





Risk Factors for Delirium in Hospitalized Seniors
Risk Factors Linked to Delirium in Hospitalized Older Adults: A Cohort Comprehensive Study
Marina Zanella Fedrigo¹, Samara Venzzzi Tsukada¹, Nicolle Cristini Blanguer Mann¹, Clarissa Percegona¹, Rafael Avelar Machado¹, Fabiana Rutes Zabudowski², Gustavo Lenci Marques³.
- Medical School Undergraduate Student at Pontifícia Universidade Católica do Paraná, Curitiba – PR, Brazil.
- Physician of the Internal Medicine department at Hospital Universitário Cajuru, Curitiba – PR, Brazil
- Associate Professor at Pontifícia Universidade Católica do Paraná, Curitiba – PR, Brazil, and at Universidade Federal do Paraná, Curitiba – PR, Brazil
OPEN ACCESS
PUBLISHED 30 September 2024
CITATION Fedrigo, MZ., Tsukada, SV., et al., 2024. Risk Factors Linked to Delirium in Hospitalized Older Adults: A Cohort Comprehensive Study. Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5874
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5874
ISSN 2375-1924
Abstract
Background: Delirium is often underdiagnosed; it is responsible for longer hospital stays and increased mortality rates. The reason to analyze risk factors that cause delirium is to expose the most common causes of this condition and in which aspects we should intervene to prevent it.
Aim: Identify the main risk factors for the development of delirium in the hospitalized elderly, verifying prevalence and time of hospitalization.
Methods: This cohort prospective study was conducted in the city of Curitiba, State of Paraná, Brazil during February 2021. All patients above 60 years old who were admitted at a local hospital for a month were analyzed. They had their medical charts analyzed and filled out a questionnaire about previous clinical data. During the hospitalization, daily visits were performed to verify the CAM score (confusion assessment method) used to diagnose Delirium.
Results: The study included 99 elderly patients, among them 13 have developed delirium during hospitalization characterizing a prevalence of 13,13%. The incidence of delirium was associated with both use of analgesics (p<0,04) and age (p<0,018). In addition, when in a multivariate analysis considering outcome through time, the use of analgesics (p<0,05) and age (p<0,022) were considered independent markers of delirium.
Conclusion: The use of analgesics and age are related to the development of delirium, regardless of time until outcome.
Keywords: delirium, aged, hospitalization, risk factors.
Introduction
Delirium is known as a neurocognitive disorder characterized by disturbance of attention, consciousness, and cognition that develops over a short period (hours or days) and cannot be better explained by another neurologic illness and is, therefore, due to a distinct medical circumstance. Patients with delirium may present three different forms of the disease: hyperactive, hypoactive, or mixed activity and flow between them.
This condition is often underdiagnosed in medical practice, mainly because it is not a primary cause of hospitalization, but it is responsible for longer hospital stays and an increase in the mortality rates of critical patients. Furthermore, the ICU (Intensive Care Unit) is a high-risk environment for the occurrence of this syndrome due to the several triggering factors for neurological disorders, such as sleep deprivation, lack of natural lighting, physical restrictions, surgical procedures, use of sedative drugs, and emotional aspects.
The prevalence of delirium is higher among hospitalized elderly patients. In the community, its incidence ranges between 1-2%, but it increases with age, affecting approximately 14% of individuals over 85 years old. Delirium is predominantly present at hospital admission, with rates ranging between 14-24%. Some estimates suggest that the development of the condition during hospitalization occurs in 6-56% of the general hospital population. Moreover, delirium occurs in 15-53% of elderly patients in the postoperative period and 70-87% of those in the ICU. In nursing homes, the percentage of affected individuals reaches 60%, and towards the end of life, approximately 83% of the population experiences delirium.
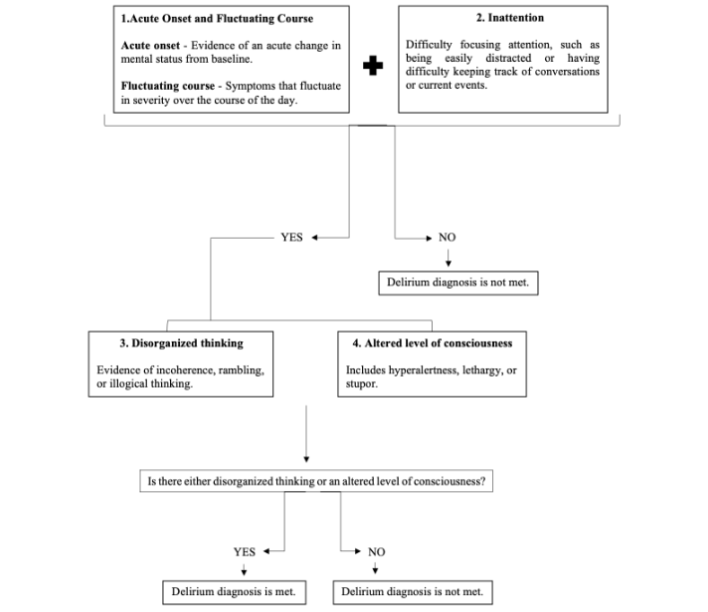
A simple tool that can be used by clinicians to integrate their observations and identify when delirium is the most probable diagnosis is called the Confusion Assessment Method (CAM), whose purpose is to assess a patient’s confusion. This method has four criteria: 1 – acute onset and fluctuation of baseline mental status; 2 – attention disorder; 3 – disorganized thinking; and 4 – altered consciousness level. The patient is diagnosed with delirium when manifests both criteria 1 and 2, together with criteria 3 or 4. This method consists of observing the patient’s non-verbal reaction to simple commands integrated with yes or no answers to simple questions. In addition, it is important to notice some findings, like disorientation, memory, disturbance of perception, psychomotor agitation, and changes in the sleep-wake cycle.
Given the most common predictors of delirium cited in the bibliography, such as older age, depression, sleep deprivation, infection, polypharmacy, constipation, and physical restraint, the most supported method for prevention and treatment of the disease is the non-pharmacological one: to create a favorable environment for the patient who is in the risk group or has already developed delirium. If it is not possible to identify or treat a single primary cause, it is better to maintain adequate hydration levels, establish some communication with the patient to orient him about time and space and, if possible, provide stimulating activities involving family members.
Objective
The purpose of this research is to evaluate the main risk factors for the development of delirium in the elderly admitted to the hospital ward for any reason.
Methods
This prospective cohort study was conducted at a hospital in Curitiba, Brazil, during February 2021. The study aimed to evaluate delirium incidence and risk factors among patients aged 60 years or older who were admitted to the hospital during this period. Enrollment criteria were limited to age, encompassing all patients who met the age threshold. A total of 134 patients were initially considered for inclusion. However, 35 patients were excluded based on the following criteria: death during hospitalization, transfer to the Intensive Care Unit (ICU), receipt of palliative care, Glasgow Coma Scale (GCS) score ≤ 8, or refusal to participate. Patients with pre-existing neurological conditions were not excluded from the study, as we aimed to assess delirium within this group as well. The method is demonstrated in “Flowchart 1”.
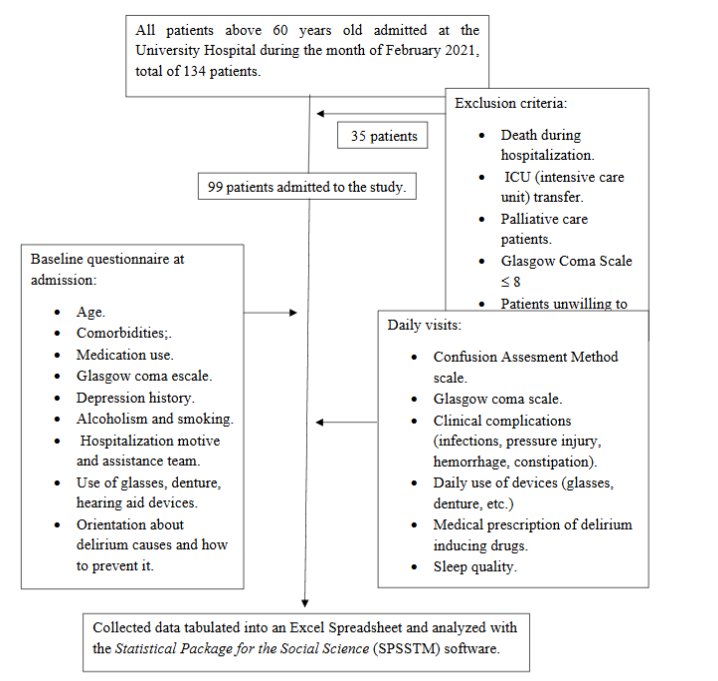
Eligible patients were enrolled and underwent a baseline assessment upon admission. This assessment, conducted in Brazilian Portuguese by the study authors, included a comprehensive questionnaire covering: age, comorbidities, prescription of medications known to induce delirium, history of depression, alcohol use, smoking status, capacity to respond to questions independently, presence of a companion at admission, reason for hospitalization, the assisting medical team, use of assistive devices, urinary catheterization, and nasogastric or nasoenteric tube placement. Additionally, we assessed whether the companion received information about delirium risk and prevention strategies. Neurological status at admission was evaluated using the Glasgow Coma Scale and the FOUR Score (Full Outline of Unresponsiveness). Patients with a Glasgow Coma Scale score of 8 or lower were excluded from the study due to their inability to respond independently; these patients were usually intubated, on mechanical ventilation, and admitted to the ICU.
Patients were subsequently followed up daily, by the authors, throughout their hospital stay. Delirium was assessed using the CAM scale (Confusion Assessment Method), a validated clinical tool that diagnoses delirium based on the following criteria: first, the patient must present both acute changes in mental status from baseline with fluctuating course and difficulty of focusing attention. Besides these two, it must have the presence of either disorganized thinking or an altered level of consciousness. Only patients meeting these CAM criteria were diagnosed with delirium. The Glasgow Coma Scale and FOUR Score were administered daily to monitor the status of alertness, a criterion for delirium that could also act as a confounding factor. As described earlier, patients who had a significant deterioration in their level of consciousness during their hospital stay, necessitating intubation or transfer to the ICU, were excluded from the study.
Daily evaluations also included the occurrence of clinical complications such as infections, pressure injuries, hemorrhages, or constipation, the use of delirium prevention devices, and the administration of medications either inducing or preventing delirium.
Upon hospital discharge, data collected included discharge date, length of hospital stay, presence of delirium during hospitalization, the presence of a companion for most of the stay, implementation of delirium prevention measures, prescription of delirium treatment, and any complications or adverse events experienced during hospitalization. The CAM diagnostic flowchart used for diagnosis of delirium in this study is demonstrated in “Flowchart 2”.
Data were entered into an Excel spreadsheet and analyzed using Statistical Package for the Social Science (SPSSTM) software. Continuous variables are reported as median (interquartile range) or mean ± standard deviation (SD), while categorical variables are expressed as frequencies and percentages. The student’s t-test was used to compare continuous quantitative variables between two groups. Multivariate linear regression analysis was conducted to examine variables in relation to the duration of hospitalization and delirium outcomes. Statistical significance was defined as p < 0.05.
The study design and methodology were approved on December 11th, 2020, by the Ethics Research Committee of Pontifícia Universidade Católica do Paraná (Protocol number CAAE: 40447820.3.0000.0020). All patients gave written informed consent before the commencement of this research.
Results
Altogether, 99 patients, 51 males and 48 females, with a medium age of 75 years old, were included in this study. The major cause of hospitalization was bone fracture, and the main assistance team was orthopedics.
The most prevalent comorbidities were systemic arterial hypertension and type 2 diabetes without complications, affecting 69.69% and 31.31% of patients, respectively. Among the medications used, diuretics constituted 31.31%, beta-blockers 25.25%, and analgesics 26.26%, with opioids (tramadol, codeine and morphine) making up 22.22% and non-steroidal anti-inflammatory drug (ketoprofen) 6.06%. Less than 1% of patients’ families received instructions about the possibility of the development of delirium during the hospitalization period and how to prevent it. This characterization of the patients participating in the study was expressed in “Table 1”.
| Variables | Delirium (n=13) | No Delirium (n=86) | p value |
|---|---|---|---|
| Age (years) | 75,85 (±2,47) | 69,91 (±0,88) | 0,018 |
| Glasgow Scale | 14,62 (±0,31) | 14,81 (±0,09) | 0,470 |
| Four Scale | 16,00 (±0,0) | 16,06 (±0,13) | 0,864 |
| Comorbidities (%): | |||
| Dementia | 2 (15,3%) | 8 (9,3%) | 0,616 |
| Diabetes type 2 without complications | 4 (30,76%) | 27 (31,39%) | 1,000 |
| Diabetes type 2 with complications | 2 (15,3%) | 3 (3,4%) | 0,127 |
| Peripheral arterial disease | 2 (15,3%) | 1 (1,16%) | 0,045 |
| Connective tissue disease | 1 (7,69%) | 0 (0,0%) | 0,131 |
| Hypertension | 9 (69,23%) | 58 (67,4%) | 1,000 |
| Myocardial Infarction | 1 (7,69%) | 4 (4,65%) | 0,513 |
| Heart Failure | 2 (15,3%) | 6 (6,97%) | 0,282 |
| Devices (%): | |||
| Glasses | 9 (69,23%) | 53 (61,62%) | 0,762 |
| Denture | 7 (53,84%) | 54 (62,79%) | 0,554 |
| Hearing aid | 1 (7,69%) | 1 (1,16%) | 0,247 |
| Bladder catheter (%) | 2 (15,3%) | 7 (8,13%) | 0,336 |
| Nasogastric tube (%) | 0 (0,0%) | 4 (4,65%) | 1,000 |
| Use of medication (%): | |||
| Antimicrobials | 13 (100%) | 66 (76,74%) | 0,700 |
| Analgesics | 3 (23,07%) | 15 (17,44%) | 0,004 |
| Corticosteroids | 8 (61,53%) | 18 (20,9%) | 1,000 |
| Dopaminergic agonists | 0 (0,0%) | 4 (4,65%) | 1,000 |
| Anticonvulsants | 0 (0,0%) | 1 (1,16%) | 0,635 |
| Antidepressants | 2 (15,3%) | 9 (10,46%) | 0,267 |
| Sedatives | 4 (30,76%) | 15 (17,44%) | 1,000 |
| Muscle relaxants | 1 (7,69%) | 10 (11,62%) | 1,000 |
| Cardiovascular medication | 0 (0,0%) | 1 (1,16%) | 0,079 |
| Herbal medicines | 9 (69,23%) | 36 (41,86%) | 1,000 |
| Donepezil | 0 (0,0%) | 1 (1,16%) | 1,000 |
| Anticholinergics | 1 (7,69%) | 1 (1,16%) | 1,000 |
| Infusion of medication after 10 pm (%) | 4 (30,76%) | 35 (40,69%) | 0,558 |
| Presence of companionship (%) | 7 (53,84%) | 38 (44,18%) | 0,561 |
| Prevention measurements applied during hospitalization (%) | 2 (15,3%) | 22 (25,58%) | 0,729 |
| Constipation (%) | 6 (46,15%) | 20 (23,25%) | 0,097 |
| Pressure ulcer (%) | 1 (7,69%) | 2 (2,32%) | 0,351 |
| Low diet acceptance (%) | 2 (15,3%) | 6 (6,97%) | 0,282 |
| Gastrointestinal bleeding (%) | 0 (0,0%) | 1 (1,16%) | 1,000 |
| Infection (%) | 1 (7,69%) | 1 (1,16%) | 0,247 |
| Sepsis (%) | 0 (0,0%) | 1 (1,16%) | 1,000 |
In this study, the mean number of days patients stayed hospitalized was 6,31. Among all, 13 patients have developed delirium during the period of hospitalization, and these remained in the hospital for 3 days, on average, and 3,3 days until the outcome. In the statistical analysis, the incidence of delirium was most associated with the use of analgesic drugs (p = 0,04) and age (p = 0,018). The multivariate analysis, considering event and time, confirmed that both analgesic use (p = 0,05) and age (p = 0,023) were independent markers for delirium, as showed in “Table 2”.
| Variables | p value | Hazard Ratio | CI 95% |
|---|---|---|---|
| Analgesics | 0,005 | 5,017 | 1,634 – 15,399 |
| Age | 0,022 | 1,073 | 1,010 – 1,140 |
Moreover, other variables, such as hospital usage of glasses (p = 0,762), hearing aid (p = 0,247) and denture (p = 0,554), bladder catheter (p = 0,336), nasogastric tube (p = 1), daily companion for at least 12 hours (p = 0,561), drug infusion after 10 pm (p = 0,558), constipation (p = 0,97) and dementia (p = 0,616) were not associated with the outcome.
Discussion
In this prospective cohort study, the incidence of delirium among hospitalized patients was found to be 13.13%. The average onset of delirium occurred approximately 3.3 days after admission, consistent with the findings of Zhang et al. who reported that delirium typically manifests around the second or third day of hospitalization.
The key predictors identified in our study for delirium were advanced age and the use of analgesics. Specifically, patients who developed delirium had an average age of 75 years, compared to 69 years in those who did not develop delirium. While both groups comprised elderly individuals (aged over 60), the older cohort in the delirium group exhibited a significantly higher average age. This underscores the heightened susceptibility of older individuals within the elderly population to delirium.
It is well-established that aging and polypharmacy are significant risk factors for delirium. However, research directly linking analgesics to delirium remains scarce. In our study, most patients were hospitalized due to bone fractures, suggesting that severe pain and subsequent analgesic use might be relevant factors. This observation is consistent with Zhang et al.’s study, which also highlighted the significance of pain (p = 0,018) in the development of delirium. Pain-induced stress can disrupt the sleep-wake cycle, contribute to decreased mobility, and exacerbate confusion in elderly patients.
Analgesic use was particularly noteworthy in our study, with opioids being more prevalent compared to non-steroidal anti-inflammatory drugs (NSAIDs). Opioids, which primarily act on mu-opioid receptors to reduce nociceptive transmission from the periphery to the thalamus, are associated with adverse effects such as respiratory depression, bradycardia, reduced gastric motility, nausea, and drowsiness. This sedative effect could contribute to a confused state, aligning with previous studies linking opioid use to an increased risk of delirium in elderly patients.
Our findings corroborate existing literature indicating a higher risk of delirium associated with opioid use. Notably, a study found a significantly higher risk of delirium in patients using opioids for hip fractures, which aligns with our results, particularly since bone fractures were the primary reason for hospitalization in our study. While the link between opioid use and delirium has been documented, our study extends these findings by suggesting that severe pain, often necessitating higher analgesic doses, may also contribute to delirium. The significance of effective pain management in preventing delirium cannot be overstated. Both under-treatment and over-treatment of pain may contribute to delirium, emphasizing the need for careful assessment and appropriate analgesic prescription. Alternative strategies such as multimodal analgesia, non-pharmacological pain management techniques, and individualized pain management plans could help mitigate delirium risk.
Additionally, age-related physiological changes may make older adults more susceptible to the effects of analgesics. Future research should explore these mechanisms in greater depth and investigate the long-term impact of different analgesics on delirium. Educational initiatives for healthcare providers and families about the risks of delirium related to analgesic use are essential. Ensuring that patients and their families are informed and involved in the care plan can improve outcomes and prevent delirium.
While advanced age and analgesic use emerged as significant predictors of delirium, other variables, including the use of glasses, hearing aids, dentures, bladder catheters, nasogastric tubes, daily companions, drug infusion timing, constipation, and pre-existing dementia, were not found to be significantly associated with delirium. The lack of association for these variables warrants a closer examination in the context of existing literature and possible explanations.
The absence of a significant association between the use of sensory aids (glasses, hearing aids, dentures) and delirium may be attributed to the fact that these sensory aids are typically used to address specific deficits rather than directly influencing cognitive function. Previous studies have indicated that while sensory impairments can contribute to confusion and cognitive decline, their direct impact on delirium is less pronounced compared to other factors like acute medical illness or medication effects.
Regarding bladder catheter and nasogastric tube, the lack of association may be due to these interventions being relatively common and not necessarily linked to delirium unless they contribute to significant discomfort or complications. Research indicates that while the presence of invasive devices can be a risk factor for delirium, their impact may vary based on individual patient conditions and the presence of other delirium risk factors.
As to having a daily companion for at least 12 hours, the absence of correlation suggests that continuous social support might not directly impact delirium risk. Studies have shown that social support can be beneficial for overall mental health and may help in the management of delirium by providing emotional comfort and reducing stress. However, our study did not find a direct link, possibly because the presence of a companion alone does not address the multifaceted causes of delirium.
The non-significant association between drug infusion after 10 PM and delirium might reflect the complexity of the pathophysiology of this illness. Although night-time drug administration could theoretically disrupt sleep patterns and contribute to delirium, our results suggest that other factors might play a more substantial role. Previous research indicates that sleep disturbances are a risk factor for delirium, but the timing of drug administration alone may not be a primary determinant.
In respect of constipation, the irrelevancy may be since while constipation can contribute to discomfort and secondary complications, its direct impact on delirium might be less significant compared to more immediate and severe medical issues. Previous studies have found that while constipation can exacerbate confusion, it is generally not a primary risk factor for delirium on its own.
The insignificance association with pre-existing dementia contrasts with some literature suggesting that dementia is a known risk factor for delirium. However, the lack of significant findings in our study could be due to the specific characteristics of our cohort or the interactions between pre-existing dementia and other risk factors. Some studies indicate that while dementia increases the risk of delirium, the presence of delirium may also depend on the interplay between various acute and chronic conditions.
In summary, while our study found no significant associations between delirium and several variables previously considered potential risk factors, it is important to consider that the impact of these variables may be influenced by other confounding factors or individual patient circumstances. The complex nature of delirium requires a multifaceted approach to understanding its predictors, and further research is needed to clarify these relationships and explore other potential risk factors in diverse patient populations.
Several limitations of this study should be acknowledged. Firstly, as an observational study, it does not establish causality. The sample size was relatively small, limiting the generalizability of our findings to all cases. Additionally, the study was conducted at a single hospital in Curitiba, PR, Brazil, which may restrict the applicability of the results to other settings. Some data were also incomplete due to constraints such as missing information from the nursing team and patients being unavailable for evaluation due to exams or surgeries. Addressing these limitations would require a more comprehensive, full-time observational approach.
Conclusion
In summary, our study highlights the significant role of advanced age and analgesic use in delirium risk. By incorporating these findings into clinical practice and further research, we can improve pain management strategies and potentially reduce the incidence of delirium in elderly patients.
Conflicts of interest statement
The authors whose names were listed previously certify that they have no affiliations with any organization or entity with a financial interest. Also, they have no economic participation in the subject matter discussed in this manuscript.
Funding statement
The authors disclose that this study did not receive any financial support for research, authorship, and publication of this article.
Acknowledgments
We would like to express our gratitude to Hospital Universitário Cajuru, where this research was conducted.
References
- Van Velthuijsen EL, Zwakhalen SMG, Mulder WJ, Verhey FRJ, Kempen GIJM. Detection and management of hyperactive and hypoactive delirium in older patients during hospitalization: a retrospective cohort study evaluating daily practice. Int J Geriatr Psychiatry. 2018;33(11):1521–9. PMID: 28194812
- Diagnostic and Statistical Manual of Mental Disorders. 5o ed. American Psychiatric Publishing; Washington, 2013. 970 p.
- Da Silva Baptista Faria R, Moreno RP. Delirium na unidade de cuidados intensivos: uma realidade subdiagnosticada. Rev Bras Ter Intensiva. 2013;25(2):139;143. DOI: 10.5935/0103-507X.20130025
- Burton JK, Craig LE, Yong SQ, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2021;2021(7). PMID: 34826144
- Mattison M, Schmader KE, Auerbach AD. Hospital management of older adults. UptoDate. 2019;1–41. Available at: https://www.uptodate.com/contents/hospital-management-of-older-adults
- National Clinical Guideline Center. DELIRIUM: diagnosis, prevention and management Update information. Clin Guidel 103 [Internet]. London, 2010;(July). Available at: www.nice.org.uk/guidance/cg103
- Zhang M, Zhang X, Gao L, Yue J, Jiang X. Incidence, predictors and health outcomes of delirium in very old hospitalized patients: a prospective cohort study. BMC Geriatr [Internet]. 2022;22(1):1–10. Available at: https://doi.org/10.1186/s12877-022-02932-9
- Lima BR, Nunes BKG, Guimarães LCC, Almeida LF, Pagotto V. Incidence of delirium following hospitalization of elderly people with fractures: risk factors and mortality. Rev Esc Enferm USP. 2021;55:e20200467. doi: https://doi.org/10.1590/1980-220X-REEUSP-2020-0467
- Pathan H, Williams J. Basic opioid pharmacology: an update. Br J Pain. 2012;6(1):11–6. PMCID: PMID: 26516461
- Souza JS, Ribeiro TB, Ferrari TC. Delirium and use of analgesics in elderly patients hospitalized with femoral fracture. Age Ageing. 2019;48(4): 545-9. doi: 10.1093/ageing/afz072
- Tzeng RC, Chiu YS, Hsu SC. The impact of sensory deficits on delirium risk in elderly patients. Geriatr Nurs. 2010;31(5):355-362.
- van Gool WA, Van de Vorst I, van der Meer J, et al. Risk factors for delirium in elderly patients after hip surgery: a review of the literature. Int J Geriatr Psychiatry. 2000;15(3):215-223.
- Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal A, Horwitz RI. Clarifying confusion: The Confusion Assessment Method. Ann Intern Med. 2001;113(12):941-948.
- Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal A, Horwitz RI. Delirium in elderly patients: Clinical review. Am J Med. 1999;106(1):1-10.
- Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306-1316.
- Krogstad U, Bruun K, Midtgaard M. Constipation and delirium: A systematic review. J Clin Nurs. 2013;22(13-14):1866-1874.
- Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2015;11(3):332-384.
- O’Keeffe ST. Delirium in the elderly. J Clin Psychiatry. 2002;63(2):110-115.