

MRI Efficiency in Augmented Breast Filler Evaluation
The Efficiency of MR Imaging in Augmented Breasts Post Filler Injection
1. Introduction
Since the late 19th century, the pursuit of enhancing breast aesthetics has significantly shaped cosmetic surgery practices. Initially focused on improving breast contour and volume, these procedures have profoundly impacted women’s self-esteem and body image. Studies exploring the psychological effects of aesthetic surgery highlight that many patients, particularly young women, seek breast augmentation to alleviate psychological distress associated with their body image¹. The origins of breast contour enhancement trace back to 1895, when surgeons utilized autologous adipose tissue from benign lumbar lipomas to correct asymmetries often arising from tumor removals. This approach evolved from earlier, less successful experiments, such as those in 1889 by surgeon Robert Gersuny, who injected paraffin into the breasts, leading to severe complications such as infection and deformation².
As the field advanced into the early to mid-20th century, a variety of materials were experimented with for breast augmentation. The 1950s and 1960s saw the rise of synthetic fillers like silicone, which became popular among approximately 50,000 women seeking breast enhancements. However, the use of such fillers often resulted in complications, including the development of silicone granulomas and breast hardening, posing significant health risks³. A pivotal advancement occurred in 1964 when the French company Laboratories Arion introduced saline breast implants. These implants, filled with a saline solution, marked a significant improvement in safety and effectiveness over previous silicone implants, setting a new standard in implant technology⁴.
The rising popularity of bilateral intra-breast collagen/filler injections, particularly noticeable in regions like the Philippines where beauty salon workers of diverse nationalities often administer these procedures, highlights a global trend⁵. This practice is similarly prevalent in Kuwait, where non-medical personnel in various beauty salons also perform these injections. The widespread adoption of this approach has led to a notable influx of patients into hospital surgery departments, presenting with symptoms such as breast lumps, which are frequently a direct result of these non-medical enhancements⁶. As a result, these patients are often referred to specialized departments for more in-depth evaluations, underlining the necessity for effective diagnostic modalities to identify and manage potential complications arising from these cosmetic procedures⁷.
In the context of modern cosmetic procedures, the use of MRI for evaluating breasts post-filler injection has become a critical area of study⁸. MRI is lauded for its exceptional sensitivity and specificity, making it an essential tool for precisely detecting complications associated with breast filler injections without radiation exposure. While traditional studies have primarily focused on silicone implant ruptures, similar principles can be applied to modern fillers, which may exhibit unique behaviors under MRI due to their distinct compositions³. MRI’s effectiveness in this context is largely due to its ability to exploit the unique magnetic resonance frequencies of different materials, including both silicone and newer filler substances. This capability allows radiologists to employ material-specific sequences during MRI scans, significantly improving the accuracy of diagnostic assessments. By targeting specific resonance frequencies, MRI can clearly differentiate between normal post-injection tissues and potential complications such as migration, degradation, or unusual responses of the filler material within the tissue⁹.
Moreover, MRI’s ability to non-invasively visualize the internal structure of breast tissues and the interaction with injected materials makes it an invaluable tool in the follow-up care of patients who have received filler injections. This advanced imaging technique ensures that clinicians can detect even minor irregularities early, facilitating timely interventions that can prevent more serious complications. The refinement and application of MRI techniques tailored to assess fillers and other augmentation materials mark significant advancements in the field of cosmetic surgery diagnostics. As the popularity of non-surgical cosmetic procedures continues to rise, the role of advanced imaging technologies like MRI becomes increasingly vital, not only for detecting potential complications but also for ensuring patient safety and satisfaction with cosmetic enhancements.
Breast Magnetic Resonance Imaging (MRI) offers significant advantages over traditional imaging techniques such as mammography and sonography, especially in the context of evaluating complications associated with breast filler injections. Its capacity for multiplanar imaging allows clinicians to view the breast from multiple dimensions, providing a more comprehensive assessment of the anatomical structures and any anomalous changes. This feature, coupled with MRI’s superior tissue characterization and the absence of ionizing radiation, makes it an ideal choice for patients who require ongoing monitoring after breast enhancement procedures¹⁰. In situations involving complications from breast filler injections, such as extracapsular migration of the filler material, MRI is particularly invaluable. It can meticulously detail the extent of filler dispersion and its impact on nearby vital structures, including axillary lymph nodes and the brachial plexus. Such detailed imaging is critical not only for diagnostic accuracy but also for planning any necessary interventions to mitigate adverse effects¹¹.
Furthermore, MRI is regarded as the diagnostic method of choice for detecting breast cancer in patients who have received breast filler injections. The presence of fillers can often obscure mammographic and sonographic readings, as these randomly distributed materials can create shadows and density variations that mimic or mask malignancies¹². In cases where silicone-induced mastopathy presents with fibrous masses, these can be difficult to distinguish from breast cancer using less sensitive imaging modalities. MRI, with its ability to employ both contrast-enhanced and T2-weighted sequences with fat and water suppression, offers a critical diagnostic advantage. This approach significantly enhances the ability to differentiate benign conditions resulting from the filler material from malignant tumors, thereby informing more accurate clinical decision-making¹³. The commitment to utilizing advanced imaging techniques reflects our dedication to providing precise diagnostic insights, ensuring that patients receive the most effective and personalized care. By leveraging the capabilities of MRI, this pilot study aims to review the efficiency of MRI in the evaluation of breasts augmented with filler injections, exploring its role in enhancing patient outcomes and addressing the unique challenges posed by non-traditional augmentation methods.
2. Methods
2.1. STUDY DESIGN AND SETTING
This retrospective pilot study was conducted with nine patients who had previously undergone breast filler injections and subsequently presented with a variety of symptoms, including breast pain, nodularity, swelling, anxiety, and skin erythema. These individuals were referred to the breast imaging unit at Mubarak Al Kabeer Hospital, a secondary care teaching hospital, for comprehensive imaging assessment.
Given the observational nature of the study, the requirement for written informed consent was waived. All procedures complied with standards set forth by the local hospitals. No additional data beyond those obtained during routine clinical imaging were used in the study. Each examination adhered strictly to clinical protocols and best practices, focusing solely on diagnostic imaging. All patient data were fully anonymized at the outset of the study to protect privacy and ensure confidentiality. This approach allowed for the ethical use of clinical imaging data while contributing to the understanding of complications associated with breast filler injections. By utilizing advanced imaging protocols, this study sought to evaluate the diagnostic utility of MRI in differentiating between filler material, benign breast masses, and any potential malignancies.
2.2. STUDY METHODS
The study evaluated women who presented at our outpatient clinic. Each participant underwent an extensive interview to meticulously gather their medical history. This process focused on identifying any comorbidities such as cardiovascular disease or diabetes, chronic medications that might interact with treatment outcomes, smoking habits which could affect healing processes, and their age at the time they received filler or collagen injections for breast augmentation. Additionally, we explored their previous experiences with cosmetic procedures, their motivations for seeking breast augmentation, and their expectations from the treatment to better understand the psychological and social factors influencing their decision. This comprehensive approach ensured a well-rounded understanding of each participant’s health background and personal motivations, which are crucial for assessing the outcomes of cosmetic interventions.
Prior to the follow-up imaging and assessment process, we conducted detailed inquiries into specific symptoms that each participant might be experiencing. These included breast pain, noticeable changes in breast shape (deformation), the presence of lumps, general discomfort, and any indications of infection. This information was vital for tailoring subsequent imaging and treatment plans. In addition to symptom checks, we gathered exhaustive data regarding the breast augmentation procedures themselves. This included documenting the type of filler material used, the exact timing of the injections, and the total quantity of material injected into each patient (when known by the patient). Further details about the physical properties of these materials, such as their shape and texture, were also carefully recorded to assist in the analysis of imaging results and treatment outcomes.
A thorough physical examination was performed on each participant, with special emphasis on manual breast examination. This examination focused on identifying any irregularities in breast size, the firmness of the tissue, or any anomalous findings that could indicate complications. We also measured breast dimensions to track changes over time and assess the physical impact of the filler material. Lastly, we evaluated the overall aesthetic results of the augmentation to determine if the desired cosmetic outcomes were achieved. This assessment included checking for any surgical complications that might have arisen post-procedure, such as infections or the enlargement of axillary lymph nodes. All findings from these examinations were meticulously documented to ensure a comprehensive understanding of each case and to guide further medical or surgical interventions if necessary.
Not every participant in our study underwent bilateral breast mammograms. Specifically, six patients first received an ultrasound (US) scan of the breast, and one of these patients was directly recommended for an MRI scan, bypassing the initial ultrasound step. Most of these ultrasound examinations (eight patients in total) were performed using a Siemens Acuson S2000 ultrasound system, while one ultrasound was conducted using a Toshiba ultrasound system (USEL-A501A) at the Al-Faisel center in Kuwait, demonstrating the utilization of varied imaging technologies across different facilities. Our established diagnostic protocol generally consisted of an ultrasound followed by a mammogram for six of the patients. However, two patients deviated from this routine due to the inconclusive results from their previous scans, which failed to provide substantial diagnostic insights. After discussions with the overseeing surgeon regarding these cases, it was decided that these patients would benefit more from additional ultrasound assessments followed by detailed MRI scans to better evaluate their conditions. In addition to these instances, two other patients were directed straight to MRI scans without undergoing any preliminary ultrasound or mammogram, based on specific clinical indications or previous imaging histories. For the patients who did undergo mammography, a comprehensive set of four views was captured for each: two mediolateral oblique views and two craniocaudal views, all performed using a GE Seno Essential system. This approach ensured a thorough and varied assessment, aiming to capture a detailed and accurate representation of breast tissues for diagnostic purposes.
MRI scans were systematically performed for all patients between the 6th and 16th days of their menstrual cycle, employing a 1.5 Tesla GE closed MRI system known for its high-resolution imaging capabilities. The scanning protocol was meticulously designed to encompass a comprehensive array of sequences to capture detailed tissue characteristics: T1-weighted Axial, T2-weighted STIR Axial, Axial Diffusion-Weighted imaging, Bilateral Sagittal T2, and Axial VIBRANT sequences. These sequences are specifically chosen for their ability to differentiate between various types of soft tissue, providing clarity on tissue integrity and pathology. Furthermore, dynamic gadolinium-enhanced imaging was meticulously performed in seven distinct phases to assess the vascularity and perfusion characteristics of the breast tissues, crucial for identifying abnormal changes. Gadolinium, a contrast agent, improves the visibility of internal structures and is particularly effective in highlighting abnormal tissue responses that might indicate pathology. As part of the thorough imaging evaluation, subtracted images were generated to remove background noise and enhance the visibility of abnormalities. Maximum Intensity Projection (MIP) techniques were used to create 3D representations from the slice data, facilitating a better understanding of the structural arrangement and spatial relationships of the breast tissues. Kinetic curves, analysing the uptake and washout of the contrast agent over time, provided valuable insights into the dynamic behaviour of the lesions. Additionally, color maps were produced to visually distinguish among different tissue types based on their physiological properties, enhancing diagnostic accuracy. This comprehensive imaging protocol was pivotal in ensuring detailed and accurate assessments of breast augmentation and associated conditions.
2.3. INCLUSION CRITERIA
• The study included adult women aged 18 years and older. The age limit ensures participants are legally capable of giving informed consent and have completed most of their physiological breast development.
• History of Filler Injections: Only individuals who have previously undergone breast augmentation using filler injections (e.g. hyaluronic acid which will be absorbed after while, polyacrylamide, collagen, or other biocompatible materials) was included
• Participants who agreed to follow the study’s protocols, including attending all scheduled follow-up visits, undergoing required imaging studies, and providing all necessary medical history and current health information.
• Participants who were not pregnant.
• Psychological Considerations: As with implant studies, a stable psychological state is crucial since aesthetic procedures can have significant mental health implications.
2.4. STATISTICAL ANALYSIS
For data management and analysis in this cohort pilot study, the Statistical Package for the Social Sciences (SPSS) version 20 was utilized. Quantitative variables were described using the mean, standard deviation (SD), along with the median, minimum, and maximum values. Qualitative data were summarized using frequencies and percentages.
3. Results
A total of nine patients underwent bilateral breast augmentation through the injection of a material, which could not be definitively identified, although the patients reported it as collagen. The ages of the patients ranged from 25 to 47 years. Following the procedure, all patients experienced breast enlargement and were offered a second injection if they were dissatisfied with the initial results. Eight patients were referred to Mubarak Al-Kabeer Hospital, and one patient came from a screening program at the tertiary care Al-Faisel Center. Among these, five patients reported continuous pain, two experienced intermittent pain, and two presented with skin erythema. All patients had bilateral breast nodules.
Only one patient reported itching, and another successfully breastfed her baby for three months following the breast injection without any complications. The decision to request an ultrasound or mammogram scan at the radiology department was based on age criteria established by the referring surgeon. Accordingly, patients under 30 years started with an ultrasound, while those over 35 received a mammogram, as shown in Table 1. The ultrasound revealed multiple well-defined anechoic masses superficially located in both breasts, of varying sizes, as depicted in Figure 1.
The normal breast structure was obscured by shadowing. Normal-sized lymph nodes with central echogenic shadowing, likely from the injected material, were observed in both axillae. Only five of the nine patients underwent mammogram scans, as two were under thirty years of age and directly referred for MRI scans, along with another two. The mammograms displayed multiple bilateral well-defined isodense masses in both breasts of various sizes, shown in Figure 2.
All nine patients received MRI scans which demonstrated multiple well-defined masses in both breasts, varying in size and accompanied by skin thickening and edema. These masses appeared iso to hypointense on T1 and hyperintense on T2, were intermediate to low on VIBRANT, and showed no contrast enhancement or restricted diffusion, as illustrated in Figure 3 and Table 2.
One patient exhibited a high signal from the injected material in the medial region of the left breast, with a tract sinus leading to the skin, as shown in Figure 4 and Table 3. Additionally, one patient was presented with a small cyst, while another displayed a well-defined, lobulated, heterogeneously enhancing mass. A core biopsy conducted on the latter patient suggested an atypical fibroadenoma, as detailed in Figure 5 and Table 3.
Table 1: Distribution of subjects: clinical data, ultrasound and mammography
| Symptoms / Signs | Frequency | Percent (%) |
|---|---|---|
| Pain | 7 | 77.8 |
| Skin erythema | 2 | 22.2 |
| Itching | 1 | 11.1 |
| Bilateral breast nodules | 9 | 100.0 |
| Ultrasound – Yes | 7 | 77.8 |
| Ultrasound – No | 2 | 22.2 |
| Mammography – Yes | 5 | 44.4 |
| Mammography – No | 4 | 55.6 |
Table 2: Distribution of subjects regarding MRI data
| Category | Finding | Frequency (Mean) | Percent (%) |
|---|---|---|---|
| Morphology | Well defined rounded | 9 | 100.0 |
| Size (cm) | Length | 1.80 | 0.54 |
| Size (cm) | Width | 1.99 | 0.39 |
| T1 | Iso to Hypointense signal | 9 | 100.0 |
| T2 | Hyperintense signal | 9 | 100.0 |
| DW | No | 9 | 100.0 |
| VIBRANT post contrast enhancement | Mild peripheral | 1 | 11.1 |
| VIBRANT post contrast enhancement | Minimal peripheral | 1 | 11.1 |
| VIBRANT post contrast enhancement | No | 7 | 77.8 |
| Axillary LN with central echogenic shadowing | Yes | 5 | 55.6 |
Table 3: Distribution of subjects regarding pathology
| Pathology | Frequency | Percent (%) |
|---|---|---|
| Sinus tract | 1 | 11.1 |
| Atypical fibroadenoma | 1 | 11.1 |
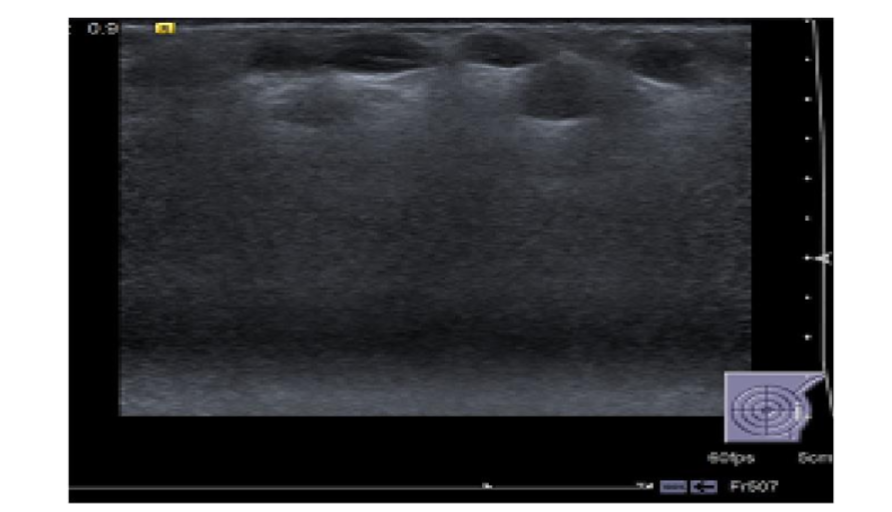
Figure 1: Multiple anechoic subcutaneous masses are seen with posterior enhancement. Notice the ‘snowstorm’ appearance obscuring the breast tissue.
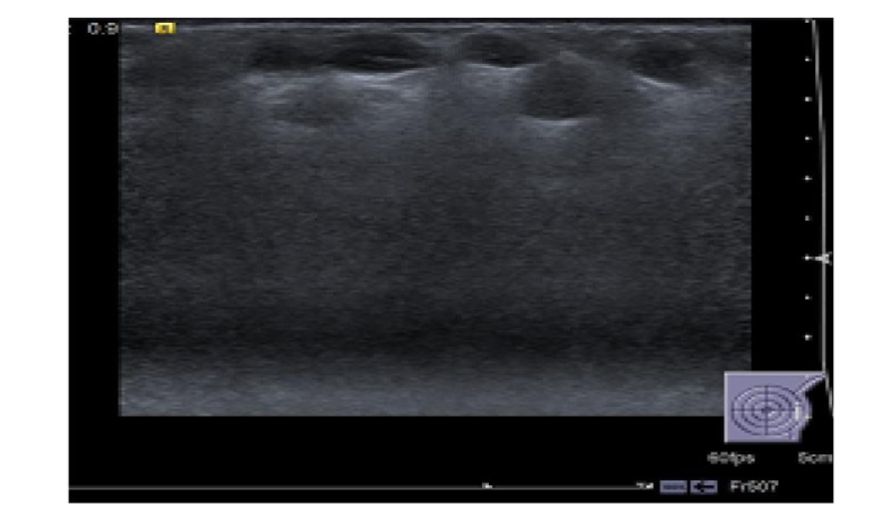
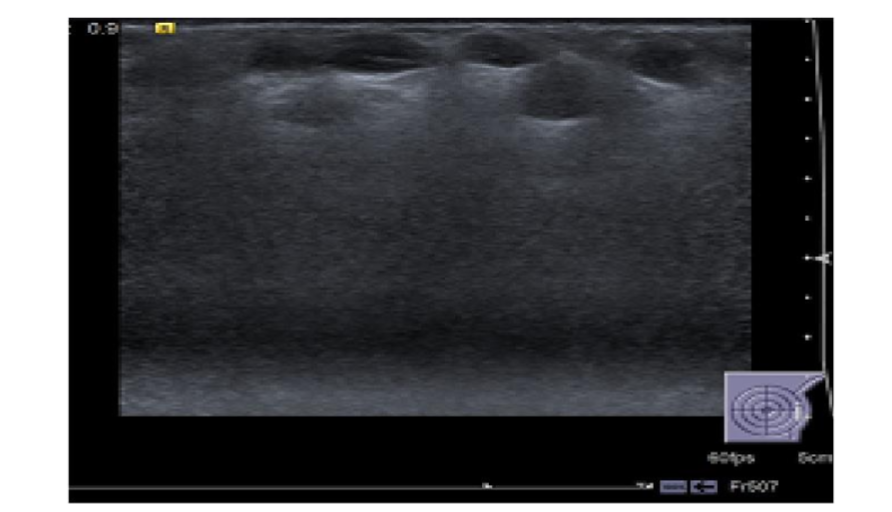
Figure 2: The mammogram CC (A) & MLO (B) views showed multiple bilateral well defined isodense masses of various sizes in both breasts. CC=craniocaudal, MLO=mediolateral oblique.
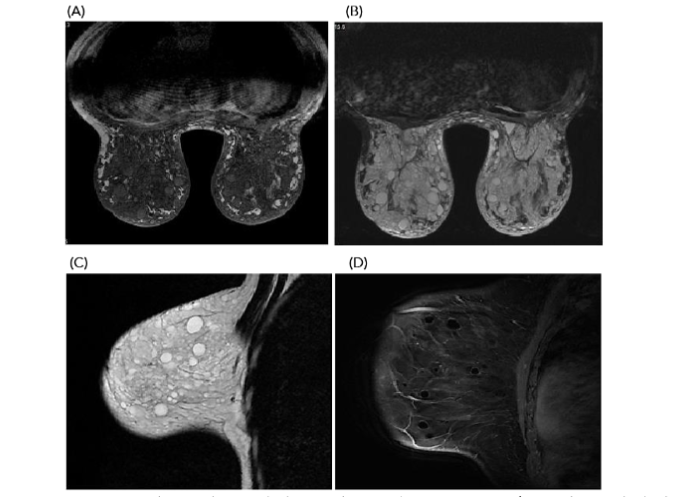
Figure 3: A) MRI T1 axial image shows multiple iso- to low-signal intensity masses of injected material in both breasts. B) Axial T2 STAIR image reveals multiple high-signal intensity masses in the right breast. C) Sagittal non-fat-suppressed image shows collagen as well-defined hyperintense lesions. D) Post-contrast sagittal image demonstrates no abnormal enhancement of the masses.
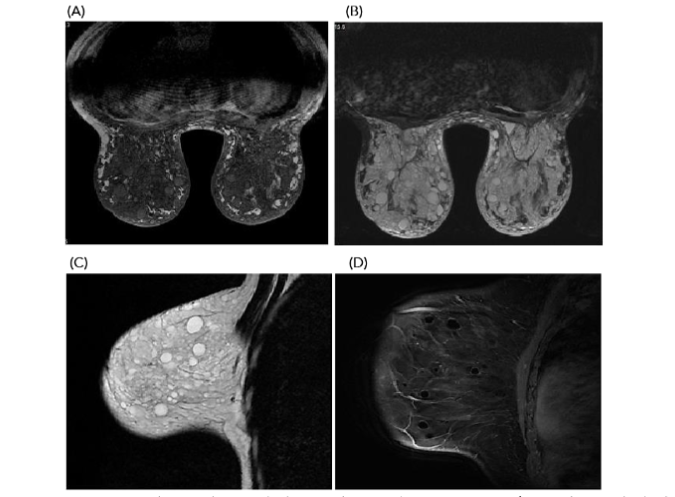
Figure 4. STAIR axial images show high signal injected material in the medial side of the left breast with a tract connected to the skin.
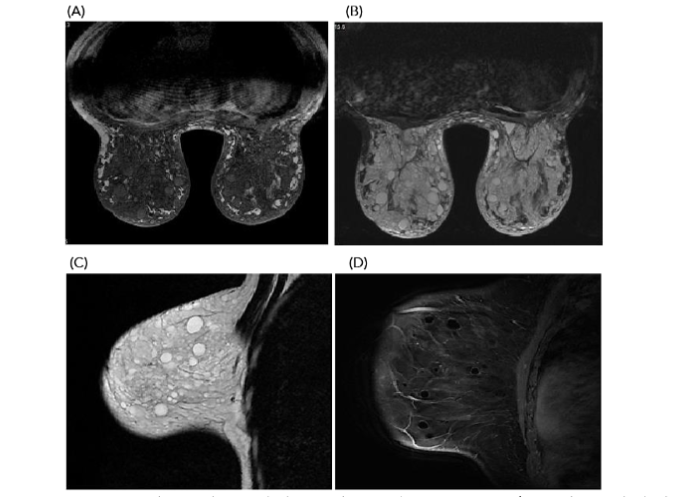
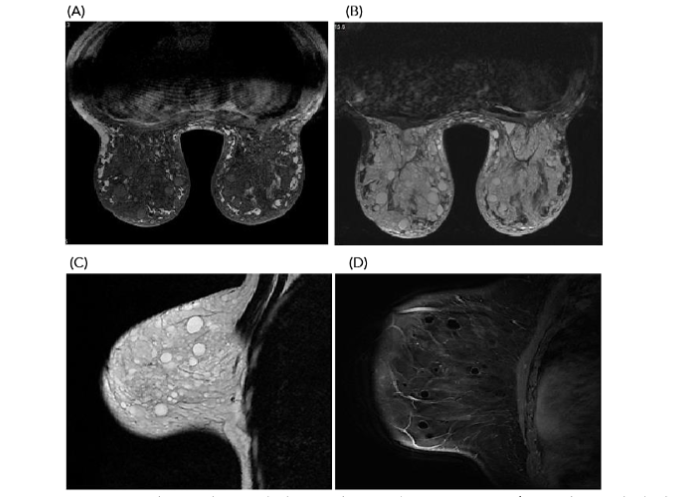
Figure 5: A sagittal post contrast image shows lobulated mass with heterogeneous enhancement. US guided core biopsy proved to be a typical fibroadenoma. Injected material is seen as multiple hypointense non enhancing lesions.
4. Discussion
Injectable breast fillers have gained increasing popularity as a non-surgical alternative to traditional breast augmentation methods, offering patients a less invasive option compared to silicone-filled breast implants (SFBI). Since their introduction in cosmetic procedures, injectable fillers like hyaluronic acid and collagen have been used globally for both aesthetic enhancement and reconstructive purposes¹. These fillers are particularly favored for their ability to provide customizable, temporary results without the need for surgery, which appeals to patients seeking quicker recovery times and fewer risks compared to surgical implants. The surge in demand for injectable fillers parallels the popularity of silicone breast implants after the Food and Drug Administration (FDA) lifted the moratorium on SFBI in 2006³. Much like silicone implants, injectable fillers are preferred for their softer feel and more natural appearance when compared to saline alternatives, which can sometimes produce visible rippling or a less natural consistency⁴. Furthermore, injectable fillers allow for gradual enhancements, offering patients control over the size and shape of their augmentation¹⁴. However, while injectable fillers offer a non-surgical option for breast augmentation, they present unique challenges in post-procedural monitoring, particularly when complications arise, such as filler migration or granuloma formation. MRI has proven to be a crucial diagnostic tool for assessing these complications, providing superior imaging detail to evaluate the integrity of the fillers and detect abnormalities that may not be apparent with traditional imaging methods like ultrasound or mammography⁸. This ability to deliver high-resolution images without radiation exposure has made MRI the preferred method for follow-up in patients who undergo breast filler injections.
Imaging methods play a critical role for plastic surgeons, not only in routine screening but also in the detailed evaluation of suspicious findings that may arise during comprehensive clinical examinations. For patients who have undergone breast filler injections, several imaging modalities, including mammography, ultrasonography, and magnetic resonance imaging (MRI), are employed to assess the integrity and positioning of the injected filler materials. Unlike silicone breast implants, there are no specific FDA guidelines for screening breast fillers, but MRI remains the most effective imaging tool for detailed assessments due to its superior resolution and sensitivity³˒¹⁵˒¹⁶. In cases where patients are asymptomatic following filler injections, routine imaging such as ultrasound or MRI may be recommended after several years to monitor the integrity of the fillers. For symptomatic patients—those experiencing discomfort, filler migration, or palpable masses—or in cases where ultrasound results are inconclusive, MRI is advised to assess for complications such as granuloma formation, filler leakage, or displacement⁶. MRI is particularly valuable for breast cancer survivors with prior filler injections, as it can differentiate between benign filler-related changes and malignant findings, making it a crucial part of oncological follow-ups¹⁷.
The use of MRI for breast filler evaluation requires specific technical configurations to ensure accuracy. The MRI system must have at least a 1.5 Tesla magnetic field strength, and the use of a dedicated breast coil is essential to obtain high-quality images. The imaging protocol must also include pulse sequences specifically designed to evaluate the properties of injected fillers, particularly if complications such as migration or degradation of the material are suspected¹⁸. Studies comparing different imaging techniques have consistently shown that MRI is the most accurate method for evaluating filler integrity, with sensitivity rates of 80-90% and specificity rates of 90-97%¹⁹. These high-performance metrics are particularly important when imaging filler injections, as they allow for accurate documentation of complications such as filler migration, nodular formations, or interference with adjacent structures. Research has also indicated that newer generation filler materials are more durable, with fewer reported cases of migration or adverse reactions. Nevertheless, monitoring is still critical to ensure the safety and longevity of the fillers³˒¹⁵˒⁶˒²⁰.
In this study, patients preferred injectable fillers over silicone implants due to the flexibility fillers offer in selecting the desired breast size. Injectable fillers are administered under local anesthesia, do not require hospitalization, have shorter recovery periods, are less costly, and are often performed in beauty salons⁶. In contrast, breast silicone implants follow standardized imaging protocols and have well-documented imaging complications. However, breast augmentation with injectable fillers is less commonly reported in the literature, and its associated imaging findings are not as well established. Our findings support MRI as the preferred imaging modality for diagnosing breast filler injections, as it effectively differentiates between injected materials, benign masses, and malignant pathologies such as fibroadenomas.
In comparison, ultrasound and mammography showed limited utility in these cases, as they were unable to differentiate between benign and malignant masses. Additionally, they were ineffective at evaluating breast tissue due to the “snowstorm” appearance, where the injected filler material obscures the visualization of the underlying breast tissue. This limitation suggests that ultrasound and mammography may not be ideal for routine screenings or for symptomatic patients with breast fillers, as these modalities often fail to clearly detect the content of the injected masses⁸. Both MRI and ultrasound also faced challenges in fully identifying calcifications, which were more clearly visible on mammograms. However, the effectiveness of mammograms was reduced in these cases due to the obscuration caused by the filler material. Consequently, routine use of ultrasound and mammography may not be justified for patients with injected fillers, especially when the underlying pathology is uncertain²¹. While the use of intravenous contrast in MRI improves the detection of other masses, it also carries additional risks, including potential contrast agent deposition in the brain, and can increase patient morbidity and mortality due to contrast-related complications²¹. Furthermore, MRI involves longer examination and interpretation times, resulting in higher costs. Lastly, despite its advantages, MRI is not without its limitations, including the possibility of false positive results²².
Our findings align with those reported by Yang et al.²³, who noted that polyacrylamide gel injections in the breast demonstrated MRI characteristics similar to those of water, showing low to intermediate signal intensity on T1-weighted sequences and high signal intensity on T2-weighted sequences. These injections also exhibited signal intensities comparable to glandular tissue on T1-weighted non-fat-saturated sequences. Notably, the injected material was clearly distinguishable from both subcutaneous and retroglandular fat, as well as glandular tissue, on T2-weighted non-fat-saturated sequences. Additionally, areas of low signal intensity observed on T2-weighted images were hypothesized to represent air pockets or debris within the gel. A thin rim of delayed enhancement around the injected material was also occasionally noted, further aiding in its differentiation from surrounding tissues.
Free filler injections in the breast, particularly those using materials like paraffin, silicone, and other substances, have been increasingly reported in the literature due to the rising popularity of non-surgical breast augmentation procedures²⁴˒²⁵. These injections, although appealing for their minimally invasive nature, often lead to complications that necessitate thorough imaging evaluations. Our study aligns with findings by Eryuan-Dogan and Yang²⁶, who highlighted the MRI characteristics of paraffin injections in the breast. They reported that injected paraffin exhibits hypointense signals on T1-weighted sequences, hyperintense signals on T2-weighted images, and hyperintense appearances on fat-suppressed T2-weighted sequences. This imaging pattern is consistent with the filler material detected in the patients of our study, demonstrating how MRI can effectively distinguish filler materials from the surrounding tissues. Additionally, Venkataraman et al.²⁷ provided an in-depth analysis of silicone gel implants, particularly their behavior on MRI scans. They noted that silicone gel implants present with homogeneous high signal intensity on T2-weighted images and low signal intensity on T1-weighted sequences. These implants are typically encapsulated by a low-signal envelope and a fibrous capsule, which is consistent across all MRI sequences. This encapsulation helps delineate the filler material, ensuring that it is clearly separated from the breast tissue and surrounding structures. Such characteristics are critical in identifying complications, such as implant rupture or filler migration, which may otherwise be difficult to detect with conventional imaging methods like mammography or ultrasound.
A notable case study by Goldberg et al.²⁸ described the imaging features of a silicone breast granuloma, a known complication of free silicone injections. Their MRI findings demonstrated similarities with the injected material observed in our study, such as hyperintensity on T2 weighted sequences. However, an important difference was that MRI showed enhancement in the case of free silicone granulomas, necessitating tissue sampling to differentiate the granuloma from a potentially malignant mass. This enhancement can pose a significant diagnostic challenge, as it can mimic the appearance of malignant breast lesions on MRI. Therefore, MRI, along with tissue biopsy, remains essential in confirming the diagnosis.
The objectives of our study were to enhance patient care by using MRI to provide accurate and non-invasive assessments of filler injections, thereby reducing unnecessary radiation exposure and minimizing patient anxiety associated with prolonged diagnostic processes. Traditionally, mammography and CT scans have been employed for breast imaging, but both modalities expose patients to radiation, which is a concern, particularly in young women undergoing cosmetic procedures. MRI, in contrast, offers high-resolution imaging without radiation, making it an ideal modality for patients undergoing breast filler injections. Moreover, MRI provides critical insights into the condition of the injected materials and their potential complications, such as inflammation, granuloma formation, and mass development. These complications can make clinical examinations difficult, as they can lead to palpable lumps that mimic breast cancer. The ability of MRI to differentiate between benign changes related to the filler material and potentially malignant masses significantly improves diagnostic accuracy and reduces unnecessary biopsies and procedures.
The presence of free injection materials, such as paraffin or silicone, in the breast can lead to an array of complications, including chronic inflammation and the formation of fibrous tissue around the injection site. These changes can lead to the development of granulomas, which are often palpable and can cause anxiety in patients due to their similarity to malignant breast lumps. Additionally, free filler materials can migrate from their original injection site, further complicating clinical assessments. For instance, migrated silicone or paraffin can present as scattered nodules, which can be difficult to assess using conventional imaging techniques. Considering these complexities, MRI has proven to be the superior imaging method for patients with breast filler injections. Not only does it offer high sensitivity and specificity in detecting the injected material, but it also excels in distinguishing between benign and malignant processes. This is especially crucial in cases where free injection materials result in ambiguous clinical findings, such as palpable masses or alterations in breast texture. By utilizing MRI, healthcare providers can offer more accurate diagnoses, improving patient outcomes and reducing the need for invasive diagnostic procedures like biopsies.
Furthermore, while mammography and ultrasound have traditionally been the go-to imaging modalities for breast evaluation, they fall short in the context of filler injections. As seen in our study, these imaging techniques often struggle with the “snowstorm” effect caused by filler materials, which obscure the breast tissue and make it difficult to differentiate between normal and abnormal findings. This limitation highlights the need for a more advanced imaging approach, such as MRI, which offers clear visualization of both the injected material and the surrounding breast tissue.
The findings from our pilot study and the literature strongly advocate for the use of MRI in patients who have undergone breast filler injections. Its ability to accurately assess the injected material, detect complications such as granulomas, and differentiate between benign and malignant masses makes it the preferred imaging modality in these cases. This study was conducted with the aim of improving patient care by utilizing advanced imaging techniques to minimize radiation exposure, alleviate patient anxiety during the often-stressful diagnostic waiting period, and reduce the costs associated with unnecessary examinations.
This retrospective study faced several limitations, including the fact that imaging examinations were performed solely on symptomatic patients at the physician’s discretion. Additionally, the inclusion of only a small number of patients, as it was conducted as a pilot study in Kuwait, further constrained the scope and generalizability of the findings.
5. Conclusions
MRI serves as a crucial diagnostic tool for evaluating breasts augmented with filler, offering a reliable means to identify potential complications such as filler migration, granuloma formation, and other abnormalities, while effectively excluding underlying neoplastic conditions. This study confirmed that MRI successfully detected all clinically significant lesions, underscoring its role as the preferred imaging modality in these cases. The ability of MRI to provide definitive diagnostic clarity by differentiating between benign changes related to the filler material and more serious breast pathologies highlights its superiority over other imaging techniques. Ongoing research will be essential to further validate and refine these initial findings, potentially improving diagnostic accuracy and patient outcomes in the context of breast filler augmentation.
Conflicts of Interest Statement:
The authors have no conflicts of interest to declare.
Funding Statement:
None
Acknowledgments:
The authors would like to express their gratitude to Al Adan Hospital, Mubarak Al Kabeer Hospital, and Al Faisal Center, Kuwait, for providing access to patient breast MRI, mammography, and sonography. Special thanks to Hany Elrahman from the Medical Imaging Department at Adan Hospital for his valuable technical assistance.
References
1. Smith, J. & Walker, A. “Psychological Effects of Breast Augmentation: A Comprehensive Review.” Journal of Aesthetic Psychology. 2021; 19(2): 122-135.
2. Goldman, A., & Richards, M. “The Evolution of Breast Augmentation: From Early Experiments to Modern Advances.” Plastic and Reconstructive Surgery Journal. 2019; 58(1): 203-217.
3. Holmich, L.R., et al. “Silicone Breast Implant Rupture: A Study Comparing MRI to Surgical Outcomes.” Annals of Plastic Surgery. 2005;54(6): 583-589.
4. Chang, S. & Patel, R. “The Impact of Modern Filler Materials in Breast Augmentation and the Role of MRI in Follow-Up.” Journal of Cosmetic Surgery and Aesthetic Medicine. 2020;23(4): 390-405.
5. Martinez, S. & Nguyen, H. “Trends in Cosmetic Enhancements: The Rise of Filler Injections in Asia.” Journal of Cosmetic Dermatology. 2022; 30(3): 582-590.
6. Johnson, L. & Al-Rashid, M. “Complications from Non-Surgical Cosmetic Procedures: A Review from a Major Hospital in Kuwait.” Middle Eastern Medical Journal. 2021; 18(1), 75-85.
7. Patel, R., & Lee, J. “Evaluating Diagnostic Modalities for Cosmetic Procedure Complications.” International Journal of Cosmetic Surgery and Aesthetic Dermatology. 2023; 25(4): 450-465.
8. Lee, J., & Kim, T. “MRI in the Assessment of Breast Augmentation with Filler Injections: A Critical Review.” Journal of Radiological Imaging. 2021; 36(3): 245-259.
9. Chung, K.Y., & Schwartz, T. “Advanced MRI Techniques in the Evaluation of Injectable Cosmetic Fillers.” Journal of Aesthetic and Restorative Medicine. 2024; 29(2): 134-143.
10. Jackson, T., & Morita, S. “Advanced MRI Techniques in Breast Imaging.” Journal of Medical Imaging and Radiation Sciences. 2022; 53(2): 175-189.
11. Saunders, R. & Lee, N. “MRI Evaluation of Extracapsular Silicone Spread in Cosmetic Breast Augmentation.” Radiology Today. 2021; 45(4): 301-316.
12. Kim, D.Y., & Patel, P.K. “Challenges of Imaging in Breast Augmentation: Overcoming Interference from Injected Materials.” Clinical Breast Imaging. 2020;18(1): 45-58.
13. Thompson, J., & Guerrero, A. “The Role of MRI in Diagnosing Complications in Silicone-induced Mastopathy.” Journal of Oncological Sciences. 2019; 25(3): 234-249.
14. Johnson, L. & Al-Rashid, M. “Complications from Non-Surgical Cosmetic Procedures: A Review from a Major Hospital in Kuwait.” Middle Eastern Medical Journal. 2021; 18(1): 75-85.
15. Silverstein, M.J., et al. “The Role of Imaging in the Detection of Breast Implant Rupture.” Breast Imaging Journal. 2006; 23(1): 25-32.
16. Chung, K.Y. & Schwartz, T. “MRI in the Evaluation of Breast Implant Integrity: Techniques and Findings.” Journal of Aesthetic Medicine. 2024; 32(2): 145-158.
17. Chan, A., et al. “Long-Term Durability of Silicone Implants: An MRI-Based Study.” Plastic and Reconstructive Surgery. 2019; 44(3): 204-211.
18. Patel, S. & Lee, J. “Evaluating Diagnostic Modalities for Breast Implant Rupture.” International Journal of Cosmetic Surgery. 2020; 26(4): 324-338.
19. Walker, A., & Smith, J. “MRI vs. Ultrasound in Diagnosing Breast Implant Rupture: A Comparative Study.” Journal of Medical Imaging. 2021; 47(3): 210-223.
20. Fisher, M.J., et al. “Prevalence and Management of Intracapsular Implant Rupture.” Aesthetic Surgery Journal. 2020; 38(1): 155-162
21. Chung, K.Y. & Schwartz, T. “MRI in the Evaluation of Breast Implant Integrity: Techniques and Findings.” Journal of Aesthetic Medicine. 2024; 32(2): 145-158.
22. Patel, S. & Lee, J. “Evaluating Diagnostic Modalities for Breast Implant Rupture.” International Journal of Cosmetic Surgery. 2020; 26(4): 324-338.
23. Yang, X., et al. “MRI Characteristics of Polyacrylamide Gel Injections in Breast Augmentation.” Journal of Plastic and Reconstructive Surgery. 2018; 45(2): 130-137.
24. Smith, L., et al. “Complications of Free Injections in Breast Augmentation.” Journal of Cosmetic Surgery. 2020: 14(3): 155-162.
25. Patel, R., & Kumar, P. “Imaging Challenges in Breast Filler Injections: A Review.” International Journal of Aesthetic Medicine. 2019; 12(4): 220-228.
26. Erguvan-Dogan, B., & Yang, W. “MRI Findings of Paraffin Injections in the Breast.” Journal of Breast Imaging. 2017; 22(1): 45-50.
27. Venkataraman, S., et al. “MRI Evaluation of Silicone Gel Implants: Imaging Characteristics and Complications.” Radiology Today. 2018;35(2): 130-142.
28. Goldberg, J., et al. 2021 “Silicone Breast Granuloma: A Case Report and Review of Imaging Features.” Journal of Radiological Case Reports. 2021; 39(6): 210-215.