Department of Pediatrics, Motherhood Hospital, Mumbai, India
⁴⁴Department of Pediatrics, Jupiter Hospital, Thane, India
⁴⁵Department of Pediatrics, Urmila Devi Hospital, Lucknow, India
⁴⁶Department of Pediatrics, Amirtha Clinic, Palani, India
⁴⁷Department of Pediatrics, Dr. Rajeev Aggarwal Child and Vaccination Centre, Ghaziabad, India
⁴⁸Department of Pediatrics, ILS Hospitals, Kolkata, India
⁴⁹Department of Pediatrics, Srinivasa Childrens Clinic, Mangalore, India
⁵⁰Department of Pediatrics, Amruta Hospital, Rajkot, India
⁵¹Department of Pediatrics, Child Care Clinic, Chennai, India
⁵²Department of Pediatrics, Utkal Hospital, Bhubaneswar, India
⁵³Department of Pediatrics, District Women Hospital and Sheetal Tara Children Hospital, Jaunpur, India
⁵⁴Department of Pediatrics, Petals Neocare Children’s Hospital, Karimnagar, India
⁵⁵Department of Pediatrics, Indravati Hospital, Navi Mumbai, India
⁵⁶Department of Pediatrics, Dr Nakhate’s Child Care Centre, Mumbai, India
⁵⁷Department of Pediatric Gastroenterology, Gujarat Superspeciality Clinic, Ahmedabad, India
⁵⁸Department of Pediatrics, Shishu Child Care Clinic, Mumbai, India
Conflict of Interest:
None
Funding Statement:
None.
References
1. Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong KL, et al. Global, regional, and national causes of under-5 mortality in 2000-19: An updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Health (2022) 6:106–15. doi: 10.1016/S2352-4642(21)00311-4
2. UNICEF. The United Nations International Children’s Emergency Fund 2019 Report on Diarrhoea. https://data.unicef.org/topic/child-health/diarrhoeal-disease/ [Accessed October 7, 2023].
3. International Institute for Population Sciences (IIPS) and Macro International. National Family Health Survey (NFHS-3), 2005–06: India: Volume I (2007). https://dhsprogram.com/pubs/pdf/frind3/frind3-vol1andvol2.pdf [Accessed September 29, 2023].
4. International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey (NFHS-4), 2015–16: India (2017). http://rchiips.org/nfhs/NFHS-4Reports/India.pdf [Accessed September 29, 2023].
5. National Family Health Survey (NFHS-5), 2019–21: India Fact Sheet. https://main.mohfw.gov.in/sites/default/files/NFHS-5_Phase-II_0.pdf [Accessed September 29,2023].
6. Roy SK, Buis M, Weersma R, Khatun W, Chowdhury S, Begum A, et al. Risk factors of mortality in severely-malnourished children hospitalized with diarrhoea. J Health Popul Nutr (2011) 29:229–35. doi:10.3329/jhpn.v29i3.7870
7. Chiabi A, Obadeyi B, Nguefack F, Chiabi R, Berinyuy E, Chiabi E, et al. The vicious cycle of malnutrition and childhood infections – What are the policy implications? Arch Pediatr Neonatol (2018) 1:21–5. doi: 10.22259/2638-5155.0101006
8. Subramani H, Patil R, Nisha N, Palve S, A L. A study of misconceptions about childhood diarrhoea among adults in urban Pondicherry, India. Int J Community Med Public Health (2016) 3:1442–48. doi: 10.18203/2394-6040.ijcmph20161608
9. Gandra NR, Farooqui D. Diarrhoea, nutrition and oral rehydration therapy: Awareness, attitude and practices among mothers of children under five years. Int J Contemp Pediatr (2017) 4:1995–2001. doi: 10.18203/2349-3291.ijcp20174182
10. Padhy S, Sethi RK, Behera N. Mother’s knowledge, attitude and practice regarding prevention and management of diarrhoea in children in Southern Odisha. Int J Contemp Pediatr (2017) 4:966-71. doi: 10.18203/2349-3291.ijcp20171708
11. Nemeth V, Pfleghaar N. Diarrhea. In: StatPearls. Treasure Island (FL): StatPearls Publishing (2023). http://www.ncbi.nlm.nih.gov/books/NBK448082/
12. Menon VK, George S, Sarkar R, Giri S, Samuel P, Vivek R, et al. Norovirus Gastroenteritis in a Birth Cohort in Southern India. PLoS One (2016) 11:e0157007. doi: 10.1371/journal.pone.0157007
13. Acharyya BC, Srivastava PK. Nutritional management during and beyond diarrhea. Role of rice-based foods. Neonat Pediatr Med (2022) 8:263. doi: 10.4172/2572-4983.1000263
14. Pocket Book of Hospital Care for Children: Guidelines for the Management of Common Childhood Illnesses. 2nd ed. Geneva: World Health Organization (2013). http://www.ncbi.nlm.nih.gov/books/NBK154447/
15. Heine RG, AlRefaee F, Bachina P, De Leon JC, Geng L, Gong S, et al. Lactose intolerance and gastrointestinal cow’s milk allergy in infants and children – common misconceptions revisited. World Allergy Organ J (2017) 10:41. doi: 10.1186/s40413-017-0173-0
16. Veerlapati R, Prasad KNV. Study on lactose intolerance in children with acute diarrhoea. JMSCR (2019) 7:502-508. doi: 10.18535/jmscr/v7i10.85
17. McClean P, Lynch AB, Dodge JA. Comparison of three regimens in the management of acute gastroenteritis in infants. Aliment Pharmacol Ther (1990) 4:457–464. doi: 10.1111/j.1365-2036.1990.tb00492.x.
18. Huppertz HI, Forster J, Heininger U, Roos R, Neumann HU, Hammerschmidt T. The Parental Appraisal of the Morbidity of Diarrhea in Infants and Toddlers (PAMODI) survey. Clin Pediatr (2008) 47:363–71. doi: 10.1177/0009922807310933
19. Dekate P, Jayashree M, Singhi SC. Management of acute diarrhea in emergency room. Indian J Pediatr (2013) 80:235–246. doi: 10.1007/s12098-012-0909-3
20. Brown KH. Diarrhea and malnutrition. J Nutr (2003) 133:328S–332S. doi:10.1093/jn/133.1 .328S
21. Talbert A, Thuo N, Karisa J, Chesaro C, Ohuma E, Ignas J, et al. Diarrhoea complicating severe acute malnutrition in Kenyan children: A prospective descriptive study of risk factors and outcome. PLoS One (2012) 7:e38321. doi: 10.1371/journal.pone.0038321
22. Viegelmann GC, Dorji J, Guo X, Lim HY. Approach to diarrhoeal disorders in children. Singapore Med J (2021) 62:623–9. doi: 10.11622/smedj.2021234
23. Guarino A, Ashkenazi S, Gendrel D, Lo Vecchio A, Shamir R, Szajewska H, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/ European Society for pediatric infectious diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: Update 2014. J Pediatr Gastroenterol Nutr (2014) 59:132–52. doi: 10.1097/MPG.0000000000000375
24. Leung A, Prince T, Canadian Paediatric Society, Nutrition and Gastroenterology Committee. Oral rehydration therapy and early refeeding in the management of childhood gastroenteritis. Paediatr Child Health (2006) 11:527–31. doi: 10.1093/pch/11.8.527
25. Sandhu BK, Isolauri E, Walker-Smith JA, Banchini G, Van Caillie-Bertrand M, Dias JA, et al. A multicentre study on behalf of the European Society of Paediatric Gastroenterology and Nutrition Working Group on acute diarrhoea. Early feeding in Childhood Gastroenteritis. J Pediatr Gastroenterol Nutr (1997) 24:522–7. doi: 10.1097/00005176-199705000-00006
26. Manary M, Iannotti L, Trehan I, Weisz A. Systematic review of the care of children with diarrhoea in the community-based management of severe acute malnutrition. In Geneva: World Health Organization; 2012.
27. Bhutta ZA, Black RE, Brown KH, Gardner JM, Gore S, Hidayat A, et al. Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: Pooled analysis of randomized controlled trials. Zinc Investigators’ Collaborative Group. J Pediatr (1999) 135:689–697. doi: 10.1016/s0022-3476(99)70086-7
28. Grenov B, Briend A, Sangild PT, Thymann T, Rytter MH, Hother AL, et al. Undernourished children and milk lactose. Food Nutr Bull (2016) 37:85–99.doi: 10.1177/0379572116629024
29. Sethi G, Sankaranarayanan S, Sukhija M. Low lactose in the nutritional management of diarrhea: Case reports from India. Clin Epidemiol Glob Health (2018) 6:160–162. doi: 10.1016/j.cegh.2018.02.002
30. Conway SP, Ireson A. Acute gastroenteritis in well-nourished infants: Comparison of four feeding regimens. Arch Dis Child (1989) 64:87–91. doi: 10.1136/adc.64.1.87
31. Romero-Velarde E, Delgado-Franco D, García-Gutiérrez M, Gurrola-Díaz C, Larrosa-Haro A, Montijo-Barrios E, et al. The importance of lactose in the human diet: Outcomes of a Mexican consensus meeting. Nutrients (2019) 11:2737. doi: 10.3390/nu11112737
32. Schaafsma G. Lactose and lactose derivatives as bioactive ingredients in human nutrition. Int Dairy J (2008) 18:458–65. doi: 10.1016/j.idairyj.2007.11.013
33.Alam S, Khanna R, Firdaus U. Acute childhood diarrhea: A review of recent advances in the standard management. Pediatr Oncall J (2006) 3:72.
34. Canadian Paediatric Society. Concerns for the use of soy-based formulas in infant nutrition. Paediatr Child Health (2009) 14:109–113.
35. Jabbar MA, Larrea J, Shaw RA. Abnormal thyroid function tests in infants with congenital hypothyroidism: the influence of soy-based formula. J Am Coll Nutr (1997) 16:280–282. doi: 10.1080/07315724.1997.10718686
36. Vega RM, Avva U. Pediatric Dehydration. In: StatPearls. Treasure Island (FL): StatPearls Publishing (2023). http://www.ncbi.nlm.nih.gov/books/NBK436022/
37. Ashraf H, Ahmed S, Fuchs GJ, Mahalanabis D. Persistent diarrhoea: Associated infection and response to a low lactose diet. J Trop Pediatr (2002) 48:142–148. doi: 10.1093/tropej/48.3.142
38. Wall CR, Webster J, Quirk P, Robb TA, Cleghorn GJ, Davidson GP, et al. The nutritional management of acute diarrhea in young infants: Effect of carbohydrate ingested. J Pediatr Gastroenterol Nutr (1994) 19:170-4. doi: 10.1097/00005176-199408000-00005
39. Guarino A, Vecchio AL, Dias JA, Berkley JA, Boey C, Bruzzese D, et al. Universal recommendations for the management of acute diarrhea in nonmalnourished children. J Pediatr Gastroenterol Nutr (2018) 67:586–93. doi: 10.1097/MPG.0000000000002053
40. Szajewska H, Hoekstra JH, Sandhu B; ESPGHAN Working Group on Acute Diarrhoea. Management of acute gastroenteritis in Europe and the impact of the new recommendations: A multicenter study. The working group on acute diarrhoea of the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr (2000) 30:522–7. doi: 10.1097/00005176-200005000-00011
41. American Academy of Pediatrics, Provisional Committee on Quality Improvement, Subcommittee on Acute Gastroenteritis. Practice parameter: The management of acute gastroenteritis in young children. Pediatrics (1996) 97:424–35.
42. Bhatnagar S, Lodha R, Choudhury P, Sachdev HP, Shah N, Narayan S, et al. IAP guidelines 2006 on hospital-based management of severely malnourished children (adapted from the WHO Guidelines). Indian Pediatr (2007) 44:443–61.
43. Centers for Disease Control and Prevention. The management of acute diarrhea in children: Oral rehydration, maintenance, and nutritional therapy (1992). https://www.cdc.gov/mmwr/preview/mmwrhtml/00018677.htm [Accessed October 10, 2023].
44. NHS Pan Mersey Area Prescribing Committee. Lactose intolerance and cows’ milk protein allergy – Prescribing guidelines for specialist infant formula feeds (2021). https://www.panmerseyapc.nhs.uk/media/1192/infant_formula.pdf [Accessed October 10, 2023].
45. Wardlaw T, Salama P, Brocklehurst C, Chopra M, Mason E. Diarrhoea: Why children are still dying and what can be done. Lancet (2010) 375:870–2. doi: 10.1016/S0140-6736(09)61798-0.