





Photobiomodulation for Parkinson’s Disease Treatment
Photobiomodulation as part of a multi-disciplinary approach for the treatment of Parkinson’s disease symptoms
Introduction
Parkinson’s disease is the second most prevalent neurodegenerative disease worldwide and is also the most rapidly increasing¹, with an enormous social and economic cost. It is a complex disease that is characterised by both motor signs and non-motor symptoms and is highly heterogeneous in both symptomology and disease trajectory. In terms of pathology, the hallmarks of Parkinson’s disease are the loss of dopaminergic neurons and the aggregation of alpha-synuclein.
The motor disorders of Parkinson’s disease have historically received more attention than the non-motor symptoms. The major therapeutic medication for Parkinson’s disease over many years has been dopamine replacement therapy with levodopa (L-dopa) combined with medications, such as carbidopa, which counters the premature conversion of the L-dopa to dopamine. L-dopa can improve motor symptoms such as tremors, rigidity and bradykinesia, although people with Parkinson’s disease (PwP) experience “off” periods where symptoms return. The effectiveness of L-dopa also gradually reduces with time due to disease progression, leading to increases in the “off” times and less effect during the “on” times, requiring dose adjustment or switching to other medications. In addition, L-dopa can have debilitating side effects. The majority of PwP using L-dopa will exhibit dyskinesis, toxicity, fluctuations in symptoms or loss of efficacy after five years of use². Other medications include dopamine agonists, monoamine oxidase B (MAO-B) inhibitors and catechol-O-methyl transferase (COMT) inhibitors as well as various medications to counter the side effects of the L-dopa and other medications.
Levodopa and dopamine agonists have little or no effect on non-motor symptoms³. Non-motor symptoms such as declining cognition, reduced sleep quality, constipation, urinary dysfunction, anxiety and depression, apathy, fatigue, and loss of sense of smell, have the potential to have a major impact on health-related quality of life (HRQOL)⁴. Treatment of non-motor symptoms is highly individual and depends on the presenting symptoms and includes many individual medications for the range of symptoms⁵.
Current medication options rely on treatment of symptoms and no medication can, at this time, slow, halt, or reverse the progression of the disease, or provide neuroprotection. Additional therapeutic interventions are required to address disease progression, as well as adverse side-effects of current medications and their reduced effectiveness over time. While there is some potential for repurposed medications, such as anti alpha-synuclein agents⁶ and glucagon-like peptide 1 (GLP-1) receptor agonists⁷, these may take some time to be generally available. Several non-pharmaceutical interventions, however, have shown merit in potentially slowing the deterioration in HRQoL of PwP and in some cases have shown improvement in the clinical motor signs and non-motor symptoms of the disease. Interventions such as exercise, improved nutrition, social activity and light therapy, known as photobiomodulation (PBM) have this potential. Photobiomodulation in particular has recently been shown to be a promising avenue for the treatment of the symptoms of Parkinson’s disease⁸–¹³.
Photobiomodulation is the use of non-thermal light radiation of specific wavelengths to bring about changes to the metabolism of cells and mitochondria¹⁴. Since its beginnings in 1967 with Endre Mester, who demonstrated that laser light accelerated wound healing and hair regrowth in mice¹⁵,¹⁶, PBM, both laser and LED, has been used to treat wounds and burns, to heal tissues such as tendon and cartilage, to reduce inflammation and to relieve pain¹⁷–¹⁹. More recently PBM has been used to target neurodegenerative, neurodevelopmental, neuropsychiatric and brain injury conditions, such as traumatic brain injury, concussion and chronic traumatic encephalopathy, stroke, depression and anxiety, Alzheimer’s disease, autism spectrum disorder, post-traumatic stress disorder, and opioid addiction²⁰–³⁰. Photobiomodulation is remarkably safe, with few adverse effects being reported in over 50 years of PBM use, including for cancers³¹ and for PBM to the brain³²,³³. Any reported side-effects are invariably minor and transient³⁴.
While the effect of PBM on cells and sub-cellular structures has been the subject of research for over 50 years, the full mechanisms have not yet been elucidated. The most widely accepted mechanism is the absorption of photons by cytochrome-C-oxidase in the electron transport chain of mitochondria, which causes the release of reactive oxygen species (ROS) and increases the binding of oxygen, which in turn increases the mitochondrial membrane potential, increases ATP production, and modulates cellular signalling and gene transcription via cAMP, nitric oxide and ROS¹⁴. Photons also directly react with ion channels, such as transient transient receptor potential vanillin (TRPV) channels, as well as potentially triggering a number of other photophysical and mechanotransduction events within the cell and tissues³⁵,³⁶. The actions of PBM on molecular and cellular structures explains the wide range of therapeutic effects that are seen with PBM therapy. One of the central effects of PBM is anti-inflammatory³⁷, which has profound effects on many body processes, including in reducing neuroinflammation in various brain disorders³⁸–⁴⁰.
The major cellular targets of PBM (mitochondrial, inflammatory processes, pain) are also hallmarks of Parkinson’s pathology. The potential of PBM to treat Parkinson’s disease has been demonstrated using in vitro models, where the effects of Parkinson’s disease inducing toxins (MPP⁺, rotenone) can be reversed when PBM is applied either before or after toxin administration⁴¹,⁴². There have also been numerous in vivo models of Parkinson’s disease, using the MPTP model in rodents⁴³–⁴⁹ and in non-human primates⁴⁷,⁵⁰–⁵³ as well as in a genetic model of Parkinson’s disease in mice⁵⁴. These models have demonstrated that PBM can not only reverse the signs of Parkinson’s disease in vivo but can protect and regenerate neurons⁴³,⁴⁶,⁵³,⁵⁴. Animal models (mice and non-human primates) have also demonstrated the effectiveness of delivering PBM to an area remote from the brain such as the tibia or abdomen⁵⁵–⁵⁷ when the head is shielded. This remote or systemic effect of PBM has also been shown in other instances, such as using PBM to treat the tibia in an animal model of cardiac infarction⁵⁸. The mechanism of action of this systemic effect of PBM has been suggested to be cytokines or other chemical messengers or activation of stem cells in the bone marrow or abdominal adipose tissue⁵⁷,⁵⁸. It is also possible that in Parkinson’s disease, which has such a profound microbiome-gut-brain axis connection⁵⁹, a potential mechanism is alteration of the gut microbiome⁶⁰ or stimulation of the vagus nerve. Remote PBM treatment in both mice and non-human primates not only improved the signs of Parkinson’s disease, but also gave neuroprotection to the neurons of the substantia nigra⁵⁵.
The level of pre-clinical evidence suggests that clinical trials are justified⁶¹. A number of small clinical studies have investigated PBM therapy as a treatment for Parkinson’s disease clinical signs and symptoms⁹–¹³, with encouraging improvements in both motor and non-motor symptoms. PBM therapy directed to the abdomen has shown benefits to clinical trial participants, both when used alone¹⁰ and in combination with PBM targeting the brain¹¹. The remote PBM mode of treatment may be especially important in Parkinson’s disease, where the neurons of the substantia nigra are well beyond the distance that light could penetrate into the brain.
Exercise is known anecdotally to help with the symptoms of Parkinson’s disease and is advocated by many Parkinson’s disease groups, movement disorder specialists, rehabilitation providers and clinics. Exercise is often attributed as having the greatest overall effect on HRQoL and progression of the disease
(https://www.hopkinsmedicine.org/health/conditions-and-diseases/parkinsons-disease/fighting-parkinson-disease-with-exercise-and-diet). In animal studies, exercise has been shown to be neuroprotective and to slow the progression of Parkinson’s disease or even reverse the disease⁶²–⁶⁴. Epidemiological studies suggest that mid-life exercise can reduce the risk of Parkinson’s disease later in life⁶⁵,⁶⁶. There is an increasing number of clinical studies using exercise to treat disease symptoms, with moderately large numbers of participants. A meta-analysis of 18 studies⁶⁷ concluded that exercise therapies were effective in improving motor symptoms of Parkinson’s disease, with a high degree of heterogeneity but with no improvement in non-motor symptoms. Another meta-analysis with 51 studies found that resistance training, endurance training and other exercises were safe, feasible and effective for strength, gait, and HRQoL, but “inconsistencies across these findings warrant cautious conclusions”⁶⁸. A further meta-analysis of 20 studies of aerobic exercise⁶⁹ found that tests of balance and mobility, including the unified Parkinson’s disease rating scale (UPDRS) part III (motor) were significantly increased with exercise but quality of life was not.
Exercise can include many formats, including aerobic exercise, treadmills, balance training, progressive resistance training, and complementary exercise such as dance, Tai Chi, and yoga. However, the optimum mode, frequency, and intensity of the exercise required to best alleviate Parkinson’s symptoms are not yet entirely clear. Some studies have suggested that high-intensity exercise can improve motor symptoms, but it is unknown as yet whether exercise can modify disease trajectory and any neuroprotective effect in humans has not yet been clearly reported. A comparison of three forms of exercise (high intensity treadmill, lower intensity treadmill, and stretching/resistance) for three months found improvements in all groups, including gait speed, strength and fitness⁷⁰, while a study that compared progressive resistance exercise to a stretch, balance and strength program found that the progressive resistance group had a greater improvement in UPDRS motor scores than did non-specific exercise over a two year period⁷¹. In a phase 2 clinical trial (Study in Parkinson Disease of Exercise – SPARX)⁷² 128 participants with Parkinson’s disease were assigned to six months of high intensity treadmill exercise, moderate intensity treadmill exercise, or wait-list (control) groups. The mean increase in UPDRS was lower (0.3) in high intensity exercise than the control group (3.2), indicating a retardation of Parkinson’s disease progression.
Recently, a small trial of 17 early Parkinson’s disease participants who completed a ten week ‘PDWarrior’ (PDW) exercise program showed significant improvements in the MDS-UPDRS motor score, the six and ten metre walk test, bradykinesia, and the Parkinson’s disease questionnaire (PDQ-39) quality of life survey⁷³. A second recent study compared aerobic exercise (Park-in-Shape) with stretching over 21 months and found a mean difference in the MDS-UPDRS-Motor score of 4.2 in favour of the aerobic exercise⁷⁴. In a subset of the participants from this trial it was found that aerobic exercise (but not stretching) lead to greater functional connectivity as measured by resting-state functional and structural magnetic resonance imaging (MRI), as well as cognitive performance⁷⁵. Intense exercise using the ‘Beat Parkinson’s Today’ program for six months resulted in a significant increase in dopamine transporter availability and neuromelanin levels in the substantia nigra when a decrease would normally be expected⁷⁶.
Diet is another lifestyle factor that Parkinson’s groups often advise can help with the symptoms of the disease. Lifelong consumption of coffee and polyunsaturated fatty acids is connected with a reduced risk of Parkinson’s disease and consumption of dairy products and saturated fatty acids is connected with an increased risk⁷⁷. Certain diets such as a Mediterranean diet, traditional Japanese diet, or a vegetarian/vegan diet can also reduce the risk of later development of neurodegenerative diseases such as Parkinson’s disease⁷⁸. It is much less clear, however, that changing diet for PwP will alter the trajectory of the disease⁷⁹.
In our clinics, we have, over several years, used PBM, both to the abdomen and to the head to treat the clinical signs and non-motor symptoms of Parkinson’s disease. We collaborate with neurologists, family physicians, physiotherapists, nurse practitioners, dieticians, speech pathologists, and exercise physiologists to provide a personalised therapy regimen for Parkinson’s disease patients, whose specific needs are met in a multidisciplinary therapeutic alliance.
Here we present a case series of seven patients from three different countries (Canada, Germany, Australia) at various stages in their Parkinson’s disease journey who have received this multidisciplinary approach based around PBM therapy, to treat Parkinson’s disease symptoms. Two of these case studies are part of a previously published clinical trial¹⁰, with the remainder attending one of our clinics, either in person or remotely. All have used an at-home PBM laser to irradiate the abdomen and neck, all participate in specific exercise interventions, and all are under the supervision of medical doctors (gerontologists or neurologists).
Aim:
The aim of this study was to report the individual symptomatic responses to a combination of abdominal photobiomodulation therapy, exercise specific for Parkinson’s disease and other interventions in Parkinson’s patients.
Methods:
All participants gave written informed consent during the studies for their data to be used, following Declaration of Helsinki guidelines for clinical patients or as part of the Sydney Adventist Healthcare Ltd Human Research Ethics Committee (HREC) approval (2019/32) and Clinical Trial Registration number: U1111-1205-2035 (Australian New Zealand Clinical Trials Registry).
PHOTOBIOMODULATION INTERVENTION
Abdominal and neck PBM was administered at home by the participants themselves, three time per week using a SYMBYX branded PDCare laser. This is a 2 diode, class 1 laser device (with no need for safety glasses), with a wavelength of 904 nm and a power output of 30 mW per diode. The laser is pressed against nine points on the abdomen (Figure 1) with a force of 5 N to activate the laser and held in place at each point for two minutes to deliver an energy of 7.2 J and a fluence of 5.64 J/cm² per point. This is repeated on the neck at the C1/C2 junction also for two minutes. The total energy delivered is 72 J at each treatment session.
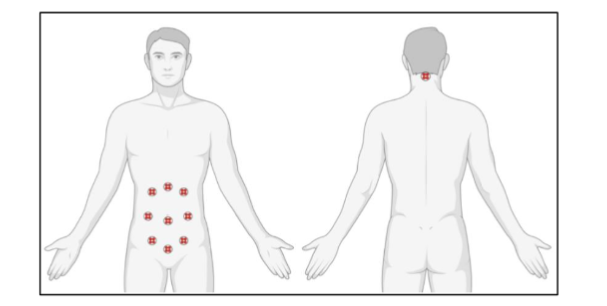
Figure 1. Positioning of the laser device for abdominal and neck treatment
TARGETED EXERCISE
PDWarrior
The PDW program consists of two or three sessions with a trained instructor for assessment, followed by a one-hour class each week as well as a home program. The program includes ten core exercises (Table 1) that cover posture, strength and whole-body movement plus additional exercises such as stationary bike, shadow boxing, and balance exercises.
Gaitway Neurophysio
The Gaitway program is similar to PDW and consists of high amplitude and neuroactive exercise in a social setting, including Rock Steady
Boxing classes, Parkinson’s Wellness Recovery Moves (PWR!Moves), as well as forced amplitude training with functional goals and physiotherapy tailored to individuals.
MEDICAL OVERSIGHT
Participants were overseen by their own neurologists or gerontologists with careful monitoring of medication. Broad recommendations were given for diet. Participants were assessed for outcomes by their own neurologist and physiotherapists.
OUTCOME MEASURES
Outcome measures for objective measures of motor signs, cognition and sense of smell for C4 and C5 are presented in Table 2.
Results
Individual improvements in the clinical signs and symptoms of Parkinson’s disease are summarized in Table 3 and remarks by the participants and their neurologists in Table 4.
Table 1. PDWarrior core exercises
| Core exercise | Exercise focus |
|---|---|
| Sky reach | Trunk rotation and big shoulder and arm movements. |
| Overhead ball throw | Elicit force and power from upper limbs. Good for those who experience bradykinesia and those who are tremor dominant. Also has an element of balance control. |
| 007 | Trunk rotation and balance. |
| Scarf snatch | Arm swing and ballistic, powerful movements. Good if main symptom is bradykinesia. Speed and timing in upper limbs with some balance component. |
| Penguin waddle | Weight shift and stepping. Helpful if experiencing mild episodes of freezing. |
| Banded side-step | Posture, coordination and upper-limb resistance. |
| Ta-Dahs | Shoulder extension, stepping and exaggerated arm movement, with an added balance and coordination component. |
| Squat and stop | Power squatting to strengthen legs and lower back and generate full extension and power in arms and hands. |
| Over the river | Coordinating big strides and powerful arm swings and stepping. Also helps with 180° turns. |
| Box step | Coordination, balance and timing. |
Table 2. Clinical study outcome measures for participants C4 and C5
| Outcome measure | Test | Description |
|---|---|---|
| Gait | TUG | Assessors measured the time taken for a participant to stand from a chair, walk 3m, turn around a marker, return to chair and sit down⁸⁰ |
| TUG manual | As for TUG except that the participant was carrying a cup of water⁸⁰ | |
| TUG cognitive | As for TUG except that the participant was asked to count backwards from 40 by twos⁸⁰ | |
| 10MWT speed | Participants walked a 10m track. After walking 2m, assessors measured the time taken to walk a further 6m⁸¹ | |
| 10MWT stride length | During the 10MWT assessors also counted the number of strides taken to walk the same 6m⁸¹ | |
| Dynamic balance | Step test | Participants stood with feet together, 10 cm from a 10 cm high step. Assessors counted the number of times that a participant placed their foot repeatedly on the step in 15 seconds. Both legs were tested⁸². |
| Fine motor control | Spiral test | The time taken to draw between the lines of a printed Archimedean spiral. A time penalty of 3 sec and 5 sec were given for touching a line or crossing a line respectively. The dominant hand was tested⁸³. |
| Static balance | TS | The time that a participant could stand with one foot in front of the other (heel to toe) until a step was taken, or the participant used a hand to steady themselves. The assessment was terminated at 30 seconds. The test was repeated with eyes open and closed and both legs were tested⁸⁴. |
| SLS | The time that a participant could stand with one foot raised in the air a step was taken, or the participant used a hand to steady themselves. The assessment was terminated at 30 seconds. The test was repeated with eyes open and closed and both legs were tested⁸⁴. | |
| Cognition | MoCA | Participants completed the MoCA test version 8.1 (www.mocatest.org), which was scored by assessors. |
| Quality of Life | PDQ-39 | Participants completed the PDQ-39 to assess QoL across eight domains. Scores for each domain were divided by the highest possible score for that domain and converted to a percentage. The PDQ summary index (PDSI) was the sum of dimension scores divided by eight⁸⁶. |
| Sleep quality | PDSS | Participants completed the PDSS (original version) with 15 items to assess sleep quality⁸⁷. |
10MWT = 10 metre walk test; CSB = combined static balance; MoCA = Montreal cognitive assessment; QoL = quality of life PDQ-39 = Parkinson’s disease questionnaire 39; Parkinson’s disease Summary Index = PDSI; PDSS = Parkinson’s disease sleep scale; SLS = single leg stance; TS = tandem stance; TUG = timed up-and-go; Table 3 Summary of reported individual changes in Parkinson’s disease symptoms
| CASE (treatment period) | tremor | mobility | balance | Fine motor control | Sense of smell | Cognition | Sleep | Quality of life |
|---|---|---|---|---|---|---|---|---|
| C1 (6 weeks) H&Y stage 2 | improved | improved | improved | improved MMSE | ||||
| C2 (6 weeks) H&Y stage 2 | reduced | improved | improved mood/motivation | |||||
| C3 (3 years) H&Y stage 1 | no deterioration | regained | ||||||
| C4 (3 years) H&Y stage 1.5 | improved | improved | no deterioration | regained | marginal MoCA improvement | improved | marginal improvement in PDQ39 | |
| C5 (3 years) H&Y stage 1.5 | improved | improved | no deterioration | improved MoCA | slight deterioration | slight deterioration in PDQ39 | ||
| C6 (2 years) H&Y stage 2 | no deterioration | improved | improved | improved | improved | improved | improved | Improved outlook |
| C7 (2 years) H&Y stage 1 | no deterioration | no deterioration | no deterioration | no deterioration | no deterioration | no deterioration |
H&Y = Hoehn & Yahr
Case Summaries
CASE 1
Photobiomodulation and PDWarrior:
C1 is an Australian male, aged 72 at referral who had been diagnosed ten years previously. He was referred by a consultant neurologist to the Sydney Parkinson’s disease clinic. His medication at that time was Karvea 300mg, Zanidip 10mg, and Staleva 150mg.
Neurologist Assessment:
23/10/2021. Compared to his assessment one year previously he was frailer and had more fatigue. He had significant extrapyramidal dysfunction with rigidity, reduced hand/fingers performance, dystonic twisting of his right foot, and postural orthostatic tachycardia syndrome (POTS). The Montreal cognitive assessment (MoCA) and the mini-mental state exam (MMSE) were administered.
Treatment:
C1 began the abdominal and neck PBM therapy at a low dose in the clinic, which was gradually increased until the full regimen was administered at home. He began targeted exercise (PDW). He received physiotherapy and additional PBM for back pain.
Neurologist Reassessment:
04/12/2021. Since beginning PBM therapy and PDW exercises, C1 showed significant objective improvements in his appearance, his posture (less stooping; less POTS), and his walking. He could sustain finger and hand motor tasks. His cognition improved on MMSE from 28 to 30.
Neurologist comment:
“Patient seemed unaware of the improvements”
Physiotherapy Assessment:
C1 had improved his walking speed and hand function.
CASE 2
Photobiomodulation and PDWarrior:
C2 is an Australian male, aged 68 at referral who had been diagnosed five years previously. He was referred to the Sydney Parkinson’s disease clinic in July 2021 by a consultant neurologist. His current medication was Sifrol 375mg, Xadago 100mg, and Staleva 200mg. He had previously used a red-light helmet for two years.
Neurologist Assessment:
06/07/2021. C2 was tired with a lack of energy and impaired mood and motivation. He had a tremor, dystonia in his calf and leg.
Treatment:
Introduction of abdominal and neck PBM therapy, initially in the clinic, then at home after four weeks. Continued with PDW.
Neurologist Reassessment:
17/08/2021. C2 showed objective improvement to assessments six weeks and one year previously with improvements in gait, tremor, walking speed, mood, and motivation. He no longer was considering deep brain stimulation.
Neurologist comment:
“His improvements coincided with his commencement of abdominal laser”
CASE 3
Photobiomodulation, non-specific exercise and diet:
C3 is an Australian male, aged 61 at referral. He self-diagnosed in February 2021 with mild “pill-rolling” symptoms, and the diagnosis was confirmed in August 2021. He self-referred to the Sydney clinic on advice of a friend.
Treatment:
C3 began using the abdominal PBM therapy product in September 2021 with the SYMBYX PDCare laser after seeing a television news story. The laser is used three times per week. He began using the SYMBYX Neuro helmet in August 2023. He also decided to reduce his carbohydrate and sugar intake and to eliminated gluten from his diet, following a modified keto diet and practised intermittent fasting. He began bike riding at the beginning of 2022 (more than 5 km per day) and walks up to 17 km each weekend and takes stairs when possible. He attends a gym twice per week. He monitors his exercise and sleep with a smart watch.
Response to treatment:
C3 lost some weight on this diet and now has a BMI of 20. At the beginning of 2022, C3 noticed that he could now smell some strong offensive odours (such as pig farms, roadkill) after having profound loss of sense of smell. Over time his sense of smell increased, and more pleasant odours were detected (roses, jasmine, cooking smells). Eating has become more enjoyable.
Reflections:
“I believe these combined protocols have helped restore my sense of smell and hopefully slowed my PD progression. … We only get 5 senses to experience the world, so to lose one of them is very stressful and hard to put into words, but to get that sense back is remarkable and something I truly cherish… able to smell nature, farms, field flowers and food again is a revelation and I can ONLY attribute this to PDCare.”
CASE 4
Photobiomodulation and PDWarrior – clinical trial:
C4 is an Australian male who was 72 years of age when he enrolled in the clinical study in September 2019¹⁰ (participant S3) and he had been diagnosed eight years previously by a neurologist. This study used abdominal and neck treatment with a 904 nm laser (the precursor to the SYMBYX PDCare) three times per week in the clinic for 12 weeks followed by at home use initially for one year and extended to three years.
Treatment:
C4 has continued to use the same protocol for three years and beyond as well as attending PDW once per week.
Assessment:
C4 was assessed for objective changes in a range of motor signs (mobility, balance, fine motor control), cognition (MoCA), sense of smell (University of Pennsylvania Smell Identification Test – UPSIT), subjective changes in HRQoL (PDQ-39 questionnaire), and Parkinson’s disease sleep scale (PDSS) questionnaire before any treatment began and again after one year and three years.
Motor outcomes:
Table 5. C4 improved his mobility over three years of PBM therapy. His walking speed improved from 2.07 m/s at baseline to 2.18 m/s in one year and further improved over three years to 3.13 m/s and his stride length remained the same (approximately one metre) over this time. His timed up-and-go (TUG) test worsened over three years from 4.2 seconds to 5.1 seconds, although the TUG (manual) and TUG (cognitive) both improved from 6.1 to 5.2 seconds and from 5.8 to 5.4 seconds respectively. C4 walks every day and completes a (walking) full marathon of 42 km each year with the Parkinson’s NSW Walking Marathon. The spiral test was essentially unchanged over three years (26.1 and 26.4 seconds).
Balance:
Dynamic balance (number of steps in 15 seconds) improved from 21 to 23 while standing on his unaffected leg and 20 to 23 steps while standing on his affected leg. Static balance, as measured by tandem stance (TS) with eyes closed, improved from 3.0 to 17.0 seconds (for affected leg behind) and from 7.4 to 17.5 seconds for unaffected leg behind. Similarly, single leg stance (SLS) with eyes closed improved from 2.4 to 5.0 seconds when standing on his affected leg. However, SLS with eyes closed standing on his unaffected leg worsened over three years (8.7 to 6.2 seconds).
Non-motor symptoms:
C4 had excellent cognition (MoCA) at baseline (29/30), which showed marginal improvement to 29.3 after three years of PBM therapy (Table 5). His subjective quality-of-life assessment score (PDSI) improved marginally from 5.7/100 to 4.5/100, which are low scores indicating a good HRQoL. The PDQ-39 domains of mobility, activities of daily living and cognition improved while the domain of communication deteriorated, and the other four domains remained unchanged. Sleep quality, as measured by the PDSS, improved from a score of 99/150 to 127/150 which is an improvement above the cut-off (100) thought to indicate troublesome sleep problems⁸⁸. C4 showed an objective sense of smell improvement after 12 weeks of PBM therapy, going from complete anosmia to severe hyposmia as determined by the UPSIT. C4 has reported that his sense of smell has continued to improve over three years.
CASE 5
Photobiomodulation and PDWarrior – clinical trial:
C5 is an Australian male who was 69 years of age when he enrolled in the clinical study in September 2019¹⁰ (participant S4) and he had been diagnosed 5.5 years previously by two neurologists. This study used abdominal and neck treatment with 904 nm laser (precursor to the SYMBYX PDCare) three times per week in the clinic for 12 weeks followed by at home use initially for one year and extended to three years.
Treatment:
C5 has continued to use the same protocol for three years and beyond, as well as attending PDW once per week.
Assessment:
He was assessed for objective changes in a range of motor signs (mobility, balance, fine motor control), and cognition (MoCA), as well as subjective changes in HRQoL (using PDQ-39) and sleep quality (using PDSS) before any treatment began and again after one year and three years.
Motor Outcomes:
Table 5. C5 initially improved his walking speed from 0.75 m/s at baseline to 1.85 m/s at one year but this deteriorated at three years to 0.58 m/s. Similarly, his stride length has deteriorated from 1.4 to 0.75 metres over three years. In contrast, his three TUG tests have all improved over three years from 8.6 to 5.9 seconds, 8.4 to 6.9 seconds and 8.9 to 6.9 seconds for TUG, TUG (manual) and TUG (cognitive) respectively. His spiral test remained essentially unchanged over three years (28.9 and 30.5 seconds).
Balance:
Table 5. Dynamic balance improved over three years from 14 to 20 steps in 15 seconds when standing on his unaffected leg and 15 to 21 steps when standing on his affected leg. Static balance improved with SLS with eyes closed from 23.5 seconds on his affected leg and 19.6 seconds on his unaffected leg to the pass value of 30 seconds for both legs. SLS with eyes closed improved from 2.2 to 3.5 seconds when standing on his unaffected leg and 2.3 to 2.9 seconds when standing on his affected leg. TS with eyes closed improved from 3.0 to 9.0 seconds with the unaffected leg behind but deteriorated from 10.9 to 3.4 with the affected leg behind.
Non-motor symptoms:
C5 improved his cognition (MoCA) from 27/30 to 29.3/30 (Table 5). His PDSI deteriorated slightly from 3.2/100 to 3.8/100, nonetheless indicating a good HRQoL. He showed an improvement in his emotional domain (4.2 to 0) and a deterioration in the mobility (2.5 to 5) and Stigma (0 to 6.3) domains, with all other sub-scores unchanged. Sleep quality (PDSS score) deteriorated from a score of 124/100 to 109/100 but remained above the cut-off (100) for troublesome sleep problems.
CASE 6
Photobiomodulation and diet:
C6 is a 62-year-old German female at the time of her initial virtual assessment in 2023, who was diagnosed by a neurologist ten years previously, although symptoms had been present one year previous to this. She felt no “normalcy” in her life. She had tremors in her right leg, had right foot drag and had micrographia. Neurology testing revealed reduced auditory processing and her MDS-UPDRS score was 24. She had been on L-dopa medication for the first two years. Since then, she has undergone metal detox, had switched to a vegetarian diet with periods of vegan diet with initial significant improvement. This had stabilized symptoms for eight years, with improved “normalcy” and reduced tremors. Since 2020 she has felt that her cognition was declining, she was beginning to frequently misplace things, her note taking had slowed, and her sleep had deteriorated to less than six hours per night.
Assessment:
with a local and internet conferencing multi-disciplinary team.
Treatment:
Began PBM therapy in 2023 to the abdomen and neck with a SYMBYX PDCare, with no additional change in diet.
Outcome:
C6 found an immediate and dramatic improvement, with all of her symptoms disappearing in the first week, which she called a “miracle cure”. Her sleep improved, her limp disappeared, her gait improved with an unconscious longer stride and greater arm swing, and she began dancing again. Her sense of smell, which had declined on objective testing since being diagnosed with Parkinson’s disease, improved to the same level as before diagnosis. Her memory improved with improvement in being able to think of words, improved short term memory, not misplacing objects and functioning at her clinical practice more effectively. As a result of these improvements she completely discontinued her Ongentys medication with the result of returning symptoms, worsening sleep, deterioration in balance and gait and inability to concentrate. When she restarted Ongentys she began to regain the improvements after three weeks and had regained all previous improvements by six weeks. C6 continues to improve and can see improvements in writing, she has a more positive outlook, has reduced “off” periods, and has less need for rests during walks. She has restarted crocheting and can continue for longer periods of time.
Reflection:
“It would seem that the things that improved have stayed improved, sometimes even getting slowly better over time. In particular, my memory and my sleep quality, both of which add to my quality of life. … the last thing – quality of life – is better than I ever thought it could be. It is strange, but I have the feeling that I am somehow healing. …sometimes a feeling of freedom and joy overtakes me so suddenly I have to cry.”
CASE 7
Photobiomodulation and Gaitway exercise program:
C7 is a Canadian male aged 73 years at the beginning of PBM therapy, diagnosed by a neurologist eight years previously, although his symptoms had been noted by his family doctor two or three years before this. For the previous 30 years he had undertaken regular vigorous exercise, yoga and meditation.
Assessed:
in Gaitway clinic in April 2020. His MDS-UPDRS score was 19 out of a maximum of 119. He was categorized as Hoehn & Yahr stage 1. He had good balance, with only mild postural changes and slight left-hand tremors when he felt stressed.
Treatment:
C7 has been attending targeted exercise classes and exercising at home three times per week, including PWR!Moves, Smovey Class and Rock Steady Boxing. He has been advised as to the timing of his protein intake and tweaking of his diet for Parkinson’s disease. He also has regular massage and uses naturopathy. C7 added the abdominal and neck laser PBM therapy in 2020, which was initially helpful for pain associated with the exercises.
Outcome:
His symptoms have remained stable for over 2 years.
Neurologist Comment:
“it is highly unusual for a person with Parkinson’s to be on the ‘baby dose’ of Prolopa and Levodopa/Benserazide for the past eight years, particularly with his symptoms noted by his GP 10-11 years ago.” The neurologist also commented on the diet and exercise routine but asked: “if there was anything else he was doing.”
Table 4 Neurologists comments and participant reflections
| CASE no. (treatment period) | Remarks |
|---|---|
| C1 (6 weeks) H&Y stage 2 | Neurologist: Patient seemed unaware of the improvements |
| C2 (6 weeks) H&Y stage 2 | Neurologist: His improvements coincided with his commencement of abdominal laser |
| C3 (3 years) H&Y stage 1 | Participant: I believe these combined protocols have helped restore my sense of smell and hopefully slowed my PD progression. … We only get 5 senses to experience the world, so to lose one of them is very stressful and hard to put into words, but to get that sense back is remarkable and something I truly cherish…. able to smell nature, farms, fields flowers and food again is a revelation and I can ONLY attribute this to PDCare |
| C6 (2 years) H&Y stage 2 | Participant: It would seem that the things that improved have stayed improved, sometimes even getting slowly better over time. In particular, my memory and my sleep quality, both of which add to my quality of life. … the last thing – quality of life – is better than I ever thought it could be. It is strange, but I have the feeling that I am somehow healing. …sometimes a feeling of freedom and joy overtakes me so suddenly I have to cry |
| C7 (2 years) H&Y stage 1 | Neurologist: It is highly unusual for a person with Parkinson’s to be on the ‘baby dose’ of Prolopa and Levodopa/Benserazide for the past eight years, particularly with his symptoms noted by his GP 10-11 years ago. (also asked) if there was anything else he was doing |
H&Y = Hoehn & Yahr
Table 5. Baseline and 3-year results for PBM therapy for C4 and C5.
| C4 baseline | C4 3-years (% improvement) | C5 baseline | C5 3-years (% improvement) | |
|---|---|---|---|---|
| Mobility tests | ||||
| 10MWT walk speed (m/s) | 2.1 | 3.1 (70%) | 0.8 | 0.6 (-25%) |
| 10MWT stride length (m) | 1.0 | 1.0 (0%) | 1.4 | 0.8 (-42%) |
| TUG (s) | 4.2 | 5.1 (-21%) | 8.6 | 5.9 (31%) |
| TUG manual (s) | 7.3 | 5.4 (26%) | 6.1 | 5.2 (15%) |
| TUG cognitive (s) | 5.8 | 5.4 (14%) | 8.9 | 6.9 (22%) |
| Fine Motor Control test | ||||
| Spiral test – dominant hand (s) | 26.1 | 26.4 | 28.9 | 30.5 |
| Dynamic Balance test (n) | ||||
| step test standing on unaffected leg | 21 | 23 (10%) | 15 | 21 (40%) |
| step test standing on affected leg | 20 | 23 (15%) | 14 | 20 (43%) |
| Static Balance tests (s) | ||||
| TS affected leg behind eyes open | 30 | 30 | 30 | 30 |
| TS unaffected leg behind eyes open | 30 | 30 | 30 | 30 |
| SLS on affected leg eyes open | 30 | 30 | 23.5 | 30 (28%) |
| SLS on unaffected leg raised eyes open | 4.2 | 16.2 (300%) | 19.6 | 30 (53%) |
| TS affected leg behind eyes closed | 3.0 | 17.0 (467%) | 10.9 | 3.4 (-69%) |
| TS unaffected leg behind eyes closed | 7.4 | 17.5 (136%) | 3.0 | 9.0 (200%) |
| SLS on affected leg eyes closed | 8.7 | 6.2 (-29%) | 2.3 | 3.5 (52%) |
| SLS on unaffected leg eyes closed | 2.4 | 5.0 (-108%) | 2.2 | 2.9 (32%) |
| Cognition test | ||||
| MoCA | 29.0 | 29.3 | 27.0 | 29.3 |
| Quality of Life | ||||
| PDQ-39 score (PDSI) | 6.09 | 4.03 | 3.18 | 2.97 |
| Sleep quality | ||||
| PDSS score | 99 | 127 | 124 | 109 |
| Sense of smell | ||||
| UPSIT | 16 | 19 (at12 weeks) | nd | nd |
* = significant improvement in outcome measure at five years compared to before commencement of PBM therapy (p<0.05); 10MWT = 10 metre walk test; TUG = timed up-and-go; TS = tandem stance; SLS = single leg stance; MoCA = Montreal Cognitive Assessment; PDQ-39 = Parkinson’s disease questionnaire-39; PDSI = PDQ summary index; PDSS = Parkinson’s disease sleep scale; n = number; s = seconds; m = metres; m/s = metres per second Discussion
All case studies described here showed an improvement in some symptoms of Parkinson’s disease, as assessed by themselves, their own neurologists, or by objective measures. These improvements were heterogeneous and individual to the participant and were seen over weeks (six weeks for C1 and C2) and years (2 years for C6; three years for C3, C4, C5; 4 years for C7). Most importantly there were very few symptoms that showed a deterioration in any participant. While it is known that there is a large placebo effect in clinical trials and especially in clinical trials of Parkinson’s disease⁸⁹ due to increases in dopamine release in the striatum⁹⁰,⁹¹, placebo effects might be expected to persist for weeks or possibly months⁹², but not the years seen in five of these case studies.
The symptoms of Parkinson’s disease would normally be expected to show a deterioration over time and with aging⁹³. For example, motor symptoms would be expected to worsen as evidenced by an increasing MDS-UPDRS-III (motor) score, which has been variously estimated to increase anywhere from 0.6 to 8.9 points per year⁹⁴–⁹⁷. Similarly, both TUG and walk speed/stride length would be expected to deteriorate as Parkinson’s disease progresses⁹³,⁹⁸,⁹⁹, as would balance¹⁰⁰. In our study, five of the seven case studies self-reported or were assessed as having improved mobility, with increased walking speed and stride length and/or reduced time to perform the TUG. The other two case studies did not report a deterioration in their motor symptoms. Balance also was measured or reported to be improved for four participants, with the remaining three not reporting a decline.
The TUG test in particular is an objective and useful test for PwP⁸¹,¹⁰⁰, since it measures functional mobility incorporating standing, initiation of walking, walking speed and balance. TUG can track subtle changes in Parkinson’s disease¹⁰¹ and has been shown to be correlated with falls risk¹⁰²,¹⁰³, as has the 10MWT⁸². While L-dopa can help with motor symptoms and improve TUG times during “on” periods, medication has little effect on balance⁹⁹. The improvement in TUG times and walk speed, as well as the improvement in balance seen in the case studies reported here, may diminish the risk of falls for these PwP. Falls are a major concern in PwP, with up to 60% having at least one fall per year and 39% having multiple falls¹⁰⁴. Falls can have an enduring impact on mobility and continuing quality of life.
Fine motor control improved in two participants, one of whom was assessed by a neurologist (C1) and one who self-assessed (C6) returning to doing crochet. Objective measures in fine motor control in C4 and C5 using a spiral test showed no improvement but also no deterioration in three years. Although often overshadowed by the focus on the changes of larger movements, the deterioration of fine motor control can have a disproportionate impact on quality of life including the inability to fasten buttons and use eating utensils. The deterioration in fine motor control has been suggested as a marker for disease progression with dexterity to fasten buttons significantly correlated with cognitive decline, and dexterity in knot tying significantly associated with the progression of functional disability¹⁰⁵.
One of the participants in the study (C5) showed an improvement in MoCA over three years, one participant (C1) demonstrated improved MMSE over six weeks and one (C6) self-assessed as having improved cognition. Cognitive dysfunction is a major symptom of Parkinson’s disease as the disease progresses, greatly affecting quality of life and ability to self-care¹⁰⁶. Although more marked in later stages of Parkinson’s disease, cognition would nonetheless be expected to deteriorate with time, estimated to be 1.1 points per year in the MMSE¹⁰⁷ and between 0.1 and 3.7 points per year in the MoCA¹⁰⁸.
Health-related quality of life, as subjectively measured by PDSI, showed little change for C4 and C5 over three years. Both had a very low score indicating a good HRQoL, and importantly this did not deteriorate markedly over three years. C2 was reported by his neurologist as having improved mood and C6 also self-reported an improvement in mood.
Sense of smell returned or improved in three of our participants. C3 reported the gradual return of his sense of smell and C4 showed objective improvement from total anosmia to severe hyposmia with UPSIT score of 16 increasing to 19 over a period of 12 weeks. He reported continued improvement over the three years of PBM therapy. Olfactory dysfunction is a common non-motor symptom for PwP and one that does not respond to medication¹⁰⁹ nor can be related to a placebo effect.
The responses of the participants in these case studies to the multidisciplinary treatment approach was highly individual, as indeed are symptoms of Parkinson’s disease. All participants showed improvement in some, although not all symptoms. Importantly there was improvement not only in motor but also non-motor symptoms and no participant felt that their Parkinson’s symptoms deteriorated during the weeks or years of the treatment.
People with Parkinson’s disease have a substantial increase in the rate of physical decline and also in quality of life compared to non-Parkinson’s women and men of the same age¹¹⁰ and this decline begins well before their neurological diagnosis. Any treatment modality that can improve or even maintain physical function and non-motor symptoms of Parkinson’s disease, is worthy of further exploration. Such a treatment regimen would play a potentially vital role in slowing the progression of symptoms of Parkinson’s disease, reducing falls and maintaining quality of life.
An integrative approach utilising precision medication as required in response to symptom change, combined with photobiomodulation treatment, dietary advice and targeted exercise would appear to be best practice. This approach could result in optimal precision medicine to potentially slow the progression of symptoms in Parkinson’s disease.
We have presented here clinical evidence that PBM, when combined with other therapies such as diet and targeted exercise, can improve some symptoms of Parkinson’s disease, including motor and non-motor symptoms. These improvements have not only been observed by the participants, but also independently confirmed by researchers and the persons’ own doctors and neurologists. Importantly, these improvements are clinically meaningful for each participant and have lasted for up to a number of years.
Conflict of Interest:
AL and BB are co-founders, shareholders and Scientific Advisors to SYMBYX Pty Ltd
AS is the principal of Saltmarche Health
MM is the founder of PDWarrior
OH is the owner of Gaitway Neurophysio
Funding Statement:
None.
Acknowledgements:
None.
References
1. Dorsey ER, Zafar M, Lettenberger SE, et al. Trichloroethylene: An Invisible Cause of Parkinson’s Disease? Journal of Parkinson’s Disease. 2023;13: 203-218. doi:10.3233/JPD-225047
2. Marsden CD. Problems with long-term levodopa therapy for Parkinson’s disease. Clin Neuropharmacol. 1994;17 Suppl 2:S32-44.
3. Antonini A, Emmi A, Campagnolo M. Beyond the dopaminergic system: lessons learned from levodopa resistant symptoms in Parkinson’s disease. Movement disorders clinical practice. 2023;10(Suppl 2):S50.
4. Heimrich KG, Schönenberg A, Santos-García D, Mir P, Coppadis Study G, Prell T. The Impact of Nonmotor Symptoms on Health-Related Quality of Life in Parkinson’s Disease: A Network Analysis Approach. J Clin Med. Mar 29 2023;12(7)doi:10 .3390/jcm12072573
5. Church FC. Treatment Options for Motor and Non-Motor Symptoms of Parkinson’s Disease. Biomolecules. Apr 20 2021;11(4)doi:10.3390/biom 11040612
6. Pagano G, Taylor KI, Anzures Cabrera J, et al. Prasinezumab slows motor progression in rapidly progressing early-stage Parkinson’s disease. Nature Medicine. 2024/04/01 2024;30(4):1096-1103. doi:10.1038/s41591-024-02886-y
7. Foltynie T, Athauda D. Chapter 13 – Repurposing anti-diabetic drugs for the treatment of Parkinson’s disease: Rationale and clinical experience. In: Björklund A, Cenci MA, eds. Progress in Brain Research. Elsevier; 2020:493-523.
8. Bicknell B, Liebert A, Herkes G. Parkinson’s Disease and Photobiomodulation: Potential for Treatment. Journal of Personalized Medicine. 2024;14(1):112.
9. Herkes G, McGee C, Liebert A, et al. A novel transcranial photobiomodulation device to address motor signs of Parkinson’s disease: a parallel randomised feasibility study. EClinicalMedicine. 2023;66
10. Liebert A, Bicknell B, Laakso E-L, et al. Remote Photobiomodulation Treatment for the Clinical Signs of Parkinson’s Disease: A Case Series Conducted During COVID-19. Photobiomodulation, photome dicine, and laser surgery. 2022;40(2):112-122.
11. Liebert A, Bicknell B, Laakso EL, et al. Improvements in clinical signs of Parkinson’s disease using photobiomodulation: a prospective proof-of-concept study. BMC Neurology. 2021/07/ 02 2021;21(1):256. doi:10.1186/s12883-021-02248-y
12. McGee C, Liebert A, Bicknell B, et al. A Randomized Placebo-Controlled Study of a Transcranial Photobiomodulation Helmet in Parkinson’s Disease: Post-Hoc Analysis of Motor Outcomes. J Clin Med. 2023;12(8):2846.
13. Liebert A, Bicknell B, Laakso E-L, et al. Improvements in the clinical signs of Parkinson’s disease using photobiomodulation: a 3-year follow-up case series. Medical Research Archives. 2023;11(3)doi:doi.org/10.18103/mra.v11i3.3690
14. Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochemistry and Photobiology. 2018;94(2):199-212. doi:doi:10.1111/php.12864
15. Mester E, Szende B, P. G. The effect of laser beams on the growth of hair in mice. Radiobiology and Radiotherapy 1968;9(5):621-626.
16. E M, G L, M S, B S, J. T. The simulating effect of low power laser rays on biological systems. Laser Review. 1968;1:3.
17. Dompe C, Moncrieff L, Matys J, et al. Photobiomodulation-Underlying Mechanism and Clinical Applications. J Clin Med. Jun 3 2020;9(6):1724. doi:10.3390/jcm9061724
18. Glass GE. Photobiomodulation: the clinical applications of low-level light therapy. Aesthetic Surgery Journal. 2021;41(6):723-738.
19. González-Muñoz A, Cuevas-Cervera M, Pérez-Montilla JJ, et al. Efficacy of Photobiomodulation Therapy in the Treatment of Pain and Inflammation: A Literature Review. Healthcare. 2023;11(7):938.
20. Kim H, Kim MJ, Kwon YW, et al. Benefits of a Skull-Interfaced Flexible and Implantable Multilight Emitting Diode Array for Photobiomodulation in Ischemic Stroke. Advanced Science. 2022;9(11):21 04629. doi: https://doi.org/10.1002/advs.202104629
21. Casalechi HL, Dumont AJL, Ferreira LAB, et al. Acute effects of photobiomodulation therapy and magnetic field on functional mobility in stroke survivors: a randomized, sham-controlled, triple-blind, crossover, clinical trial. Lasers in medical science. 2020;35(6):1253-1262.
22. Longo F, Gabriela M, Tan CO, et al. Effect of Transcranial Low-Level Light Therapy vs Sham Therapy Among Patients With Moderate Traumatic Brain Injury: A Randomized Clinical Trial. JAMA Network Open. 2020;3(9):e2017337-e2017337. doi:10.1001/jamanetworkopen.2020.17337
23. Naeser MA, Martin PI, Ho MD, et al. Transcranial, Red/Near-Infrared Light-Emitting Diode Therapy to Improve Cognition in Chronic Traumatic Brain Injury. Photomed Laser Surg. Dec 2016;34(12):610-626. doi:10.1089/pho.2015.4037
24. Naeser MA, Martin PI, Ho MD, et al. Transcranial Photobiomodulation Treatment: Significant Improvements in Four Ex-Football Players with Possible Chronic Traumatic Encephalopathy. Journal of Alzheimer’s Disease Reports. 2023;7:77-105. doi:10.3233/ADR-220022
25. Li Y, Dong Y, Yang L, et al. Transcranial photobiomodulation prevents PTSD-like comorbidities in rats experiencing underwater trauma. Translational Psychiatry. 2021;11(1):270.
26. Cassano P, Petrie SR, Mischoulon D, et al. Transcranial Photobiomodulation for the Treatment of Major Depressive Disorder. The ELATED-2 Pilot Trial. Photomed Laser Surg. Dec 2018;36(12):634-646. doi:10.1089/pho.2018.4490
27. Saltmarche AE, Naeser MA, Ho KF, Hamblin MR, Lim L. Significant improvement in cognition in mild to moderately severe dementia cases treated with transcranial plus intranasal photobiomodulation: case series report. Photomedicine and laser surgery. 2017;35(8):432-441.
28. Chao LL. Effects of Home Photobiomodulation Treatments on Cognitive and Behavioral Function, Cerebral Perfusion, and Resting-State Functional Connectivity in Patients with Dementia: A Pilot Trial. Photobiomodul Photomed Laser Surg. Mar 2019;37(3):133-141. doi:10.1089/photob.2018.4555
29. Ceranoglu TA, Cassano P, Hoskova B, et al. Transcranial Photobiomodulation in Adults with High-Functioning Autism Spectrum Disorder: Positive Findings from a Proof-of-Concept Study. Photobiomodulation, Photomedicine, and Laser Surgery. 2022/01/01 2021;40(1):4-12. doi:10.1089 /photob.2020.4986
30. Schiffer F, Khan A, Bolger E, Flynn E, Seltzer WP, Teicher MH. An Effective and Safe Novel Treatment of Opioid Use Disorder: Unilateral Transcranial Photobiomodulation. Front Psychiatry. 2021;12:713686. doi:10.3389/fpsyt.2021.713686
31. de Pauli Paglioni M, Araújo ALD, Arboleda LPA, et al. Tumor safety and side effects of photobiomodulation therapy used for prevention and management of cancer treatment toxicities. A systematic review. Oral oncology. 2019;93:21-28.
32. Cassano P, Norton R, Caldieraro MA, et al. Tolerability and safety of transcranial photobiomodulation for mood and anxiety disorders. Photonics. 2022;9(8):507.
33. Wang EB, Kaur R, Fierro M, Austin E, Jones LR, Jagdeo J. Chapter 5 – Safety and penetration of light into the brain. In: Hamblin MR, Huang Y-Y, eds. Photobiomodulation in the Brain. Academic Press; 2019:49-66.
34. Cassano P, Caldieraro MA, Norton R, et al. Reported Side Effects, Weight and Blood Pressure, After Repeated Sessions of Transcranial Photobiomodulation. Photobiomodulation, photo medicine, and laser surgery. 2019;37(10):651-656.
35. Sharma SK, Sardana S, Hamblin MR. Role of opsins and light or heat activated transient receptor potential ion channels in the mechanisms of photobiomodulation and infrared therapy. Journal of Photochemistry and Photobiology. 2023/02/01/ 2023;13:100160. doi: https://doi.org/10.1016/j.jpap.2023.100160
36. Liebert A, Capon W, Pang V, et al. Photophysical Mechanisms of Photobiomodulation Therapy as Precision Medicine. Biomedicines. 2023;11(2):237.
37. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobio modulation. AIMS biophysics. 05/19 2017;4(3): 337-361. doi:10.3934/biophy.2017.3.337
38. Cardoso FDS, Salehpour F, Coimbra NC, Gonzalez-Lima F, Gomes da Silva S. Photobiomodulation for the treatment of neuroinflammation: A systematic review of controlled laboratory animal studies. Front Neurosci. 2022;16:1006031. doi:10.3389/fnins.20 22.1006031
39. Hamblin MR. Chapter 8 – Mechanisms of photobiomodulation in the brain. In: Hamblin MR, Huang Y-Y, eds. Photobiomodulation in the Brain. Academic Press; 2019:97-110.
40. Shamloo S, Defensor E, Ciari P, et al. The anti-inflammatory effects of photobiomodulation are mediated by cytokines: Evidence from a mouse model of inflammation. Front Neurosci. 2023; 17:1150156. doi:10.3389/fnins.2023.1150156
41. Liang HL, Whelan HT, Eells JT, Wong-Riley MT. Near-infrared light via light-emitting diode treatment is therapeutic against rotenone-and 1-methyl-4-phenylpyridinium ion-induced neurotoxicity. Neuroscience. 2008;153(4):963-974.
42. Ying R, Liang HL, Whelan HT, Eells JT, Wong-Riley MT. Pretreatment with near-infrared light via light-emitting diode provides added benefit against rotenone- and MPP+-induced neurotoxicity. Brain Res. Dec 3 2008;1243:167-73. doi:10.1016/j.brainres.2008.09.057
43. Shaw VE, Spana S, Ashkan K, et al. Neuroprotection of midbrain dopaminergic cells in MPTP‐treated mice after near‐infrared light treatment. Journal of Comparative Neurology. 2010;518(1):25-40.
44. Peoples C, Spana S, Ashkan K, et al. Photobiomodulation enhances nigral dopaminergic cell survival in a chronic MPTP mouse model of Parkinson’s disease. Parkinsonism & related disorders. 2012;18(5):469-476.
45. Moro C, Torres N, El Massri N, et al. Photobiomodulation preserves behaviour and midbrain dopaminergic cells from MPTP toxicity: evidence from two mouse strains. BMC neuroscience. 2013;14(1):40.
46. Reinhart F, El Massri N, Darlot F, et al. 810 nm near-infrared light offers neuroprotection and improves locomotor activity in MPTP-treated mice. Neuroscience Research. 2015;92:86-90.
47. El Massri N, Moro C, Torres N, et al. Near-infrared light treatment reduces astrogliosis in MPTP-treated monkeys. Experimental brain research. 2016;234(11):3225-3232.
48. Reinhart F, Massri NE, Torres N, et al. The behavioural and neuroprotective outcomes when 670nm and 810nm near infrared light are applied together in MPTP-treated mice. Neurosci Res. Apr 2017;117:42-47. doi:10.1016/j.neures.2016.11.006
49. Reinhart F, El Massri N, Chabrol C, et al. Intracranial application of near-infrared light in a hemi-parkinsonian rat model: the impact on behavior and cell survival. Journal of Neurosurgery. 2016;124(6):1829-1841.
50. Moro C, El Massri N, Torres N, et al. Photobiomodulation inside the brain: a novel method of applying near-infrared light intracranially and its impact on dopaminergic cell survival in MPTP-treated mice. Journal of Neurosurgery. 2014;120(3):670-683. doi:doi:10.31 71/2013.9.JNS13423
51. El Massri N, Lemgruber AP, Rowe IJ, et al. Photobiomodulation-induced changes in a monkey model of Parkinson’s disease: changes in tyrosine hydroxylase cells and GDNF expression in the striatum. Experimental brain research. 2017;235(6):1861-1874.
52. El Massri N, Cullen KM, Stefani S, et al. Evidence for encephalopsin immunoreactivity in interneurones and striosomes of the monkey striatum. Exp Brain Res. 04 2018;236(4):955-961. doi:10.1007/s00221-018-5191-9
53. Moro C, El Massri N, Darlot F, et al. Effects of a higher dose of near-infrared light on clinical signs and neuroprotection in a monkey model of Parkinson’s disease. Brain Research. 2016;1648:19-26.
54. Purushothuman S, Nandasena C, Johnstone DM, Stone J, Mitrofanis J. The impact of near-infrared light on dopaminergic cell survival in a transgenic mouse model of parkinsonism. Brain research. 2013;1535:61-70.
55. Gordon LC, Martin KL, Torres N, et al. Remote photobiomodulation targeted at the abdomen or legs provides effective neuroprotection against parkinsonian MPTP insult. European Journal of Neuroscience. 2023;57(9):1611-1624.
56. Stone J, Johnstone D, Mitrofanis J. The helmet experiment in Parkinson’s disease: an observation of the mechanism of neuroprotection by near infra-red light. 2013:
57. Johnstone DM, Mitrofanis J, Stone J. Targeting the body to protect the brain: inducing neuroprotection with remotely-applied near infrared light. Neural Regen Res. Mar 2015;10 (3):349-51. doi:10.4103/1673-5374.153673
58. Tuby H, Maltz L, Oron U. Induction of Autologous Mesenchymal Stem Cells in the Bone Marrow by Low-Level Laser Therapy Has Profound Beneficial Effects on the Infarcted Rat Heart. Lasers in surgery and medicine. 2011;43:401-409.
59. Bicknell B, Liebert A, Borody T, Herkes G, McLachlan C, Kiat H. Neurodegenerative and Neurodevelopmental Diseases and the Gut-Brain Axis: The Potential of Therapeutic Targeting of the Microbiome. International Journal of Molecular Sciences. 2023;24(11):9577.
60. Bicknell B, Liebert A, Johnstone D, Kiat H. Photobiomodulation of the microbiome: implications for metabolic and inflammatory diseases. Lasers in medical science. 2018;34(2):317-327.
61. Salehpour F, Sadigh-Eteghad s, Mahmoudi J, Kamari F, Cassano P, Hamblin M. Photobio modulation Therapy for Parkinson’s Disease. Photo biomodulation for the Brain Photobiomodulation Therapy in Neurology and Neuropsychiatry. Springer; 2023:chap 10. Synthesis Lectures on Biomedical Engineering.
62. Tajiri N, Yasuhara T, Shingo T, et al. Exercise exerts neuroprotective effects on Parkinson’s disease model of rats. Brain research. 2010;1310 :200-207.
63. Svensson M, Lexell J, Deierborg T. Effects of physical exercise on neuroinflammation, neuroplasticity, neurodegeneration, and behavior: what we can learn from animal models in clinical settings. Neurorehabilitation and neural repair. 2015;29(6):577-589.
64. Ferreira AFF, Binda KH, Real CC. The effects of treadmill exercise in animal models of Parkinson’s disease: A systematic review. Neuroscience & Biobehavioral Reviews. 2021;131 :1056-1075.
65. Chahine LM, Darweesh SKL. Physical Activity and the Risk of Parkinson Disease. Neurology. 2023;101(4):151-152. doi:10.1212/WNL.00000000 00207527
66. Fang X, Han D, Cheng Q, et al. Association of levels of physical activity with risk of Parkinson disease: a systematic review and meta-analysis. JAMA network open. 2018;1(5):e182421-e182421.
67. Choi H-y, Cho K-H, Jin C, et al. Exercise Therapies for Parkinson’s Disease: A Systematic Review and Meta-Analysis. Parkinson’s Disease. 2020/09/08 2020;2020:2565320. doi:10.1155/202 0/2565320
68. Gamborg M, Hvid LG, Dalgas U, Langeskov‐Christensen M. Parkinson’s disease and intensive exercise therapy—An updated systematic review and meta‐analysis. Acta Neurologica Scandinavica. 2022;145(5):504-528.
69. Zhen K, Zhang S, Tao X, Li G, Lv Y, Yu L. A systematic review and meta-analysis on effects of aerobic exercise in people with Parkinson’s disease. NPJ Parkinsons Dis. Oct 31 2022;8(1):146. doi:10.1038/s41531-022-00418-4
70. Shulman LM, Katzel LI, Ivey FM, et al. Randomized clinical trial of 3 types of physical exercise for patients with Parkinson disease. JAMA neurology. 2013;70(2):183-190.
71. Corcos DM, Robichaud JA, David FJ, et al. A two‐year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Movement Disorders. 2013;28(9):1230-1240.
72. Schenkman M, Moore CG, Kohrt WM, et al. Effect of High-Intensity Treadmill Exercise on Motor Symptoms in Patients With De Novo Parkinson Disease: A Phase 2 Randomized Clinical Trial. JAMA Neurol. Feb 1 2018;75(2):219-226. doi:10.1001/jamaneurol.2017.3517
73. Tucak C, Chih H, Mastaglia F, Rodrigues J. The ‘PD Warrior’exercise program improves motor outcomes and quality of life in patients with early Parkinson’s disease: results of a pilot study. Internal Medicine Journal. 2023;
74. van der Kolk NM, de Vries NM, Kessels RP, et al. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: a double-blind, randomised controlled trial. The Lancet Neurology. 2019;18(11):998-1008.
75. Johansson ME, Cameron IGM, Van der Kolk NM, et al. Aerobic Exercise Alters Brain Function and Structure in Parkinson’s Disease: A Randomized Controlled Trial. Annals of Neurology. 2022/02/01 2022;91(2):203-216. doi: https://doi.org/10.1002/ana.26291
76. de Laat B, Hoye J, Stanley G, et al. Intense exercise increases dopamine transporter and neuromelanin concentrations in the substantia nigra in Parkinson’s disease. npj Parkinson’s Disease. 2024/02/09 2024;10(1):34. doi:10.1038/s 41531-024-00641-1
77. Boulos C, Yaghi N, El Hayeck R, Heraoui GN, Fakhoury-Sayegh N. Nutritional risk factors, microbiota and Parkinson’s disease: what is the current evidence? Nutrients. 2019;11(8):1896.
78. Knight E, Geetha T, Burnett D, Babu JR. The Role of Diet and Dietary Patterns in Parkinson’s Disease. Nutrients. 2022;14(21):4472.
79. Hegelmaier T, Lebbing M, Duscha A, et al. Interventional Influence of the Intestinal Microbiome Through Dietary Intervention and Bowel Cleansing Might Improve Motor Symptoms in Parkinson’s Disease. Cells. 2020;9(2):376.
80. Shumway-Cook A, Brauer S, Woollacott M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Physical Therapy. 2000;80(9):896-903. doi:10.1093/ptj/80.9.896
81. Lang JT, Kassan TO, Devaney LL, Colon-Semenza C, Joseph MF. Test-Retest Reliability and Minimal Detectable Change for the 10-Meter Walk Test in Older Adults With Parkinson’s disease. Journal of Geriatric Physical Therapy. 2016;39(4) doi:https://doi.org/10.1519/JPT.0000000000000068
82. Hill K, Bernhardt J, McGann A, Maltese D, Berkovits D. A new test of dynamic standing balance for stroke patients: reliability, validity, and quantitative clinical tests. Physiotherapy Canada. 1996;47:257-262.
83. Pullman SL. Spiral Analysis: A New Technique for Measuring Tremor With a Digitizing Tablet. Movement Disorders. 1998;13(S3):85-89. doi:10.1 002/mds.870131315
84. Smithson F, Morris ME, Iansek R. Performance on Clinical Tests of Balance in Parkinson’s Disease. Physical Therapy. 1998;78(6):577-592. doi:10.1093 /ptj/78.6.577
85. Gill DJ, Freshman A, Blender JA, Ravina B. The Montreal cognitive assessment as a screening tool for cognitive impairment in Parkinson’s disease. Movement Disorders. 2008;23(7):1043-1046.
86. Peto V, Jenkinson C, Fitzpatrick R. PDQ-39: a review of the development, validation and application of a Parkinson’s disease quality of life questionnaire and its associated measures. Journal of Neurology. 1998/04/01 1998;245(1):S10-S14. doi:10.1007/PL00007730
87. Chaudhuri KR, Pal S, DiMarco A, et al. The Parkinson’s disease sleep scale: a new instrument for assessing sleep and nocturnal disability in Parkinson’s disease. J Neurol Neurosurg Psychiatry. Dec 2002;73(6):629-35. doi:10.1136/ jnnp.73.6.629
88. Ray Chaudhuri K, Martinez-Martin P, Rolfe KA, et al. Improvements in nocturnal symptoms with ropinirole prolonged release in patients with advanced Parkinson’s disease. European Journal of Neurology. 2012;19(1):105-113. doi:https://doi.org/10.1111/j.1468-1331.2011.03442.x
89. Lidstone SC. Great Expectations: The Placebo Effect in Parkinson’s Disease. In: Benedetti F, Enck P, Frisaldi E, Schedlowski M, eds. Placebo. Springer Berlin Heidelberg; 2014:139-147.
90. Quattrone A, Barbagallo G, Cerasa A, Stoessl AJ. Neurobiology of placebo effect in Parkinson’s disease: What we have learned and where we are going. Movement Disorders. 2018;33(8):1213-1227. doi:https://doi.org/10.1002/mds.27438
91. Wager TD, Atlas LY. The neuroscience of placebo effects: connecting context, learning and health. Nat Rev Neurosci. Jul 2015;16(7):403-18. doi:10.1038/nrn3976
92. Goetz CG, Leurgans S, Raman R. Placebo-associated improvements in motor function: Comparison of subjective and objective sections of the UPDRS in early Parkinson’s disease. Movement Disorders. 2002;17(2):283-288. doi: https://doi.org/10.1002/mds.10024
93. Wilson J, Alcock L, Yarnall AJ, et al. Gait Progression Over 6 Years in Parkinson’s Disease: Effects of Age, Medication, and Pathology. Front Aging Neurosci. 2020;12:577435. doi:10.3389/fna gi.2020.577435
94. Schrag A, Dodel R, Spottke A, Bornschein B, Siebert U, Quinn NP. Rate of clinical progression in Parkinson’s disease. A prospective study. Movement disorders. 2007;22(7):938-945. doi: https://doi.org/10.1002/mds.21429
95. Lawton M, Ben-Shlomo Y, May MT, et al. Developing and validating Parkinson’s disease subtypes and their motor and cognitive progression. Journal of Neurology, Neurosurgery & Psychiatry. 2018;89(12):1279-1287.
96. Alves G, Wentzel-Larsen T, Aarsland D, Larsen JP. Progression of motor impairment and disability in Parkinson disease. Neurology. 2005;65(9):1436-1441. doi:10.1212/01.wnl.0000183359.50822.f2
97. Holden SK, Finseth T, Sillau SH, Berman BD. Progression of MDS-UPDRS Scores Over Five Years in De Novo Parkinson Disease from the Parkinson’s Progression Markers Initiative Cohort. Movement Disorders Clinical Practice. 2018/01/01 2018;5(1) :47-53. doi: https://doi.org/10.1002/mdc3.12553
98. Shalash A, Helmy A, Salama M, Gaber A, El-Belkimy M, Hamid E. A 6-month longitudinal study on worsening of Parkinson’s disease during the COVID-19 pandemic. NPJ Parkinsons Dis. Aug 31 2022;8(1):111. doi:10.1038/s41531-022-00376-x
99. Johansson C, Lindström B, Forsgren L, Johansson GM. Balance and mobility in patients with newly diagnosed Parkinson’s disease – a five-year follow-up of a cohort in northern Sweden. Disability and Rehabilitation. 2020/03/12 2020;42 (6):770-778. doi:10.1080/09638288.2018.1509240
100. Morris S, Morris ME, Iansek R. Reliability of measurements obtained with the Timed “Up & Go” test in people with Parkinson disease. Physical therapy. 2001;81(2):810-818. doi: https://doi.org/10.1093/ptj/81.2.810
101. Steffen T, Seney M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Physical therapy. 2008;88(6):733-746. doi: https://doi.org/10.2522/ptj.20070214
102. Vance RC, Healy DG, Galvin R, French HP. Dual tasking with the timed “up & go” test improves detection of risk of falls in people with Parkinson disease. Physical therapy. 2015;95(1):95-102.
103. Nocera JR, Stegemöller EL, Malaty IA, et al. Using the Timed Up & Go test in a clinical setting to predict falling in Parkinson’s disease. Archives of physical medicine and rehabilitation. 2013;94 (7):1300-1305.
104. Allen NE, Schwarzel AK, Canning CG. Recurrent falls in Parkinson’s disease: a systematic review. Parkinson’s disease. 2013;2013 doi: https://doi.org/10.1155/2013/906274
105. Huang Y-C, Hong C-T, Chi W-C, et al. Deterioration of fine motor skills and functional disability in patients with moderate-to-advanced Parkinson disease: A longitudinal follow-up study. Archives of Gerontology and Geriatrics. 2024/06/01/ 2024;121:105366. doi:https://doi.org/10.1016/j.archger.2024.105366
106. Wills A-MA, Elm JJ, Ye R, et al. Cognitive function in 1736 participants in NINDS Exploratory Trials in PD Long-term Study-1. Parkinsonism & Related Disorders. 2016/12/01/ 2016;33:127-133. doi:https://doi.org/10.1016/j.parkreldis.2016.10.005
107. Aarsland D, Andersen K, Larsen JP, et al. The Rate of Cognitive Decline in Parkinson Disease. Archives of Neurology. 2004;61(12):1906-1911. doi:10.1001/archneur.61.12.1906
108. Greenland JC, Camacho M, Williams-Gray CH. Chapter 12 – The dilemma between milestones of progression versus clinical scales in Parkinson’s disease. In: Espay AJ, ed. Handbook of Clinical Neurology. Elsevier; 2023:169-185.
109. Tarakad A, Jankovic J. Chapter Seventeen – Anosmia and Ageusia in Parkinson’s Disease. In: Chaudhuri KR, Titova N, eds. International Review of Neurobiology. Academic Press; 2017:541-556.
110. Palacios N, Gao X, Schwarzschild M, Ascherio A. Declining quality of life in Parkinson disease before and after diagnosis. J Parkinsons Dis. 2012;2(2):153-60. doi:10.3233/jpd-2012-12083.