

Radiation Maculopathy: Evolving Treatment Paradigms
Treatment Paradigms in Radiation Maculopathy Treatment: What’s Next?
Brittany E. Powell, MD¹, Rachel A. Lieberman, MD², Paul T. Finger, MD³
- Department of Ophthalmology, Naval Medical Center San Diego, San Diego, CA, USA
- Department of Ophthalmology, Walter Reed National Military Medical Center, Bethesda, MD, USA
- The New York Eye Cancer Center, New York, NY, USA
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Powell, BE., Lieberman, RA., et al., 2024. Treatment Paradigms in Radiation Maculopathy Treatment: What’s Next? Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5708
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5708
ISSN 2375-1924
ABSTRACT
Radiation is the most common life and sight-sparing treatment for eye cancer patients. However, it can subsequently lead to a dose-dependent, progressive radiation vasculopathy, which results in retinopathy- or optic neuropathy-related vision loss. Before the advent of intravitreal drug therapy, laser destruction of the ischemic retina was found to be effective for select patients. However, in 2006, the anti-vascular endothelial growth factor bevacizumab was found to trigger regression and suppress radiation maculopathy and optic neuropathy. Anti-vascular endothelial growth factor drugs were administered initially to forestall vision loss in patients with clinically significant disease. Advancements in retinal imaging and a better understanding of their capabilities resulted in earlier intervention with anti-vascular endothelial growth factor treatment. Still, not all the radiation damage to the retina was reversible. To prevent this irreversible injury, periodic anti-vascular endothelial growth factor therapy was given to those patients at the highest risk of developing radiation-related maculopathy within six months of high-dose foveal plaque radiation therapy. This research found that treating patients before clinically evident radiation maculopathy prevented or delayed the onset of radiation maculopathy with preservation of vision. Other strategies to prevent vision loss due to progressive, recalcitrant retinopathy have included the off-label use of alternative therapeutic agents and polypharmacy with intravitreal steroids. These therapeutic agents should be evaluated in protocols where intervention can be guided by optical coherence tomography angiography as subclinical obliterative retinal microangiopathy appears to start at the time of or soon after ocular irradiation. Treatment strategies have evolved, especially as our understanding of the condition has improved. We propose that future protocols take advantage of new therapies, use advances in retinal imaging, and employ novel technologies to establish optimal treatment regimens.
Keywords: radiation retinopathy, radiation optic neuropathy, radiation maculopathy, anti-VEGF, drug, radiation dose, intravitreal, bevacizumab, ranibizumab, steroid.
Introduction
Radiation maculopathy (RM) and optic neuropathy (RON) are vision-threatening complications of radiation therapy used for ocular, periocular, orbital, and sinus tumors. Radiation therapy has primarily replaced enucleation for patients with intraocular melanoma, resulting in significant quality-of-life improvements by conserving both the eye and useful vision. While radiation has changed how ocular melanoma is treated, it can cause damage to surrounding structures. Common complications include dry eye, cataracts, radiation maculopathy, and radiation optic neuropathy. Of these complications, radiation maculopathy is the most frequent cause of irreversible vision loss in eyes treated with radiation and most often results following the treatment of choroidal melanoma.
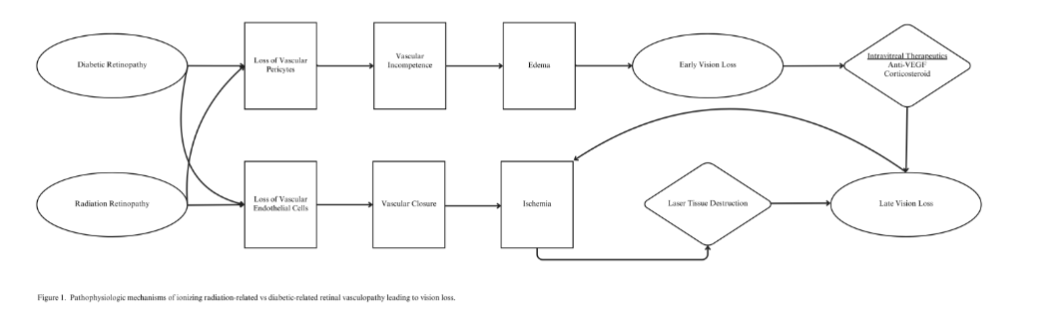
Radiation maculopathy is a result of radiation-induced damage to the retinal microvasculature. Radiation destroys vascular pericytes, leading to leakage of serum and inflammatory components into the retina. Early clinical findings include retinal hemorrhages, cotton wool spots, and macular edema. Later findings, such as capillary dropout, retinal ischemia, and intraretinal neovascular microangiopathy, are best identified on fluorescein angiography. This pathway is similar to the underlying etiology of diabetic retinopathy (DR). Unsurprisingly, patients with radiation maculopathy present similarly to those with diabetic retinopathy, as both conditions are characterized by delayed onset vascular incompetence leading to retinal edema, exudation, and end-stage ischemia with vision loss (Figure 1). Clinically, both are notable for decreased visual acuity and retinal changes, including microaneurysms (MA’s), retinal hemorrhages (RH), exudates, and cotton-wool spots (CWS). Though the vascular changes are similar, radiation optic neuropathy often presents as disc edema or neovascularization.
Innovations in retinal imaging and therapeutics for radiation maculopathy and diabetic retinopathy have advanced in parallel. For both diseases, laser photocoagulation, intravitreal anti-vascular endothelial growth factor (VEGF), and steroid treatments have been used to suppress VEGF. Thus, a historical perspective is essential in mapping out future research goals and understanding shifts in treatment paradigms. For diabetic retinopathy, advancements in retinal imaging from FA to optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA) have helped establish diabetic retinopathy treatment protocols. Though radiation maculopathy tends to be a more fulminant disease, eye cancer and retinal specialists should consider these parallels when developing protocols for the treatment of radiation maculopathy and radiation optic neuropathy.
We propose that the treatment of radiation maculopathy and radiation optic neuropathy mimic the protocols used for diabetic retinopathy. Anti-VEGF therapies have already been widely adopted as a first-line treatment option, and this shift was driven by the recognition that both conditions share similar pathophysiological features, such as increased VEGF levels leading to macular edema and capillary non-perfusion. As such, the treatment of radiation maculopathy and radiation optic neuropathy should continue to evolve, with a strong emphasis on early intervention and the use of newer anti-VEGF therapies closely resembling the treatment protocols for diabetic retinopathy. We postulate that prospective randomized or extensive registry studies will support initial data that such treatment protocols will improve visual outcomes and quality of life for patients with this condition.
Methods
A literature search was last conducted in PubMed and the Cochrane Library databases on 01 July 2024 using the following MeSH terms: radiation retinopathy, radiation maculopathy, radiation optic neuropathy, treatment, light coagulation, intraocular, and anti-VEGF agents. The search used the following text terms: radiation retinopathy, radiation maculopathy, radiation optic neuropathy, light coagulation, photocoagulation, and intraocular injections. Articles were limited to those in English. Relevant articles were pursued, and the initial search expanded using the “pearl-growing” technique. The investigators reviewed articles. The lead investigator performed a full-text review of the articles included, and after the full-text review, an in-depth analysis of the remaining articles was conducted.
Progression of Radiation Maculopathy and Radiation Optic Neuropathy
The speed of onset of clinically detectable radiation-induced vascular incompetence is proportional to radiation dose and dose rate. Typically, the first evidence of radiation maculopathy is macular edema, best measured by OCT or radiation optic neuropathy with disc edema-associated loss of the optic cup. Recent research reveals that early microvascular changes can be found on OCTA. OCT findings have been detected before other clinical signs, including retinal hemorrhages and cotton-wool spots. Late or end-stage radiation maculopathy is characterized by capillary dropout and foveal avascular zone enlargement, best seen on fluorescein angiography. Late-stage radiation optic neuropathy is characterized by disc pallor, fluorescein leakage, and vision loss.
Shields et al. found early evidence of superficial and deep capillary plexus dropout on OCTA in 65 eyes after plaque radiotherapy of choroidal melanoma patients without clinical evidence of radiation maculopathy. This finding was confirmed by Fam et al. after slotted plaque brachytherapy. Highlighting the limitations of ophthalmoscopy for the diagnosis of radiation maculopathy, Horgan et al. used OCT to assess the onset of radiation macular edema in 135 patients after relatively high-dose 125I plaque radiotherapy plus transpupillary thermotherapy for choroidal melanoma. Horgan found a progressive incidence of pre-clinical radiation-induced macular edema as it occurred in 17% of patients by six months, 40% by one year, and 61% by two years. In that series, clinical findings of radiation maculopathy were detected much later, at an average of 17 months, and 38% of cases were complicated by neovascularization, vitreous hemorrhage, and tractional retinal detachments.
First Efforts at Control of Radiation Maculopathy
Before the advent of intravitreal anti-VEGF therapy, sector laser photocoagulation, including demarcation occlusion of the tumor’s circulation and/or a grid pattern laser to extrafoveal areas of the ischemic retina, was initially employed to prevent or delay the progression of radiation maculopathy. This concept resembled laser treatment of branch vein occlusions and diabetic retinopathy. As this was before the advent of OCT, clinical examination and fluorescein angiography were used to demonstrate the efficacy of laser treatment. Materin also found that laser photocoagulation reduced circulation within irradiated choroidal melanomas and minimized hypoxia in tissues downstream. Thus, laser reduced VEGF production, not only from the tumor itself but also from nearby irradiated retinal ischemic tissue. While this was the only method available at the time to reduce VEGF levels, photocoagulation was not ideal for those tumors near, touching, or located beneath the fovea and adjacent to the optic disc due to risks for acute vision loss.
Evolution of Case Selection
Anti-vascular endothelial growth factor therapy provided an exciting solution to this treatment dilemma. Supported by the macular edema measurement capabilities of OCT imaging, intravitreal anti-VEGF medications were initially offered to patients with RM-associated vision loss who could not be treated with laser photocoagulation. This promising new therapeutic demonstrated clinical results with reductions in CWS, RH, and macular edema, preserving vision. As the safety profile was established, anti-VEGF treatment was offered to progressively less advanced radiation maculopathy cases and mirrored ongoing treatment regimens for diabetic retinopathy and macular degeneration. For example, anti-VEGF injections were initially reserved for radiation maculopathy patients with vision loss, then for those with metamorphopsia, and later for eyes with CWS, RH, or macular edema (ME) without metamorphopsia or vision loss. All these cases demonstrated clinical signs or evidence of radiation maculopathy on OCT or FA. However, it became evident that despite the drug-induced resolution of these clinical and OCT findings, persistent retinal vascular damage—and vision loss—remained.
Optical coherence tomography angiography has recently demonstrated early subclinical retinal microangiopathy and that vascular compromise occurred before otherwise measurable radiation maculopathy, such as leakage, edema, hemorrhage, nonperfusion, and neovascularization. Powell and Finger showed that a dose-dependent, ischemic radiation vasculopathy begins at or soon after irradiation but only becomes clinically evident when it causes retinal edema, ischemia, and vision loss. An ever-increasing body of evidence supports targeting this subclinical phase with intravitreal anti-VEGF treatment, particularly in those patients at the highest risk for vision loss due to radiation maculopathy. This was confirmed most recently in a meta-analysis analyzing four studies involving 2109 patients by Victor et al., demonstrating that prophylactic anti-VEGF therapy prevented high-risk patients from developing poor visual acuity (20/200 or worse) by 50%. In addition, there were significant reductions in radiation maculopathy, radiation optic neuropathy, and loss of visual acuity.
Paradigm Shift: Resemblance to Diabetic Retinopathy Treatment Protocols
As retinal imaging advances, the future treatment of radiation maculopathy and radiation optic neuropathy has multiple directions: new pharmacologic agents, combination therapies, gene therapy, radiation protectants, stem cell therapy, new drug delivery systems, and personalized medicine. Traditional treatment approaches to radiation maculopathy and radiation optic neuropathy involve observation of early or mild cases, laser photocoagulation, intravitreal steroids, and anti-VEGF therapy. The first reports of anti-VEGF treatment for radiation maculopathy and radiation optic neuropathy were published in 2007. At that time, bevacizumab and ranibizumab were the only commercially available drugs. Since then, aflibercept, ranibizumab, and brolucizumab have all been used to treat radiation retinopathy. Additional variations include higher-monthly dose therapies utilizing bevacizumab, ranibizumab, and aflibercept, as well as adjuvant intravitreal steroid polypharmacy, which have emerged. Such polypharmacy has been used for cases recalcitrant to anti-VEGF therapy alone. Steroid medications have included triamcinolone acetonide, dexamethasone, and fluocinolone acetonide. Each differs in risk for acute obscuration of vision, duration of action, and cost.
As the treatment of radiation maculopathy and radiation optic neuropathy increasingly paralleled the protocols used for diabetic retinopathy, particularly with the adoption of anti-VEGF therapies as a first-line treatment option, we propose a paradigm shift to include early detection with newer retinal imaging modalities and intervention with proactive treatment initiation rather than a wait-and-see approach, regular intravitreal anti-VEGF injections with formalized protocols that involve early monthly injections initially with a treat-and-extend approach based on the patient’s response, and combination therapy or the use of newer therapeutic agents in such protocols.
Amongst anti-VEGF drugs, high-dose aflibercept is a promising therapeutic option deserving of additional study, particularly in refractory or high-risk cases. Increasing anti-VEGF strength had a beneficial effect in previously unresponsive cases of RM treated with intravitreal ranibizumab (2.0 mg) and bevacizumab (2.0, 2.5, or 3.0 mg). Although high-dose therapy increased drug volume, it resulted in significant reductions in macular edema and maintained or improved best-corrected visual acuity. Aflibercept 8 mg is an anti-VEGF inhibitor that blocks vascular endothelial growth factor-A (VEGF-A) and placental growth factor (PGF), thereby reducing angiogenesis and vascular permeability. The United States Food and Drug Administration (FDA) approved the use of this high-dose formulation of aflibercept in August 2023 for the treatment of diabetic macular edema (recommended dose of 8 mg administered intravitreally every 8 to 16 weeks, after three monthly loading doses) and diabetic retinopathy (recommended dose every 8 to 12 weeks after three monthly loading doses). These recommendations were based on the randomized, double-masked phase 2/3 trial where the 8 mg formulation demonstrated clinically equivalent vision gains to aflibercept 2 mg and that these gains were maintained with fewer injections. In this non-inferiority study, patients receiving aflibercept 8 mg were initially randomized to either 12- or 16-week dosing intervals after three initial monthly doses, compared to an 8-week dosing regimen for aflibercept 2 mg after five initial monthly doses.
In the treatment of radiation retinopathy, aflibercept 2mg/0.05mL injection has been shown in one prospective study by Murry et al. to help maintain vision in patients with radiation maculopathy. In this prospective study, patients were randomly assigned to receive aflibercept 2.0 mg/0.05 mL injections on a fixed 6-week schedule or under a treat-and-extend protocol. In this paper, the authors note that they initially hoped that the treat-and-extend arm would allow for fewer intravitreal injections during the study, but almost all patients required treatment every six weeks. Aflibercept 8 mg may help minimize the number of injections needed while maintaining visual benefit.
Steroids have been a helpful treatment adjunct to anti-VEGF therapy. In patients who did not respond to maximum doses of anti-VEGF medications, Kaplan et al. demonstrated the efficacy of adding 4 mg of triamcinolone acetonide to treatment with anti-VEGF medicines. Vision stabilized or improved in 100% of patients at three months, 88% at six months, 88% at nine months, and 75% at 12 months. If the primary goal is to decrease the VEGF drive and inflammatory cascade that begins at the time of treatment, adjunctive steroids and aflibercept 8 mg should be considered in future treatment protocols.
Faricimab is also deserving of further investigation. Faricimab is a bispecific antibody inhibiting VEGF-A and angiopoietin-2 (Ang-2). It promotes vascular stability by inhibiting Ang-2, which destabilizes blood vessels and exacerbates inflammation. The FDA approved the use of this medication in January 2022 for diabetic macular edema, recommending 6 mg intravitreal injections every four weeks for the first four doses, followed by as-needed dosing. These approvals were based on encouraging results across two identical Phase 3 studies in diabetic macular edema (YOSEMITE and RHINE), which showed that after four initial monthly doses, patients treated with faricimab given at intervals of up to 4 months achieved non-inferior vision gains versus aflibercept given every two months in the first year.
Applying our knowledge of the commonalities in the pathophysiology of diabetic retinopathy and radiation maculopathy, we have had preliminary success in using faricimab to successfully treat refractory radiation maculopathy in two patients with persistent macular edema minimally responsive to aflibercept 2mg/0.05mL. Both patients experienced improvements in their visual acuity along with improvement of macular edema both clinically and on imaging. Faricimab may be particularly applicable in refractory cases that require treatment with both corticosteroids and anti-VEGF agents.
Conclusion
We have presented the microvascular and anatomic pathophysiology of radiation maculopathy and radiation optic neuropathy and compared their current treatment strategies with diabetic retinopathy, given the similarities in their underlying pathophysiology. Diabetic retinopathy has benefited from organized prospective, randomized studies. We postulate that due to their shared vascular findings, those who treat radiation maculopathy and radiation optic neuropathy can benefit from known diabetic retinopathy experience and give an example framework for future studies. We also reviewed the evolution of radiation maculopathy treatments, revealing that at first, laser photocoagulation was used, albeit unknowingly, to reduce VEGF production from choroidal melanomas and radiation-induced ischemic retina, after which it was largely abandoned with the advent of tissue-sparing intravitreal anti-VEGF therapy. During this time, fundus photography, fluorescein angiography, and, most importantly, OCT allowed for periodic assessments of macular thickness and provided a means to quantify the need for periodic treatment. In its many forms, anti-VEGF therapy has been found to prevent or delay vision loss due to radiation maculopathy and optic neuropathy. However, we have also learned that radiation vasculopathy starts at the time of ocular irradiation. Its onset and severity depend on radiation dose to the macula and optic nerve. Both radiation maculopathy and diabetic retinopathy are chronic progressive disease processes that often require continuous periodic treatment.
Advances in retinal imaging will continue to guide the use of newer therapeutic agents in future treatment and research protocols for radiation-related maculopathy and optic neuropathy. For example, OCTA, which can detect subclinical radiation vasculopathy, should be used in future studies to formalize anti-VEGF treatment protocols to prevent vision-threatening radiation maculopathy. Like the more evolved study-based protocols used for treating diabetic retinopathy, the radiation maculopathy literature supports the need for prospective, randomized clinical trials or retrospective multicenter registries. However, unlike diabetic retinopathy, such studies are complicated, using many different radiation sources and methods. Prospective randomized or extensive registry studies are needed to test our early findings that intravitreal anti-VEGF injections may prevent or delay radiation maculopathy and optic neuropathy-related vision loss and can be used to establish ideal treatment regimens. Such data will support the economic commitment of the government, insurers, and patients to radiation maculopathy treatment. It will also allow for the personalization of treatment, improve outcomes, and save vision worldwide.
Conflict of Interest: Dr. Finger holds United States Patent #7,553,486, June 30th, 2009, titled, “Anti-VEGF Treatment for Radiation Induced Vasculopathy.”
References
- Finger PT. Radiation therapy for orbital tumors: concepts, current use, and ophthalmic radiation side effects. Surv Ophthalmol. 2009;54(5):545-568. doi:10.1016/j.survophthal.2009.06.004
- Finger PT. Radiation therapy for choroidal melanoma. Surv Ophthalmol. 1997;42(3):215-232.
- American Brachytherapy Society – Ophthalmic Oncology Task Force. Electronic address: [email protected], ABS – OOTF Committee. The American Brachytherapy Society consensus guidelines for plaque brachytherapy of uveal melanoma and retinoblastoma. Brachytherapy. 2014;13(1):1-14. doi:10.1016/j.brachy.2013.11.008
- Finger PT, Chin KJ, Duvall G, Palladium-103 for Choroidal Melanoma Study Group. Palladium-103 ophthalmic plaque radiation therapy for choroidal melanoma: 400 treated patients. Ophthalmology. 2009;116(4):790-796, 796.e1. doi:10.1016/j.ophtha.2008.12.027
- Melia M, Moy CS, Reynolds SM, et al. Quality of life after iodine 125 brachytherapy vs enucleation for choroidal melanoma: 5-year results from the Collaborative Ocular Melanoma Study: COMS QOLS Report No. 3. Arch Ophthalmol Chic Ill 1960. 2006;124(2):226-238. doi:10.1001/archopht.124.2.226
- Miniati M, Fabrini MG, Genovesi Ebert F, et al. Quality of Life, Depression, and Anxiety in Patients with Uveal Melanoma: A Review. J Oncol. 2018;2018:5253109. doi:10.1155/2018/5253109
- Quality of life assessment in the collaborative ocular melanoma study: design and methods. COMS-QOLS Report No. 1. COMS Quality of Life Study Group. Ophthalmic Epidemiol. 1999;6(1):5-17.
- Finger PT, Chin KJ, Yu GP. Risk Factors for Radiation Maculopathy after Ophthalmic Plaque Radiation for Choroidal Melanoma. Am J Ophthalmol. 2010;149(4):608-615. doi:10.1016/j.ajo.2009.11.006
- Finger PT. Tumour location affects the incidence of cataract and retinopathy after ophthalmic plaque radiation therapy. Br J Ophthalmol. 2000;84(9):1068-1070.
- Hall EJ. Radiation dose-rate: a factor of importance in radiobiology and radiotherapy. Br J Radiol. 1972;45(530):81-97. doi:10.1259/0007-1285-45-530-81
- Groenewald C, Konstantinidis L, Damato B. Effects of radiotherapy on uveal melanomas and adjacent tissues. Eye Lond Engl. 2013;27(2):163-171. doi:10.1038/eye.2012.249
- Archer DB, Gardiner TA. Ionizing radiation and the retina. Curr Opin Ophthalmol. 1994;5(3):59-65.
- Bawankar P, Barman M, Bhattacharjee H, Soibam R, Paulbuddhe V. Radiation retinopathy after external beam irradiation for nasopharyngeal carcinoma: A case report and review of the literature. Pract Radiat Oncol. 2018;8(6):366-368. doi:10.1016/j.prro.2018.03.010
- Hsu CR, Tai MC, Chang YH, Chien KH. Rapid onset of radiation maculopathy after whole-brain radiation therapy: A case report. Medicine (Baltimore). 2016;95(39):e4830. doi:10.1097/MD.0000000000004830
- Gliedman PR, Steinfeld AD. Radiation retinopathy. JAMA. 1987;257(6):780.
- Brown GC, Shields JA, Sanborn G, Augsburger JJ, Savino PJ, Schatz NJ. Radiation retinopathy. Ophthalmology. 1982;89(12):1494-1501.
- Gupta A, Dhawahir-Scala F, Smith A, Young L, Charles S. Radiation retinopathy: case report and review. BMC Ophthalmol. 2007;7:6. doi:10.1186/1471-2415-7-6
- Bianciotto C, Shields CL, Pirondini C, Mashayekhi A, Furuta M, Shields JA. Proliferative radiation retinopathy after plaque radiotherapy for uveal melanoma. Ophthalmology. 2010;117(5):1005-1012. doi:10.1016/j.ophtha.2009.10.015
- Kinyoun JL. Long-term visual acuity results of treated and untreated radiation retinopathy (an AOS thesis). Trans Am Ophthalmol Soc. 2008;106:325-335.
- Young WC, Thornton AF, Gebarski SS, Cornblath WT. Radiation-induced optic neuropathy: correlation of MR imaging and radiation dosimetry. Radiology. 1992;185(3):904-907. doi:10.1148/radiology.185.3.1438784
- Yousef YA, Finger PT. Optical coherence tomography of radiation optic neuropathy. Ophthalmic Surg Lasers Imaging Off J Int Soc Imaging Eye. 2012;43(1):6-12. doi:10.3928/15428877-20111129-09
- Powell BE, Chin KJ, Finger PT. Early anti-VEGF treatment for radiation maculopathy and optic neuropathy: lessons learned. Eye Lond Engl. 2023;37(5):866-874. doi:10.1038/s41433-022-02200-5
- Shields CL, Say EAT, Samara WA, Khoo CTL, Mashayekhi A, Shields JA. Optical Coherence Tomography Angiography of the Macula after Plaque Radiotherapy of Choroidal Melanoma: Comparison of Irradiated Versus Nonirradiated Eyes in 65 Patients. Retina Phila Pa. 2016;36(8):1493-1505. doi:10.1097/IAE.0000000000001021
- Fam A, Tomar AS, Finger PT. OCT-A evaluation of radiation vasculopathy following slotted plaque brachytherapy. Eur J Ophthalmol. 2022;32(4):2459-2568. doi:10.1177/11206721211044339
- Horgan N, Shields CL, Mashayekhi A, Teixeira LF, Materin MA, Shields JA. Early Macular Morphological Change Following Plaque Radiotherapy for Uveal Melanoma. Retina. 2008;28(2):263-273. doi:10.1097/IAE.0b013e31814b1b75
- Horgan N, Shields CL, Mashayekhi A, Shields JA. Classification and treatment of radiation maculopathy. Curr Opin Ophthalmol. 2010;21(3):233-238. doi:10.1097/ICU.0b013e3283386687
- Finger PT. Laser photocoagulation for radiation retinopathy after ophthalmic plaque radiation therapy. Br J Ophthalmol. 2005;89(6):730-738. doi:10.1136/bjo.2004.052159
- Argon laser photocoagulation for macular edema in branch vein occlusion. The Branch Vein Occlusion Study Group. Am J Ophthalmol. 1984;98(3):271-282. doi:10.1016/0002-9394(84)90316-7
- Argon laser scatter photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion. A randomized clinical trial. Branch Vein Occlusion Study Group. Arch Ophthalmol Chic Ill 1960. 1986;104(1):34-41. doi:10.1001/archopht.1986.01050130044017
- A randomized clinical trial of early panretinal photocoagulation for ischemic central vein occlusion. The Central Vein Occlusion Study Group N report. Ophthalmology. 1995;102(10):1434-1444.
- Fundus photographic risk factors for progression of diabetic retinopathy. ETDRS report number 12. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1991;98(5 Suppl):823-833.
- Photocoagulation treatment of proliferative diabetic retinopathy: the second report of diabetic retinopathy study findings. Ophthalmology. 1978;85(1):82-106. doi:10.1016/s0161-6420(78)35693-1
- Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. The Diabetic Retinopathy Study Research Group. Ophthalmology. 1981;88(7):583-600.
- Materin MA, Bianciotto CG, Wu C, Shields CL. Sector laser photocoagulation for the prevention of macular edema after plaque radiotherapy for uveal melanoma: a pilot study. Retina Phila Pa. 2012;32(8):1601-1607. doi:10.1097/IAE.0b013e3182437e70
- Vinores SA, Youssri AI, Luna JD, et al. Upregulation of vascular endothelial growth factor in ischemic and non-ischemic human and experimental retinal disease. Histol Histopathol. 1997;12(1):99-109.
- Banai S, Shweiki D, Pinson A, Chandra M, Lazarovici G, Keshet E. Upregulation of vascular endothelial growth factor expression induced by myocardial ischaemia: implications for coronary angiogenesis. Cardiovasc Res. 1994;28(8):1176-1179. doi:10.1093/cvr/28.8.1176
- Maheshwari A, Finger PT. Laser treatment for choroidal melanoma: Current concepts. Surv Ophthalmol. 2023;68(2):211-224. doi:10.1016/j.survophthal.2022.05.002
- Finger PT, Chin K. Anti–vascular endothelial growth factor bevacizumab (Avastin) for radiation retinopathy. Arch Ophthalmol. 2007;125(6):751-756.
- Finger PT. Radiation retinopathy is treatable with anti-vascular endothelial growth factor bevacizumab (Avastin). Int J Radiat Oncol Biol Phys. 2008;70(4):974-977. doi:10.1016/j.ijrobp.2007.11.045
- Finger PT. Anti-VEGF bevacizumab (Avastin) for radiation optic neuropathy. Am J Ophthalmol. 2007;143(2):335-338. doi:10.1016/j.ajo.2006.09.014
- Finger PT, Chin KJ, Semenova EA. Intravitreal anti-VEGF therapy for macular radiation retinopathy: a 10-year study. Eur J Ophthalmol. 2016;26(1):60-66. doi:10.5301/ejo.5000670
- Fallico M, Reibaldi M, Avitabile T, et al. Intravitreal aflibercept for the treatment of radiation-induced macular edema after ruthenium 106 plaque radiotherapy for choroidal melanoma. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2019;257(7):1547-1554. doi:10.1007/s00417-019-04347-6
- Pooprasert P, Young-Zvandasara T, Al-Bermani A. Radiation retinopathy treated successfully with aflibercept. BMJ Case Rep. 2017;2017. doi:10.1136/bcr-2017-220744
- Skalet AH, Liu L, Binder C, et al. Quantitative OCT Angiography Evaluation of Peripapillary Retinal Circulation after Plaque Brachytherapy. Ophthalmol Retina. 2018;2(3):244-250. doi:10.1016/j.oret.2017.06.005
- Skalet AH, Liu L, Binder C, et al. Longitudinal Detection of Radiation-Induced Peripapillary and Macular Retinal Capillary Ischemia Using OCT Angiography. Ophthalmol Retina. 2020;4(3):320-326. doi:10.1016/j.oret.2019.10.001
- Chu Z, Lin J, Gao C, et al. Quantitative assessment of the retinal microvasculature using optical coherence tomography angiography. J Biomed Opt. 2016;21(6):066008. doi:10.1117/1.JBO.21.6.066008
- Torkashvand A, Riazi-Esfahani H, Ghassemi F, et al. Evaluation of radiation maculopathy after treatment of choroidal melanoma with ruthenium-106 using optical coherence tomography angiography. BMC Ophthalmol. 2021;21(1):385. doi:10.1186/s12886-021-02140-w
- Shah SU, Shields CL, Bianciotto CG, et al. Intravitreal Bevacizumab at 4-Month Intervals for Prevention of Macular Edema after Plaque Radiotherapy of Uveal Melanoma. Ophthalmology. 2014;121(1):269-275. doi:10.1016/j.ophtha.2013.08.039
- Powell BE, Finger PT. Anti–VEGF Therapy Immediately after Plaque Radiation Therapy Prevents or Delays Radiation Maculopathy. Ophthalmol Retina. 2020;4(5):547-550. doi:10.1016/j.oret.2020.01.010
- Kim IK, Lane AM, Jain P, Awh C, Gragoudas ES. Ranibizumab for the Prevention of Radiation Complications in Patients Treated with Proton Beam Irradiation for Choroidal Melanoma (An American Ophthalmological Society Thesis). Trans Am Ophthalmol Soc. Published online 2016:19.
- Shields CL, Dalvin LA, Chang M, et al. Visual Outcome at 4 Years Following Plaque Radiotherapy and Prophylactic Intravitreal Bevacizumab (Every 4 Months for 2 Years) for Uveal Melanoma: Comparison With Nonrandomized Historical Control Individuals. JAMA Ophthalmol. 2020;138(2):136. doi:10.1001/jamaophthalmol.2019.5132
- Victor AA, Andayani G, Djatikusumo A, et al. Efficacy of Prophylactic Anti-VEGF in Preventing Radiation Retinopathy: A Systematic Review and Meta-Analysis. Clin Ophthalmol Auckl NZ. 2023;17:2997-3009. doi:10.2147/OPTH.S433531
- Villegas NC, Mishra K, Steinle N, Liu W, Beadle B, Mruthyunjaya P. Intravitreal brolucizumab as treatment of early onset radiation retinopathy secondary to plaque brachytherapy for choroidal melanoma. Am J Ophthalmol Case Rep. 2022;27:101581. doi:10.1016/j.ajoc.2022.101581
- Finger PT, Chin KJ. High-dose (2.0 mg) Intravitreal Ranibizumab for Recalcitrant Radiation Retinopathy. Eur J Ophthalmol. 2013;23(6):850-856. doi:10.5301/ejo.5000333
- Brown DM, Boyer DS, Do DV, et al. Intravitreal aflibercept 8 mg in diabetic macular oedema (PHOTON): 48-week results from a randomised, double-masked, non-inferiority, phase 2/3 trial. Lancet Lond Engl. 2024;403(10432):1153-1163. doi:10.1016/S0140-6736(23)02577-1
- Murray TG, Latiff A, Villegas VM, Gold AS. Aflibercept for Radiation Maculopathy (ARM Study): Year-2 Extension of a Prospective Clinical Study. J Vitreoretin Dis. 2021;5(3):232-238. doi:10.1177/2474126420958894
- Kaplan RI, Chaugule SS, Finger PT. Intravitreal triamcinolone acetate for radiation maculopathy recalcitrant to high-dose intravitreal bevacizumab. Br J Ophthalmol. 2017;101(12):1694-1698. doi:10.1136/bjophthalmol-2017-310315
- Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. The Lancet. 2022;399(10326):741-755. doi:10.1016/S0140-6736(22)00018-6
References
1. Finger PT. Radiation therapy for orbital tumors: concepts, current use, and ophthalmic radiation side effects. Surv Ophthalmol. 2009;54(5):545-568. doi:10.1016/j.survophthal.2009.06.004
2. Finger PT. Radiation therapy for choroidal melanoma. Surv Ophthalmol. 1997;42(3):215-232.
3. American Brachytherapy Society – Ophthalmic Oncology Task Force. Electronic address: [email protected], ABS – OOTF Committee. The American Brachytherapy Society consensus guidelines for plaque brachytherapy of uveal melanoma and retinoblastoma. Brachytherapy. 2014;13(1):1-14. doi:10.1016/j.brachy.2013.11.008
4. Finger PT, Chin KJ, Duvall G, Palladium-103 for Choroidal Melanoma Study Group. Palladium-103 ophthalmic plaque radiation therapy for choroidal melanoma: 400 treated patients. Ophthalmology. 2009;116(4):790-796, 796.e1. doi:10.1016/j.ophtha.2008.12.027
5. Melia M, Moy CS, Reynolds SM, et al. Quality of life after iodine 125 brachytherapy vs enucleation for choroidal melanoma: 5-year results from the Collaborative Ocular Melanoma Study: COMS QOLS Report No. 3. Arch Ophthalmol Chic Ill 1960. 2006;124(2):226-238. doi:10.1001/archopht.124.2.226
6. Miniati M, Fabrini MG, Genovesi Ebert F, et al. Quality of Life, Depression, and Anxiety in Patients with Uveal Melanoma: A Review. J Oncol. 2018;2018:5253109. doi:10.1155/2018/5253109
7. Quality of life assessment in the collaborative ocular melanoma study: design and methods. COMS-QOLS Report No. 1. COMS Quality of Life Study Group. Ophthalmic Epidemiol. 1999;6(1):5-17.
8. Finger PT, Chin KJ, Yu GP. Risk Factors for Radiation Maculopathy after Ophthalmic Plaque Radiation for Choroidal Melanoma. Am J Ophthalmol. 2010;149(4):608-615. doi:10.1016/j.ajo.2009.11.006
9. Finger PT. Tumour location affects the incidence of cataract and retinopathy after ophthalmic plaque radiation therapy. Br J Ophthalmol. 2000;84(9):1068-1070.
10. Hall EJ. Radiation dose-rate: a factor of importance in radiobiology and radiotherapy. Br J Radiol. 1972;45(530):81-97. doi:10.1259/0007-1285-45-530-81
11. Groenewald C, Konstantinidis L, Damato B. Effects of radiotherapy on uveal melanomas and adjacent tissues. Eye Lond Engl. 2013;27(2):163-171. doi:10.1038/eye.2012.249
12. Archer DB, Gardiner TA. Ionizing radiation and the retina. Curr Opin Ophthalmol. 1994;5(3):59-65.
13. Bawankar P, Barman M, Bhattacharjee H, Soibam R, Paulbuddhe V. Radiation retinopathy after external beam irradiation for nasopharyngeal carcinoma: A case report and review of the literature. Pract Radiat Oncol. 2018;8(6):366-368. doi:10.1016/j.prro.2018.03.010
14. Hsu CR, Tai MC, Chang YH, Chien KH. Rapid onset of radiation maculopathy after whole-brain radiation therapy: A case report. Medicine (Baltimore). 2016;95(39):e4830. doi:10.1097/MD.0000000000004830
15. Gliedman PR, Steinfeld AD. Radiation retinopathy. JAMA. 1987;257(6):780.
16. Brown GC, Shields JA, Sanborn G, Augsburger JJ, Savino PJ, Schatz NJ. Radiation retinopathy. Ophthalmology. 1982;89(12):1494-1501.
17. Gupta A, Dhawahir-Scala F, Smith A, Young L, Charles S. Radiation retinopathy: case report and review. BMC Ophthalmol. 2007;7:6. doi:10.1186/1471-2415-7-6
18. Bianciotto C, Shields CL, Pirondini C, Mashayekhi A, Furuta M, Shields JA. Proliferative radiation retinopathy after plaque radiotherapy for uveal melanoma. Ophthalmology. 2010;117(5):1005-1012. doi:10.1016/j.ophtha.2009.10.015
19. Kinyoun JL. Long-term visual acuity results of treated and untreated radiation retinopathy (an AOS thesis). Trans Am Ophthalmol Soc. 2008;106:325-335.
20. Young WC, Thornton AF, Gebarski SS, Cornblath WT. Radiation-induced optic neuropathy: correlation of MR imaging and radiation dosimetry. Radiology. 1992;185(3):904-907. doi:10.1148/radiology.185.3.1438784
21. Yousef YA, Finger PT. Optical coherence tomography of radiation optic neuropathy. Ophthalmic Surg Lasers Imaging Off J Int Soc Imaging Eye. 2012;43(1):6-12. doi:10.3928/15428877-20111129-09
22. Powell BE, Chin KJ, Finger PT. Early anti-VEGF treatment for radiation maculopathy and optic neuropathy: lessons learned. Eye Lond Engl. 2023;37(5):866-874. doi:10.1038/s41433-022-02200-5
23. Shields CL, Say EAT, Samara WA, Khoo CTL, Mashayekhi A, Shields JA. O Optical Coherence Tomography Angiography of the Macula after Plaque Radiotherapy of Choroidal Melanoma: Comparison of Irradiated Versus Nonirradiated Eyes in 65 Patients. Retina Phila Pa. 2016;36(8):1493-1505. doi:10.1097/IAE.0000000000001021
24. Fam A, Tomar AS, Finger PT. OCT-A evaluation of radiation vasculopathy following slotted plaque brachytherapy. Eur J Ophthalmol. 2022;32(4):2459-2568. doi:10.1177/11206721211044339
25. Horgan N, Shields CL, Mashayekhi A, Teixeira LF, Materin MA, Shields JA. Early Macular Morphological Change Following Plaque Radiotherapy for Uveal Melanoma. Retina. 2008;28(2):263-273. doi:10.1097/IAE.0b013e31814b1b75
26. Horgan N, Shields CL, Mashayekhi A, Shields JA. Classification and treatment of radiation maculopathy. Curr Opin Ophthalmol. 2010;21(3):233-238. doi:10.1097/ICU.0b013e3283386687
27. Finger PT. Laser photocoagulation for radiation retinopathy after ophthalmic plaque radiation therapy. Br J Ophthalmol. 2005;89(6):730-738. doi:10.1136/bjo.2004.052159
28. Argon laser photocoagulation for macular edema in branch vein occlusion. The Branch Vein Occlusion Study Group. Am J Ophthalmol. 1984;98(3):271-282. doi:10.1016/0002-9394(84)90316-7
29. Argon laser scatter photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion. A randomized clinical trial. Branch Vein Occlusion Study Group. Arch Ophthalmol Chic Ill 1960. 1986;104(1):34-41. doi:10.1001/archopht.1986.01050130044017
30. A randomized clinical trial of early panretinal photocoagulation for ischemic central vein occlusion. The Central Vein Occlusion Study Group N report. Ophthalmology. 1995;102(10):1434-1444.
31. Fundus photographic risk factors for progression of diabetic retinopathy. ETDRS report number 12. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1991;98(5 Suppl):823-833.
32. Photocoagulation treatment of proliferative diabetic retinopathy: the second report of diabetic retinopathy study findings. Ophthalmology. 1978;85(1):82-106. doi:10.1016/s0161-6420(78)35693-1
33. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. The Diabetic Retinopathy Study Research Group. Ophthalmology. 1981;88(7):583-600.
34. Materin MA, Bianciotto CG, Wu C, Shields CL. Sector laser photocoagulation for the prevention of macular edema after plaque radiotherapy for uveal melanoma: a pilot study. Retina Phila Pa. 2012;32(8):1601-1607. doi:10.1097/IAE.0b013e3182437e70
35. Vinores SA, Youssri AI, Luna JD, et al. Upregulation of vascular endothelial growth factor in ischemic and non-ischemic human and experimental retinal disease. Histol Histopathol. 1997;12(1):99-109.
36. Banai S, Shweiki D, Pinson A, Chandra M, Lazarovici G, Keshet E. Upregulation of vascular endothelial growth factor expression induced by myocardial ischaemia: implications for coronary angiogenesis. Cardiovasc Res. 1994;28(8):1176-1179. doi:10.1093/cvr/28.8.1176
37. Maheshwari A, Finger PT. Laser treatment for choroidal melanoma: Current concepts. Surv Ophthalmol. 2023;68(2):211-224. doi:10.1016/j.survophthal.2022.05.002
38. Finger PT, Chin K. Anti–vascular endothelial growth factor bevacizumab (Avastin) for radiation retinopathy. Arch Ophthalmol. 2007;125(6):751-756.
39. Finger PT. Radiation retinopathy is treatable with anti-vascular endothelial growth factor bevacizumab (Avastin). Int J Radiat Oncol Biol Phys. 2008;70(4):974-977. doi:10.1016/j.ijrobp.2007.11.045
40. Finger PT. Anti-VEGF bevacizumab (Avastin) for radiation optic neuropathy. Am J Ophthalmol. 2007;143(2):335-338. doi:10.1016/j.ajo.2006.09.014
41. Finger PT, Chin KJ, Semenova EA. Intravitreal anti-VEGF therapy for macular radiation retinopathy: a 10-year study. Eur J Ophthalmol. 2016;26(1):60-66. doi:10.5301/ejo.5000670
42. Fallico M, Reibaldi M, Avitabile T, et al. Intravitreal aflibercept for the treatment of radiation-induced macular edema after ruthenium 106 plaque radiotherapy for choroidal melanoma. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2019;257(7):1547-1554. doi:10.1007/s00417-019-04347-6
43. Pooprasert P, Young-Zvandasara T, Al-Bermani A. Radiation retinopathy treated successfully with aflibercept. BMJ Case Rep. 2017;2017. doi:10.1136/bcr-2017-220744
44. Skalet AH, Liu L, Binder C, et al. Quantitative OCT Angiography Evaluation of Peripapillary Retinal Circulation after Plaque Brachytherapy. Ophthalmol Retina. 2018;2(3):244-250. doi:10.1016/j.oret.2017.06.005
45. Skalet AH, Liu L, Binder C, et al. Longitudinal Detection of Radiation-Induced Peripapillary and Macular Retinal Capillary Ischemia Using OCT Angiography. Ophthalmol Retina. 2020;4(3):320-326. doi:10.1016/j.oret.2019.10.001
46. Chu Z, Lin J, Gao C, et al. Quantitative assessment of the retinal microvasculature using optical coherence tomography angiography. J Biomed Opt. 2016;21(6):066008. doi:10.1117/1.JBO.21.6.066008
47. Torkashvand A, Riazi-Esfahani H, Ghassemi F, et al. Evaluation of radiation maculopathy after treatment of choroidal melanoma with ruthenium-106 using optical coherence tomography angiography. BMC Ophthalmol. 2021;21(1):385. doi:10.1186/s12886-021-02140-w
48. Shah SU, Shields CL, Bianciotto CG, et al. Intravitreal Bevacizumab at 4-Month Intervals for Prevention of Macular Edema after Plaque Radiotherapy of Uveal Melanoma. Ophthalmology. 2014;121(1):269-275. doi:10.1016/j.ophtha.2013.08.039
49. Powell BE, Finger PT. Anti–VEGF Therapy Immediately after Plaque Radiation Therapy Prevents or Delays Radiation Maculopathy. Ophthalmol Retina. 2020;4(5):547-550. doi:10.1016/j.oret.2020.01.010
50. Kim IK, Lane AM, Jain P, Awh C, Gragoudas ES. Ranibizumab for the Prevention of Radiation Complications in Patients Treated with Proton Beam Irradiation for Choroidal Melanoma (An American Ophthalmological Society Thesis). Trans Am Ophthalmol Soc. Published online 2016:19.
51. Shields CL, Dalvin LA, Chang M, et al. Visual Outcome at 4 Years Following Plaque Radiotherapy and Prophylactic Intravitreal Bevacizumab (Every 4 Months for 2 Years) for Uveal Melanoma: Comparison With Nonrandomized Historical Control Individuals. JAMA Ophthalmol. 2020;138(2):136. doi:10.1001/jamaophthalmol.2019.5132
52. Victor AA, Andayani G, Djatikusumo A, et al. Efficacy of Prophylactic Anti-VEGF in Preventing Radiation Retinopathy: A Systematic Review and Meta-Analysis. Clin Ophthalmol Auckl NZ. 2023;17:2997-3009. doi:10.2147/OPTH.S433531
53. Villegas NC, Mishra K, Steinle N, Liu W, Beadle B, Mruthyunjaya P. Intravitreal brolucizumab as treatment of early onset radiation retinopathy secondary to plaque brachytherapy for choroidal melanoma. Am J Ophthalmol Case Rep. 2022;27:101581. doi:10.1016/j.ajoc.2022.101581
54. Finger PT, Chin KJ. High-dose (2.0 mg) Intravitreal Ranibizumab for Recalcitrant Radiation Retinopathy. Eur J Ophthalmol. 2013;23(6):850-856. doi:10.5301/ejo.5000333
55. Brown DM, Boyer DS, Do DV, et al. Intravitreal aflibercept 8 mg in diabetic macular oedema (PHOTON): 48-week results from a randomised, double-masked, non-inferiority, phase 2/3 trial. Lancet Lond Engl. 2024;403(10432):1153-1163. doi:10.1016/S0140-6736(23)02577-1
56. Murray TG, Latiff A, Villegas VM, Gold AS. Aflibercept for Radiation Maculopathy (ARM Study): Year-2 Extension of a Prospective Clinical Study. J Vitreoretin Dis. 2021;5(3):232-238. doi:10.1177/2474126420958894
57. Kaplan RI, Chaugule SS, Finger PT. Intravitreal triamcinolone acetate for radiation maculopathy recalcitrant to high-dose intravitreal bevacizumab. Br J Ophthalmol. 2017;101(12):1694-1698. doi:10.1136/bjophthalmol-2017-310315
58. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. The Lancet. 2022;399(10326):741-755. doi:10.1016/S0140-6736(22)00018-6