





Atypical CT Features of Pulmonary Tuberculosis in Adults
Atypical Computed Tomography Features of Pulmonary Tuberculosis: Findings and Diagnostic Challenges
I. Introduction
Tuberculosis (TB), caused by Mycobacterium tuberculosis, is still an endemic infection worldwide particularly in low-and middle-income countries with 10 million new cases per year¹. It is estimated that a quarter of the world’s population has been infected with TB¹. TB was the leading cause of death from an infection before the COVID-19 era and causes twice as many deaths as HIV/AIDS.
Screening for tuberculosis in the target population is based on symptoms, molecular tests and chest X- ray (CXR). The latter has a sensitivity varying between 85 and 94% and a specificity varying between 89% and 96%. Computer-aided detection is being recommended as an alternative to physicians’ interpretation with target sensitivity and specificity higher than 90% and 70%, respectively².
Computed tomography (CT) is more sensitive than CXR for the detection of subtle signs of pulmonary TB. Typical features include consolidations, centrilobular micronodules with a tree-in-bud feature, nodules and consolidations. Cavitation is a hallmark of activity and is correlated with positive smear sputum. Lesions are typically located in the upper lobes and the Fowler segments³.
However, CT scans may show subtle and unique features that can overlap with other respiratory conditions leading to a delay in diagnosis and treatment. These mainly include uncommon lung lesions and locations as well as the association with other pulmonary conditions. There is a predisposition for unusual tubercular sites and features in patients with conditions affecting cell-mediated immunity such as immunosuppression caused by HIV/AIDS, immune-mediated inflammatory diseases, steroid use, organ transplant recipients, malnutrition and low body mass index, diabetes, smoking and alcohol consumption⁴.
This paper is a narrative review of atypical CT features of pulmonary TB that clinicians and radiologists should be mindful of to improve diagnostic accuracy.
II. Uncommon computed tomography features:
- MASSES :
TB and lung cancer often present with the same clinical symptoms and physical signs such as weight loss, chest pain, hemoptysis and cough. Radiological signs of both conditions are different in most cases. However, TB may present with a phenotype that overlaps with peripheral lung cancer explained by the widespread consumption of antibiotics and the aging population⁵. Pseudotumoral TB is rare and accounts for less than 5% of all cases of pulmonary TB, particularly in immunocompetent patients⁶˒⁷˒⁸. Both conditions may be associated in extremely rare cases⁸. CT is commonly used to characterize lung nodules and masses based on their size, shape, margins, density, enhancement and follow-up in order to suggest whether they are benign or malignant. Radiomics, which involves computer analysis of image features may help distinguish TB from lung cancer⁹. Some CT features that may help distinguish TB from lung cancer include the low-density center, ring-like enhancement, location to the upper lobes and Fowler segments, and association with centrilobular micronodules (figure 1). Proof of TB infection is obtained through lesion biopsy with pathological and bacteriological examinations. - SOLITARY NODULE:
Solitary pulmonary nodules are discovered in less than 1% of cases on CXR and on 30% of CT scans¹⁰˒¹¹. Every solitary nodule should be characterized by CT and should have the appropriate work up according to its density and size. More than 95% of identified solitary nodules are benign and correspond either to granulomas or intra-parenchymal lymph nodes¹¹. Typical features of benignity include the presence of macroscopic fat, concentric, popcorn or central calcifications as well as a long doubling time. Typical features of malignancy include irregular margins, bronchogram, bubble-like lucencies as well as short doubling time and growing sub-solid nodules. Sometimes, some nodules may remain indeterminate¹². It is reported that TB is responsible for 57 to 92% of false positive diagnosis of primary lung cancer in endemic regions¹³. It is difficult in front of a single nodule to suggest tuberculosis particularly when it is a sub-solid nodule. TB is identified in less than 1% of surgically removed nodules. Atypical mycobacteria cause more frequently solitary nodules than Mycobacterium tuberculosis. Nodules may correspond to tuberculomas or less frequently to an active TB¹⁴. Presence of calcification and ring-like enhancement in an endemic context makes the diagnosis of tuberculomas easy (figure 2). TB solitary nodules may be cavitary or not, whether corresponding to tuberculomas or not¹⁵. Tree-in-bud pattern and satellite lesions favor the diagnosis of TB whereas lobulations, pleural indentations and vessel convergence favor the diagnosis of lung cancer¹³.
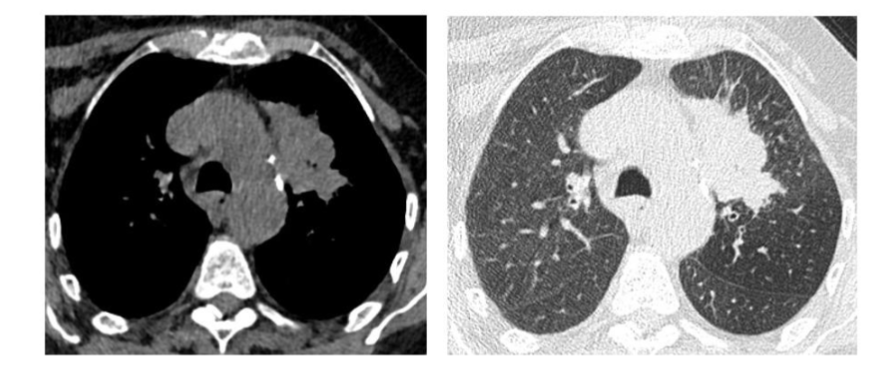
Figure 1: Isolated mass of the culmen in a 75-year-old women. Transparietal biopsy : TB
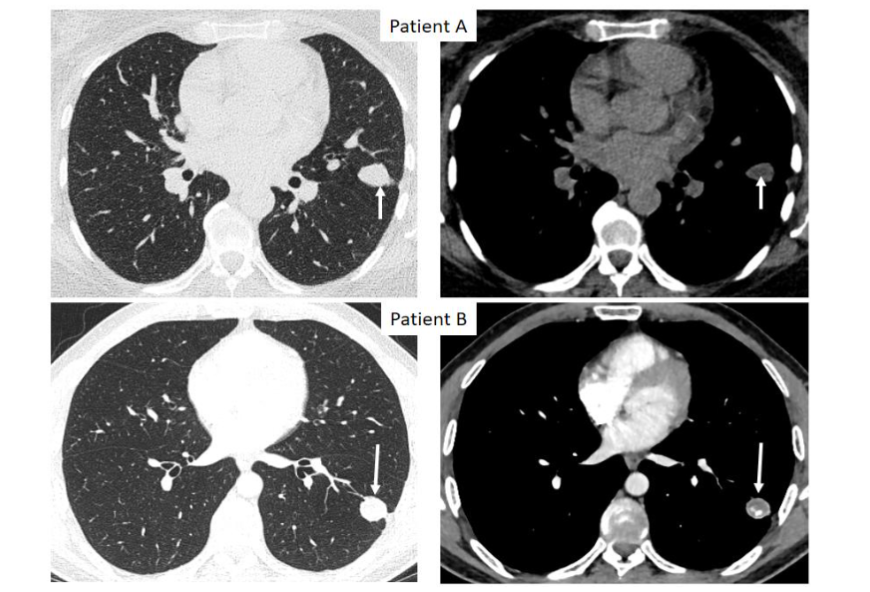
Figure 2: Solitary nodules in two different patients (arrows). Patient A: nodule of the lingula with central necrosis. Patient B: Nodule of the left lower lobe with central necrosis, calcifications and ring-like enhancement. Lung biopsy in patient A and surgery in patient B confirmed the diagnosis of pulmonary TB.
- MULTIPLE NODULES:
Hematogeneous dissemination of TB typically results in a miliary feature, which corresponds to dense, tiny and randomly distributed micronodules. Nodules with more than three millimeters size is a rare feature of hematogeneous spread. They may be associated to a pleural effusion or to other organs involvement¹⁶. Presence of multiple nodules, first suggest metastasis, especially when there is no sign of bronchial dissemination. Cavitation may suggest granulomatosis with polyangeitis¹⁷ (figure 3).
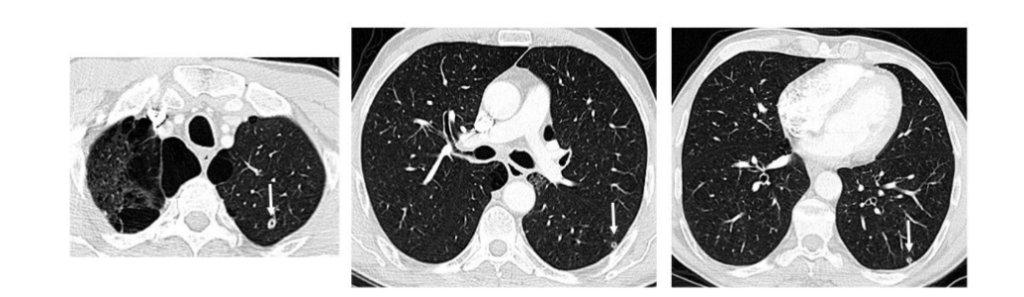
Figure 3: three cavitary nodules of the left lung with no other sign suggestive of TB in 54-year-old men. Surgical biopsy confirmed the diagnosis of TB
- GROUND GLASS OPACITIES:
Ground glass opacities (GGO) are defined by high-density parenchymal areas with vessels and bronchial walls remaining visible inside. They may result from an interstitial modification or from an incomplete alveolar filling. GGO are rare in TB, and are present in less than 1% of cases of active TB. They are particularly observed in HIV seropositive patients¹⁸. Patients present generally with respiratory failure or acute respiratory distress syndrome. GGO generally coexist with a miliary feature and with interlobular septal thickening¹⁹˒²⁰˒²¹ (figure 4). It may also be observed in paradoxical reaction or in patients with lung transplant²²˒²³.
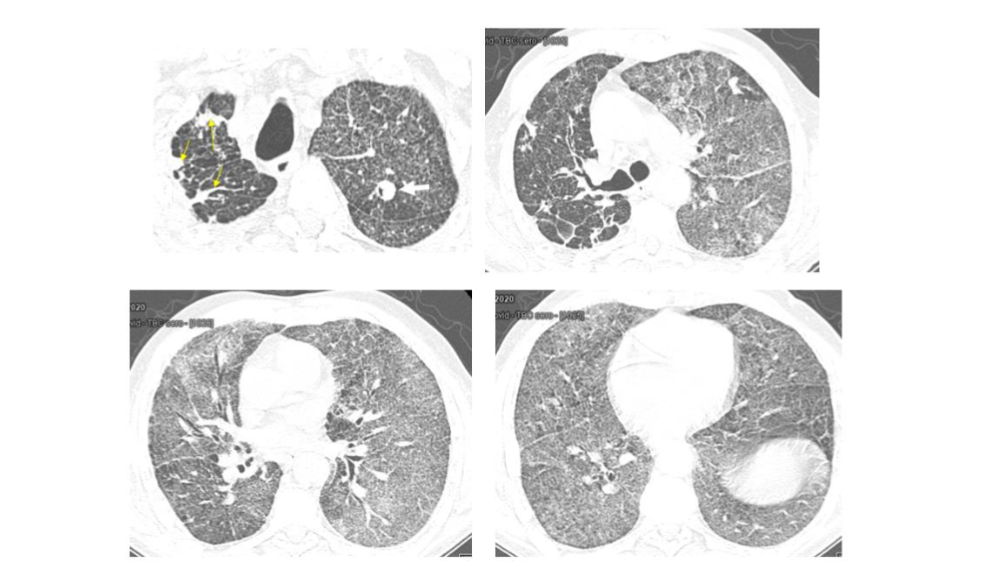
Figure 4: Respiratory failure in a 54 year-old men. CT showed TB sequels of the right lung (yellow arrows), with a cavitary nodule of the culmen (white arrow) and diffuse GGO. Sputum culture: TB positive
- REVERSED HALO SIGN:
Reversed halo sign refers to a parenchymal consolidation surrounding an area of a central lucency or GGO. It was first described in cryptogenic organizing pneumonia. However, it was later described in secondary organizing pneumonia to many other conditions such as infections or radiotherapy and in many other conditions²⁴˒²⁵. It is significantly highly observed in granulomatous diseases, particularly in TB, rather than in non-granulomatous diseases²⁵. This sign is observed in 17% to 29% of patients with active TB²⁵˒²⁶. It is characterized by the presence of nodules or micronodules within and inside the wall. The peripheral rim may be complete or incomplete²⁶˒²⁷. Lesions may be solitary or multiple²⁸ (figure 5). Pathology studies confirm the presence of granulomas in the wall, with or without acid-fast stain positivity as well as caseous necrosis²⁵˒²⁸. The nodular reversed halo sign is not exclusively observed in TB. It may also be found in cryptogenic organizing pneumonia, lung cancer, sarcoidosis, cryptococcosis, and granulomatosis with polyangiitis²⁶. Its association with more typical features is suggestive of the diagnosis.
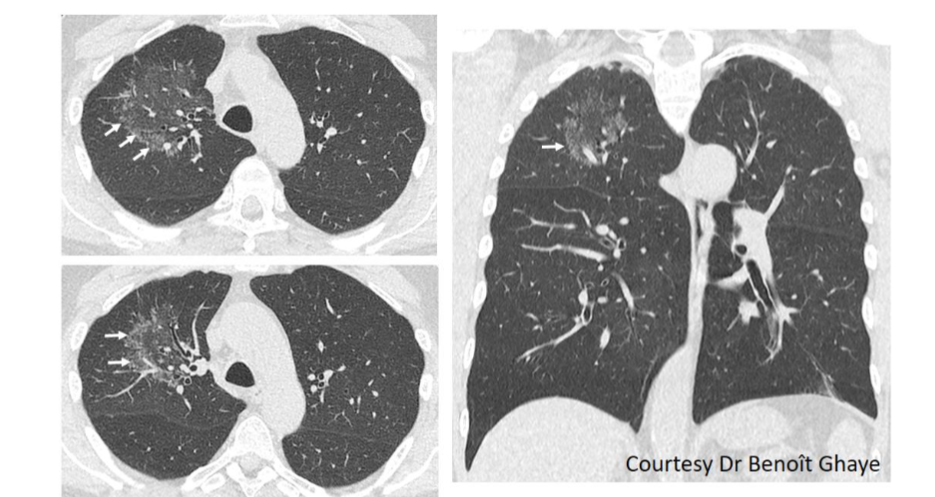
Figure 5: Subtle reversed halo sign of the right upper lobe with peripheral micronodules (arrows). The diagnosis of TB was confirmed by surgery
- CYSTIC AND BULLOUS LESIONS
Cysts, defined as airspaces with a thin wall, are an extremely rare feature of pulmonary TB. There are only few published papers about this condition. This pattern occurs accordingly often in young people and children as well as in women²⁹˒³⁰˒³¹˒³²˒³³. Patients present generally with severe respiratory impairment²⁹. Cysts may appear before or during anti-tuberculous treatment and they may be complicated by pneumothorax or pneumomediastinum²⁴˒²⁹. Cysts predominate to the upper lobes and the mid lungs and curiously to the anterior regions²⁹˒³⁴. They are frequently of a small size²⁹. They generally coalesce and have an irregular shape³⁰ (figure 6). Proposed mechanisms for the development of such lesion include the check-valve effect caused by granulomatous inflammation development in distal bronchi, cystic bronchiectasis following caseous necrosis of bronchial walls, interstitial air leakage following rupture of tubercle lesions and bronchioles dilatation²⁹˒³⁰˒³¹˒³². They may increase in size especially in the first weeks of treatment and they may resolve or be stable later on²⁹. Cystic TB is lethal in 14% of cases³²˒³⁵.
Differential diagnoses include Langerhans histiocytosis, lymphangioleiomyomatosis, pneumocystis and lymphocytic interstitial pneumonia²⁹˒³⁰.
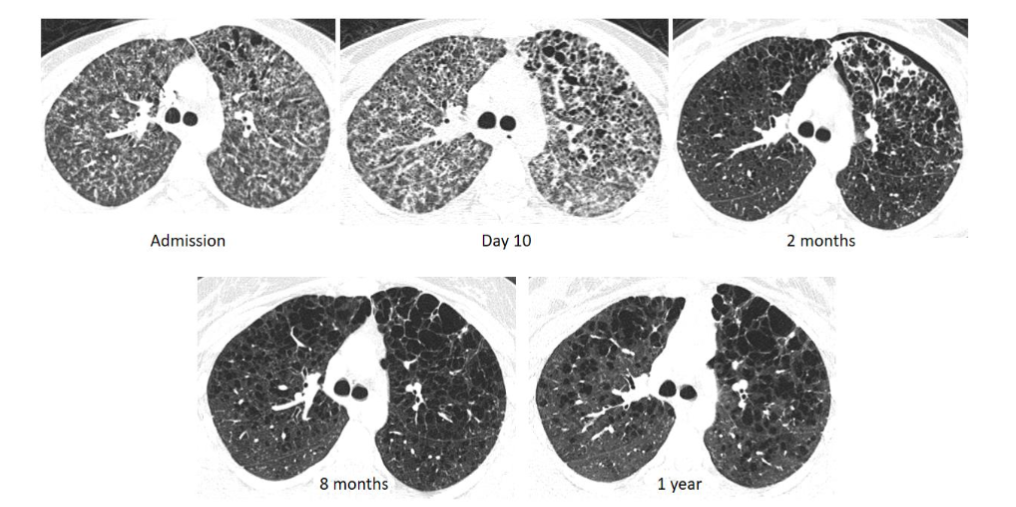
Figure 6: a 21 year-old women presented with fever and respiratory failure. CT at admission showed a pulmonary miliary and few cysts of the culmen. PCR for TB was positive. Cysts enlarged at day 10 control. They were complicated by a pneumothorax at 2 months. They became bigger and remained stable thereafter
III. Uncommon location of pulmonary tuberculosis:
Classically, post primary TB lesions are located in the upper lobes and in the Fowler segments. However, in immunocompromised patients, consolidations can be observed in the basal segments of the lower lobes. TB of the lower lobes is defined by the presence of lesions exclusively under the carina³⁶ (figures 7 and 8).
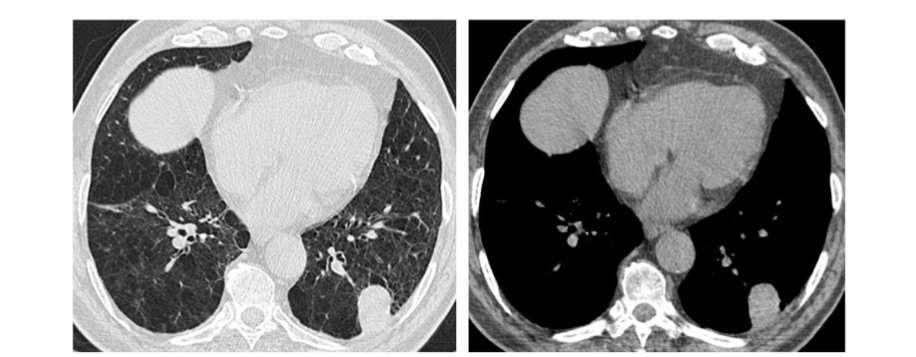
Figure7: a well-limited and isolated mass of the lower left lobe that was removed by surgery. Pathology examination confirmed the diagnosis of TB
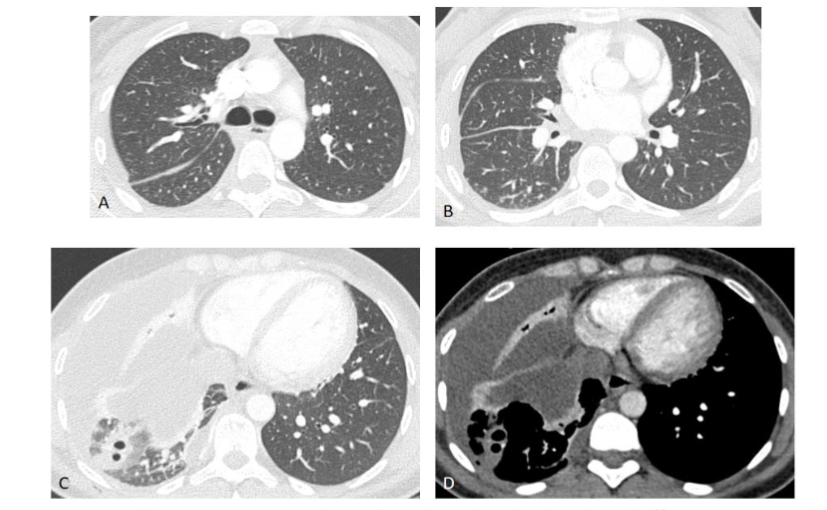
Figure 8: A 28 year-old women presented initially with isolated right pleural effusion. Two weeks later, she developed acinar nodules and cavitary consolidation of the right lower lobe with no lesions of the upper lobes. TB positive in the pleural fluid.
IV. Association with other pulmonary conditions:
- EMPHYSEMA
Patients with chronic obstructive lung disease have a higher risk than normal population to develop tuberculosis³⁷. In fact, in case of emphysema, there is a local lack of phagocytosis cells and general immune suppression explained by constant systemic inflammation. Lesions location does not differ between patients with or without emphysema. However, consolidations are more frequent than tree-in-bud feature. In fact, they are present in 82% of TB cases whereas tree-in-bud is present in only 36% of cases³⁷˒³⁸.
Development of consolidations on a background of emphysema may result in a honeycomb-like feature or may look like tuberculosis cavity¹⁶ (figure 9).
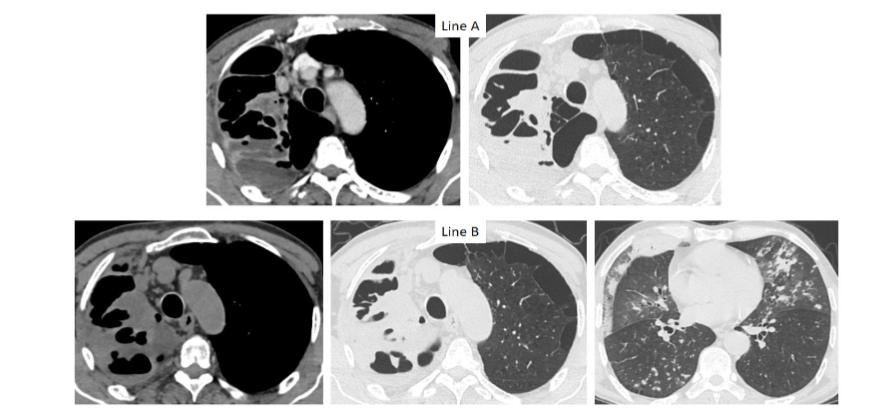
Figure9: A 59 year-old men presented with fever and increased blood inflammatory markers. First CT (line A) showed complicated bullous emphysema of the right upper lobe. The patients didn’t improve under antibiotics. Second CT showed persistence of complicated emphysema and new signs of active TB. Sputum culture positive for TB.
- INTERSTITIAL LUNG DISEASE:
Coexistence of TB with an interstitial lung disease (ILD) is a rare situation. ILDs are observed in 6% of TB positive patients. UIP is the most frequently reported ILD to be reported³⁹. Previous studies confirmed that TB is 4 to 5 times more frequent in patients with ILDs, than in other patients. Presence of an underlying ILD may lead to misdiagnosis of TB either clinically or radiologically⁴⁰. Lesions are, as usual, often located to the upper lobes. However, non-segmental consolidation, developing in fibrotic areas without centrilobular micronodules, is the most frequent sign³⁹.
Some ILDs may be misdiagnosed as TB if clinicians and radiologists are not aware of these conditions particularly in countries with high TB burden⁴¹. In fact, TB and silicosis may present with fibrotic lesions of the upper lungs, micronodules nodules and calcified lymph nodes making the radiological diagnosis difficult. Cavitation, hallmark of active TB, is also possible in silicosis. Co-occurrence of TB and silicosis, known as silicotuberculosis, is also frequently reported in miners and in countries with extractive industries whether they have a heavy burden of TB or not. Silicosis multiplies the risk for TB by 2.5, which is explained by the impairment of antibacterial mechanism by silica exposure⁴²˒⁴³ (figure 10).
Sarcoidosis is the second ILD that may mimic TB. In fact, lesions in the fibrotic form predominate to the upper lungs making distinction with TB sequels sometimes difficult. However, the proximal and peri-bronchovascular distribution of lesions as well as the presence of perilymphatic micronodules help diagnosis. Miliary sarcoidosis is the second presentation that may make the diagnosis confusing³⁶ (figure 11). Moreover, both diseases may be associated. As both diseases may share the same clinical, radiological and immunological features, sarcoidosis should be considered whenever TB is diagnosed and the patient does not improve under adequate and well-conducted treatment⁴⁴.
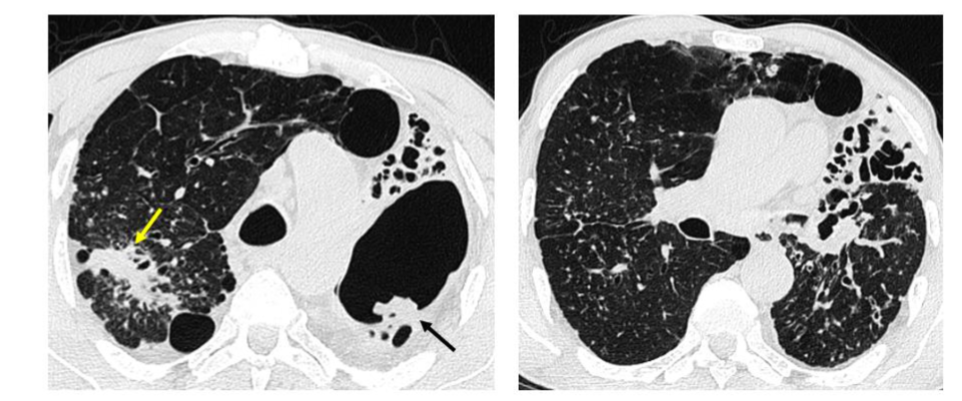
Figure 10: a 70 year-old men with silicotuberculosis. CT shows fibrotic mass of the right upper lobe (yellow arrow) with bilateral perilymphatic micronodules. Sequels of TB are obvious in the left upper lobe with aspergilloma development (black arrow)
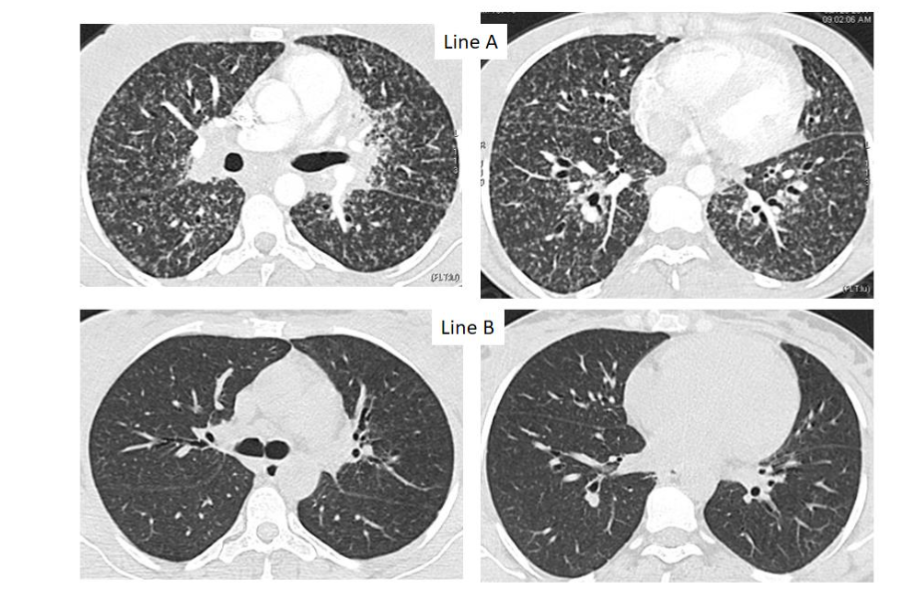
Figure 11: Miliary feature in a 32 year-old woman with mediastinal and hilar enlarged lymph nodes (line A). Bronchial biopsy showed tuberculoid granuloma with tiny necrosis. The patient didn’t improve under anti-tubercular treatment and improved under corticosteroids.
- LUNG CANCER
The association between tuberculosis and cancer is not fortuitous. Chronic inflammation and the process fibrous healing causes metaplasia predisposing to malignant transformation⁴⁵. Two recent meta-analysis demonstrated that TB increases the risk of lung cancer development with an odds ratio of 1.74 and 2.09. This risk is high in the first 2 years after TB and decreases thereafter. It is also higher in young people⁴⁶˒⁴⁷. A relationship has been found between pulmonary tuberculosis and EGFR mutations in patients with lung adenocarcinoma. The diagnosis is difficult due to the existence of sequelae lesions. Occurrence of lung cancer is suggested on CT by the modification of pre-existing lesions, the convexity of their contours, the appearance or existence of pleural extension and bone lysis. When a patient first presents with lung cancer, coexistence of TB is suggested when there is an association of tree-in-bud feature, acinar nodules, cavitary consolidations and nodules in relevant areas⁴⁵.
V. Conclusion
Atypical imaging findings are far to be uncommon in pulmonary TB, which may lead to delay in diagnosis and treatment. CT scan plays an essential role in the diagnosis of these forms that can occur in conditions affecting cell-mediated immunity. Therefore radiologists should be aware of these unusual imaging features to avoid misdiagnosis and to guide bacteriological sampling and, if necessary, biopsies with histological and bacteriological study.
Conflicts of interest:
All authors declare that they have no conflict of interest in relationship with this work.
Acknowledgment:
We would like to thank:
- Mouna Gacem for pathological data gathering through the electronic system of the hospital.
- Hamza Aouididi for data gathering through the PACS of the medical Imaging Department.
References
1. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO
2. WHO consolidated guidelines on tuberculosis. Module 2: screening – systematic screening for tuberculosis disease. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO
3. Kim JH, Kim MJ, Ham SY. Clinical characteristics and chest computed tomography findings of smear-positive and smear-negative pulmonary tuberculosis in hospitalized adult patients. Medicine (Baltimore). 2019;98(34):e16921. doi: 10.1097/MD.0000000000016921.
4. Rana, A., Krishnan, V. & Aggarwal, A. Unusual patterns of tuberculosis on cross-sectional imaging: a pictorial review. Egypt J Radiol Nucl Med. 2022;53:190 doi:10.1186/s43055-022-00875-0
5. Wei S, Shi B, Zhang J, Li N. Differentiating mass-like tuberculosis from lung cancer based on radiomics and CT features. Transl Cancer Res. 2021;10(10):4454-4463. doi: 10.21037/tcr-21-1719.
6. Afriyie-Mensah JS, Awindaogo FR, Asomani SK. Pseudotumour presentation of pulmonary tuberculosis. Ghana Med J. 2020;54(2):126-130. doi: 10.4314/gmj.v54i2.12.
7. Agarwal R, Srinivas R, Aggarwal AN. Parenchymal pseudotumoral tuberculosis: case series and systematic review of literature. Respir Med. 2008;102(3):382-9. doi: 10.1016/j.rmed.2007.10.017.
8. Zayet S, Berriche A, Ammari L, Kanoun F, Kilani B, Benaissa HT. Pseudotumoural pulmonary tuberculosis: a case series. IJID Reg. 2022;2:158-161. doi: 10.1016/j.ijregi.2022.01.009.
9. Xiang Y, Huang C, He Y and Zhang Q (2021) Cancer or Tuberculosis: A Comprehensive Review of the Clinical and Imaging Features in Diagnosis of the Confusing Mass. Front. Oncol. 11:644150. doi: 10.3389/fonc.2021.644150
10. Patro M, Gothi D, Sah RB, et al. An interesting case of incidental solitary pulmonary nodule. Breathe 2018; 14: e128–e133.
11. Mazzone PJ, Lam L. Evaluating the Patient With a Pulmonary Nodule: A Review. JAMA. 2022; 327(3):264-273. doi: 10.1001/jama.2021.24287.
12. Cruickshank A, Stieler G, Ameer F. Evaluation of the solitary pulmonary nodule. Intern Med J. 2019;49(3):306-315. doi: 10.1111/imj.14219.
13. Zhang, J.; Han, T.; Ren, J.; Jin, C.; Zhang, M.; Guo, Y. Discriminating Small-Sized (2 cm or Less), Noncalcified, Solitary Pulmonary Tuberculoma and Solid Lung Adenocarcinoma in Tuberculosis-Endemic Areas. Diagnostics 2021;11:930. doi.org/10.3390/diagnostics11060930
14. Hosaka N, Kameko M, Nishimura H, Hosaka S. Prevalence of tuberculosis in small pulmonary nodules obtained by video-assisted thoracoscopic surgery. Respir Med. 2006;100(2):238-43. doi: 10.1016/j.rmed.2005.05.004.
15. Kaoutar I, Billah NM, Nassar I. Solitary excavated lung nodule revealing pulmonary tuberculosis: A case report. Int J Case Rep Images 2021;12:101248Z01IK2021.
16. Zeng Y, Zhai XL, Wáng YXJ, Gao WW, Hu CM, Lin FS, Chai WS, Wang JY, Shi YL, Zhou XH, Yu HS, Lu XW. Illustration of a number of atypical computed tomography manifestations of active pulmonary tuberculosis. Quant Imaging Med Surg. 2021;11(4):1651-1667. doi: 10.21037/qims-20-1323.
17. Nèji H, Affes M, Attia M, Ben Saad S, Berraies A, Baccouche I, Hantous-Zannad S, Ben Milad-M’rad K. Atypical Pleuropulmonary Tuberculosis Mimicking a Malignant Disease. J Thorac Oncol. 2017;12(9):e145-e147.
doi: 10.1016/j.jtho.2017.05.003.
18. Kim JY, Jeong YJ, Kim KI, Lee IS, Park HK, Kim YD, Seok I H. Miliary tuberculosis: a comparison of CT findings in HIV-seropositive and HIV-seronegative patients. Br J Radiol. 2010;83(987): 206-11. doi: 10.1259/bjr/95169618.
19. Choi D, Lee KS, Suh GY, Kim TS, Kwon OJ, Rhee CH, Han J. Pulmonary tuberculosis presenting as acute respiratory failure: radiologic findings. J Comput Assist Tomogr. 1999;23(1):107-13. doi: 10.1097/00004728-199901000-00023.
20. Jeong YJ, Lee KS. Pulmonary tuberculosis: up-to-date imaging and management. AJR Am J Roentgenol. 2008;191(3):834-44. doi: 10.2214/AJR.07.3896.
21. Jin SM, Lee HJ, Park EA, Lee HY, Lee SM, Yang SC, Yoo CG, Kim YW, Han SK, Shim YS, Yim JJ. Frequency and predictors of miliary tuberculosis in patients with miliary pulmonary nodules in South Korea: a retrospective cohort study. BMC Infect Dis. 2008;8:160. doi: 10.1186/1471-2334-8-160.
22. Giacomelli IL, Schuhmacher Neto R, Nin CS, Cassano PS, Pereira M, Moreira JDS, Nascimento DZ, Hochhegger B. High-resolution computed tomography findings of pulmonary tuberculosis in lung transplant recipients. J Bras Pneumol. 2017;43(4):270-273. doi: 10.1590/S1806-37562016000000306.
23. Tokuyama Y, Matsumoto T, Kusakabe Y, Yamamoto N, Aihara K, Yamaoka S, Mishima M. Ground-glass opacity as a paradoxical reaction in miliary tuberculosis: A case report and review of the literature. IDCases. 2019;19:e00685. doi: 10.1016/j.idcr.2019.e00685.
24. Nattusamy L, Madan K, Bhalla AS, Guleria R. Reversed halo sign in active pulmonary tuberculosis. BMJ Case Rep. 2014;2014:bcr2013202981. doi: 10.1136/bcr-2013-202981.
25. Zhan X, Zhang L, Wang Z, Jin M, Liu M, Tong Z. Reversed Halo Sign: Presents in Different Pulmonary Diseases. PLoS One. 2015;10(6):e01 28153. doi: 10.1371/journal.pone.0128153.
26. Martini K, Loubet A, Bankier A, Bouam S, Morand P, Cassagnes L, Revel MP, Chassagnon G. Nodular reverse halo sign in active pulmonary tuberculosis: A rare CT feature? Diagn Interv Imaging. 2020;101(5):281-287.
doi: 10.1016/j.diii.2020.01.013.
27. Maturu VN, Agarwal R. Reversed halo sign: a systematic review. Respir Care. 2014;59(9):1440-9. doi: 10.4187/respcare.03020.
28. Marchiori E, Zanetti G, Irion KL, Nobre LF, Hochhegger B, Mançano AD, Escuissato DL. Reversed halo sign in active pulmonary tuberculosis: criteria for differentiation from cryptogenic organizing pneumonia. Am J Roentgenol. 2011;197(6):1324-7. doi: 10.2214/AJR.11.6543.
29. Van LD, Le HN, Pletschette M, Nguyen AT, Nguyen TH, Nguyen NBT. Cystic pulmonary tuberculosis: A rare form of an ancient disease. Respirology Case Reports. 2022;10:e01020. doi.org/10.1002/rcr2.1020
30. Perim J, Pimenta ES, Marchiori E. Cystic tuberculosis: a very unusual aspect of a common disease. Pulmonology. 2020;26(6):400-403. doi: 10.1016/j.pulmoe.2019.12.001.
31. Ray A, Suri JC, Sen MK, Khanna A. Cystic lung disease in tuberculosis: An unusual presentation. Lung India. 2013;30(4):351-3. doi: 10.4103/0970-2113.120620.
32. Ray A, Suri JC, Sen MK, Khanna A. Cystic lung disease in tuberculosis: An unusual presentation. Lung India. 2013;30(4):351-3. doi: 10.4103/0970-2113.120620.
33. Cukic V. The Association Between Lung Carcinoma and Tuberculosis. Med Arch. 2017;71 (3):212-214. doi: 10.5455/medarh.2017.71.212-214.
34. Lee HJ, Goo JM, Im JG. Rapid and irreversible cystic change of pulmonary tuberculosis in an immunocompetent adult. J Thorac Imaging. 2003; 18(4):254-6. doi: 10.1097/00005382-200310000-00009.
35. Kodati R, Tadepalli A, Reddy C. Pulmonary tuberculosis presenting as diffuse cystic lung disease: An atypical manifestation. Indian J Tuberc. 2020;67(3):397-399. doi: 10.1016/j.ijtb.2019.11.016.
36. Hantous-Zannad S, Néji H, Affes M, Attia M, Baccouche I, Kechaou S, Tritar F, Ben Miled-M’rad Kh. Imaging of thoracic tuberculosis. In M. F. Ladeb, W. C. G. Peh (eds.), Imaging of Tuberculosis, Medical Radiology Diagnostic Imaging, https://doi.org/10.1007/978-3-031-07040-2_8
37. Jeon KN, Ha JY, Park MJ, Bae K, Baek HJ, Choi BH, Cho SB, Moon JI, Kim HC. Pulmonary Tuberculosis in Patients With Emphysema: Computed Tomography Findings. J Comput Assist Tomogr. 2016;40(6):912-916.
doi: 10.1097/RCT.0000000000000452.
38. Sershen CL, Salim T and May EE (2023), Investigating the comorbidity of COPD and tuberculosis, a computational study. Front. Syst. Biol. 3:940097.doi: 10.3389/fsysb.2023.940097.
39. Ogawa K, Kurosaki A, Miyamoto A, Takahashi Y, Murase K, Hanada S, Uruga H, Takaya H, Morokawa N, Kishi K. Clinicoradiological Features of Pulmonary Tuberculosis with Interstitial Pneumonia. Intern Med. 2019;58(17):2443-2449. doi: 10.2169/internalmedicine.2341-18.
40. Wong C, Sahni S, Cheema MAI, Iftikhar A. Mycobacterium tuberculosis Infection in the Setting of Interstitial Lung Disease: Coincidence or Bad Luck? Cureus. 2018;10(10):e3391.
doi: 10.7759/cureus.3391.
41. Akhter N, Rizvi NA. Interstitial Lung Diseases Misdiagnosed as Tuberculosis. Pak J Med Sci. 2018; 34(2):338-341. doi: 10.12669/pjms.342.14407.
42. Ehrlich R, Akugizibwe P, Siegfried N, Rees D. The association between silica exposure, silicosis and tuberculosis: a systematic review and meta-analysis. BMC Public Health. 2021;21(1):953. doi: 10.1186/s12889-021-10711-1.
43. Lanzafame M, Vento S. Mini-review: Silico-tuberculosis. J Clin Tuberc Other Mycobact Dis. 2021; 23:100218. doi: 10.1016/j.jctube.2021.100218.
44. Pedroso A, Ferreira I, Chikura T. Tuberculosis and Sarcoidosis Overlap: A Clinical Challenge From Diagnosis to Treatment. Cureus. 2020;12(11):e11662. doi: 10.7759/cureus.11662.
45. Hantous-Zannad S, Zidi A, Néji H, Attia M, Baccouche I, Ben Miled-M’rad K. Apport de l’imagerie dans la tuberculose thoracique [The role of imaging in thoracic tuberculosis]. Rev Pneumol Clin. 2015;71(2-3):93-109.
doi: 10.1016/j.pneumo.2014.02.006.
46. Cabrera-Sanchez J, Cuba V, Vega V, Van der Stuyft P, Otero L. Lung cancer occurrence after an episode of tuberculosis: a systematic review and meta-analysis. Eur Respir Rev. 2022;31(165):220025. doi: 10.1183/16000617.0025-2022.
47. Hwang SY, Kim JY, Lee HS, Lee S, Kim D, Kim S, Hyun JH, Shin JI, Lee KH, Han SH, Song YG. Pulmonary Tuberculosis and Risk of Lung Cancer: A Systematic Review and Meta-Analysis. J Clin Med. 2022;11(3):765. doi: 10.3390/jcm11030765.