





Hodgkin Lymphoma: Diagnosis and Treatment Insights
Hodgkin Lymphoma: Diagnostic and Therapeutic Approach
Ovilla Martínez Roberto 1, De la Peña Celaya José Antonio 2, Harnández Ruíz Eleazar 2, Pérez Zincer Fernando 1, Ramírez Muñiz Nishalle 1 and Alvarado Ibarra Martha.1,3,*
- Hematology Hospital Angeles Lomas
- Centro Médico Nacional “20 de noviembre ISSSTE
- Correspondence: Alvarado Ibarra Martha Hematology. Hospital Angeles Lomas. Vialidad de la Barranca s/n Hacienda de las Palmas CP 52763 Huixquilucan México. Tel 5552465000 extensión 1003.
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Roberto, OM., Antonio, DPCJ., et al., 2024. Hodgkin Lymphoma: Diagnostic and Therapeutic Approach. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5751
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5751
ISSN 2375-1924
ABSTRACT
Hodgkin Lymphoma is a malignant neoplasm derived from B cells, it corresponds to 10% of hematological neoplasms and has the best prognosis among lymphoid malignancies. About 80-90% of Hodgkin Lymphoma can be cured with the first line of treatment. An inflammatory microenvironment with at least 1% neoplastic cells (Reed-Sternberg cells and their variants) is observed in the architecture of the node. Its incidence is estimated at 1 case/100,000/inhabitants per year and a mortality of 0.7 per individuals/100,000 inhabitants per year. It characteristically has a bimodal presentation and has a close relationship with EBV as the etiological agent in 45% of cases. Historically, the AVBD regimen has been considered the standard treatment regimen; however, management with anti-CD30 in the first line may be a therapeutic option. In our review we describe the usefulness of adequate stratification, use of interim-PET to avoid overtreating or undertreating patients, as well as PET-CT at the end of treatment to omit the need for radiotherapy and thereby reduce the risk of chronic toxicities. It is of utmost importance that in the evaluation at the end of treatment in cases of treatment with immunotherapy, consider pseudoprogression based on the LYRYC criteria with the need for PET-Ct 3 months later to consider or rule out pseudoprogression. Historically, the ABVD or BEACOPP Scheme have been the treatment standards, however with immunotherapy with Brentuximab and checkpoint inhibitors such as nivolumab or pembrolizumab either with first-line regimens such as BV + AVD or nivolumab +AVD or pembrolizumab or in Rescue schemes have revolutionized the natural history of Hodgkin’s disease, improving disease-free and overall survival, reducing the risk of chronic toxicity presented with traditional schemes.
Keywords: Reed Sternberg, Immunohistochemistry, Brentuximab, Chemotherapy, Deauville.
Introduction
Hodgkin lymphoma (HL) was first described in 1832, the etiology was unknown for a long time but the last two decades the nature of B cells and their pathognomonic form called Reed-Sternberg Cells (CRS) have been revealed along with several recurrent genetic lesions and the pathogenic role of Epstein-Barr virus infection. CRS in classical Hodgkin lymphoma have several characteristics that are unusual for lymphoid tumor cells, and the microenvironment of Hodgkin lymphoma in that it is dominated by an extensive mixed potentially inflammatory cellular infiltrate.
Reed-Sternberg cells are derived from central germinal center B cells that have acquired immunoglobulin variable chain gene mutations, the cause is unknown, but genetic susceptibility and environmental associations are involved (for example: occupations such as carpentry, history of treatment with phenytoin, radiotherapy or chemotherapy, infections by Epstein-Barr virus, Mycobacterium tuberculosis, herpes virus type 6 and HIV), the risk is slightly increased in individuals with certain types of immunosuppression (e.g. transplant patients receiving immunosuppressants), patients with congenital immunodeficiency disorders (e.g. ataxia telangiectasia syndrome, Klinefelter syndrome, Chédiak Higashi syndrome and Wiskott Aldrich syndrome) and those with certain autoimmune disorders (rheumatoid arthritis, celiac disease, Sjögren’s syndrome and systemic lupus erythematosus).
According to the WHO classification HL is divided into 2 histopathological subtypes: Classic (95% of cases) and nodular lymphocytic predominance (5% of cases); Can be subclassified into Nodular Sclerosis 40-75%, Mixed Cellularity 20-40%, Lymphocyte Depletion 5-15%, Lymphocyte Rich 5-15%. Multiple signaling pathways and transcription factors have been found that show dysregulated activity in CRSs, including nuclear factor κB, Jak, Stat, PI3K, Akt, Erk, AP1, and tyrosine kinases. CRS attract many cells to the lymphoma tissue, resulting in a typical inflammatory microenvironment, this altered environment probably promotes the survival of malignant cells that escape the attack of cytotoxic T or Natural Killer cells.
Objective
The authors have attempted to provide updated information that can be useful to new generations of doctors and quick consultation for many colleagues.
Staging
According to the Ann Arbor classification, B symptoms are defined as the presence of any of the following: fever >38.3ºC, weight loss and nocturnal diaphoresis. The classification criteria were established at the 11th International Malignant Lymphoma Conference in Lugano, Switzerland; held in June 2011, at this expert meeting, positron emission tomography (PET) with 18-fluorodeoxyglucose (FDG) was formally incorporated into the staging of FDG-avid lymphomas, including Hodgkin lymphoma, at the aforementioned conference, the previous Ann Arbor classification was modified, leaving the suffixes A and B (symptoms) only to HL. The response to treatment will be assessed by PET using the 5-point scale, likewise, the product of the perpendicular diameters of a single nodule can be used to identify disease progression.
The recommendations of the Costwold meeting were that computed tomography be included as the technique for evaluating intrathoracic and infradiaphragmatic nodules, the criteria for spleen and liver involvement were modified, and that alterations in the hepatic function tests should be ignored. The suffix X was introduced at this meeting to define bulky disease (>10cm), finally, the category of Uncertain Complete Response was created in patients with persistent radiological alterations, although with uncertain clinical significance, likewise, the ominous nature of the voluminous disease was evident, establishing that lymph nodes with a diameter greater than 2.5 cm are considered abnormal in a tomographic sections that must be 1 cm.
The suffix E is used in the clinical classification when the extranodal involvement is contiguous or proximal to the nodal lesion. To be considered a voluminous mass, the isolated nodule or conglomerate must exceed 10cm in diameter, the size of lesions in the spleen or liver should not be used for prognostic purposes. In the mediastinum, the definition of voluminous is given when the mass exceeds or is equal to one third of the transverse diameter at the T5/6 level.
NODAL DISEASE:
- Stage I: Involvement of a single region or nodal structure such as the spleen, thymus, or Waldeyer’s ring.
- Stage II: Involvement of 2 or more nodal regions on the same side of the diaphragm. Hilar nodes should be considered “lateralized”; Therefore, when both sides are involved, it constitutes stage II. The number of affected anatomical regions should be indicated with a signed (i.e., II3).
- Stage III: Involvement of nodal regions or lymphoid structures on both sides of the diaphragm.
Use of PET/CT
In accordance with the work at the Fourth International Workshop on PET in Lymphoma in the city of Menton, France, guidelines have been established for staging and assessment of the response in FDG-avid lymphomas. The five-point scale was proposed and recommended at the First International Workshop on PET in Lymphoma (Deauville, France). In this work the criteria for the use of PET in the clinical context of lymphomas (including HL) and late-phase trials were established. This classification does not have good sensitivity for central nervous system infiltration, so magnetic resonance is preferred in case of suspected infiltration at that level. The intensity of the uptake is reported according to the SUV (standardized uptake value) scale. Deauville’s 5-point score is as set out in the table 1.
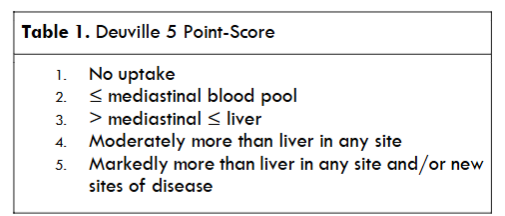
Scores 1 and 2 are considered complete metabolic response (CMR), while a score of 3 is considered CMR only in intermediate PET. In interim PET (PETi) scores of 4 and 5 are considered a partial metabolic response although in PET at the end of treatment it is considered residual metabolic disease. The purpose of the PETi is to ensure the effectiveness of the treatment by excluding the possibility of progression and to determine the escalation or reduction of chemotherapy doses, this because the metabolic response (shown by PET) is earlier than the anatomical response. It has been shown that the PETi exceeds the prognostic value of the IPS (International Prognostic Index), the negative predictive value for PETi is 95% in HL that translate as ≥ 2 years of Progression-Free Survival (PFS), with an acceptable Positive Productive Value (PPV), with PFS of 13% to 27%. Hepatic FDG uptake may be influenced by glycemic and insulin levels, on the other hand, uptake in BM and spleen would be affected by chemotherapy or use of colony-stimulating factor in granulocytes.
PET will be performed at least 3 weeks after the last application of chemotherapy although preferably after 6 to 8 weeks, 2 weeks after the use of granulocyte colony stimulating factor, and 3 months after radiotherapy is completed.
PET at the end of treatment.
PET for assessment of remission at the end of treatment has high precision, it has been reported after ABVD and BEACOPP schemes in advanced HL. In recent years the contribution of PET-CT in the evaluation of response has made it possible to identify a group of patients with an excellent prognosis in whom it is feasible to omit radiotherapy (RT), however it must be taken into account that the correct interpretation of an interim or evaluation PET-CT at the end of treatment is necessary for this.
Such evaluation is based on the 5-point Deauville visual scale described above which considers:
- Complete metabolic response (CMR) Score 1, 2 and 3 in nodal or extra-nodal sites with or without residual mass by PET.
- Partial metabolic response (PMR) Persistence of metabolic lesions, but with lower metabolism compared to baseline.
- No metabolic response (SRM) Score 4 and 5 without changes with respect to the baseline PET, either in the interim PET or PET at the end of treatment.
- Progressive metabolic disease (PMD) Score 4 and 5 with increased uptake compared to baseline PET.
This should be considered for both interim PET and end-of-treatment PET. Score 3 means good response and good prognosis in most patients, however, in those protocols that use PET to de-escalate treatment a score of 3 may be inadequate to avoid ineffective treatment reductions.
Interim PET/CT has taken particular importance and relevance due to what was evidenced in the RATHL trial where there was upward re-staging according to PET, compared to CT and bone marrow biopsy. Follow-up of discrepant results confirmed the PET-CT findings in the majority of patients. Which indicates the superiority of PET/CT with respect to CT and bone marrow biopsy.
Brentuximab Vedotin (BV).
Brentuximab vedotin (BV) is a chimeric IgG1 conjugated antibody directed against CD30 that is covalently linked to the microtubule-disrupting agent monomethyl auristatin E; BV alone achieves ORR of 75% with CR of 34% in previously treated patients. Prior to the O’Connor study, BV was approved only after ASCT or disease refractory to ≥ 2 lines of treatment. O’Connor et al evaluated the safety and activity of the BV/Bendamustine combination in patients previously treated with R/R HL and anaplastic large T cell lymphoma, the authors carried out an international multicenter phase 1-2 study concluding that the dose of BV to be administered would be 1.8 mg/kg and 90 mg/m2 of bendamustine to be applied every 3 weeks. With this, an ORR of 78% (95% CI, 62-91) was achieved. Adverse events were grade 3 pneumonia and grade 3-4 neutropenia in 14% and 25%, respectively.
The authors evaluated the combination of BV/B in a phase 1-2 study in R/R HLH after first-line treatment. In a total of 55 patients with a median age of 36 years, 50.9% were primarily refractory and 49.1% relapsed, they were administered at least 2 cycles before autologous hematopoietic stem cells transplant (AutoHSCT), whether or not the transplant was performed, patients could receive a total of 16 cycles of BV monotherapy, the observed ORR was 92.5% and 73.6% of CR.
On the other hand, in the AETHERA trial, BV was studied as a consolidation option in patients with cHL at high risk of relapse or progression after AutoHSCT. The dose of BV was 1.8 mg/kg every 3 weeks for up to 16 applications. The benefit of BV continued to be shown at 5 years with a PFS of 59% in BV vs 41% with placebo, the stipulated risk factors were: relapse in less than 12 months or refractoriness to initial treatment, the best response was partial or stable disease to the last line of treatment, extranodal disease to relapse prior to AutoHSCT, or ≥2 rescue treatments. In patients with two or more risk factors within the BV group, PFS was better than in the placebo group (HR of 0.424, with 95% CI of 0.30-0.59. BV has also been combined with schemes such as DHAP, ESHAP (in this case with global response of 96% and a CR of 70%).
Table 2. Standardized treatment regimens for Hodgkin lymphoma.
| Chemotherapy | Doses | Administration Time |
|---|---|---|
| ABVD | Doxorubicin 25 mg/m2 intravenous 1 y 15 days Bleomicine 10 U/m2 intravenous 1 y 15 days Vinblastine 6 mg/m2 intravenous 1 y 15 days Dacarabazine 375 mg/m2 intravenous 1 y 15 days |
|
| BEACOPP | Bleomicine 10 U/m2 intravenous 8 day Etopóside 200 mg/m2 intravenous 1 a 3 days Doxorubicin 35 mg/m2 intravenous 1 day Ciclophosphamide 1250 mg/m2 intravenous 1 day Vincristine 1.4 mg/m2 B intravenous 8 day Procarbazine 100 mg/m2 oral 1-7 Prednisone 40 mg/m2 oral 1-14 FEC-G 300 mcg Subcutaneos From 8 day |
|
| Stanford V | Mecloretamina 6 mg/m2 intravenous weeks 1 y 5 Doxorubicin 25 mg/m2 intravenous weeks 1, 3, 5 y 7 Vinblastine 6 mg/m2 intravenous weeks 1, 3, 5 y 7 Vincristine 1.4 mg/m2 intravenous Weeks 2, 4, 6 y 8 Bleomicine 5 U/m2 intravenous weeks 2, 4, 6 y 8 Etopóside 60 mg/m2 intravenous weeks 3 y 7 Prednisone 40 mg/m2 Oral weeks 1-6 |
In one study, the authors evaluated the clinical efficacy of BV as first line in combination with standard or modified treatment in HL, the inclusion requirements were: recently diagnosed HL, CD 30 positive, with clinical stage IIAx or IIB-IV and ECOG ≤ 2. The primary objective was to evaluate safety and establish the maximum tolerated dose. 95% of patients with the BV + ABVD combination achieved CR, while 96% of the BV + AVD group did so as well, In the first group, 44% presented pulmonary toxicity, which did not occur in any of the BV + AVD patients, despite 45% having stage IV and 25% having an IPS score of 4 or more. Another point in favor of the scheme was that PETi (after the 2nd cycle) was negative in 96% of patients compared to 70-85% reported in the literature for conventional ABVD, in this BV + treatment combination, the dose used of Brentuximab Vedotin the dose used was 1.2 mg/kg 2 doses per cycle unlike the monotherapy regimen at a dose of 1.8 mg/kg.
ECHELON-1 trial showed better PFS in A+ AVD group, compared to ABVD in classic HL stages III and IV. It was a global study with 39% patients from North America (Canada and the United States), 50% from Europe and 11% from Asia, patients with classic HL with ECOG ≤2. 250 patients were compared in the A + AVD group and 247 in the ABVD group. A PFS with HR of 0.60 (P=.012) was observed in those who received A+ AVD. Regarding adverse effects, febrile neutropenia was observed in 20% of A+ AVD and 9% of ABVD, peripheral neuropathy 80% vs 56% in the control group, however, pulmonary toxicity was lower in A+AVD (only 3%) than in ABVD.
In the ECHELON-1 study, the combination of BV with AVD omitting bleomycin achieved CR in 95% (45/47 patients). BV was observed to exacerbate the toxicity caused by bleomycin when combined with ABVD; concluding that BV should not be combined with bleomycin. On the other hand, the concomitant use of RT to the mediastinum for bulky disease and previous BV did not increase the risk of pulmonary toxicity.
Radiotherapy
In a multicenter randomized study with patients diagnosed with early-stage HL and a favorable prognosis 4 groups of 2 different intensities of chemotherapy and 2 different doses of RT were established:
- Group 1: ABVD 4 cycles + 30Gy of RT.
- Group 2: ABVD 4 cycles + 20Gy of RT.
- Group 3: ABVD 2 cycles + 30Gy of RT.
- Group 4: ABVD 2 cycles + 20Gy of RT.
The two doses of chemotherapy, showed no significant difference for treatment failure-free survival (TFS) (p= 0.39) or OS (p=0.61). At 5 years, the TFS was 93% (95% CI, 90.5 to 94.8) with the use of 4 cycles and 91.1% with only 2 cycles (95% CI, 88.3-93.2), on the contrary, toxicity and adverse events were more common in those who received 4 cycles of chemotherapy and 30Gy of RT. This toxicity associated with radiotherapy may be reduced in the assessments that PET at the end of treatment achieves a Deauville 1 or 2 response and radiation can be omitted.
Rescue Treatment
Up to 30% of patients initially treated for HL will experience relapse. These patients will be receiving a second line treatment, and in case of response they will be candidates for autologous transplant as a curative attempt. Second-line therapies can achieve CR in HL prior to AutoHSCT from 17% to 76%, in fact, the CR rate with the different second line schemes range from 20 to 60%. The depth of the response is relevant, because it has been shown that achieving CR prior to transplantation is a predictor of favorable prognosis. Bendamustine + regimen based on gemcitabine and vinorelbine has been used to achieve this gold. This last scheme shows an OR of 83% and CR of 73%, with a 2-year PFS of 62.2% in the general population and 80.8% in transplant patients.
Treatment of Relapsed or Refractory Disease
15% to 25% of patients with classic HL will fail first-line treatment. 50% of patients may be cured after AutoHSCT, although the majority with unfavorable prognostic factors (relapse in less than 12 months or refractoriness to initial treatment, best response partial or stable disease to the last line of treatment, extranodal disease at relapse prior to AutoHSCT, or ≥2 prior rescue treatments) will progress after transplantation with a poor prognosis, in these patients with R/R after AutoHSCT the median OS is 2.4 years and 1.2 years if the relapse is less than 1 year after transplant. In other work was included 102 patients in a phase II HL R/R study after ASCT using BV, a maximum of 16 cycles were administered at doses of 1.8 mg/kg every 3 weeks. The objective overall response was 75% with CR in 34% of patients, the median PFS was 5.6 months, and 20.5 months in CR. Other regimens available as rescue options in classic HL relapse are anti-PDL1 drugs such as Nivolumab or pembrolizumab with adequate responses and toxicity profile.
Long-Term Prognosis
This type of lymphoma presents a second peak of presentation in patients over 60 years of age; HL presents worse evolution with usual regimens. The biology of HL differs in older patients, with the MC variety being more common in patients > 60 years of age, in addition to greater EBV positivity, with the consequent greater risk of fatal outcomes. Likewise, the presence of other comorbidities, mainly cardiac, affect the prognosis of HL and the use of usual regimens, patients in this age group have less PFS (48% vs 74%), and worse OS (58% vs 90%).
In women previously treated with thoracic RT for HL there is an increased risk of breast cancer, which ranges from 5 to 20 times higher compared to the general population. At 40 years, the cumulative incidence of breast cancer in this population is 30-40%, this high incidence is similar to that of BCRA1/2 mutation carriers.
It is considered that the risk of breast cancer due to RT in LH is modified by radiotherapy dose and radiated volume, the age at the time of exposure to RT, inversely proportional to the risk of cancer, as well as premature menopause induced by alkylating agents. In other work they analyzed genes associated with interaction with radiation or risk of breast cancer in 327 patients with breast cancer after RT for HL and 4,671 patients with primary breast cancer. Patients in the highest decile of the RT-interaction-PRS (polygenic risk score) presented a risk 1.6 times higher than those in the lowest decile, in PRS breast cancer the risk was 4 times higher in patients within the highest decile compared to the lowest, therefore, susceptibility to breast cancer in HL survivors would be influenced by genetic factors inherent to the patients.
Hodgkin Lymphoma and HIV
Approximately 10 to 30% of classic HL/HIV patients will relapse after CR, in these cases, second line CT and subsequent ASCT are also indicated with good outcomes in 30 to 65% of cases. In case of relapse or refractoriness after AutoHSCT rescue and allogeneic transplant with reduced conditioning will be chosen, despite the above, the mortality associated with Allogenic HSCT in HL/HIV is 20%, with 2-year survival of 50%. Regarding BV, a study evaluated the safety of the BV-AVD scheme in HIV patients with cHL, those patients who required the use of antiretrovirals with strong inhibition of CYP3A4 were excluded. There was negativity in 5/6 patients in the PETi and in 6/6 in the final PET. PFS was 100% at 25 months of follow-up. The levels of CD4+ lymphocytes and viral load were not affected during treatment, with even improvement in 4/5 patients after the second cycle. Regarding adverse effects, there was no significant difference with respect to HIV-negative patients. Others researchers have demonstrated a transient negativization of the HIV-1 RNA partially explained in that there is a linear correlation between the increase in the levels of Plasma HIV-1 RNA and clinical stage with soluble CD30 levels; Reporting that signaling through CD30 increases the transcriptional activity of HIV-1, when CD30 is inhibited, there would be a decrease in viral transcription.
Despite the favorable responses of BV in HL/HIV patients, there is a theoretical increased risk of progressive multifocal leukoencephalopathy in this population with the use of BV. The usual presentation of this side effect is weeks after the last exposure to BV taking into account the above, the eligibility criteria in HL/HIV patients for BV should perhaps be:
- CD4 > 50 cells/μL.
- Active HAART therapy.
- Brain MRI prior to treatment.
Acceptable results have also been obtained with check point inhibitors such as nivolumab and pembrolizumab in this population.
Immunotherapy
Programmed cell death protein (PD-1) is an important immune response receptor expressed on T cells. PD-1 binds to its ligand (PD-L1 or PD-L2) on tumor cells and in their microenvironment, promoting tolerance to tumor evasion which facilitates tumor growth; therefore, this protein is important in the sense that it can be a target to restore antitumor immunity. Regarding RR classic LH, the FDA has approved the use of nivolumab or pembrolizumab due to high response rates, its activity is explained by the fact that Reed-Sternberg cells overexpress PD-L1/PD-L2, in addition to silencing the expression of the major histocompatibility complex (MCH). In patients with classic HL, PD-1 is found at higher levels both in lymphoma-infiltrating T lymphocytes and in peripheral blood, compared to healthy people and in patients with B-cell non-Hodgkin lymphoma. Most patients with classic HL presents an amplification of 9q24.1, which causes strong expression of PD-L1/PD-L2. The most common 9q24.1 abnormalities are copy number gain (58%), amplification (35%) and polysomy (5%), which can be detected in almost all patients with classic HL by FISH.
In a group of 23 patients with RR classic HL, nivolumab achieve an OR of 87% and CR of 17%. 35% of patients had a response duration of up to 1.5 years.
On the other hand, pembrolizumab showed an OR of 65% and CR of 16% in 31 patients with RR classic HL, with a PFS of 11.4 months.
In the phase 2 study, 243 patients with RR classic HL were exposed to nivolumab, who had relapsed after AutoHSCT, ORR was 69% with complete response of 19%, with a PFS of 12 to 18 months. PD-L1/PD-L2 amplification was associated with a high response rate to nivolumab and pembrolizumab.
Regarding pembrolizumab, reported that in 210 RR classic LH patients, an OR of 69% and CR of 22%. The adverse effects of both agents are diarrhea, skin rash, pruritus, infusion reaction, asthenia and dysthyroidism, although only 4-6% of patients have had to discontinue treatment; Other frequent phenomena when using anti-PDL1 are immunological phenomena.
On the other hand, nivolumab may present a phenomenon classified as pseudoprogression, the majority of this small subgroup showed a stable reduction in tumor burden, this increase in the size of the lesions is explained by therapeutic immune activation or a delayed immune response to treatment, due to the above, this pseudoprogression has been classified as indeterminate response in the recent modifications of the Lugano classification in the immunotherapy; recommending a reevaluation of the case in 3 months to confirm or rule out true progression and use of the immunotherapy criteria for response evaluation. In patients treated after allogeneic transplant, the ORR was 95% for nivolumab as monotherapy and CR 42%, with 1-year PFS of 58% and 79% OS.
The combination of nivolumab and brentuximab as first line presents an ORR of 82% and CR of 61%. However, the responses were favorable, 44% of patients experienced grade 1-2 infusion reactions and 84% of patients experienced immune-related adverse events, although only 8% required the use of systemic steroids.
These responses are better than those observed in traditional schemes, even superior to the response of BV-AVD.
Finally, dual immunotherapy by combining PD-1 and CTLA-4 blockade has also been studied in RR classic HL with 29% of patients with grade 3 adverse effects and 8% having to discontinue treatment.
The 5-year PFS in patients with early stages of classic HL classified as unfavorable risk is 80 to 85%. This was documented in a multicenter study evaluating the safety and efficacy of BV and AVD, with radiotherapy as consolidation (30Gy) to the involved field. Patients were treated with 4 cycles of A +AVD, those who achieved CR by PET (Deauville 1-3) would receive RT at the aforementioned dose. AEs ≥ 3 were observed in 4 patients (severe febrile neutropenia, peripheral neuropathy and hypertension). Negative PET was achieved in 93% of patients after 4 cycles. The patients who underwent the 4 cycles A+AVD and Rt had CR, with a 1-year PFS of 93.3%. The authors conclude a good response even in patients with high tumor burden. The adverse effects reported were severe febrile neutropenia in 53% of patients, peripheral neuropathy in 40%. No patient presented significant pulmonary toxicity (grade 2 or greater).
The response to retreatment with BV was assessed in patients with classic HL who had previously been exposed to the drug in question and had presented a minimal partial response. The global response was 60% with 30% achieving a complete response and a duration of 9.5 months. AEs had the same incidence, except for peripheral neuropathy which showed a cumulative effect.
The authors inquired about the preferences of patients and treating physicians regarding the different HL regimens. The schemes evaluated were ABVD, BEACOPP and BV-AVD. In the 3 countries in which the survey was carried out (United Kingdom, France and Germany), the possibility of pulmonary toxicity significantly affected the decision of which regimen to use, it was evident that physicians prefer better OS over PFS, while the opposite occurs in patients. Therefore, patients would usually prefer a more toxic treatment, although with greater chances of success.
Acknowledgments:
None
Conflicts Of Interest:
The authors declare that there are no conflicts of interest.
References
- Ralf Küppers, Klaus Rajewsky. The origin of Hodgkin and Reed/Sternberg Cells in Hodgkin Disease. Annu Rev Immunol.1998;16: 471-93
- Küppers, R. The biology of Hodgkin lymphoma Nat Rev Canc.2009;9(1):15–27
- Ansell SM. Hodgkin Lymphoma: Diagnosis and Treatment. Mayo Clin Proc.2015;90(11):1574-1583.
- Eichenauer DA, Aleman BMP, André M, Federico M, Hutchings M, Illidge et al. Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol.2018;29(Suppl 4):iv19-iv29.
- Lister T, Crowther D, Sutcliffe S, Glatsteins E, Canellos G, Young R. Report of a Committee convened to discuss the evaluation and staging of patients with Hodgkin’s disease: Cotswolds meeting. J Clin Oncol 1989;7(11):1630-6
- Swerdlow SH, Campo E, Pileri SA, Lee Harris N, Stein Harald, Siebert Reiner et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375-2390.
- Barrington SF, Kirkwood AA, Franceschetto A, Fulham M, Roberts T, Almquist H. et al. PET-CT for staging and early response: results from the Response-Adapted Therapy in Advanced Hodgkin Lymphoma study. Blood. 2016;127(12):1531-1538
- Barrington SF, Mikhaeel NG, Kostakoglu L, Meignan M, Hutchings M, Müller S. et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J Clin Oncol. 2014;32(27):3048-3058.
- Advani RH, Hoppe RT, Baer D, Advani RH, Hoppe RT, Baer D, et al. Efficacy of abbreviated Stanford V chemotherapy and involved-field radiotherapy in early-stage Hodgkin lymphoma: mature results of the G4 trial. Ann Oncol. 2013;24(4):1044-1048.
- Gordon LI, Hong F, Richard I, Fisher RI, Bartlett L, Connors JM. et al. Randomized Phase III Trial of ABVD Versus Stanford V with or Without Radiation Therapy in Locally Extensive and Advanced-Stage Hodgkin Lymphoma: An Intergroup Study Coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol. 2013;31(6):684-691.
- Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-68
- O’Connor OA, Lue JK, Sawas A, Amengual J, Deng Ch, Kalac M. et al. Brentuximab vedotin plus bendamustine in relapsed or refractory Hodgkin’s lymphoma: an international, multicentre, single-arm, phase 1–2 trial. Lancet Oncol. 2018;19(2):257-266.
- Connors JM, Ansell SM, Fanale M, Park SI, Younes A. Five-year follow-up of brentuximab vedotin combined with ABVD or AVD for advanced-stage classical Hodgkin lymphoma. Blood. 2017;130(11):1375-1377.
- LaCasce AS, Bociek RG, Sawas A, Caimi P, Agura E, Matous J. et al. Brentuximab vedotin plus bendamustine: a highly active first salvage regimen for relapsed or refractory Hodgkin lymphoma. Blood.2018;132(1):40-48
- Moskowitz CH, Walewski J, Nademanee A, Masszi T, Agura E, Holowiecki J. et al. Five-year PFS from the AETHERA trial of brentuximab vedotin for Hodgkin lymphoma at high risk of progression or relapse. Blood. 2018;132(25):2639-2642.
- Herrera AF, Palmer J, Martin P, Armenian S, Tsai N, Kennedy N. et al. Autologous stem-cell transplantation after second-line brentuximab vedotin in relapsed or refractory Hodgkin lymphoma. Ann Oncol. 2018;29(3):724-730
- Vitolo U, Chiappella A. Salvage regimens for Hodgkin’s lymphoma in the brentuximab vedotin era. Lancet Oncol. 2018;19(2):162-163
- Younes A, Gopal AK, Smith SE, Ansell S, Rosenblatt J, Savage K. et al. Results of a Pivotal Phase II Study of Brentuximab Vedotin for Patients with Relapsed or Refractory Hodgkin’s Lymphoma. J Clin Oncol.2012;30(18):2183-2189
- Moskowitz AJ, Schöder H, Yahalom J, McCall S, Fox SY, Gerecitano J. et al. PET-adapted sequential salvage therapy with brentuximab vedotin followed by augmented ifosfamide, carboplatin and etoposide for patients with relapsed and refractory Hodgkin’s lymphoma: a non-randomised, open-label, single-centre, phase 2 study. Lancet Oncol. 2015;16(3):284-292
- Younes A, Connors JM, Park SI, Fanale M, O´Meara M, Hunder N. et al. Brentuximab vedotin combined with ABVD or AVD for patients with newly diagnosed Hodgkin’s lymphoma: a phase 1, open-label, dose-escalation study. Lancet Oncol. 2013;14(13):1348-1356
- Engert A, Plûtschow A, Eich A, Lohri A, Dörken B, Borchmann P. et al. Reduced Treatment Intensity in Patients with Early-Stage Hodgkin’s Lymphoma. N Engl J Med. 2010; 2;363(7):640-52
- Forero-Torres A, Holkova B, Goldschmidt J, Chen R, Olsen G, Boccia R. et al. Phase 2 study of frontline brentuximab vedotin monotherapy in Hodgkin lymphoma patients aged 60 years and older. Blood. 2015;126(26):2798-2804.
- Opstal-van Winden AWJ, de Haan HG, Hauptmann M, Schmidt Marjanka, Broeks A, Russell N. et al. Genetic susceptibility to radiation-induced breast cancer after Hodgkin lymphoma. Blood.2019;133(10):1130-1139
- Re A, Cattaneo C, Rossi G. HIV and lymphoma from epidemiology to clinical management. Mediterr J Hematol Infect Dis. 2019;11(1): e2019004
- Rubinstein PG, Moore PC, Rudek MA, Henry D, Ramos JC, Ratner L. et al. Brentuximab vedotin with AVD shows safety, in the absence of strong CYP3A4 inhibitors, in newly diagnosed HIV associated Hodgkin lymphoma. AIDS.2018;32(5):605-611
- Wang C-C, Thanh C, Gibson EA, Burack M, Hogan L, Descours B. et al. Transient loss of detectable HIV-1 RNA following brentuximab vedotin anti-CD30 therapy for Hodgkin lymphoma. Blood Adv.2018;2(23):3479-3482.
- Gandhi M, Petrich A. Brentuximab Vedotin in Patients With Relapsed HIV-Related Lymphoma. J Natl Compr Canc Net.2014;12(1):16-19.
- Ramchandren R, Advani RH, Ansell S, Bartlett N, Chen R, Connors J. et al. Brentuximab Vedotin plus Chemotherapy in North American Subjects with Newly Diagnosed Stage III or IV Hodgkin Lymphoma. Clin Cancer Res. 2019;25(6):1718-1726.
- Hu B, Jacobs R, Ghosh N. Checkpoint Inhibitors Hodgkin Lymphoma and Non-Hodgkin Lymphoma. Curr Hematol Malig Rep. 2018;13(6):543-554.
- Kumar A, Casulo C, Yahalom J, Schöder H, Barr P, Caron P. et al. Brentuximab vedotin and AVD followed by involved-site radiotherapy in early stage, unfavorable risk Hodgkin lymphoma. Blood.2016;128(11):1458-1464
- Bartlett NL, Chen R, Fanale M, Brice P, Gopal A, Smith S. et al. Retreatment with brentuximab vedotin in patients with CD30-positive hematologic malignancies. J Hematol Oncol Hematol Oncol.2014;7(1):1-8
- Chen R, Palmer JM, Martin P, Tsai N, Young K, Chen B et al. Results of a Multicenter Phase II Trial of Brentuximab Vedotin as Second-Line Therapy before Autologous Transplantation in Relapsed/Refractory Hodgkin Lymphoma. Biol Blood Marrow Transplant.2015;21(12):2136-2140.
- Ansell SM, Bröckelmann PJ, von Keudell G, et al. Nivolumab for relapsed/refractory classical Hodgkin lymphoma: 5-year survival from the pivotal phase 2 CheckMate 205 study. Blood Adv. 2023;7(20):6266-6274.