





Efficacy and Safety of Azithromycin in URTI Treatment
Efficacy, Safety, and Economic Outcomes of Using Azithromycin in Upper Respiratory Tract Infections: A Systematic Literature Review
Dr. MB Bharathi¹, Dr. Susheen Dutt², Dr. Mubarak Khan³, Dr. Jaskaran Singh⁴, Dr. Dinesh Patil⁵, Dr. Darshan Rana⁵, Dr. Onkar Swami⁵*
- JSS Hospital-Medical college, JSS University, Mysore, Karnataka, India.
- Fortis Hospital, Bangalore, Karnataka, India.
- MIMER Medical College, Talegaon, Maharashtra, India.
- Apollo Spectra Hospital, Amritsar, Punjab, India.
- Alembic Pharmaceuticals Ltd. Mumbai, Maharashtra, India.
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Swami, O., Bharathi, MB., et al., 2024.
The Efficacy, Safety, and Economic Outcomes of Using Azithromycin in Upper Respiratory Tract Infections: A Systematic Literature Review.
Medical Research Archives, [online] 12(10).
https://doi.org/10.18103/mra.v12i10.5678
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5678
ISSN 2375-1924
ABSTRACT
Background: Azithromycin is widely used for the treatment of respiratory tract infections (RTIs) due to its broad-spectrum antibacterial activity and preferred safety profile. This study aimed to evaluate efficacy, safety, cost-effectiveness and societal benefits of azithromycin therapy in RTIs.
Methods: An extensive literature search was conducted following PRISMA guidelines. PubMed, Google scholar and Cochrane libraries database was searched for relevant studies published from 1990 to present. The population, intervention, comparator, outcomes, and study design (PICO) framework guided study selection criteria. Published literatures included randomized controlled trials (RCTs), observational studies, and economic evaluations assessing safety, efficacy, and cost outcomes of azithromycin therapy in respiratory tract infections, specifically upper respiratory tract infections. Data extraction and screening were performed by two independent researchers, with discrepancies resolved by a third researcher.
Results: Efficacy evaluation included systematic reviews and meta-analysis comparing azithromycin with other antibiotics. Azithromycin demonstrated superior clinical and comparable efficacy to alternative treatments. Safety analysis indicated that azithromycin had fewer adverse effects, although results varied across studies. Cost-effectiveness analysis revealed that azithromycin was consistently most cost-effective option, with lower direct and indirect costs compared to alternative treatments. Azithromycin’s shorter treatment duration also led to reduced healthcare resource utilization, reduced sickness absenteeism, improved in work and daily activities thereby mitigating overall societal costs.
Conclusion: Azithromycin exhibits a favorable risk-benefit profile in management of Upper RTIs, supported by its superior clinical efficacy, safety, and cost-effectiveness compared to alternative antimicrobials. Its shorter treatment duration contributes to reduced hospitalization periods and societal costs, making it a valuable therapeutic option for upper respiratory tract infections.
Limitations: Limited generalizability.
Key words: Azithromycin, URTI, RTI, Cost-effectiveness, Systematic review, Macrolides, Antibiotics, Economic outcome.
Introduction
Azithromycin is a macrolide antimicrobial, having broad-spectrum activity against gram-negative bacteria and various gram-positive organisms¹. It offers efficient pharmacokinetics and pharmacodynamics properties which can successfully mitigate plethora of infections hence considered to be most utilized antimicrobial drug globally².
Azithromycin’s pharmacokinetics allow it to be effective against intracellular pathogens after it is transported from the bloodstream into tissues and readily crosses cellular membranes¹. Azithromycin has been reported to be effective against “atypical” bacteria such as chlamydiae, mycoplasma, and mycobacteria, some protozoal organisms, community-acquired pneumonia, and has also been used in treatment of pharyngitis caused by Streptococcus pyogenes, etc. Over years it has been used in prophylaxis for advanced acquired immunodeficiency syndrome (AIDS); and various sexually transmitted infections³.
According to a study conducted by Kong F Y et al. after a single 500 mg oral dose administration of azithromycin, minimum tissue concentrations that would inhibit 90% of likely pathogens (MIC90) exceeds, while phagocytic concentrations reaches over 200 times serum concentrations and, these levels can be maintained for a longer period due to its 68 hours half-life⁴.
Upper respiratory tract infection (URTI) is self-limited irritation and swelling of upper airways with associated cough reported with frequent prevalence over the years globally⁵. Upper respiratory tract infection has been associated with various risk factors including smoking, systemic disorders such as allergic rhinitis, immunocompromised individuals, and individuals with anatomical anomalies including facial dysmorphic changes or nasal polyposis.
Azithromycin, because of its favorable effects, affordability, and pleiotropic action, has been used to treat the early inflammatory phase of COVID-19 infection⁶. Other antibiotics used in treatment of URTIs is associated with decrease treatment adherence affecting compliance to treatment, this might be due to longer treatment duration along with increased frequency of dosing as compared to Azithromycin⁷. Also, this antibiotic are less tolerated because of side effects such as diarrhea, rash, etc, these side effects, like diarrhea, later require add on treatment with probiotics, which overall adds to the total cost of treating URTIs⁸.
With increasing challenges of antibiotic resistance and need for efficient resource allocation in healthcare, understanding Azithromycin impact on clinical outcomes and healthcare costs specific to upper and lower respiratory tract infections is essential. By identifying key drivers of cost-effectiveness, such as reduced treatment duration and favorable safety profile, this study seeks to provide practical insights for optimizing RTI management and guiding antibiotic prescribing practices in clinical settings. The objective of current study is to evaluate efficacy, safety, and cost-effectiveness and societal benefits of using Azithromycin in both Upper and Lower Respiratory Tract Infections, thus filling a critical gap in evidence-based antibiotic selection for Upper and Lower Respiratory Tract Infections.
Methodology
This study was conducted following PRISMA guidelines for systemic review and meta-analysis to generate high-level evidences for our study objective.
DATA SOURCE:
An extensive literature search of published studies from year 1990 to till date, was conducted using PubMed database, which included randomized controlled trials (RCTs), observational studies, and economic evaluations, to gather relevant data on safety, efficacy and cost outcome of azithromycin therapy on respiratory tract infection.
The search string for literature search included Azithromycin” [MeSH Terms] OR “Azithromycin” [Title/Abstract] AND (“Safety” [MeSH Terms] OR “Safety” [Title/Abstract] OR “Adverse Effects” [MeSH Terms] OR “Adverse Effects” [Title/Abstract] OR “Side Effects” [Title/Abstract] OR “Comparison” [Title/Abstract] AND (“Antibiotics” [MeSH Terms] OR “Antibiotics” [Title/Abstract])
During literature search, eligibility criteria was set based on population, intervention, comparators, outcomes, and study design (PICO) framework.
- “Population”: all patients with any form upper Respiratory tract Infections
- “intervention”: Azithromycin therapy
- “comparator”: other antimicrobial drugs
- “outcomes” were efficacy (improvement in symptoms of RTI, number of infusions needed to bring about improvement) safety and tolerability in terms of adverse events (AEs), treatment withdrawals and mortality, patient-reported outcomes and economic outcomes.
Studies of those, including patients without RTI, not meeting our pre-determined PICO criteria, at pre-clinical stage or those involving animal were excluded.
The literature search and screening were conducted by two researchers independently from Pubmed, Google and Cochrane data base using predetermined search string following same inclusion and exclusion criteria, articles appearing after search string were screened over three stages, initially all articles were screened based on title, followed by abstracts screening and lastly full text screening of selected articles was done by two researchers independently, and further any disagreement, was resolved by intervening third independent researchers. All data after being reviewed were entered in Microsoft Excel (Microsoft Corporation, Redmond, WA), and were subjected to further analysis to meet objectives of present study.
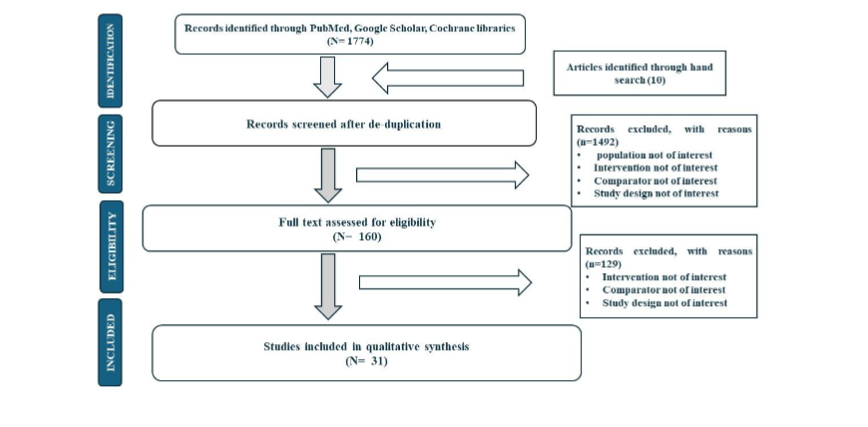
For Study selection flow Chart refer Figure 1
Further, for critical appraisal, we utilized the Oxford Centre for Evidence-based Medicine criteria to assign levels of evidence to studies included in this review. Each study was categorized based on its type and design, as specified in Table 1. This approach allowed for a systematic assessment of the quality and strength of evidence across reviewed literature. (Refer table 1: Evidence level criteria)
Table 1:
| Evidence level | Study type |
|---|---|
| 1 | A systematic review of randomized trials or n-of-1 trials |
| 2 | Randomized trial or observational study with dramatic effect |
| 3 | Nonrandomized controlled cohort / follow-up study |
| 4 | Case-series, case-control studies, or historically controlled studies |
| 5 | Mechanism-based reasoning |
Result:
Out of 1774 articles identified, 160 articles provided eligible following full-text review. For data analysis, the present study included articles of various study designs including 19 Randomized clinical trials, 5 Systematic reviews, 1 Narrative review, and 3 meta-analyses, and 3 studies were reported to be observational studies.
Further, of all study designs, clinical efficacy of Azithromycin was assessed in 14 studies, safety in 9 studies, and its cost-effectiveness was reported only in 9 studies.
1. CLINICAL EFFICACY
A systematic review by Davidson RJ et al. on patients with respiratory tract infections, reported that in treatment of acute bacterial maxillary sinusitis, azithromycin has similar clinical cure rate, compared to amoxicillin and also that long half-life of azithromycin allows for prolonged concentrations, which may be beneficial in treating certain infections⁹.
Li et al. in their study among 256 children with Group A beta-hemolytic streptococcus (GAS) tonsillitis reported that 96.4% of patients in azithromycin group, 92.4% of patients in cefaclor group, and 91.0% of patients in amoxicillin group were recorded as clinical success at the end of therapy. Further, bacteriological eradication rates of 3 groups at the end of therapy were 94.0%, 89.9%, and 88.5%, respectively. At follow-up, pathogen recurrence rate was evaluated as 2.6%, 7.0%, and 5.9% respectively. However, differences were reported to be statistically insignificant. Further, Azithromycin having shorter treatment duration as compared to Cefaclor and Amoxicillin adds to advantage¹⁰.
Similarly, Dawit et al. in Systematic review and meta-analysis found that difference in clinical efficacy after completion of treatment was statistically insignificant among azithromycin and amoxicillin/clavulanate group. Further, efficacy assessment on long term follow-up between 3 and 5 weeks, clinical and bacteriological efficacies were comparable with no statistically significant difference¹¹.
El Hennawi et al., in RCT among 284 patients with recurrent streptococcal tonsillitis, reported statistically significant improvement in symptoms intensity among both benzathine penicillin and azithromycin groups from before treatment to end of six-month follow-up (p = 0.03). However, two groups had no statistically significant difference¹².
Amali et al. in their study among patients with chronic rhinosinusitis reported that azithromycin group, post Sino-Nasal Outcome Test (SNOT-22) questionnaire survey showed an 80% change after treatment, whereas placebo group showed 68% change. The improvement in SNOT-22 scores after treatment and percentage change were statistically significant in azithromycin group compared with control group after 3 months of therapy (p <0.05)¹³.
Donde et al. in their non-interventional study, reported that azithromycin had significantly higher clinical success rates (98.92%) compared to typical antibiotic treatments like amoxicillin (85-87%) and it was reported that azithromycin treatment was as effective as other antibiotics¹⁴.
Lakos et al. in a multicenter, non-comparative study conducted among 156 children suffering from respiratory tract infections reported relief of symptoms within 3 days of azithromycin therapy among 89.1% of patients. The clinical effectiveness of azithromycin was further reported to be 94.8% across all respiratory tract infections studied¹⁵.
Gulani et al. in their systematic review, including 35 RCTs, reported no evidence regarding treatment failure risk with short-course azithromycin compared to longer antibiotic courses (RR=0.93, 95% CI0.79-1.09). They further reported that azithromycin use in short course and compliance monitoring emerged as significant predictors of lower risk of treatment failure in meta-regression analysis¹⁶.
Altunaji et al. in their review including 12 RCTs with 1720 patients reported that short-term antibiotics such as azithromycin was equally effective with long-term antibiotic treatment (erythromycin estolate or erythromycin for 14 days) in microbiological eradication of Bordetella pertussis (B. pertussis) from nasopharynx. The relative risk (RR) was 1.02 (95% confidence interval (CI) 0.98 to 1.05). Side effects were fewer with short-term treatment (RR 0.66; 95% CI 0.52 to 0.83)¹⁷.
Murray et al. in their RCT based on acute bacterial sinusitis among 541 patients reported that azithromycin provided high clinical cure rates of 97.3%, 96.3%, and 100% against key pathogens Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis respectively and found that single-dose azithromycin microspheres provided clinical and bacteriologic efficacy and safety comparable to 10 days of levofloxacin¹⁸.
Oguz et al. in their RCT among 330 child patients of Acute Otitis media, found no significant differences in cure rates between azithromycin therapy and cefaclor therapy. Further, it was stated that compliance is likely better with azithromycin regimen compared to of cefaclor. The shorter duration of therapy with azithromycin may help prevent premature discontinuation of antibiotics¹⁹.
Lildholdt et al. in their study found that 32 (60%) of patients treated with azithromycin did not have recurrence of acute pharyngotonsillitis (RAPT) compared to 29 (51%) in placebo group (RR = 0.81, CI95 0.53–1.23, p = 0.32), however difference was not reported to be statistically significant²⁰.
John AP Ioannidis et al. in their RCT based on URTI among 45 patients, reported that azithromycin had similar clinical failure rates to other antibiotics for acute otitis media (19 comparisons, 3421 patients), acute sinusitis (11 comparisons, 1742 patients), and acute pharyngitis (16 comparisons, 2447 patients). The differences were small, and statistically insignificant with none of the 95% confidence intervals exceeding 2%. The study further reported that 3-5 day azithromycin regimen is more convenient than typically longer 7-14 day courses of comparator antibiotics²¹.
Guay D R P et al. in their review regarding beta-hemolytic streptococcal (GABHS) tonsillopharyngitis, acute (suppurative) otitis media, and acute sinusitis reported that 5-day course of azithromycin (10 mg/kg once daily on all 5 days in pediatric patients) is as or more effective than 10-day course of penicillin. However, it was further reported that 3-day regimen of azithromycin (10 mg/kg on all 3 days in pediatric patients) generally produces low clinical (80% in 2/4 studies) and bacteriologic (<80% in 3/4 studies at end of therapy and 2/3 studies at long-term follow-up) efficacy²².
O Muller et al. in RCT conducted among 380 adult upper respiratory tract infection patients reported that short course of azithromycin had similar efficacy and safety compared to long course of clarithromycin for treating upper respiratory tract infections. The overall clinical efficacy was similar between azithromycin (95%) and clarithromycin (96%) and difference was reported to be non-significant²³.
Further, similar results have been reported regarding efficacy of azithromycin against Lower respiratory tract infections as well:
Aldahhri et al. in their retrospective cohort study among 197 patients with severe CAP reported that azithromycin has significantly higher clinical cure rate as compared to clarithromycin group (97.3% vs. 84.8% and p<0.0009) and was reported with shorter length of hospital stay as compared to clarithromycin group (6.5 days vs. 8 days). Further, no ICU admissions and no mortality were reported in azithromycin group whereas 4.5% of patients were reported with ICU admissions and 3% mortality was reported in clarithromycin group²⁴.
Salloum et al. in their systematic review, including 7 clinical trials, among patients diagnosed with community-acquired pneumonia (CAP), treatment success rate after azithromycin–beta-lactam administration for 10 to 14 days was reported to be 87.55% and that for clarithromycin–beta-lactam after 5 to 7 days of therapy was 75.42%²⁵.
Kawamura et al. conducted cohort study based on acute exacerbation of chronic fibrosing interstitial pneumonia, including 76 patients. The study reported that use of azithromycin was associated with significantly longer survival time (HR 0.22, 95% CI 0.08–0.61, p=0.004) compared to fluoroquinolone treatment, and difference was reported to be statistically significant. Further, Propensity score-adjusted analysis also showed azithromycin use was associated with longer survival (HR 0.17, 95% CI 0.05-0.61)²⁶.
Beigelman A et al. in their randomized, double-masked, placebo-controlled proof-of-concept trial reported that compared with placebo, azithromycin treatment did not reduce serum IL-8 levels at day 8 (P=0.6) but resulted in greater decrease in nasal lavage fluid IL-8 levels by day 15 (P=0.03) among infants with recurrent wheezing in infants with respiratory syncytial virus bronchiolitis. It was further reported that Azithromycin treatment resulted in prolonged time to third wheezing episode (P=0.048) and in fewer days with respiratory symptoms over subsequent year in comparison with placebo (36.7 vs. 70.1 days, P=0.01)²⁷.
Smith et al. in their systematic review including 11 RCTs and total of 473 neonates, reported significant reduction in bronchopulmonary dysplasia (BPD) risk in extremely premature infants undergoing azithromycin therapy (RR=0.83, 95% CI 0.71 to 0.98, p=0.02) and findings were reported to be statistically significant²⁸.
Joseph D’Ignazio et al., in their Randomized clinical trial, reported that single 2.0g oral dose of azithromycin microspheres was as effective as 7-day course of levofloxacin (500mg daily) for treatment of mild to moderate CAP in adults. Further, compliance was reported to be 100% in azithromycin group since it was single dose, compared to 95.3% in 7-day levofloxacin group²⁹.
Albert RK et al. in their study among 1577 subjects with COPD reported that median time to first exacerbation of COPD was 266 days among participants receiving azithromycin, as compared to 174 days among participants receiving placebo (P<0.001). The frequency of exacerbations was 1.48 exacerbations per patient-year in azithromycin group, as compared with 1.83 per patient-year in placebo group (P = 0.01), and hazard ratio for having an acute exacerbation of COPD per patient-year in azithromycin group was 0.73 (P<0.001)³⁰.
Sternon et al, study among 134 patients reported that both azithromycin (and clarithromycin showed equivalent clinical efficacy in treating acute purulent tracheobronchitis. However, the median time to improvement of symptoms was significantly shorter for azithromycin patients (3 days) compared to clarithromycin patients (4 days) (P = 0.014)³¹.
2. SAFETY
Sun et al. in their meta-analysis, which included 14 RCTs reported that overall incidence of adverse reactions among patients treated with azithromycin was 24.20%, compared to 48.05% in patients treated with other antibiotics or other treatments than AZM³¹.
Li et al. found that among patients with Group A beta-hemolytic streptococcus (GAS) treatment-stimulated adverse events occurred in 2.4% of patients in azithromycin group, 11.3% in cefaclor group, and 11.4% in amoxicillin group¹⁰.
Gabriel Dawit et al. in their systematic review and meta-analysis in 2018 stated that azithromycin was found to be safer and more tolerable than amoxicillin/clavulanate, with fewer adverse events reported¹¹.
El Hennawi et al. found that among recurrent tonsillitis patients treated with azithromycin, three patients had minor adverse reactions e.g. nausea, vomiting, and abdominal cramps with diarrhea associated with recurrent streptococcal tonsillitis. It was further reported that satisfaction among azithromycin group patients was significantly higher among 58 patients (95.61%). Only three reported to be uncomfortable (4.9%). It is evident that Azithromycin was better tolerated than Benzathine Penicillin, with statistically significant difference between both groups regarding satisfaction¹².
Shantanu Donde et al. in their non-interventional study reported Azithromycin with fewer rates of adverse events (3.9%)¹⁴.
Albert RK et al. discussed that rate of death from any cause was 3% in azithromycin group and lesser than 4% in placebo group, although difference was statistically insignificant³⁰.
Gulani et al. reported in their systematic review that the risk of adverse effects, especially diarrhea and rash, was significantly lower with azithromycin use compared to other antibiotics, resulting in better compliance with azithromycin therapy¹⁶.
Smith et al., based on their systematic review, which included 11 RCTs and 473 neonates, found that azithromycin had a better safety profile compared to erythromycin, with a lower incidence of diarrhea, abdominal discomfort, and reduced appetite²⁸.
Murray et al. in their RCT stated that azithromycin microspheres were well tolerated with mostly mild to moderate gastrointestinal side effects and only one treatment-related discontinuation¹⁸.
Oguz et al. in their RCT among 330 Pediatric patients of acute otitis media with azithromycin and cefaclor groups reported that single patient from each group had side effects that included vomiting and diarrhea with no statistically significant difference¹⁹.
D’Ignazio et al., in their randomized double-blind, noninferiority study among patients with LRTI, including mild to moderate CAP, stated that the single-dose azithromycin microsphere regimen was well tolerated with mainly mild gastrointestinal side effects²⁹.
3. ECONOMIC CONSIDERATIONS:
a) Cost-effectiveness:
Donde et al. reported that azithromycin treatment costs an average of INR 716 per patient compared to INR 780-844 for amoxicillin, making it more cost-effective option for treatment of acute bacterial upper RTIs¹⁴.
Parmar et al., in their observational study in 2007, reported that azithromycin could be suitable substitute for amoxicillin in treatment of upper respiratory tract infections (URTI) and that use of azithromycin instead of amoxicillin can lead to cost savings for primary health centers (PHCs) with lesser number of dosages required³².
Lavoie et al., in their study including LRTI patients, reported that cost of treatment episode is significantly lower with azithromycin, with an average of $10.87 lower compared to other treatments. Further, azithromycin’s cost is $28.91 per treatment episode, while clarithromycin costs $34.32, ciprofloxacin costs $47.39, and other second-line antibiotics cost $37.62³³.
Samsa et al. in their RCT including 163 patients and reported that over a period of 30-day follow-up, total direct medical costs of azithromycin group were $2,481 less per patient compared to levofloxacin group, and findings were reported to be statistically significant. The difference was mainly due to shorter length of hospital stay for azithromycin group (7.0 days for azithromycin vs 8.8 days for levofloxacin). Further, it was stated that post-discharge resource utilization was lower for azithromycin group, leading to an estimated $233 per patient savings in post-hospitalization costs³⁴.
Rahav et al. among 123 CAP patients, reported, the total cost per 100 patients was $28,224 for azithromycin group vs $54,590 for comparison group treated with erythromycin, amoxicillin-clavulanate, roxithromycin, cefuroxime axetil, amoxicillin, doxycycline, cefaclor³⁵.
Paladino et al. in their study based on cost-effectiveness analysis of IV-to-oral regimens of azithromycin vs cefuroxime with or without erythromycin for CAP patients, it was reported that, as empiric therapy, azithromycin monotherapy (5265$ per expected cure) was cost-effective compared to cefuroxime (6145$)³⁴.
McCarty et al. in their review, reported that in treating indicated respiratory tract and skin and skin structure infections, 5-day azithromycin therapy has lowest cost per treatment of any branded antibiotic³⁶.
Morimoto et al. compared cost-effectiveness of amoxicillin/clavulanate, azithromycin, clarithromycin, cefdinir, levofloxacin, and minocycline, when used on an ambulatory basis for management of adult patients with community-acquired pneumonia and it was reported that azithromycin was most beneficial when number of times antibiotics are taken in a day and period of therapy were taken into account³⁷.
b) Hospitalization cost:
Carbon et al. in their study including 262 pharyngitis patients, reported that total costs over 4 weeks were lower for 3-day azithromycin ($193.60 per patient) and 5-day azithromycin ($195.30) compared to 10-day roxithromycin ($202.10)³⁸.
c) Indirect cost:
Sternon et al. among 134 patients, reported that mean indirect costs due to lost productivity were estimated at 15,913 BFr (~$438 USD) per bronchitis episode for all groups combined. Indirect costs accounted for over 85% of total costs. Further, direct medical costs (services, medications excluding antibiotics) were comparable between azithromycin (47,579 BFr) and clarithromycin groups (53,556 BFr)³⁹.
d) Quality of life:
Morimoto et al. reported that in terms of frequency of antibiotics taken in a day and period of therapy, azithromycin was reported to be beneficial with 917,179-1,152,694 yen (US$ 7,643-9,606) per additional Quality-adjusted life year (QALY) over minocycline in patients without comorbidity. Azithromycin provides a higher quality of life for adults without comorbidity with generally acceptable marginal cost³⁷.
Discussion:
Upper respiratory tract infections typically involve direct invasion of upper airway mucosa by an organism that is acquired through inhalation of infected droplets. When treating patients with upper respiratory tract infections using antibiotics, important factors to consider are the antibacterial activity of medication, its tolerability profile, and required treatment duration. At the same time, LRTI is a broad terminology that includes acute bronchitis, pneumonia, acute exacerbations of chronic obstructive pulmonary disease/chronic bronchitis (AECB), and acute exacerbation of bronchiectasis. Beta-lactam antibiotics, macrolides, and fluoroquinolones are routinely prescribed medicines for managing LRTIs. Further, macrolides are time-tested and effective agents for the treatment of LRTIs⁴⁰.
Azithromycin, an azalide macrolide antibiotic, has been approved worldwide across around 100 countries for the treatment of a variety of community-acquired infections. These infections include those of the upper respiratory tract, genitourinary tract, skin, and skin structures, such as group A streptococci, S. pneumoniae, H. influenzae, and M. catarrhalis, with good safety profiles³². As per Gotfried MH et al., macrolides, a class of antibiotics to which azithromycin belongs, can improve sinusitis symptoms by increasing mucociliary clearance, decreasing nasal secretions, and reducing polyp size. Moreover, they have been found to change the inflammatory response associated with chronic sinusitis, and it was implied that previous clinical studies demonstrated.
Apart from the broad spectrum anti-microbial activities, the drug has large distribution volume of approximately 23 L/kg of body weight and long half-life of 68–79 h. Azithromycin 0.5 g has 50 times more tissue concentration as compared to plasma for up to 96 h after administration of single oral dose. These features contribute to its sustained efficacy and therapeutic potential, ensuring prolonged drug action and enhanced tissue distribution, particularly in infection sites where adequate drug levels are critical for optimal outcomes³⁹˒⁴¹. The shorter treatment duration of azithromycin promotes treatment adherence and enhances patient compliance. The convenience of shorter therapeutic regimens, typically 3–5 days for select indications, mitigates treatment burden on patients and healthcare providers while ensuring optimal pharmacotherapeutic outcomes⁴⁰.
Clinical evidence consistently validates azithromycin’s efficacy and tolerability across diverse patient demographics, thereby establishing azithromycin as a cornerstone therapeutic option in URTI management, such as acute bacterial sinusitis, otitis media, and pharyngitis, as preferred empirical therapy¹⁴.
1. CLINICAL EFFICACY
For efficacy evaluation, present study included 6 systematic reviews and one meta-analysis that assessed clinical efficacy of azithromycin with other antibiotics. Azithromycin exhibits variable efficacy compared to other antibiotics. Some studies suggest superiority over specific antibiotics like clarithromycin and beta-lactam, while others indicate similar efficacy to amoxicillin and clavulanate. The systematic review Studies like Salloum et al. and Gulani et al. indicated that azithromycin outperforms specific antibiotics such as clarithromycin and beta-lactam¹⁶˒²⁵˒²⁸. However, these results were in contrast with the previous systematic review, which reported that azithromycin had clinical efficacy similar to amoxicillin and clavulanate⁹˒¹¹˒²². Furthermore, all the cohorts and non-comparative studies included in the present review reported the superiority of azithromycin in clinical efficacy when compared to any other antibiotics¹⁴˒¹⁵˒²⁴˒²⁶.
The RCT conducted by Murray et al. reported that azithromycin had better clinical efficacy as compared to levofloxacin in URTI; results were similar to the previously reported studies reporting the clinical efficacy of azithromycin similar to other antibiotics¹³˒¹⁷–²¹˒²⁹. Albert RK et al. reported that among patients with chronic obstructive pulmonary disease (COPD), life-table analysis showed that risk of acute exacerbations of COPD was reduced among participants receiving azithromycin³⁰.
2. SAFETY
Antibiotics represent the cornerstone in addressing mild to severe and, in some cases, potentially life-threatening infections. Concurrently, their administration is associated with potential for adverse effects, necessitating prudent use to diminish these concerns. The systematic review by Gabriel Dawit et al., reported azithromycin to be safer than amoxicillin clavulanate, and results similar to studies conducted by Gulani et al., Sun et al. and Smith et al., reporting azithromycin to be safer than other antibiotics including erythromycin with fewer adverse effects¹¹˒²⁸˒³¹.
Oguz et al. found no significant difference in adverse effects or relapse rate between azithromycin and cefaclor for otitis media. Similarly, Albert RK et al. reported comparable safety between azithromycin and placebo in COPD patients. This contrasts with other RCTs in study (El Hennawi et al., Murray et al., Joseph D’ Lgnazio et al.) which found azithromycin to be safer and better tolerated than other antibiotics¹²˒¹⁸˒¹⁹˒²⁹˒³⁰.
Since most frequently observed adverse effect of antibiotics was reported to be gastrointestinal, G. Treadway et al. observed lower level of adverse effects associated with azithromycin and discussed presence of 15-membered lactone ring as reason for reduced stimulation of gastrointestinal motility in azithromycin, compared with other antibiotics⁴².
3. COST-EFFECTIVENESS
Among all nine studies that involved cost analysis of azithromycin included in the present review, azithromycin was reported to be the most cost-effective option compared to other antibiotics. Previous studies consistently highlight the economic advantages of azithromycin over alternatives like amoxicillin, cefuroxime, and levofloxacin¹¹˒²⁹˒³⁵, irrespective of their study design. Rahav et al. and Sternon et al. reported that the total time the patients were unable to work due to illness was shorter than those treated with azithromycin; hence, indirect costs due to lost productivity would be lower in the azithromycin group. Further, Rahav et al. discussed that the direct treatment cost covered by insurance per 100 patients was lower for the azithromycin group compared to the comparison group. For an indirect comparison, it was found that the cost of absentee workdays per 100 patients for the azithromycin group was almost half as compared to other antibiotic-treated groups, and azithromycin therapy saved insurers $7,238 per 100 patients and the general economy $26,366 per 100 patients compared to other antibiotics³⁵˒³⁹.
Carbon et al. found that azithromycin was associated with faster symptom resolution and incremental cost savings due to lower antibiotic costs and reduced absenteeism costs. Further, Samsa et al. also found better cost-effectiveness among azithromycin, which was mainly due to shorter length of hospital and lower post-discharge resource utilization leading to savings in overall post-hospitalization costs³⁴˒³⁸.
reported that patients on once-daily (OD) antibiotic therapy as of azithromycin show approximately 22% higher compliance as compared to those on multiple daily regimens. Low compliance with latter is due to longer treatment durations leading to treatment failure and increased healthcare costs⁴⁶.
And allows savings in overall post-hospitalization costs³⁴˒³⁸.
Risk benefit analysis
• Scientific evidence supports the favorable risk-benefit profile of azithromycin in the management of respiratory tract infections. Its superior clinical efficacy, evidenced by enhanced symptom resolution and reduced recurrence rates compared to alternative treatments, underscores its therapeutic value.
• While mild to moderate adverse outcomes may occur infrequently, severe adverse events are exceedingly rare, as indicated by comprehensive clinical trials and pharmacovigilance data.
• Furthermore, azithromycin’s shorter treatment duration minimizes hospitalization periods, leading to reduced healthcare resource utilization and associated costs.
• Its cost-effectiveness, coupled with a lower recurrence rate, further solidifies its position as a scientifically sound therapeutic option for respiratory tract infections. It offers substantial benefits while maintaining a favorable risk profile.
Societal impact:
• Azithromycin’s shorter treatment duration than alternative antibiotics contributes significantly to its societal impact.
• The reduced duration of treatment translates to lower medication costs for both patients and healthcare systems, easing financial burdens and optimizing resource allocation.
• Moreover, shorter treatment regimens with azithromycin lead to decreased hospital stays, freeing up beds for other patients and reducing strain on hospital personnel.
• Additionally, fewer days spent in the hospital due to azithromycin therapy result in reduced absenteeism among individuals, minimizing disruptions in work and daily activities.
• Altogether, these factors underscore azithromycin’s role in enhancing resource allocation within healthcare systems while mitigating societal costs associated with URTI management.
Limitations:
Literature regarding the cost-effectiveness of azithromycin in the treatment of URTI is scarce.
Conclusion:
The present (HEOR) analysis found that azithromycin demonstrates a comparable or superior clinical efficacy in treating Upper Respiratory Tract Infections (URTIs) while maintaining an equivalent safety profile as other antibiotics. Further, the evident advantage lies in its cost-effectiveness, particularly in evaluations encompassing in-hospital and post-hospitalization expenses, making the drug a preferred therapeutic option among clinicians for managing URTIs.
Contributions:
This manuscript represents the collaborative efforts of 7 authors, each contributing significantly to its development. The outlined contributions of each author are as follows:
- DR. Onkar Swami: Concept and design, Acquisition of data, Drafting of the manuscript, Critical revision of the manuscript, Administration, technical and material support.
- DR. MB Bharathi: Conceptualization, methodology, and review of the original draft.
- DR. Susheen Dutt: Concept and design, Systemic review of the data, Critical review of the manuscript for intellectual content.
- DR. Mubarak Khan: Concept and design, Systemic review of the data, Critical review of the manuscript for intellectual content.
- DR. Jaskaran Singh: Concept and design, Systemic review of the data, Critical review of the manuscript for intellectual content.
- DR. Dinesh Patil: Acquisition of data, Drafting of the manuscript, and Critical revision of the manuscript for important intellectual content.
- DR. Darshan Rana: Acquisition of data, Drafting of the manuscript, and Critical revision of the manuscript for important intellectual content.
Declarations:
• Ethics Compliance: This is a review article hence does not require EC approval
• Conflict of interest
Dr. Dinesh Patil, Dr. Darshan Rana and Dr. Onkar Swami are full time employees of the Alembic Pharma Ltd which actively markets Azithromycin.
Acknowledgments:
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work and have given final approval for the version to be published.
Funding declaration:
Funding for medical writing support was provided Alembic Pharmaceuticals Ltd.
• Medical Writing assistance:
The authors thank Dr. Punit Srivastava of Mediception Science Pvt. Ltd (www.mediception.com) for providing medical writing support in the preparation of this publication.
References
1. Goldman RC, Fesik SW, Doran CC. Role of protonated and neutral forms of macrolides in binding to ribosomes from gram-positive and gram-negative bacteria. Antimicrob Agents Chemother. 1990;34(3):426-431. doi:10.1128/AAC.34.3.426
2. Alvear G, Santibáñez L, Sepúlveda R, Ramírez V, Martínez B. [Prescription of antibiotics in acute respiratory infections non-pneumonia in a private outpatient practice]. Rev Med Chil. 2022;150(8):10 00-1009. doi:10.4067/S0034-98872022000801000
3. Sandman Z, Iqbal OA. Azithromycin. In: StatPearls. StatPearls Publishing; 2024. Accessed March 4, 2024. http://www.ncbi.nlm.nih.gov/books/NBK557766/
4. Kong FYS, Rupasinghe TW, Simpson JA, et al. Pharmacokinetics of a single 1g dose of azithromycin in rectal tissue in men. PLoS One. 2017;12(3):e0174372. doi:10.1371/journal.pone.0174372
5. Wenzel RP, Fowler AA. Clinical practice. Acute bronchitis. N Engl J Med. 2006;355(20):2125-2130. doi:10.1056/NEJMcp061493
6. Gyselinck I, Janssens W, Verhamme P, Vos R. Rationale for azithromycin in COVID-19: an overview of existing evidence. BMJ Open Respir Res. 2021 ;8(1):e000806. doi:10.1136/bmjresp-2020-000806
7. Klapan I, Culig J, Oresković K, Matrapazovski M, Radosević S. Azithromycin versus amoxicillin/ clavulanate in the treatment of acute sinusitis. Am J Otolaryngol. 1999;20(1):7-11. doi:10.1016/s0196 -0709(99)90044-3
8. Henry DC, Riffer E, Sokol WN, Chaudry NI, Swanson RN. Randomized double-blind study comparing 3- and 6-day regimens of azithromycin with a 10-day amoxicillin-clavulanate regimen for treatment of acute bacterial sinusitis. Antimicrob Agents Chemother. 2003;47(9):2770-2774. doi:10. 1128/AAC.47.9.2770-2774.2003
9. Davidson RJ.
In vitro activity and pharmacodynamic/pharmacokinetic parameters of clarithromycin and azithromycin: why they matter in the treatment of respiratory tract infections. IDR. 2019;12:585-596. doi:10.2147/IDR.S187226
10. Li P, Jiang G, Shen X. Evaluation of 3-day azithromycin or 5-day cefaclor in comparison with 10-day amoxicillin for treatment of tonsillitis in children. Can J Physiol Pharmacol. 2019;97(10):939 -944. doi:10.1139/cjpp-2019-0087
11. Dawit G, Mequanent S, Makonnen E. Efficacy and safety of azithromycin and amoxicillin/ clavulanate for otitis media in children: a systematic review and meta-analysis of randomized controlled trials. Annals of Clinical Microbiology and Antimicrobials. 2021;20(1):28. doi:10.1186/s12941-021-00434-x
12. El Hennawi DED, Geneid A, Zaher S, Ahmed MR. Management of recurrent tonsillitis in children. Am J Otolaryngol. 2017;38(4):371-374. doi:10.101 6/j.amjoto.2017.03.001
13. Amali A, Saedi B, Rahavi-Ezabadi S, Ghazavi H, Hassanpoor N. Long-term postoperative azithromycin in patients with chronic rhinosinusitis: A randomized clinical trial. Am J Rhinol Allergy. 2015;29(6):421-424. doi:10.2500/ajra.2015.29.4244
14. Donde S, Mishra A, Kochhar P. Azithromycin in Acute Bacterial Upper Respiratory Tract Infections: An Indian Non-Interventional Study. Indian J Otolaryngol Head Neck Surg. 2014;66(Suppl 1):225-230. doi:10.1007/s12070-011-0437-x
15. Lakoš AK, Pangerčić A, Gašparić M, Kukuruzović MM, Kovačić D, Baršić B. Safety and effectiveness of azithromycin in the treatment of respiratory infections in children. Current Medical Research and Opinion. 2012;28(1):155-162. doi:10. 1185/03007995.2011.639355
16. Gulani A, Sachdev HPS, Qazi SA. Efficacy of short course (<4 days) of antibiotics for treatment of acute otitis media in children: A systematic review of randomized controlled trials. Indian Pediatr. 2010;47(1):74-87. doi:10.1007/s13312-010-0010-9
17. Altunaiji S, Kukuruzovic R, Curtis N, Massie J. Antibiotics for whooping cough (pertussis). Cochrane Database Syst Rev. 2005;(1):CD004404. doi:10.1002/14651858.CD004404.pub2
18. Murray JJ, Emparanza P, Lesinskas E, Tawadrous M, Breen JD. Efficacy and Safety of a Novel, Single‐dose Azithromycin Microsphere Formulation Versus 10 Days of Levofloxacin for the Treatment of Acute Bacterial Sinusitis in Adults. Otolaryngol–head neck surg. 2005;133(2):194-200. doi:10.1016/j.otohns.2005.04.020
19. Oğuz F, Ünüvar E, Süoğlu Y, et al. Etiology of acute otitis media in childhood and evaluation of two different protocols of antibiotic therapy: 10 days cefaclor vs. 3 days azitromycin. International Journal of Pediatric Otorhinolaryngology. 2003;67( 1):43-51. doi:10.1016/S0165-5876(02)00360-9
20. Lildholdt T, Doessing H, Lyster M, Outzen KE. The natural history of recurrent acute tonsillitis and a clinical trial of azithromycin for antibiotic prophylaxis. Clin Otolaryngol. 2003;28(4):371-373. doi:10.1046/j.1365-2273.2003.00728.x
21. Ioannidis JPA. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for upper respiratory tract infections. Journal of Antimicrobial Chemotherapy. 2001;48(5):677-689. doi:10.1093/jac/48.5.677
22. Guay DRP. Short-course antimicrobial therapy for upper respiratory tract infections. Clinical Therapeutics. 2000;22(6):673-684. doi:10.1016/S0 149-2918(00)90003-1
23. Müller O. Comparison of azithromycin versus clarithromycin in the treatment of patients with upper respiratory tract infections. J Antimicrob Chemother. 1993;31 Suppl E:137-146. doi:10.1093 /jac/31.suppl_e.137
24. Aldhahri RK, Gabb SG, Shoaib OA, Almadani RM, Eljaaly K, Thabit AK. Doxycycline vs. macrolides in combination with a β-lactam antibiotic for the treatment of community-acquired pneumonia in inpatients. Eur J Med Res. 2022; 27(1):279. doi:10.1186/s40001-022-00912-8
25. Al-Salloum J, Gillani SW, Mahmood RK, Gulam SM. Comparative efficacy of azithromycin versus clarithromycin in combination with beta-lactams to treat community-acquired pneumonia in hospitalized patients: a systematic review. J Int Med Res. 2021;49(10):030006052110499. doi:10.1177/03000605211049943
26. Kawamura K, Ichikado K, Suga M, Yoshioka M. Efficacy of Azithromycin for Treatment of Acute Exacerbation of Chronic Fibrosing Interstitial Pneumonia: A Prospective, Open-Label Study with Historical Controls. Respiration. 2014;87(6):478-484. doi:10.1159/000358443
27. Beigelman A, Isaacson-Schmid M, Sajol G, et al. Randomized trial to evaluate azithromycin’s effects on serum and upper airway IL-8 levels and recurrent wheezing in infants with respiratory syncytial virus bronchiolitis. J Allergy Clin Immunol. 2015;135(5):1171-1178.e1. doi:10.1016/j.jaci.2014.10.001
28. Smith C, Egunsola O, Choonara I, Kotecha S, Jacqz-Aigrain E, Sammons H. Use and safety of azithromycin in neonates: a systematic review. BMJ Open. 2015;5(12):e008194. doi:10.1136/bmjopen-2015-008194
29. D’Ignazio J, Camere MA, Lewis DE, Jorgensen D, Breen JD. Novel, Single-Dose Microsphere Formulation of Azithromycin versus 7-Day Levofloxacin Therapy for Treatment of Mild to Moderate Community-Acquired Pneumonia in Adults. Antimicrob Agents Chemother. 2005;49(10):4035-4041. doi:10.1128/AAC.49.10.4035-4041.2005
30. Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011;365(8):689-698. doi:10 .1056/NEJMoa1104623
31. Sun Y wen, Cen Y hua, Chen M heng, Yan X ke, Jin X fen. Safety profiles and adverse reactions of azithromycin in the treatment of pediatric respiratory diseases: A systematic review and meta-analysis. Medicine. 2023;102(48):e36306. doi:10.1097/MD.0000000000036306
32. Parmar D, Jadav S, Shah B. Can azithromycin be substituted for amoxycillin in upper respiratory tract infections? An observation based on a drug utilization at some primary health centers. Indian J Pharmacol. 2007;39(1):55. doi:10.4103/0253-7613.30766
33. EFFECTIVENESS AND COST-EFFECTIVENESS OF ANTIBIOTIC TREATMENTS FOR COMMUNITY ACQUIRED PNEUMONIA (CAP) AND ACUTE EXACERBATIONS OF CHRONIC BRONCHITIS (AECB) | Journal of Population Therapeutics and Clinical Pharmacology. Accessed March 7, 2024. https://www.jptcp.com/index.php/jptcp/article/view/90
34. Samsa GP, Matchar DB, Harnett J, Wilson J. A Cost-Minimization Analysis Comparing Azithromycin-Based and Levofloxacin-Based Protocols for the Treatment of Patients Hospitalized With Community-Acquired Pneumonia. Chest. 2005;128(5):3246-3254. doi:10.1378/chest.128.5.3246
35. Rahav G, Fidel J, Gibor Y, Shapiro M. Azithromycin versus comparative therapy for the treatment of community acquired pneumonia. Int J Antimicrob Agents. 2004;24(2):181-184. doi:10.10 16/j.ijantimicag.2004.01.011
36. McCarty JM. Azithromycin (Zithromax(R)).
37. Morimoto T, Koyama H, Shimbo T, Fukui T. [Cost-effectiveness analysis of ambulatory treatment for adult patients with community-acquired pneumonia: according to Japanese Respiratory Society guidelines]. Nihon Kokyuki Gakkai Zasshi. 2002;40(1):17-25.
38. Economic analysis of antibiotic regimens used in the treatment pharyngitis: a prospective comparison of azithromycin versus roxithromycin | Journal of Antimicrobial Chemotherapy | Oxford Academic. Accessed March 7, 2024. https://academic.oup.com/jac/article/37/suppl_C/151/683595?login=false
39. Azithromycin Compared with Clarithromycin in the Treatment of Adult Patients with Acute Purulent Tracheobronchitis: A Cost of Illness Study – J Sternon, , Bruxelles the Collaborative Group of the Centre Universitaire de Medécine Générale de l’ Université Libre, Bruxelles the Collaborative Group of the Centre Universitaire de Medécine Générale de l’ Université Libre, P Leclerq, C Knepper, K Blot, 1995. Accessed March 7, 2024. https://journals.sagepub.com/doi/abs/10.1177/030006059502300602
40. Mahashur A. Management of lower respiratory tract infection in outpatient settings: Focus on clarithromycin. Lung India. 2018;35(2):143-149. doi:10.4103/lungindia.lungindia_262_17
41. Azithromycin – an overview | ScienceDirect Topics. Accessed April 29, 2024. https://www.sciencedirect.com/topics/chemistry/azithromycin
42. Treadway G, Pontani D, Reisman A. The safety of azithromycin in the treatment of adults with community-acquired respiratory tract infections. Int J Antimicrob Agents. 2002;19(3):189-194. doi:10. 1016/s0924-8579(01)00490-3